
Implementation of COVID-19 Infection Control Measures by German Dentists: A Qualitative Study to Identify Enablers and Barriers

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Qualitative Approach and Research Paradigm
2.2. Research Characteristics and Reflexivity
2.3. Context
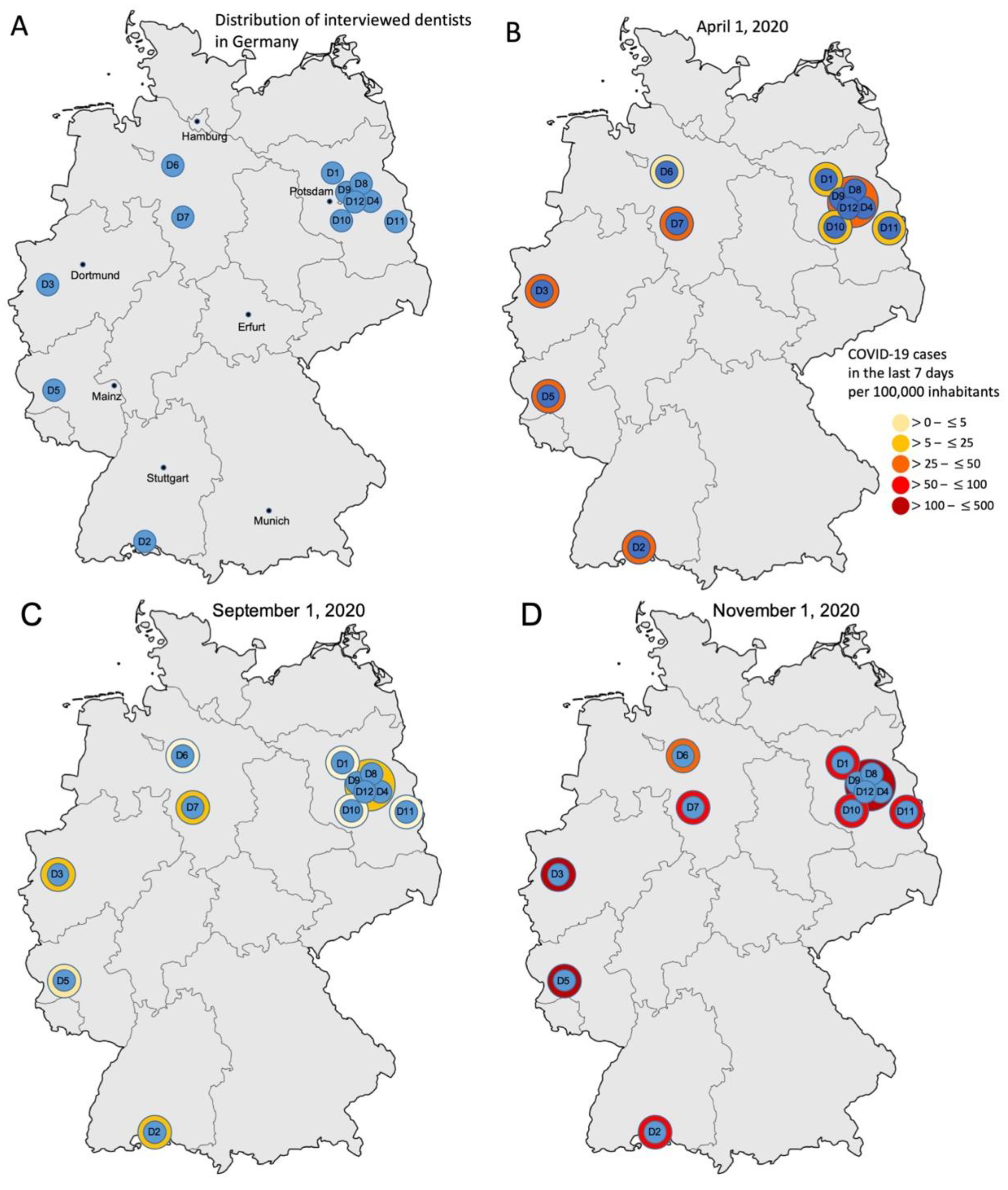
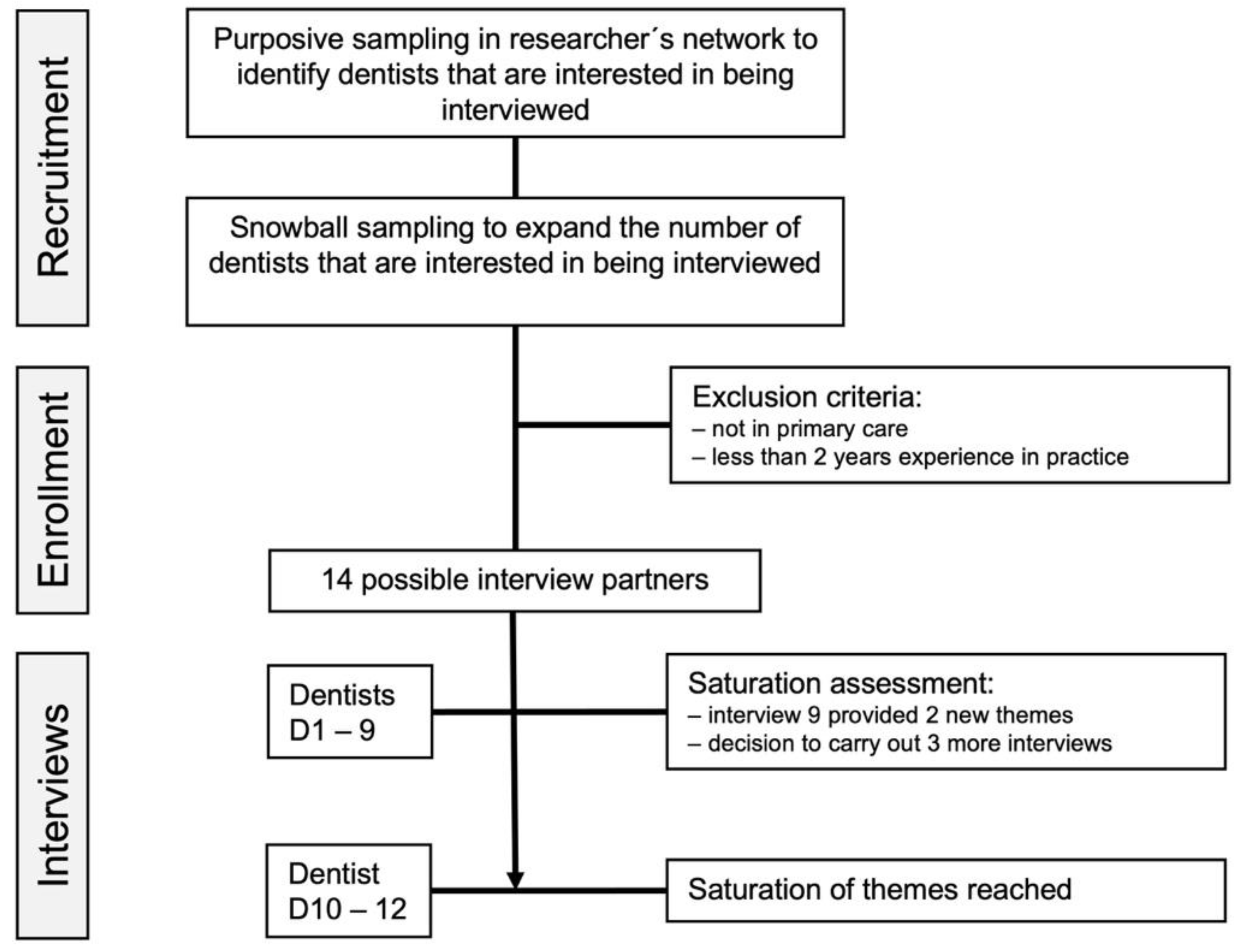
2.4. Sampling Strategy
2.5. Ethical Issues Pertaining to Human Subjects
2.6. Data Collection Methods
2.7. Data Collection Instruments and Technologies
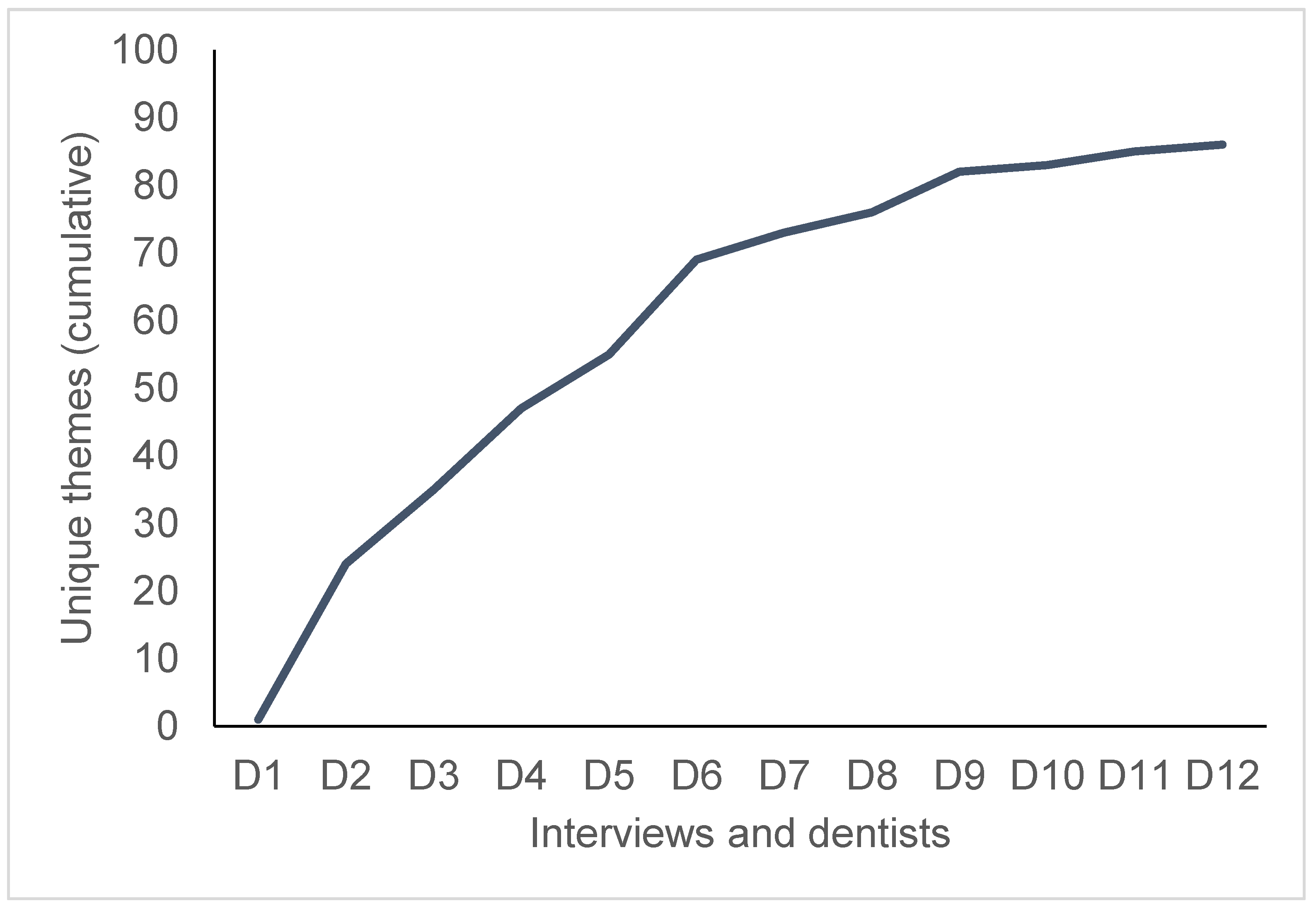
2.8. Data Processing, Data Analysis and Techniques to Enhance Trustworthiness
3. Results
3.1. Knowledge
D5: “Each Dental Association initially talked about something. There were no uniform recommendations from the Federal Dental Association”.
D10: “I would have wished that a Dental Association /, because when I think about older colleagues who do not have PubMed or any contact /, how are they there? A kind of recommendation checklist of the Dental Association, where very clear product recommendations are given /”
D12: “A guideline would have somehow secured you in the event of a COVID-19 infection in practice /, if then somehow a patient calls afterwards and says: ‘Yes, I tested positive and was in your practice last week.’ One would have felt much safer”.
3.2. Availability and Costs
D5: “Right at the beginning, I was not sure whether I could have worked with a normal surgical mask /, yes, but it calms you down when you hear other colleagues who say: ‘Yes, we don’t get anything either. We also do it like that for now, right.’”
D1: “They (concerning regional dental association) wanted to deliver to us too, but that was not possible. They could hardly take care of us”.
D2: “How do I get the things? Why do mouthguards or gloves cost more now than before?”
D3: “Lately I have actually been using masks, but at some point, you simply cannot stem the price”.
D2: “And this lump sum from private patients for increased hygienic standard, of course, only covers a fraction of the expanses. It is only available for private patients and it has been reduced although the prices are rising”.
D5: “For the private patients you can charge a lump sum for increased hygiene costs at least. For the statutory health insurance patients that is not allowed”.
D6: “/ if there are risk patients they will be informed in advance /, but otherwise /, since we were kicked out of the safety parachute /, because we were pushed into the hairdresser’s corner /, we do normal treatment”.
3.3. Applicability of Measures during Treatment
D1: “So I have to be completely honest about that. I just wear the normal surgical face mask and safety glasses of course. When you extract teeth, and you always hit your own rib cage with the face shield /, very difficult. I really have problems to work well with these things”.
D3: “We had face shields, but we do not use them because the glasses simply fog up”.
D7: “We all wear FFP2 masks now and we actually have to take them off every now and then because otherwise we get a headache. We have face shields. Personally, I do not wear them because I still have magnifying glasses. I did that at the beginning, but that is not my thing /. Because the magnifying glasses press completely on my eyes when the face shield is still in front of them. Then I cannot work properly”.
D10: “But I cannot /, I would suffocate if I had to wear a FFP2 mask too. That is why I am only wearing surgical face mask at the moment /, and you can try to look through a face shield with the magnifying glasses”.
3.4. Experience with COVID-19
D2: “So we have already been through quarantine ourselves and we only wear FFP2 masks, right down to the cleaner”.
D6: “People get scared when someone accidentally leaves the treatment room without a mask. I have now noticed that one thing. We have to pay more attention to the fact that the people have to put back on their masks right after the treatment”.
3.5. Impact of COVID-19 on Staff Availability
D4: “We have a Corona-denier in practice. I am an employee and can no longer enforce everything. That is conditioned from the practice owner. In my opinion, she is a little too indulgent”.
D7: “We had an employee who panicked in March and said she wants to quit the job /, because she is afraid of being infected”.
D9: “I think an employee was now on sick leave for 75 days /, easily for risk reasons by her doctor. Another assistant is now depressed, because she could not cope with the psychological stress of being at home”.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| COM-B Domains | TDF Domains | TDF Construct | Reasons (D1–D12) | Quotes | |
|---|---|---|---|---|---|
| Enablers/Facilitators | Capability | Knowledge | Knowledge of |
|
|
| Skills | Ability |
|
| ||
| Opportunity | Environmental Context and Resources | Resources/ Material Resources |
|
| |
| Environmental stressors—Time, Number of Patients |
|
| |||
| Dentist—Team Interaction |
|
| |||
| Motivation | Reinforcement | Consequents |
| ||
| Reward |
| ||||
| Reinforcement |
|
| |||
| Beliefs aboutConsequences | Outcome Expectancies |
|
| ||
| Belief to be save enough |
|
| |||
| Social/ Professional Role and Identity | Professional Identity |
|
| ||
| Identity |
|
| |||
| Emotion | Fear |
|
| ||
| Conflicting | Capability | Knowledge | Knowledge of |
|
|
| Skills | Ability |
|
| ||
| Opportunity | Social Influences | Social Pressure |
|
| |
| Group Conformity |
|
| |||
| Motivation | Social/ Professional Role and Identity | Social Identity |
|
| |
| Identity |
|
| |||
| Beliefs about Capabilities | Self-confidence |
|
| ||
| Reinforcement | Reinforcement |
|
| ||
| Barriers | Capability | Skills | Ability |
|
|
| Knowledge | Knowledge |
|
| ||
| Social Influences | Social Pressure |
|
| ||
| Environmental Context and Resources | Environmental stressor—Time, Patients, Material, Costs, Staff |
|
| ||
| Motivation | Reinforcement | Reinforcement |
|
| |
| Emotion | No Fear |
|
| ||
| Beliefs about Capabilities | Beliefs |
|
| ||
| Beliefs about Consequences | Beliefs |
|
| ||
References
- Kathree, B.A.; Khan, S.B.; Ahmed, R.; Maart, R.; Layloo, N.; Asia-Michaels, W. COVID-19 and its impact in the dental set-ting: A scoping review. PLoS ONE 2020, 15, e0244352. [Google Scholar] [CrossRef]
- Karayürek, F.; Yilmaz Çırakoğlu, N.; Gülses, A.; Ayna, M. Awareness and Knowledge of SARS-CoV-2 Infection among Dental Professionals According to the Turkish National Dental Guidelines. Int. J. Environ. Res. Public Health 2021, 18, 442. [Google Scholar] [CrossRef]
- Bakaeen, L.G.; Masri, R.; AlTarawneh, S.; Garcia, L.T.; AlHadidi, A.; Khamis, A.H.; Hamdan, A.M.; Baqain, Z.H. Dentists’ knowledge, attitudes, and professional behavior toward the COVID-19 pandemic: A multisite survey of dentists’ perspectives. J. Am. Dent. Assoc. 2021, 152, 16–24. [Google Scholar] [CrossRef]
- Shahin, S.Y.; Bugshan, A.S.; Almulhim, K.S.; AlSharief, M.S.; Al-Dulaijan, Y.A.; Siddiqui, I.; Al-Qarni, F.D. Knowledge of dentists, dental auxiliaries, and students regarding the COVID-19 pandemic in Saudi Arabia: A cross-sectional survey. BMC Oral Health 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Wolf, T.G.; Zeyer, O.; Campus, G. COVID-19 in Switzerland and Liechtenstein: A Cross-Sectional Survey among Dentists’ Awareness, Protective Measures and Economic Effects. Int. J. Environ. Res. Public Health 2020, 17, 9051. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, R.M.; AlShali, R.Z.; Bukhary, D.M. Dentists’ Knowledge, Attitudes, and Awareness of Infection Control Measures during COVID-19 Outbreak: A Cross-Sectional Study in Saudi Arabia. Int. J. Environ. Res. Public Health 2020, 17, 9016. [Google Scholar] [CrossRef] [PubMed]
- Widyarman, A.S.; Bachtiar, E.W.; Theodorea, C.F.; Rizal, M.I.; Roeslan, M.O.; Djamil, M.S.; Santosa, D.N.; Bachtiar, B.M. COVID-19 Awareness Among Dental Professionals in Indonesia. Front. Med. 2020, 7, 589759. [Google Scholar] [CrossRef]
- Sah, M.K.; Singh, A.; Sangroula, R.K. Knowledge of novel coronavirus disease (COVID-19) among dental surgeons of Ne-pal: A nationwide study. BMC Infect. Dis. 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Maru, V.; Padawe, D.; Singh, A.; Takate, V.; Dighe, K.; Singh, S. Awareness, Perception, Attitude Regarding CoViD-19 and Infection Control among Indian Pediatric Dentists: A Cross Sectional Study. J. Clin. Pediatr. Dent. 2020, 44, 211–220. [Google Scholar] [CrossRef]
- Nasser, Z.; Fares, Y.; Daoud, R.; Abou-Abbas, L. Assessment of knowledge and practice of dentists towards Coronavirus Disease (COVID-19): A cross-sectional survey from Lebanon. BMC Oral Health 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Arora, S.; Saquib, S.A.; Attar, N.; Pimpale, S.; Zafar, K.S.; Saluja, P.; Abdulla, A.M.; Shamsuddin, S. Evaluation of Knowledge and Preparedness Among Indian Dentists During the Current COVID-19 Pandemic: A Cross-Sectional Study. J. Multidiscip. Health 2020, 13, 841–854. [Google Scholar] [CrossRef]
- Sezgin, G.P.; Şirinoğlu Çapan, B. Assessment of dentists’ awareness and knowledge levels on the Novel Coronavirus (COVID-19). Braz. Oral Res. 2020, 34, 112. [Google Scholar] [CrossRef]
- Singh, K.T.; Mishra, G.; Shukla, A.K.; Behera, S.; Tiwari, A.K.; Panigrahi, S.; Chhabra, K.G. Preparedness among dental professionals towards COVID-19 in India. Pan Afr. Med. J. 2020, 36, 108. [Google Scholar] [CrossRef]
- Al-Khalifa, K.S.; AlSheikh, R.; Al-Swuailem, A.S.; Alkhalifa, M.S.; Al-Johani, M.H.; Al-Moumen, S.A.; Almomen, Z.I. Pandemic preparedness of dentists against coronavirus disease: A Saudi Arabian experience. PLoS ONE 2020, 15, e0237630. [Google Scholar] [CrossRef] [PubMed]
- Shirahmadi, S.; Seyedzadeh-Sabounchi, S.; Khazaei, S.; Bashirian, S.; Miresmæili, A.F.; Bayat, Z.; Houshmand, B.; Semyari, H.; Barati, M.; Jenabi, E.; et al. Fear control and danger control amid COVID-19 dental crisis: Application of the Extended Parallel Process Model. PLoS ONE 2020, 15, e0237490. [Google Scholar] [CrossRef]
- Putrino, A.; Raso, M.; Magazzino, C.; Galluccio, G. Coronavirus (COVID-19) in Italy: Knowledge, management of patients and clinical experience of Italian dentists during the spread of contagion. BMC Oral Health 2020, 20, 1–15. [Google Scholar] [CrossRef]
- Gambhir, R.S.; Dhaliwal, J.S.; Aggarwal, A.; Anand, S.; Anand, V.; Bhangu, A.K. Covid-19: A survey on knowledge, awareness and hygiene practices among dental health professionals in an Indian scenario. Rocz. Państwowego Zakładu Hig. 2020, 71, 223–229. [Google Scholar]
- De Stefani, A.; Bruno, G.; Mutinelli, S.; Gracco, A. COVID-19 Outbreak Perception in Italian Dentists. Int. J. Environ. Res. Public Health 2020, 17, 3867. [Google Scholar] [CrossRef]
- Quadri, M.F.; Jafer, M.A.; Alqahtani, A.S.; Al Mutahar, S.A.; Odabi, N.I.; Daghriri, A.A.; Tadakamadla, S.K. Novel corona virus disease (COVID-19) awareness among the dental interns, dental auxiliaries and dental specialists in Saudi Arabia: A nationwide study. J. Infect. Public Health 2020, 13, 856–864. [Google Scholar] [CrossRef]
- Ahmed, M.A.; Jouhar, R.; Ahmed, N.; Adnan, S.; Aftab, M.; Zafar, M.S.; Khurshid, Z. Fear and Practice Modifications among Dentists to Combat Novel Coronavirus Disease (COVID-19) Outbreak. Int. J. Environ. Res. Public Health 2020, 17, 2821. [Google Scholar] [CrossRef] [PubMed]
- Khader, Y.; Al Nsour, M.; Al-Batayneh, O.B.; Saadeh, R.; Bashier, H.; Alfaqih, M.; Al-Azzam, S.; Alshurman, B.A. Dentists’ Awareness, Perception, and Attitude Regarding COVID-19 and Infection Control: Cross-Sectional Study Among Jordanian Dentists. JMIR Public Health Surveill. 2020, 6, e18798. [Google Scholar] [CrossRef]
- Sandelowski, M. Sample size in qualitative research. Res. Nurs. Health 1995, 18, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, M. Qualitative research methods: Why, when, and how to conduct interviews and focus groups in pharmacy research. Curr. Pharm. Teach. Learn. 2016, 8, 509–516. [Google Scholar] [CrossRef]
- Vasileiou, K.; Barnett, J.; Thorpe, S.; Young, T. Characterising and justifying sample size sufficiency in interview-based studies: Systematic analysis of qualitative health research over a 15-year period. BMC Med. Res. Methodol. 2018, 18, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- French, S.D.; E Green, S.; A O’Connor, D.; E McKenzie, J.; Francis, J.J.; Michie, S.; Buchbinder, R.; Schattner, P.; Spike, N.; Grimshaw, J.M. Developing theory-informed behaviour change interventions to implement evidence into practice: A systematic approach using the Theoretical Domains Framework. Implement. Sci. 2012, 7, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michie, S.; Johnston, M.; Abraham, C.; Lawton, R.; Parker, D.; Walker, A. Making psychological theory useful for implementing evidence based practice: A consensus approach. BMJ Qual. Saf. 2005, 14, 26–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeggle, L.M.; Baker, S.R.; Schwendicke, F. Changing dentists’ carious tissue removal behavior: Qualitative study and behavioral change simulation experiment. J. Dent. 2019, 81, 43–51. [Google Scholar] [CrossRef]
- Schwendicke, F.; Göstemeyer, G. Understanding dentists’ management of deep carious lesions in permanent teeth: A systematic review and meta-analysis. Implement. Sci. 2016, 11, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Templeton, A.R.; Young, L.; Bish, A.; Gnich, W.; Cassie, H.; Treweek, S.; Bonetti, D.; Stirling, D.; Macpherson, L.; McCann, S.; et al. Patient-, organization-, and system-level barriers and facilitators to preventive oral health care: A convergent mixed-methods study in primary dental care. Implement. Sci. 2015, 11, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Gnich, W.; Bonetti, D.; Sherriff, A.; Sharma, S.; Conway, D.I.; Macpherson, L.M. Use of the theoretical domains framework to further understanding of what influences application of fluoride varnish to children’s teeth: A national survey of general dental practitioners in Scotland. Community Dent. Oral Epidemiol. 2015, 43, 272–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, C. Presenting and Evaluating Qualitative Research. Am. J. Pharm. Educ. 2010, 74, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, V.T.; Porcher, R.; Tran, V.C.; Ravaud, P. Predicting data saturation in qualitative surveys with mathematical models from ecological research. J. Clin. Epidemiol. 2017, 82, 71–78. [Google Scholar] [CrossRef]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Mayring, P. Qualitative Inhaltsanalyse: Grundlagen und Techniken; Deutscher Studien Verlag: Weinheim, Germany, 2000. [Google Scholar]
- O´Sullivan, T.A.; Jefferson, C.G. A Review of Strategies for Enhancing Clarity and Reader Accessibility of Qualitative Research Results. Am. J. Pharm. Educ. 2020, 84, 7124. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Krois, J.; Gomez, J. Impact of SARS-CoV2 (Covid-19) on dental practices: Economic analysis. J. Dent. 2020, 99, 103387. [Google Scholar] [CrossRef]




| Dentist (Gender, Age at 10.12.20) | D1 (f, 43y) | D2 (f, 41y) | D3 (m, 60y) | D4 (m, 71y) | D5 (m, 37y) | D6 (m, 48y) | D7 (f, 45y) | D8 (m, 67y) | D9 (m, 35y) | D10 (m, 47y) | D11 (m, 49y) | D12 (f, 28y) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Location of dental surgery (federal state of Germany) | Brandenburg | Baden-Wuerttemberg | North Rhine-Westphalia | Berlin | Rhineland-Palatinate | Lower Saxony | Lower Saxony | Berlin | Berlin | Brandenburg | Brandenburg | Berlin |
| Population of town | 31,000 | 85,524 | 619,294 | 3,762,456 | 18,762 | 3838 | 532,163 | 3,762,456 | 3,762,456 | 13,984 | 1633 | 3,762,456 |
| COVID-19 quick tests available? | Yes | No | No (ordered) | No | Yes | Yes | No | Yes | Yes | No | No | Yes |
| COVID-19 quick test used? | In case of symptoms | n/a | n/a | n/a | In case of symptoms | Regularly | n/a | Regularly | In case of symptoms | In case of symptoms | ||
| COVID-19 + tested staff? | No | Yes | No | No | No | No | No | No | Yes | No | No | No |
| COVID-19 + patients in the past? | No | No | No | No | Yes | Yes | No | No | No | No | No | Yes |
| Staff with high-risk individuals? | No | No | No | Yes | Yes | No | No | Yes | Yes | No | No | n/a |
| Number of patients | Increased | Decreased | Decreased | Unchanged | Decreased | Decreased | Decreased | Decreased | Decreased | Decreased | Unchanged | Decreased |
| Interaction on infection control with colleagues | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes |
| Personal protective equipment (PPE) dentist, staff | ||||||||||||
| Mask (type) between treatments | Surgical face mask | FFP2 | Surgical face mask | No mask (standard) or surgical face mask | FFP2 | Surgical face mask | FFP2 | No mask | FFP2 | Surgical face mask | Surgical face mask | Surgical face mask or FFP2 |
| Mask (type) during treatment; surgical face mask, FFP2 | Surgical face mask (standard) | Not mentioned | Surgical face mask | Surgical face mask | Not mentioned | Not mentioned | Not mentioned | Surgical face mask | Not mentioned | Surgical face mask | Surgical face mask | Not mentioned |
| FFP2 not applicable during treatment | FFP2 | FFP2 is too expansive | FFP2 sometimes | FFP2 | FFP2 | FFP2 | FFP2 is too uncomfortable | FFP2 | FFP2 not applicable during treatment | FFP2 not applicable during treatment | FFP2 | |
| Gloves | Yes (standard) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes, disinfected before use | Yes | Yes | Yes |
| Safety glasses or face shield during treatment | Safety glasses | Safety glasses | Safety glasses | Not mentioned | Not mentioned | Not mentioned | Not mentioned | Not mentioned | Not mentioned | Not mentioned | Not mentioned | Not mentioned |
| Face shield is not applicable during treatments | Face shield is not applicable during treatments | Face shield is not applicable during treatments | Face shield optional | Face shield is not applicable during treatments | Face shield | Face shield is not applicable during treatments | Face shield is too uncomfortable | Face shield optional | Face shield optional | Face shield is not applicable during treatments | Face shield | |
| Protective suit in addition to workwear (during treatment) | No (standard) | No | No | No | No | Yes | No | No | No | No | No | No |
| Different PPE for staff | Not mentioned | Not mentioned | Yes, face shield for prophylaxis | Yes, decided individually | Yes, face shields | No | Yes, face shields | Yes, FFP2 for prophylaxis | No | Yes, FFP2 and surgical face | Not mentioned | No |
| General measures | ||||||||||||
| Social distancing during breaks | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | Yes | No | Not mentioned |
| More frequent surface disinfection | Yes | No | Yes | Not any longer | Yes | Yes, UV-lamps | Yes | Yes | Yes | Yes | Yes | Yes |
| Adequate hand hygiene | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Problems with team members due to COVID-19? | No | No | No | Yes | No | No | Yes | No | Yes | No | No | No |
| Organisation—Appointments (apmt.) and patients | ||||||||||||
| Apmt. for health patients | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Apmt. for emergencies without symptoms of cold | Yes | No | No | No | Yes | Yes | No | Yes | No | Yes | Yes | Not mentioned |
| Apmt. for patients with symptoms of cold | No | No | No | No | No | Yes | No | No | No | No | Yes | No |
| Apmt. for patients from high-risk group | Yes (a lot) | Yes (a lot) | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Not mentioned |
| Apmt. for COVID-19 positive patients | No | No | No | No | No | No | No | No | No | No | Not clear | No |
| Prolonged appointments | No (standard) | Yes | Yes | No | Yes | Yes | No | Yes | Yes | No | No | Yes |
| Hand disinfection (entry/leave) | Yes/optional | Yes/optional | Yes/optional | Yes/optional | Yes/optional | Yes/optional | Yes/optional | Yes/optional | Yes/optional | Yes/optional | Yes/optional | Yes/optional |
| No physical greeting | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Face mask constant (except during treatment) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Inquiry about COVID-19 symptoms | Yes | Yes | Yes | Yes | Yes | Yes | No | No | No | No | No | Yes |
| Temperature measurement | No | No | No | No | No | No | No | No | No | No | No | No |
| Planned patient flow | Yes | Yes | Yes | Sometimes not | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Waiting room | ||||||||||||
| Information signs for safe behavior | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Restricted number of patients and distance | Yes | Yes | Yes | Sometimes not | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Restricted access to toilet | No (standard) | No | No | No | No | Yes | No | No | No | No | No | No |
| Accessoires present (magazines…) | No | No | Magazines | No | No | No | Magazines | Yes | No | No | Yes | Not mentioned |
| Treatment | ||||||||||||
| Different teams | No | No | No | No | No | No | No | No | No | Yes (standard) | n/a (single dentist) | Not mentioned |
| Avoidance of certain treatments | No | No | Yes, x-ray from outside the mouth prefered to avoid coughing | Yes, reduced prophylaxis | No | Yes, reduced prophylaxis | Yes, reduced prophylaxis | Yes, reduced prophylaxis | Yes, no prophylaxis | No | No | No |
| Disinfecting mouthwash | No (H2O2 was tried to use but foam blocked units) | Yes, Cool Mint from Listerine or chlorhexidine digluconate (acc. to recent information, also H2O2 was not orderable) | Yes, H2O2 | Yes, chlorhexidine digluconate (acc. to recent information, previously H2O2) | No (dentist has no information) | No longer (information that chlorhexidine digluconate is ineffective) | Yes, H2O2 | Yes, H2O2 | Yes, H2O2 | Yes, Betaisodona or Cool Mint from Listerine | Yes, chlorhexidine digluconate (standard) | Yes (no further information) |
| Ventilation after every patient | Yes (standard) | Yes | Yes | Yes (standard) | Yes | Yes, also air filter | Yes | Yes | Yes, also air filter | Yes (standard) | Yes (standard) | Yes |
| Aspiration of liquids from mouth | No (standard, patient spits out) | No | Aspiration preferred | No | No | Aspiration prefered | Aspiration (standard) | No | No | Aspiration (standard) | No | No |
| Changing of face protection | After each patient | At start of work | After each patient | Rarely, is often forgotten | Every 4 h | Daily | Daily | Approximately after 5–6 patients | Every 2 h | After each patient | After each patient | Not mentioned |
| Infrastructural measures | No | Plexiglass at reception | Plexiglass at reception | Plexiglass at reception | Plexiglass at reception | Plexiglass at reception | Plexiglass at reception | No | Plexiglass at reception, protective walls | Plexiglass at reception | Plexiglass at reception | Plexiglass at reception |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Müller, A.; Melzow, F.S.; Göstemeyer, G.; Paris, S.; Schwendicke, F. Implementation of COVID-19 Infection Control Measures by German Dentists: A Qualitative Study to Identify Enablers and Barriers. Int. J. Environ. Res. Public Health 2021, 18, 5710. https://doi.org/10.3390/ijerph18115710
Müller A, Melzow FS, Göstemeyer G, Paris S, Schwendicke F. Implementation of COVID-19 Infection Control Measures by German Dentists: A Qualitative Study to Identify Enablers and Barriers. International Journal of Environmental Research and Public Health. 2021; 18(11):5710. https://doi.org/10.3390/ijerph18115710
Chicago/Turabian StyleMüller, Anne, Florentina Sophie Melzow, Gerd Göstemeyer, Sebastian Paris, and Falk Schwendicke. 2021. "Implementation of COVID-19 Infection Control Measures by German Dentists: A Qualitative Study to Identify Enablers and Barriers" International Journal of Environmental Research and Public Health 18, no. 11: 5710. https://doi.org/10.3390/ijerph18115710