Living with Chronic Heart Failure: Exploring Patient, Informal Caregiver, and Healthcare Professional Perceptions

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Ethical Considerations
2.4. Analysis of Data
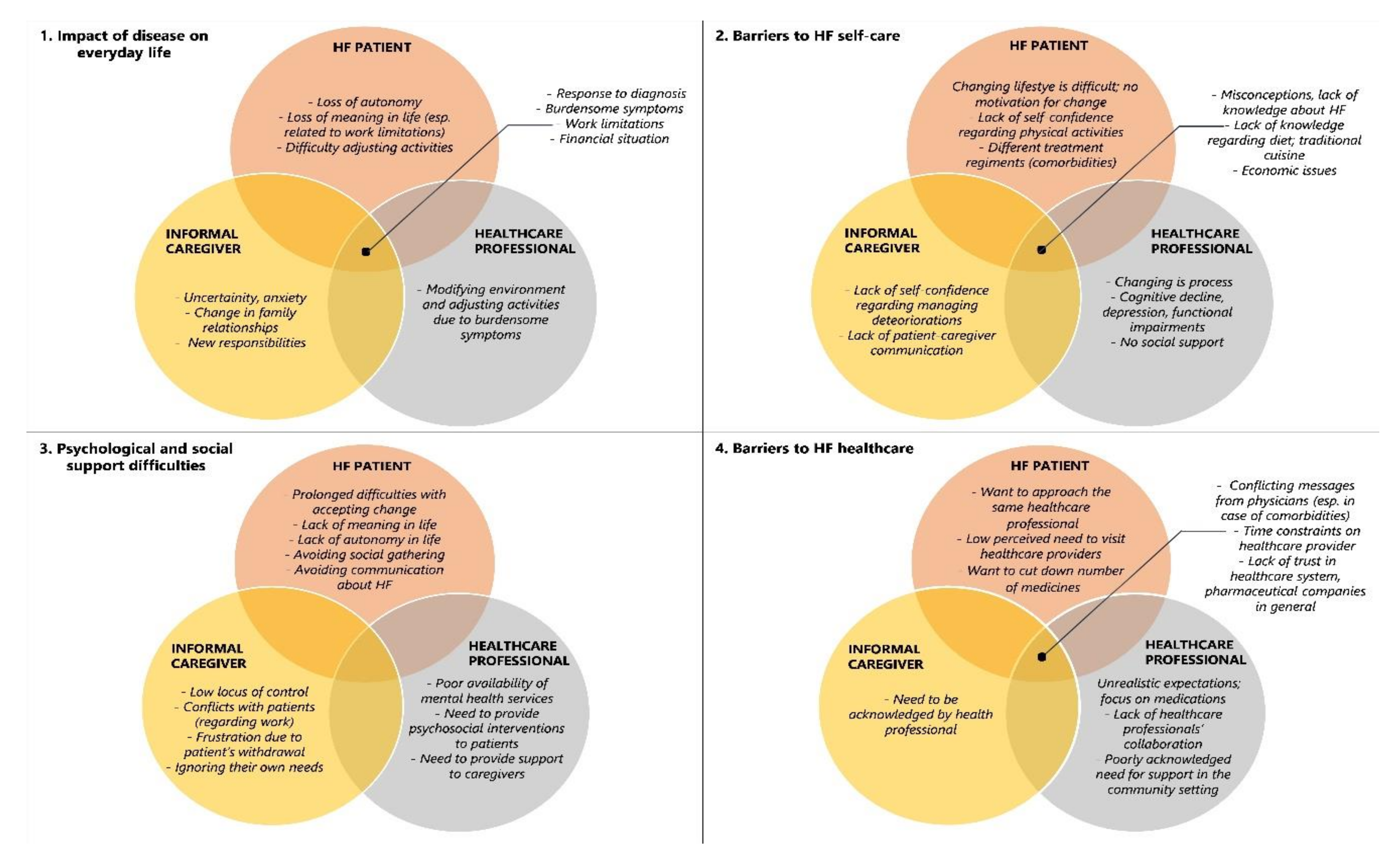
3. Results
3.1. Impact of HF on Everyday Life
3.2. Barriers to HF Self-Care
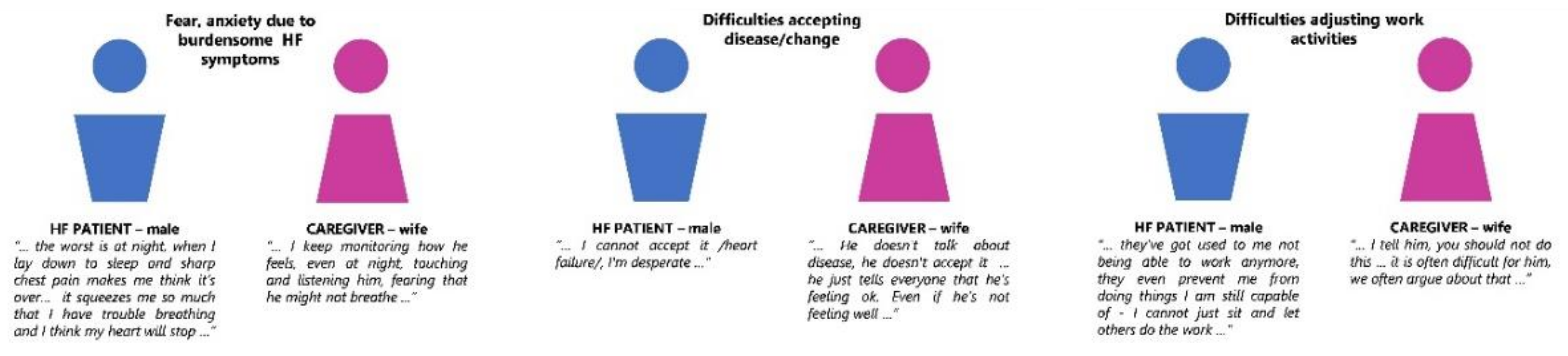
3.3. Psychological and Social Support Difficulties
3.4. Barriers to Effective Healthcare in HF Clinic
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Categories | Subcategories |
|---|---|
| 1. Impact of disease on everyday life | |
| Immediate response to diagnosis | –Shock |
| –Denial | |
| –Anger | |
| –Sadness | |
| –Fear, anxiety | |
| Burdensome symptoms | –Fatigue |
| –Shortness of breath | |
| –Swelling | |
| –Weight gain | |
| –Lack of appetite | |
| Limitations | -Physical |
| –Work-inability to continue with job | |
| –Work-inability to continue with domestic work, farming | |
| Quality of life | –Loss of autonomy |
| –Loss of meaning | |
| –Uncertainty, anxiety | |
| –Social isolation | |
| Change in lifestyle | –Modifying environment |
| –Adjusting activities | |
| –Change in family relationships | |
| –Change in work-family balance | |
| –New responsibilities | |
| Financial situation | –Lower income |
| –More expenses | |
| 2. Barriers to self-care | |
| Self-care skills | –Medication taking–low |
| –Self-monitoring–low | |
| –Adherence to recommendations - low | |
| Knowledge | –Misconceptions about heart failure |
| –Lack of knowledge–heart failure in general | |
| –Lack of knowledge–self-care recommendations | |
| Motivation | –No motivation |
| –Change is difficult | |
| –Change is a process | |
| Self-confidence | –Physical activity |
| –Managing deterioration | |
| Comorbidities | –Different treatment regiments |
| –Functional impairments | |
| –Cognitive decline | |
| –Depression | |
| Social support | –No social support |
| –Lack of patient-caregiver communication | |
| Social context | –Traditional cuisine |
| –Social pressure | |
| Economic issues | –Extra cost–food |
| –Extra cost–devices–Extra cost–transportation | |
| 3. Psychological, social support difficulties | |
| Psychological difficulties | –Prolonged experience of psychological distress |
| –Prolonged difficulties with accepting change | |
| –Lack of meaning in life | |
| –Lack of autonomy | |
| –Low locus of control | |
| –Ignoring own needs | |
| Social/relationship difficulties | –Avoiding social gatherings |
| –Avoiding communication about heart failure | |
| –Conflicts | |
| –Lack of emotional support | |
| Need for organized psychosocial interventions | –Mental health services to chronic patients in hospitals |
| –Psychosocial interventions for heart failure patients | |
| –Psychosocial interventions for informal caregivers | |
| 4. Received healthcare in outpatient heart failure clinic | |
| Satisfaction with received healthcare | –Obtained knowledge–low |
| –Obtained self-care skills–low | |
| Organizational issues | –Conflicting messages from different specialists |
| –Lack of collaboration between different healthcare professionals | |
| –Time constraints | |
| –Not being able to approach the same healthcare professional | |
| Attitudes towards healthcare | –Lack of trust–healthcare |
| –Lack of trust–pharmaceutical companies | |
| –Low perceived need to visit healthcare professionals | |
| –Unrealistic expectations | |
| Need for supportive environment in heart failure management | –Lack of (interpersonal) skills by healthcare professionals |
| –Lack of resources by healthcare professionals | |
| –Need for inclusion of informal caregivers in healthcare | |
| –Need for support in the community setting | |
| Categories | Frequencies * | ||
|---|---|---|---|
| Patients | Informal Caregivers | Healthcare Professionals | |
| 1. Impact of disease on everyday life | |||
| Immediate response to diagnosis | [6/32] | [12/21] | [3/5] |
| Burdensome symptoms | [25/32] | [5/21] | [5/5] |
| Limitations | [23/32] | [5/21] | [5/5] |
| Quality of life | [11/32] | [15/21] | [3/5] |
| Change in lifestyle | [23/32] | [20/21] | [5/5] |
| Financial situation | [7/32] | [6/21] | [5/5] |
| 2. Barriers to self-care | |||
| Self-care skills | [6/32] | [9/21] | [5/5] |
| Knowledge | [5/32] | [4/21] | [4/5] |
| Motivation | [19/32] | [6/21] | [5/5] |
| Self-confidence | [6/32] | [6/21] | [2/5] |
| Comorbidities | [14/32] | [4/21] | [5/5] |
| Social support | [2/32] | [6/21] | [2/5] |
| Social context | [12/32] | [7/21] | [5/5] |
| Economic issues | [8/32] | [4/21] | [5/5] |
| 3. Psychological, social support difficulties | |||
| Psychological difficulties | [22/32] | [11/21] | [3/5] |
| Social/relationship difficulties | [11/32] | [13/21] | [3/5] |
| Need for organized psychosocial interventions | [0/32] | [0/21] | [5/5] |
| 4. Received healthcare in outpatient heart failure clinic | |||
| Satisfaction with received healthcare | [13/32] | [6/21] | [2/5] |
| Organizational issues | [5/32] | [2/21] | [5/5] |
| Attitudes towards healthcare | [7/32] | [3/21] | [4/5] |
| Need for supportive environment in heart failure management | [5/32] | [4/21] | [5/5] |
References
- Bui, A.L.; Horwich, T.B.; Fonarow, G.C. Epidemiology and risk profile of heart failure. Nat. Rev. Cardiol. 2010, 8, 30–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Riet, E.E.; Hoes, A.W.; Wagenaar, K.P.; Limburg, A.; Landman, M.J.; Rutten, F.H. Epidemiology of heart failure: The prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur. J. Hear. Fail. 2016, 18, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.S.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. Guidelines for the diagnosis and treatment of acute and chronic heart failure The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- Omersa, D.; Farkas, J.; Erzen, I.; Lainscak, M. National trends in heart failure hospitalization rates in Slovenia 2004–2012. Eur. J. Hear. Fail. 2018, 20, 1321–1328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambrosy, A.P.; Fonarow, G.C.; Butler, J.; Chioncel, O.; Greene, S.J.; Vaduganathan, M.; Nodari, S.; Lam, C.S.; Sato, N.; Shah, A.N.; et al. The Global Health and Economic Burden of Hospitalizations for Heart Failure. J. Am. Coll. Cardiol. 2014, 63, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Kessing, D.; Denollet, J.; Widdershoven, J.; Kupper, N. Self-care and health-related quality of life in chronic heart failure: A longitudinal analysis. Eur. J. Cardiovasc. Nurs. 2017, 16, 605–613. [Google Scholar] [CrossRef] [Green Version]
- Bekelman, D.B.; Havranek, E.P.; Becker, D.M.; Kutner, J.S.; Peterson, P.N.; Wittstein, I.S.; Gottlieb, S.H.; Yamashita, T.E.; Fairclough, D.L.; Dy, S.M. Symptoms, depression, and quality of life in patients with heart failure. J. Card. Fail. 2007, 13, 643–648. [Google Scholar] [CrossRef]
- Yu, D.S.F.; Lee, T.F.D.; Kwong, A.N.; Thompson, D.R.; Woo, J. Living with chronic heart failure: A review of qualitative studies of older people. J. Adv. Nurs. 2008, 61, 474–483. [Google Scholar] [CrossRef]
- Lainscak, M.; Blue, L.; Clark, A.; Dahlström, U.; Dickstein, K.; Ekman, I.; McDonagh, T.; McMurray, J.J.; Ryder, M.; Stewart, S.; et al. Self-care management of heart failure: Practical recommendations from the Patient Care Committee of the Heart Failure Association of the European Society of Cardiology. Eur. J. Hear. Fail. 2011, 13, 115–126. [Google Scholar] [CrossRef] [Green Version]
- Sedlar, N.; Lainscak, M.; Mårtensson, J.; Strömberg, A.; Jaarsma, T.; Farkas, J. Factors related to self-care behaviours in heart failure: A systematic review of European Heart Failure Self-Care Behaviour Scale studies. Eur. J. Cardiovasc. Nurs. 2017, 16, 272–282. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, M.D. The new subjective medicine: Taking the patient’s point of view on health care and health. Soc. Sci. Med. 2003, 56, 1595–1604. [Google Scholar] [CrossRef]
- Ekman, I.; Wolf, A.; Olsson, L.-E.; Taft, C.; Dudas, K.; Schaufelberger, M.; Swedberg, K. Effects of person-centred care in patients with chronic heart failure: The PCC-HF study. Eur. Hear. J. 2011, 33, 1112–1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, M. Why Is U.S. Poverty Higher in Nonmetropolitan than in Metropolitan Areas? Growth Chang. 2007, 38, 56–76. [Google Scholar] [CrossRef]
- Kociol, R.; Greiner, M.A.; Fonarow, G.C.; Hammill, B.G.; Heidenreich, P.A.; Yancy, C.W.; Peterson, E.D.; Curtis, L.H.; Hernandez, A.F. Associations of Patient Demographic Characteristics and Regional Physician Density With Early Physician Follow-Up Among Medicare Beneficiaries Hospitalized With Heart Failure. Am. J. Cardiol. 2011, 108, 985–991. [Google Scholar] [CrossRef]
- Eberhardt, M.S.; Pamuk, E.R. The Importance of Place of Residence: Examining Health in Rural and Nonrural Areas. Am. J. Public Health 2004, 94, 1682–1686. [Google Scholar] [CrossRef]
- Weber, B.; Jensen, L.; Miller, K.; Mosley, J.; Fisher, M. A Critical Review of Rural Poverty Literature: Is There Truly a Rural Effect? Int. Reg. Sci. Rev. 2005, 28, 381–414. [Google Scholar] [CrossRef]
- Dracup, K.; Moser, D.K.; Pelter, M.M.; Nesbitt, T.; Southard, J.; Paul, S.M.; Robinson, S.; Zegre-Hemsey, J.; Cooper, L. Rural patients’ knowledge about heart failure. J. Cardiovasc. Nurs. 2013, 29, 423–428. [Google Scholar] [CrossRef] [Green Version]
- Clark, A.M.; Thompson, D.R. What heart failure programme works best? Wrong question, wrong assumptions. Eur. J. Hear. Fail. 2010, 12, 1271–1273. [Google Scholar] [CrossRef]
- Coats, A.J. Ageing, demographics, and heart failure. Eur. Hear. J. Suppl. 2019, 21, L4–L7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riegel, B.; Carlson, B. Facilitators and barriers to heart failure self-care. Patient Educ. Couns. 2002, 46, 287–295. [Google Scholar] [CrossRef]
- Gusdal, A.K.; Josefsson, K.; Adolfsson, E.T.; Martin, L. Informal Caregivers’ Experiences and Needs When Caring for a Relative with Heart Failure. J. Cardiovasc. Nurs. 2016, 31, 1. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, B.M.; Jaligam, V.; Conish, B.K.; Johnson, W.D.; Melancon, B.; Katzmarzyk, P.T. Exploring Patient, Caregiver, and Healthcare Provider Perceptions of Caring for Patients With Heart Failure: What Are the Implications? Ochsner J. 2017, 17, 93–102. [Google Scholar] [PubMed]
- Granger, B.B.; Sandelowski, M.; Tahshjain, H.; Swedberg, K.; Ekman, I. A Qualitative Descriptive Study of the Work of Adherence to a Chronic Heart Failure Regimen. J. Cardiovasc. Nurs. 2009, 24, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Jamshed, S. Qualitative research method-interviewing and observation. J. Basic Clin. Pharm. 2014, 5, 87–88. [Google Scholar] [CrossRef] [Green Version]
- Miles, M.; Huberman, A. Qualitative Data Analysis: An Expanded Sourcebook, 2nd ed.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Patton, M. Qualitative Research and Evaluation Methods, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2002. [Google Scholar]
- Zhang, Y.; Wildemuth, B.M. Qualitative analysis of content. In Applications of Social Research Methods to Questions in Information and Library Science; Wildemuth, B., Ed.; Libraries Unlimited: Westport, CT, USA, 2009; pp. 308–319. [Google Scholar]
- Trivedi, R.B.; Slightam, C.; Nevedal, A.; Guetterman, T.C.; Fan, V.S.; Nelson, K.M.; Rosland, A.-M.; Heidenreich, P.A.; Timko, C.; Asch, S.M.; et al. Comparing the Barriers and Facilitators of Heart Failure Management as Perceived by Patients, Caregivers, and Clinical Providers. J. Cardiovasc. Nurs. 2019, 34, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Hooker, S.A.; Schmiege, S.J.; Trivedi, R.B.; Amoyal, N.R.; Bekelman, D.B. Mutuality and heart failure self-care in patients and their informal caregivers. Eur. J. Cardiovasc. Nurs. 2017, 17, 102–113. [Google Scholar] [CrossRef]
- Retrum, J.H.; Nowels, C.T.; Bekelman, D.B. Patient and Caregiver Congruence. J. Cardiovasc. Nurs. 2013, 28, 129–136. [Google Scholar] [CrossRef]
- Hupcey, J.; Fenstermacher, K.; Kitko, L.; Penrod, J. Achieving medical stability: Wives’ experiences with heart failure. Clin. Nurs. Res. 2010, 19, 211–229. [Google Scholar] [CrossRef]
- Clark, A.M.; Freydberg, C.N.; McAlister, F.A.; Tsuyuki, R.T.; Armstrong, P.W.; Strain, L.A. Patient and informal caregivers’ knowledge of heart failure: Necessary but insufficient for effective self-care. Eur. J. Hear. Fail. 2009, 11, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Jeon, Y.-H.; Kraus, S.G.; Jowsey, T.; Glasgow, N. The experience of living with chronic heart failure: A narrative review of qualitative studies. BMC Health Serv. Res. 2010, 10, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durante, A.; Greco, A.; Annoni, A.M.; Steca, P.; Alvaro, R.; Vellone, E. Determinants of caregiver burden in heart failure: Does caregiver contribution to heart failure patient self-care increase caregiver burden? Eur. J. Cardiovasc. Nurs. 2019, 18, 691–699. [Google Scholar] [CrossRef] [PubMed]
- Bidwell, J.T.; Lyons, K.S.; Lee, C.S. Caregiver Well-being and Patient Outcomes in Heart Failure. J. Cardiovasc. Nurs. 2017, 32, 372–382. [Google Scholar] [CrossRef] [PubMed]
- Buck, H.G.; Stromberg, A.; Chung, M.L.; Donovan, K.A.; Harkness, K.; Howard, A.M.; Kato, N.; Polo, R.; Evangelista, L. A systematic review of heart failure dyadic self-care interventions focusing on intervention components, contexts, and outcomes. Int. J. Nurs. Stud. 2018, 77, 232–242. [Google Scholar] [CrossRef] [PubMed]
- Siabani, S.; Leeder, S.R.; Currow, D.C. Barriers and facilitators to self-care in chronic heart failure: A meta-synthesis of qualitative studies. SpringerPlus 2013, 2, 320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickens, C.; Dickson, V.V.; Piano, M.R. Perceived Stress Among Patients With Heart Failure Who Have Low Socioeconomic Status. J. Cardiovasc. Nurs. 2019, 34, E1–E8. [Google Scholar] [CrossRef]
- SURS, Republic of Slovenia Statistical Office. Pomurska Region. 2019. Available online: www.stat.si/obcine (accessed on 7 January 2020).
- Ming, L.C.; Hassali, M.A.; Shafie, A.A.; Awaisu, A.; Hadi, M.A.; Al-Haddad, M. Perspectives of heart failure patients in Malaysia towards medications and disease state management: Findings from a qualitative study. J. Public Health 2011, 19, 569–577. [Google Scholar] [CrossRef]
- Boyd, K.; Murray, S.A.; Kendall, M.; Worth, A.; Benton, T.F.; Clausen, H. Living with advanced heart failure: A prospective, community based study of patients and their carers. Eur. J. Hear. Fail. 2004, 6, 585–591. [Google Scholar] [CrossRef]
- Pattenden, J.; Roberts, H.; Lewin, R. Living with Heart Failure; Patient and Carer Perspectives. Eur. J. Cardiovasc. Nurs. 2007, 6, 273–279. [Google Scholar] [CrossRef]
- Liljeroos, M.; Ågren, S.; Jaarsma, T.; Årestedt, K.; Strömberg, A. Long-term effects of a dyadic psycho-educational intervention on caregiver burden and morbidity in partners of patients with heart failure: A randomized controlled trial. Qual. Life Res. 2016, 26, 367–379. [Google Scholar] [CrossRef]
- Liljeroos, M.; Kato, N.P.; Van Der Wal, M.H.; Brons, M.; Luttik, M.L.; Van Veldhuisen, D.J.; Strömberg, A.; Jaarsma, T. Trajectory of self-care behaviour in patients with heart failure: The impact on clinical outcomes and influencing factors. Eur. J. Cardiovasc. Nurs. 2020. [Google Scholar] [CrossRef] [PubMed]


| Interview Domain | Sample Question |
|---|---|
| General questions about the disease | –Tell me about heart failure and how you/patient found out you had it? |
| –How does your present life differ from your life before heart failure? | |
| General questions about self-care | –What are you doing on a daily basis to manage your condition/help patient (dealing with symptoms, specific tasks–taking medication, monitoring weight, managing appointments etc.)? |
| –What makes it easier/harder to take care of yourself/patient? | |
| –How do you know you’re/patient’s doing ok, what do you do to monitor yourself/patient? | |
| General questions about psychological, social support | –How does heart failure affect the relationship with your relatives/friends/family? |
| –Who do you talk to about (issues mentioned throughout the interview)? | |
| –What would you do if you/patient felt down, frustrated or worried? | |
| General questions about received healthcare in an outpatient heart failure clinic | –How do you experience your encounters with healthcare? |
| –Which information have you received by healthcare professionals? | |
| –What instructions did you receive about taking care of yourself/patient at home? Do you think the instructions are easy to understand, what would help you fit the instructions into your normal activities better? | |
| –How comfortable are you talking to your physician about your/patient’s health concerns? |
| Demographics | Patients n = 32 | Informal Caregivers n = 21 | Patients with Informal Caregiver n = 18 | Patients without Informal Caregiver n = 14 | p-Value (Patients with-without Informal Caregiver) |
|---|---|---|---|---|---|
| Gender, n (%) | |||||
| Male | 20 (63) | 4 (19) | 14 (77) | 6 (43) | p = 0.018 |
| Age, M ± SD | 72.9 ± 11.3 | 59.7 ± 13.7 | 77.1 ± 7.6 | 67.7 ± 13.3 | p = 0.013 |
| Educational Level, n (%) | |||||
| Incomplete primary | 2 (6) | 1 (5) | 1 (6) | 1 (7) | p = 0.081 |
| Primary school | 14 (44) | 5 (24) | 9 (50) | 5 (36) | |
| Vocational | 9 (28) | 4 (19) | 5 (28) | 3 (21) | |
| Secondary | 2 (6) | 8 (38) | 1 (6) | 1 (7) | |
| College | 1 (3) | 0 | 0 | 1 (7) | |
| University | 1 (3) | 2 (10) | 1 (6) | 0 | |
| Marital Status, n (%) | |||||
| Single/never married | 5 (16) | 3 (14) | 2 (11) | 3 (21) | p = 0.831 |
| Married | 19 (59) | 16 (76) | 11 (61) | 8 (57) | |
| Divorced/separated | 1 (3) | 1 (5) | 2 (11) | 0 | |
| Widowed | 5 (16) | 0 | 3 (17) | 1 (7) | |
| Employment Status, n (%) | |||||
| Full-time | 1 (3) | 6 (29) | 1 (6) | 0 | p = 0.210 |
| Part-time | 0 | 1 (5) | 0 | 0 | |
| Retired | 25 (78) | 9 (43) | 16 (89) | 9 (64) | |
| Unemployed | 2 (6) | 2 (10) | 0 | 2 (14) | |
| Others | 1 (3) | 3 (14) | 0 | 1 (7) | |
| Years Since Heart Failure Diagnosis, M ± SD | 5.8 ± 5.1 | 6.5 ± 5.8 | 4.7 ± 4.1 | p = 0.282 | |
| Relationship to Patient, n (%) | |||||
| Husband/Wife/Partner | 10 (48) | 9 (50) | |||
| Son/Daughter | 8 (38) | 7 (39) | |||
| Other relative1 | 2 (10) | 1 (6) | |||
| Friend | 1 (5) | 1 (6) | |||
| Lives in Same Household, n (%) | |||||
| Yes | 15 (71) | 14 (78) | |||
| No | 5 (24) | 4 (22) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sedlar, N.; Lainscak, M.; Farkas, J. Living with Chronic Heart Failure: Exploring Patient, Informal Caregiver, and Healthcare Professional Perceptions. Int. J. Environ. Res. Public Health 2020, 17, 2666. https://doi.org/10.3390/ijerph17082666
Sedlar N, Lainscak M, Farkas J. Living with Chronic Heart Failure: Exploring Patient, Informal Caregiver, and Healthcare Professional Perceptions. International Journal of Environmental Research and Public Health. 2020; 17(8):2666. https://doi.org/10.3390/ijerph17082666
Chicago/Turabian StyleSedlar, Natasa, Mitja Lainscak, and Jerneja Farkas. 2020. "Living with Chronic Heart Failure: Exploring Patient, Informal Caregiver, and Healthcare Professional Perceptions" International Journal of Environmental Research and Public Health 17, no. 8: 2666. https://doi.org/10.3390/ijerph17082666