The Emergence of a Sustainable Tobacco Treatment Program across the Cancer Care Continuum: A Systems Approach for Implementation at the University of California Davis Comprehensive Cancer Center


Abstract
:1. Introduction
2. Materials and Methods
2.1. UCD Stakeholders Involved in Implementation and Evaluation
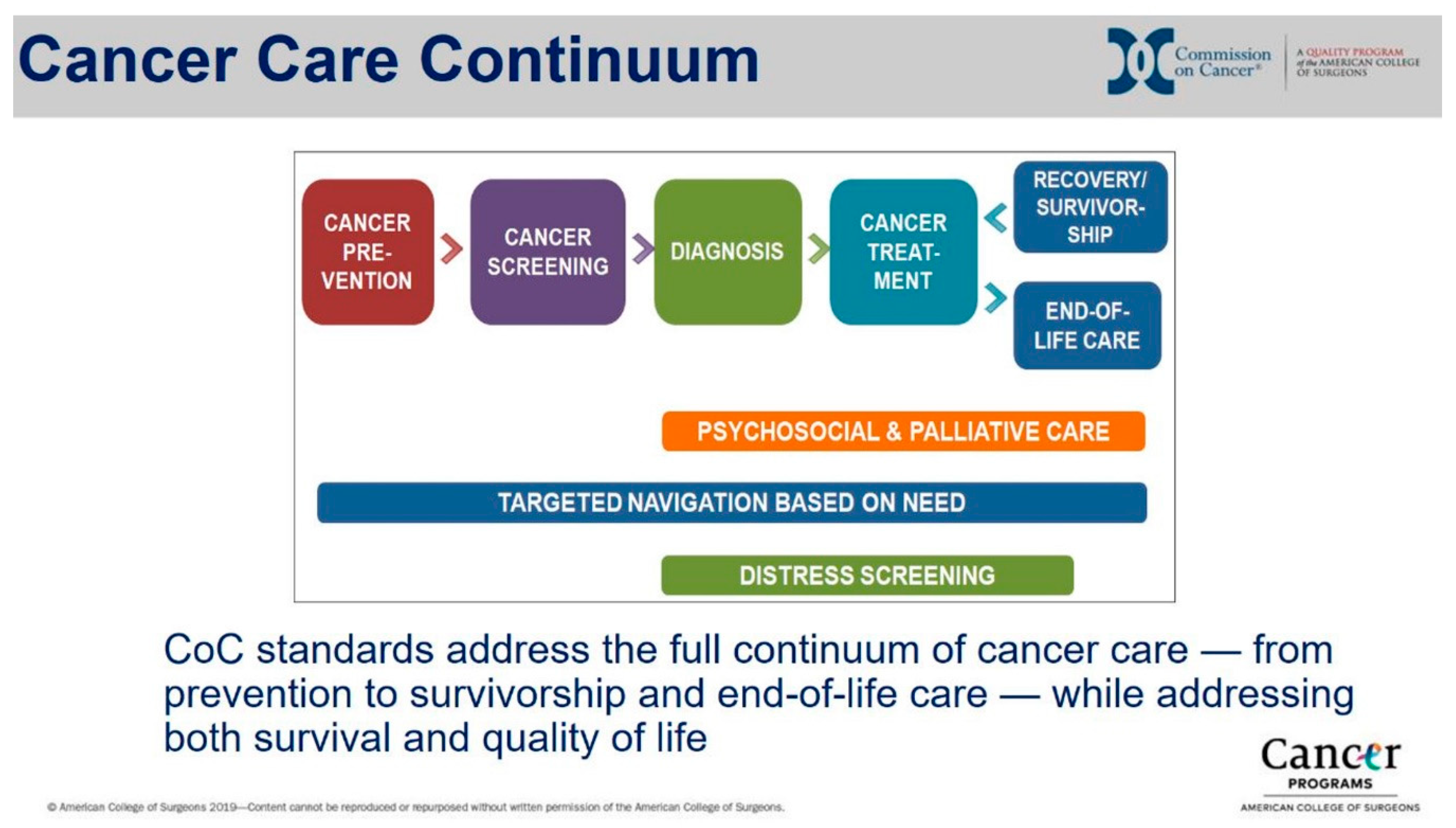
2.2. The Cancer Care Continuum as a Systems Framework
2.3. Constructs from an Implementation Research Framework
2.4. Analysis
3. Results
3.1. Characteristics of the Intervention: Referral to Quitline or UCD Group Class
3.2. Outer Setting: Motivational Drivers for the Health System
3.3. Inner Setting: Implementation Readiness across the Domains of the Cancer Care Continuum
3.3.1. Prevention: Primary Care and Other Settings
3.3.2. Screening: Lung Cancer Screening as a Model
3.3.3. Diagnosis: From Various Settings into Cancer Clinics
3.3.4. Treatment: Cancer Clinic or Hospital Services
3.3.5. Survivorship: Supportive Oncology
3.4. Implementation Process in the Treatment Domain
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cinciripini, P.M.; Karam-Hage, M.; Kypriotakis, G.; Robinson, J.D.; Rabius, V.; Beneventi, D.; Minnix, J.A.; Blalock, J.A. Association of a Comprehensive Smoking Cessation Program With Smoking Abstinence Among Patients With Cancer. JAMA Netw. Open 2019, 2, e1912251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- US Department of Health and Human Services. The Health Consequences of Smoking: 50 Years of Progress: A Report of the Surgeon General; US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2014.
- Fukui, M.; Suzuki, K.; Matsunaga, T.; Oh, S.; Takamochi, K. Importance of Smoking Cessation on Surgical Outcome in Primary Lung Cancer. Ann. Thorac. Surg. 2019, 107, 1005–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, A.O.; Ripley-Moffitt, C.E.; Pathman, D.E.; Patsakham, K.M. Tobacco use treatment at the U.S. National Cancer Institute’s designated Cancer Centers. Nicotine. Tob. Res. 2013, 15, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Sarna, L.; Bialous, S.A. Implementation of Tobacco Dependence Treatment Programs in Oncology Settings. Semin. Oncol. Nurs. 2016, 32, 187–196. [Google Scholar] [CrossRef]
- Schroeder, S.A. An update about tobacco and cancer: What clinicians should know. J. Cancer Educ. 2012, 27, 5–10. [Google Scholar] [CrossRef]
- Morgan, G.; Schnoll, R.A.; Alfano, C.M.; Evans, S.E.; Goldstein, A.; Ostroff, J.; Park, E.R.; Sarna, L.; Cox, L.S. National cancer institute conference on treating tobacco dependence at cancer centers. J. Oncol. Pract. 2011, 7, 178–182. [Google Scholar] [CrossRef]
- Croyle, R.T.; Morgan, G.D.; Fiore, M.C. Addressing a Core Gap in Cancer Care - The NCI Moonshot Program to Help Oncology Patients Stop Smoking. N. Engl. J. Med. 2019, 380, 512–515. [Google Scholar] [CrossRef]
- Hood-Medland, E.A.; Stewart, S.L.; Nguyen, H.; Avdalovic, M.; MacDonald, S.; Zhu, S.H.; Mayoral, A.; Tong, E.K. Health System Implementation of a Tobacco Quitline eReferral. Appl. Clin. Inform. 2019, 10, 735–742. [Google Scholar] [CrossRef]
- California Dialogue On Cancer (CDOC) Tobacco Stakeholder Advisory Group. Tobacco Cessation in Cancer Prevention and Treatment: A Call to Action for California Cancer Centers; California Department of Public Health: Sacramento, CA, USA, 2015.
- National Academy of Sciences Engineering and Medicine. Delivering High-Quality Cancer Care: Charting a New Course for a System in Crisis; National Academies Press: Washington, DC, USA, 2013. [Google Scholar]
- U.S. Department of Health and Human Services. Smoking Cessation; U.S. Department of Health and Human Services, Centers for Disease Control and PRevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2020.
- De Koning, H.J.; van der Aalst, C.M.; de Jong, P.A.; Scholten, E.T.; Nackaerts, K.; Heuvelmans, M.A.; Lammers, J.J.; Weenink, C.; Yousaf-Khan, U.; Horeweg, N.; et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N. Engl. J. Med. 2020, 382, 503–513. [Google Scholar] [CrossRef]
- Church, T.R.; Black, W.C.; Aberle, D.R.; Berg, C.D.; Clingan, K.L.; Duan, F.; Fagerstrom, R.M.; Gareen, I.F.; Gierada, D.S.; Jones, G.C.; et al. Results of initial low-dose computed tomographic screening for lung cancer. N. Engl. J. Med. 2013, 368, 1980–1991. [Google Scholar] [CrossRef] [Green Version]
- American Lung Association. State of Lung Cancer; American Lung Association: Chicago, IL, USA, 2019. [Google Scholar]
- Bassett, J.C.; Gore, J.L.; Chi, A.C.; Kwan, L.; McCarthy, W.; Chamie, K.; Saigal, C.S. Impact of a bladder cancer diagnosis on smoking behavior. J. Clin. Oncol. 2012, 30, 1871–1878. [Google Scholar] [CrossRef] [PubMed]
- Funk-Lawler, R.; Mundey, K.R. Understanding Distress Among Patients With Cancer Receiving Specialized, Supportive Care Services. Am. J. Hosp. Palliat. Care 2020, 1049909120905780. [Google Scholar] [CrossRef] [PubMed]
- Karam-Hage, M.; Oughli, H.A.; Rabius, V.; Beneventi, D.; Wippold, R.C.; Blalock, J.A.; Cinciripini, P.M. Tobacco Cessation Treatment Pathways for Patients With Cancer: 10 Years in the Making. J. Natl. Compr. Cancer Netw. 2016, 14, 1469–1477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanchard, C.M.; Courneya, K.S.; Stein, K.; SCS-II, A.C.S.s. Cancer survivors’ adherence to lifestyle behavior recommendations and associations with health-related quality of life: Results from the American Cancer Society’s SCS-II. J. Clin. Oncol. 2008, 26, 2198–2204. [Google Scholar] [CrossRef]
- Karam-Hage, M.; Cinciripini, P.M.; Gritz, E.R. Tobacco use and cessation for cancer survivors: An overview for clinicians. CA Cancer J. Clin. 2014, 64, 272–290. [Google Scholar] [CrossRef] [Green Version]
- Birken, S.A.; Powerll, B.J.; Presseau, J.; Kirk, M.A.; Lorencatto, F.; Gould, N.J.; Shea, C.M.; Weiner, B.J.; Francis, J.J.; Yu, Y.; et al. Combined use of the consolidated framework for implementation research (CFIR) and the theorhetical domains framework (TDF): A systematic review. Implement. Sci. 2017, 12. [Google Scholar] [CrossRef] [Green Version]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef] [Green Version]
- Denizen, N.; Lincoln, Y. The Sage Handbook of Qualitative Research, 4th ed.; Sage Publications: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- Mustoe, M.; Clark, J.; Huynh, T.; Tong, E.; Wolf, T.; Brown, L.; Cooke, D. Surgery and Population Health: Engagement and Effectiveness of a Smoking Cessation Quitline Intervention in a Thoracic Surgery Clinic. JAMA Surgery 2020, in press. [Google Scholar]
- Kaslow, A.A.; Romano, P.S.; Schwarz, E.; Shaikh, U.; Tong, E.K. Building and Scaling-up California Quits: Supporting Health Systems Change for Tobacco Treatment. Am. J. Prev. Med. 2018, 55, S214–S221. [Google Scholar] [CrossRef]
- Commission on Cancer. Optimal Resources for Cancer Care: 2020 Standards; American College of Surgeons: Chicago, IL, USA, 2019. [Google Scholar]
- Nekhlyudov, L.; Levit, L.; Hurria, A.; Ganz, P.A. Patient-centered, evidence-based, and cost-conscious cancer care across the continuum: Translating the Institute of Medicine report into clinical practice. CA Cancer J. Clin. 2014, 64, 408–421. [Google Scholar] [CrossRef]
- Land, S.R.; Warren, G.W.; Crafts, J.L.; Hatsukami, D.K.; Ostroff, J.S.; Willis, G.B.; Chollette, V.Y.; Mitchell, S.A.; Folz, J.N.; Gulley, J.L.; et al. Cognitive testing of tobacco use items for administration to patients with cancer and cancer survivors in clinical research. Cancer 2016, 122, 1728–1734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Land, S.R.; Toll, B.A.; Moinpour, C.M.; Mitchell, S.A.; Ostroff, J.S.; Hatsukami, D.K.; Duffy, S.A.; Gritz, E.R.; Rigotti, N.A.; Brandon, T.H.; et al. Research Priorities, Measures, and Recommendations for Assessment of Tobacco Use in Clinical Cancer Research. Clin. Cancer Res. 2016, 22, 1907–1913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamal, A.H.; Krzyzanowska, M.K. Real-World Approaches to Quality Improvement in Oncology. J. Clin. Oncol. Pract. 2018. [Google Scholar] [CrossRef] [PubMed]
- Warren, G.W.; Dibaj, S.; Hutson, A.; Cummings, K.M.; Dresler, C.; Marshall, J.R. Identifying Targeted Strategies to Improve Smoking Cessation Support for Cancer Patients. J. Thorac. Oncol. 2015, 10, 1532–1537. [Google Scholar] [CrossRef] [Green Version]
- Acquavita, S.P. How social work can address the tobacco epidemic. J. Soc. Work Pract. Addict. 2020, 20, 82–87. [Google Scholar] [CrossRef]
- Schwindt, R.; McNelis, A.M.; Agley, J.; Hudmon, K.S.; Lay, K.; Wilgenbusch, B. Training future clinicians: An interprofessional approach to treating tobacco use and dependence. J. Interprofessional Care 2019, 33, 200–208. [Google Scholar] [CrossRef]
- Notier, A.E.; Hager, P.; Brown, K.S.; Petersen, L.; Bedard, L.; Warren, G.W. Using a Quitline to Deliver Opt-Out Smoking Cessation for Cancer Patients. JCO Oncol. Pract. 2020. [Google Scholar] [CrossRef]
- U.S. National Cancer Institute. A Socioecological Approach to Addressing Tobacco-Related Health Disparities; U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute: Bethesda, MD, USA, 2017.


{kind=link}
| Readiness Subconstruct | Factor Addressed | Prevention | Screening | Diagnosis | Treatment | Survivorship |
|---|---|---|---|---|---|---|
| Leadership Engagement: Barriers | Administrative level | Variable coordination with county or state health departments | Variable coordination with external community health systems and insurance plans | Cancer clinic operations report to the hospital and not to ambulatory care operations | Cancer pharmacy has limited staffing to support furnishing and counseling for nicotine replacement medication | Commitment priorities are for providing clinical services to specific populations |
| Department or clinic level | Multiple leaders across primary and specialty care services | Multiple leaders across primary and specialty care services | Multiple leaders across hospital-based teams, primary care (especially external) and oncology services | Some departments have clinics and leadership external to cancer clinics | ||
| Leadership Engagement: Facilitators | Administrative level | Executive leadership support for program and tobacco quality metrics UCD CCC Office of Community Outreach and Engagement support | Leadership support (ambulatory care, population health) for Lung Cancer Screening (LCS) program | Cancer Center Director, Physician-in-Chief, and Executive Director of oncology services support program activities | ||
| Department or clinic level | Ambulatory Care Nursing and Medical Directors support workflow/IT changes | LCS committee chair includes tobacco treatment program staff | Hospital-based pharmacy faculty incorporate student learners to assist some patients for tobacco treatment | Cancer Committee adopted tobacco treatment quality improvement as a programmatic goal Clinic supervisors engaged with supporting program | Supportive Oncology and Survivorship Director includes tobacco treatment program staff | |
| Available Resources: Barriers | Money | Insufficient funding for TTS in every clinic | Insufficient funds for dedicated nurse practitioner to manage a LCS clinic that could include tobacco treatment | External primary care clinics may not have funds for TTS | Insufficient funding for TTS in every department or clinic | Limited funding for hiring additional staff for substance use or tobacco treatment while addressing psychological distress |
| Training or education | Tobacco treatment not part of annual provider training | Cancer screening not part of annual provider training | External primary care clinics referring new cancer patients may not have tobacco treatment workflow | |||
| Physical space | HME group class rotates across different clinic sites every month. | LCS has only 1-2 clinic sites for PCP referrals | Limited cancer clinic space for classes | Limited space for additional staff | ||
| Time | Primary care has competing priorities to conduct LCS | Staff processing new patient referrals have limited time | Limited cancer clinic staff time for interventions | Limited time for Supportive Oncology and Survivorship staff for interventions | ||
| Available Resources: Facilitators | Money | Free state quitline services | Ambulatory care support for LCS program | Health system leadership commits resources to sustain tobacco treatment program | ||
| Training or education | Staff training for tobacco treatment in oncology | Online provider training video for LCS referrals | Staff training for tobacco treatment in oncology | Medical assistant training on assessment | ||
| Physical space | HME conducts online group class | Cancer pharmacy in cancer clinic building | Nurse program manager co-located with Supportive Oncology and Survivorship | |||
| Time | Public Affairs and marketing staff promote program | |||||
| Access to Information and Knowledge: Barriers | Workflow in clinical setting | Communication gap between rooming assessment and provider social history | Tobacco treatment not mandated in cancer screening, except for LCS External referrals for LCS depends on contractual arrangements | New patient referral workflow processing paperwork does not make referrals to tobacco treatment Medical assistants initially not required to assess tobacco status | Providers document tobacco in notes instead of the EMR Tobacco History Data analytics challenging with IT report teams for research, clinical operations, quality improvement Hospital cancer patients on different clinical services | No routine review of tobacco assessment or referrals with patient outreach Supportive care screening questionnaire includes self-reported substance use but not tobacco |
| Information technology | Referring health systems may not have tobacco treatment tracking and referral systems | EMR tobacco history section challenging to identify LCS eligibility accurately | New cancer patient questionnaire not entered into EMR Tobacco History | Cancer pharmacy and radiation oncology utilize different electronic systems | Delays in production for population registries | |
| Training or education | Brief provider/clinic staff meetings | No ongoing training | Brief provider/clinic meetings or huddles | |||
| Access to Information and Knowledge:Facilitators | Workflow in clinical setting | Primary care workflow for tobacco treatment. HME uses workbench reports for outreach | Tobacco treatment program collaborating on outreach to eligible patients | Hospital teams or UCD primary care may already assess or refer | Medical assistants assess and refer patients. Cancer pharmacy affiliated with outpatient pharmacy | Interprofessional team helps to refer. Navigators added tobacco to survivorship care plans |
| Information technology | EMR Health Maintenance Alert, tobacco treatment orders, tobacco registry | EMR Health Maintenance alert for LCS has link to order | Cancer Patient Tobacco Use Questionnaire; tobacco registry for oncology patients (pending) | |||
| Training or education | Pre-Visit Planners in UCD primary care clinics | Medical assistants and nurses trained on referrals | Supportive oncology team trained on referrals |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tong, E.K.; Wolf, T.; Cooke, D.T.; Fairman, N.; Chen, M.S., Jr. The Emergence of a Sustainable Tobacco Treatment Program across the Cancer Care Continuum: A Systems Approach for Implementation at the University of California Davis Comprehensive Cancer Center. Int. J. Environ. Res. Public Health 2020, 17, 3241. https://doi.org/10.3390/ijerph17093241
Tong EK, Wolf T, Cooke DT, Fairman N, Chen MS Jr. The Emergence of a Sustainable Tobacco Treatment Program across the Cancer Care Continuum: A Systems Approach for Implementation at the University of California Davis Comprehensive Cancer Center. International Journal of Environmental Research and Public Health. 2020; 17(9):3241. https://doi.org/10.3390/ijerph17093241
Chicago/Turabian StyleTong, Elisa K., Terri Wolf, David T. Cooke, Nathan Fairman, and Moon S. Chen, Jr. 2020. "The Emergence of a Sustainable Tobacco Treatment Program across the Cancer Care Continuum: A Systems Approach for Implementation at the University of California Davis Comprehensive Cancer Center" International Journal of Environmental Research and Public Health 17, no. 9: 3241. https://doi.org/10.3390/ijerph17093241