Development and Validation of an Atrial Fibrillation Knowledge Assessment Tool (AFKAT)

 ,
, 
Abstract
:1. Introduction
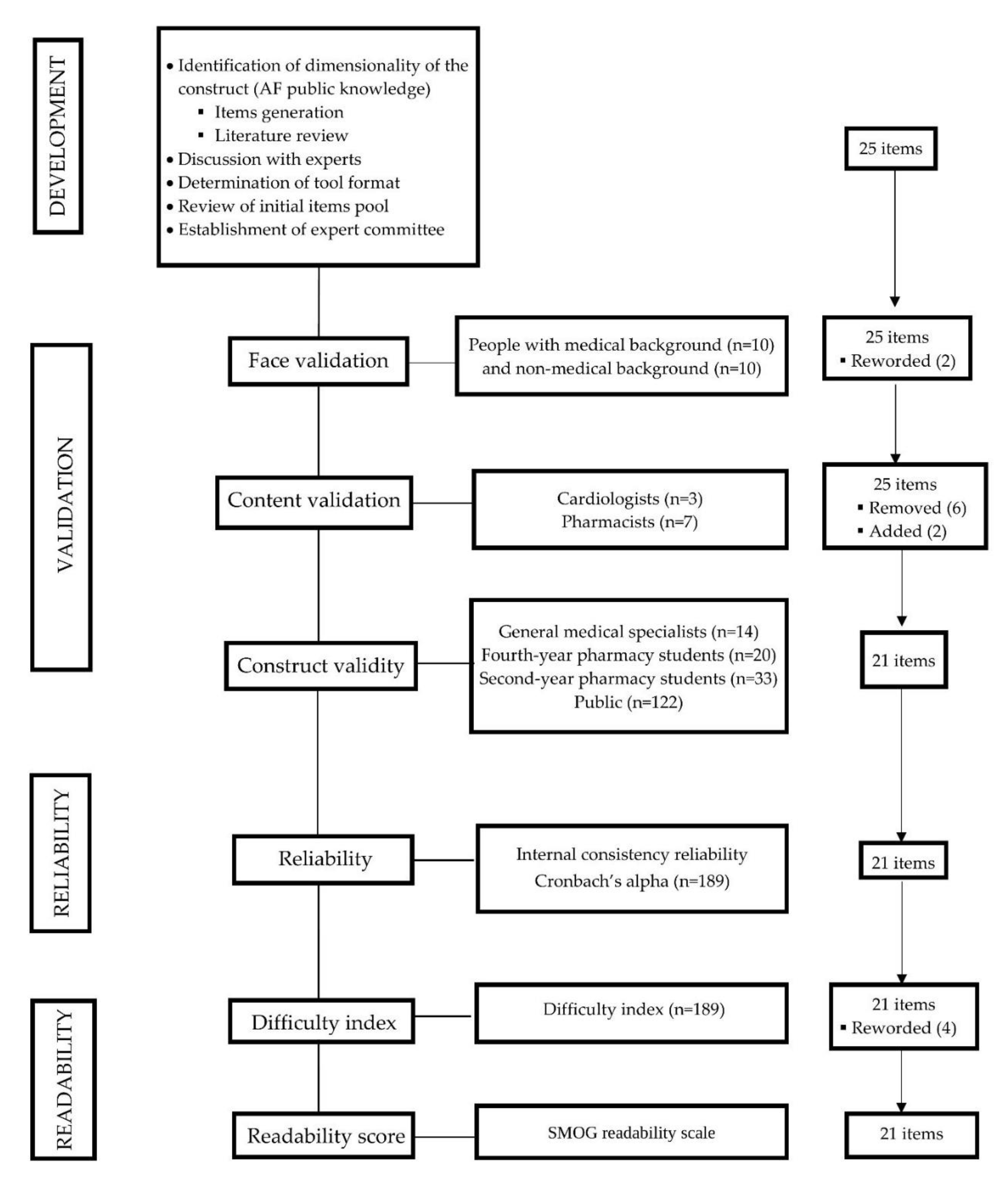
2. Materials and Methods
2.1. Development of AF Knowledge Assessment Tool
2.2. Psychometric Testing of the Tool
Face Validity
2.3. Content Validity
2.4. Validation Study
2.5. Recruitment of Participants
2.6. Study Procedures
2.7. Construct Validity
2.8. Internal Consistency Reliability
2.9. Item Discrimination
2.10. Difficulty Index
2.11. Readability Analysis
2.12. Statistical Analysis
3. Results
3.1. Face Validity
3.2. Content Validity Index
3.3. Validation Study
3.4. Construct Validity
3.5. Internal Consistency-Reliability
3.6. Item Discrimination
3.7. Difficulty Index
3.8. Readability Index
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| S/N | Item | I-CVI | Modified Kappa (k*) |
|---|---|---|---|
| 1 | Atrial fibrillation is a medical condition where the heart beats slower than normal. | 0.8 | 0.8 |
| 2 | The precise cause of atrial fibrillation is unknown. | 0.3 | 0.2 |
| 3 | Atrial fibrillation occurs only in old age. | 0.8 | 0.8 |
| 4 | Atrial fibrillation is a lifelong condition. | 0.9 | 0.9 |
| 5 | Atrial fibrillation may cause blood clots in the heart. | 0.8 | 0.7 |
| 6 | People with atrial fibrillation can still have an active life. | 0.9 | 0.9 |
| 7 | Episodes of atrial fibrillation can be recurrent. | 0.9 | 0.9 |
| 8 | Episodes of atrial fibrillation are predictable. | 0.8 | 0.7 |
| 9 | Atrial fibrillation is diagnosed using a chest X-ray. | 0.3 | 0.18 |
| 10 | Early diagnosis of atrial fibrillation can prevent stroke. | 0.9 | 0.9 |
| 11 | Hypertension increases the risk of developing atrial fibrillation. | 0.9 | 0.9 |
| 12 | Atrial fibrillation significantly increases the risk of stroke. | 1.0 | 1.0 |
| 13 | Atrial fibrillation is associated with a heart attack. | 0.6 | 0.5 |
| 14 | Atrial fibrillation, by itself, is life-threatening. | 0.30 | 0.2 |
| 15 | Shortness of breath, chest pain can be potential symptoms of atrial fibrillation. | 0.7 | 0.7 |
| 16 | Someone could have atrial fibrillation without having any symptoms. | 1.0 | 1.0 |
| 17 | Symptoms of atrial fibrillation may be occasional, persistent, or permanent. | 0.9 | 0.9 |
| 18 | Atrial fibrillation has psychological effects on people’s lives. | 0.8 | 0.9 |
| 19 | Atrial fibrillation is modifiable with lifestyle changes. | 0.9 | 1.0 |
| 20 | Avoiding excessive alcohol intake can prevent atrial fibrillation. | 0.7 | 0.7 |
| 21 | Atrial fibrillation can be detected by checking the pulse rate. | 0.8 | 0.8 |
| 22 | Screening for atrial fibrillation may reduce the risk of developing a stroke. | 0.5 | 0.3 |
| 23 | Atrial fibrillation can be treated with medications. | 0.8 | 0.8 |
| 24 | Atrial fibrillation can be treated with surgery. | 0.7 | 0.7 |
| 25 | The goal of treating atrial fibrillation is to increase the heart rate. | 0.3 | 0.2 |
References
- Kirchhof, P.; Breithardt, G.; Bax, J.; Benninger, G.; Blomstrom-Lundqvist, C.; Boriani, G.; Brandes, A.; Brown, H.; Brueckmann, M.; Calkins, H.; et al. A roadmap to improve the quality of atrial fibrillation management: Proceedings from the fifth Atrial Fibrillation Network/European Heart Rhythm Association consensus conference. Europace 2016, 18, 37–50. [Google Scholar] [CrossRef]
- McCabe, P.J.; Barton, D.L.; DeVon, H.A. Older Adults at Risk for Atrial Fibrillation Lack Knowledge and Confidence to Seek Treatment for Signs and Symptoms. SAGE Open Nurs. 2017, 3, 2377960817720324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregory, Y.H.; Lip, H.F.T.; Lane, D.A. Atrial fibrillation. Lancet 2012, 379, 18–24. [Google Scholar]
- Wendelboe, A.M.; Raskob, G.E.; Angchaisuksiri, P.; Blanco, A.N.; Büller, H.; Ddungu, H.; Dvorak, J.D.; Hunt, B.J.; Hylek, E.M.; Kakkar, A. Global public awareness about atrial fibrillation. Res. Pract. Thromb. Haemost. 2018, 2, 49–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCabe, P.J.; Rhudy, L.M.; Chamberlain, A.M.; DeVon, H.A. Fatigue, dyspnea, and intermittent symptoms are associated with treatment-seeking delay for symptoms of atrial fibrillation before diagnosis. Eur. J. Cardiovasc. Nurs. 2016, 15, 459–468. [Google Scholar] [CrossRef]
- McCabe, P.J.; Rhudy, L.M.; DeVon, H.A. Patients’ experiences from symptom onset to initial treatment for atrial fibrillation. J. Clin. Nurs. 2015, 24, 786–796. [Google Scholar] [CrossRef] [PubMed]
- Frewen, J.; Finucane, C.; Cronin, H.; Rice, C.; Kearney, P.; Harbison, J.; Kenny, R. Factors that influence awareness and treatment of atrial fibrillation in older adults. QJM 2013, 106, 415–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, E.; Hyslop, F.; Richmond, R. Barriers and facilitators to uptake of cervical cancer screening among women in Uganda: A systematic review. BMC Women Health 2019, 19, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Javanparast, S.; Ward, P.R.; Carter, S.M.; Wilson, C.J. Barriers to and facilitators of colorectal cancer screening in different population subgroups in Adelaide, South Australia. Med. J. Aust. 2012, 196, 521–523. [Google Scholar] [CrossRef]
- Briggs, R.; Drumm, B.; Dwyer, R.; O’Neill, D.; Kennelly, S.P.; Coughlan, T.; Collins, R. Awareness of atrial fibrillation—Effectiveness of a pilot national awareness campaign. Ir. J. Med. Sci. 2019, 189, 149–153. [Google Scholar] [CrossRef]
- Rosenfeld, L.E.; Amin, A.N.; Hsu, J.C.; Oxner, A.; Hills, M.T.; Frankel, D.S. The Heart Rhythm Society/American College of Physicians Atrial Fibrillation Screening and Education Initiative. Heart Rhythm 2019, 16, e59–e65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best practices for developing and validating scales for health, social, and behavioral research: A primer. Front. Public Health 2018, 6, 149. [Google Scholar] [CrossRef] [PubMed]
- Polit, D.F.; Beck, C.T. The Content Validity Index: Are You Sure You Know What’s Being Reported? Critique and Recommendations. Res. Nurs. Health 2006, 29, 489–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, L.L. Instrument review: Getting the most from a panel of experts. Appl. Nurs. Res. 1992, 5, 194–197. [Google Scholar] [CrossRef]
- Wynd, C.A.; Schmidt, B.; Schaefer, M.A. Two Quantitative Approaches for Estimating Content Validity. West. J. Nurs. Res. 2003, 25, 508–518. [Google Scholar] [CrossRef]
- Zamanzadeh, V.; Ghahramanian, A.; Rassouli, M.; Abbaszadeh, A.; Alavi-Majd, H.; Nikanfar, A.-R. Design and implementation content validity study: Development of an instrument for measuring patient-centered communication. J. Caring Sci. 2015, 4, 165. [Google Scholar] [CrossRef]
- PennState Eberly College of Science Evaluating (2018). The Binomial Random Variable in SPSS. Available online: https://newonlinecourses.science.psu.edu/stat800/node/29/ (accessed on 20 December 2018).
- Lloyd-Jones, D.M.; Wang, T.J.; Leip, E.P.; Larson, M.G.; Levy, D.; Vasan, R.S.; D’Agostino, R.B.; Massaro, J.M.; Beiser, A.; Wolf, P.A. Lifetime risk for development of atrial fibrillation: The Framingham Heart Study. Circulation 2004, 110, 1042–1046. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A.G. Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- DeVon, H.A.; Block, M.E.; Moyle-Wright, P.; Ernst, D.M.; Hayden, S.J.; Lazzara, D.J.; Savoy, S.M.; Kostas-Polston, E. A psychometric toolbox for testing validity and reliability. J. Nurs. Scholarsh. 2007, 39, 155–164. [Google Scholar] [CrossRef]
- Clark, L.A.; Watson, D. Constructing validity: Basic issues in objective scale development. Psychol. Assess. 1995, 7, 309. [Google Scholar] [CrossRef]
- Piedmont, R.L. Inter-item Correlations. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 3303–3304. [Google Scholar]
- Streiner, D.L.; Norman, G.R.; Cairney, J. Health Measurement Scales: A Practical Guide to Their Development and Use; Oxford University Press: Oxford, NY, USA, 2015. [Google Scholar]
- Univeristy of Washington. Understanding Item Analysis. 2019. Available online: http://www.washington.edu/assessment/scanning-scoring/scoring/reports/item-analysis/ (accessed on 24 January 2019).
- Contreras, A.; Garcia-Alonso, R.; Echenique, M.; Daye-Contreras, F. The SOL formulas for converting SMOG readability scores between health education materials written in Spanish, English, and French. J. Health Commun. 1999, 4, 21–29. [Google Scholar]
- Readable.io. Readability Index. 2011. Available online: https://app.readable.io/text/?demo (accessed on 2 January 2019).
- El-Haddad, N.; Spooner, C.; Faruqi, N.; Denney-Wilson, E.; Harris, M. Readability and content analysis of lifestyle education resources for weight management in Australian general practice. BMC Obes. 2016, 3, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IBM Knowledge Centre. One-Way ANOVA Post Hoc Tests. 2019. Available online: https://www.ibm.com/support/knowledgecenter/en/SSLVMB_23.0.0/spss/base/idh_onew_post.html (accessed on 20 July 2019).
- Sarantakos, S. Surveys: Interviewing. In Social Research; Macmillan Education: London, UK, 1998; pp. 246–271. [Google Scholar]
- Salkind, N.J. Encyclopedia of Research Design; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2010; Volume 1. [Google Scholar]
- Polit, D.F.; Beck, C.T.; Owen, S.V. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res. Nurs. Health 2007, 30, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Polit, D.F.; Beck, C.T. Nursing Research: Principles and Methods; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2004. [Google Scholar]
- National Institute of Health. Clear & Simple: Developing Effective Print Materials for Low-Literacy Audiences. 2018. Available online: https://www.nih.gov/institutes-nih/nih-office-director/office-communications-public-liaison/clear-communication/clear-simple (accessed on 24 January 2019).

| S/N | Item | Correct Answer |
|---|---|---|
| 1 | Atrial fibrillation is a medical condition where the heart beats slower than normal. | False |
| 2 | Atrial fibrillation may cause blood clots in the heart. | True |
| 3 | Episodes of atrial fibrillation are predictable. | False |
| 4 | People with atrial fibrillation can still have an active life. | True |
| 5 | Atrial fibrillation can only be treated with surgery. | False |
| 6 | Episodes of atrial fibrillation can be recurrent. | True |
| 7 | Early diagnosis and management of atrial fibrillation can prevent stroke. | True |
| 8 | Low blood pressure increases the risk of developing atrial fibrillation. | False |
| 9 | Atrial fibrillation significantly increases the risk of stroke. | True |
| 10 | Atrial fibrillation occurs only in people with prior signs of heart disease. | False |
| 11 | Shortness of breath and fainting can be potential symptoms of atrial fibrillation. | True |
| 12 | Atrial fibrillation occurs only in old age. | False |
| 13 | Someone could have atrial fibrillation without having any symptoms. | True |
| 14 | Symptoms of atrial fibrillation may be occasional, persistent, or permanent. | True |
| 15 | Atrial fibrillation usually has major psychological effects on people’s lives. | False |
| 16 | The risk of developing atrial fibrillation can be reduced with lifestyle changes. | True |
| 17 | Atrial fibrillation can be detected by checking the regularity of the pulse. | True |
| 18 | Screening for atrial fibrillation is safe. | True |
| 19 | Once present, atrial fibrillation is always a lifelong condition. | False |
| 20 | Atrial fibrillation can be treated with medications. | True |
| 21 | Anticoagulants (“blood thinners”) are often used to reduce the risk of stroke in people with atrial fibrillation. | True |
| Study Sub-Groups | Mean Percentage Score (SD) | F Statistics (df) | p-Value * |
|---|---|---|---|
| General medical specialist (n = 14) | 92.9 (6.9) | 21.044 (3, 185) | <0.001 |
| Fourth-year pharmacy student (n = 20) | 87.6 (7.5) | ||
| Second-year pharmacy student (n = 33) | 68.5 (20.4) | ||
| Members of the general public (n = 122) | 53.4 (27.7) |
| Item Number | Difficulty Index | Item-Total Correlation | Cronbach’s Alpha * |
|---|---|---|---|
| 1 | 55.6 | 0.54 | 0.91 |
| 2 | 57.7 | 0.39 | 0.91 |
| 3 | 82.5 | 0.66 | 0.90 |
| 4 | 30.2 | 0.39 | 0.91 |
| 5 | 60.3 | 0.64 | 0.90 |
| 6 | 79.4 | 0.71 | 0.90 |
| 7 | 79.9 | 0.69 | 0.90 |
| 8 | 67.7 | 0.58 | 0.90 |
| 9 | 68.3 | 0.63 | 0.90 |
| 10 | 37.0 | 0.48 | 0.91 |
| 11 | 64.6 | 0.67 | 0.90 |
| 12 | 76.7 | 0.66 | 0.90 |
| 13 | 66.7 | 0.52 | 0.91 |
| 14 | 73.5 | 0.64 | 0.90 |
| 15 | 67.7 | 0.38 | 0.91 |
| 16 | 46.6 | 0.23 | 0.91 |
| 17 | 42.3 | 0.32 | 0.91 |
| 18 | 66.7 | 0.46 | 0.91 |
| 19 | 68.8 | 0.67 | 0.90 |
| 20 | 58.7 | 0.63 | 0.90 |
| 21 | 64.0 | 0.63 | 0.90 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jatau Abubakar, I.; Wimmer, B.C.; Bereznicki, L.R.; Dwan, C.; Black, J.A.; M. Bezabhe, W.; M. Peterson, G. Development and Validation of an Atrial Fibrillation Knowledge Assessment Tool (AFKAT). Int. J. Environ. Res. Public Health 2020, 17, 1721. https://doi.org/10.3390/ijerph17051721
Jatau Abubakar I, Wimmer BC, Bereznicki LR, Dwan C, Black JA, M. Bezabhe W, M. Peterson G. Development and Validation of an Atrial Fibrillation Knowledge Assessment Tool (AFKAT). International Journal of Environmental Research and Public Health. 2020; 17(5):1721. https://doi.org/10.3390/ijerph17051721
Chicago/Turabian StyleJatau Abubakar, Ibrahim, Barbara C. Wimmer, Luke R. Bereznicki, Corinna Dwan, J. Andrew Black, Woldesellassie M. Bezabhe, and Gregory M. Peterson. 2020. "Development and Validation of an Atrial Fibrillation Knowledge Assessment Tool (AFKAT)" International Journal of Environmental Research and Public Health 17, no. 5: 1721. https://doi.org/10.3390/ijerph17051721