Disparities in the Use of General Somatic Care among Individuals Treated for Severe Mental Disorders and the General Population in France

Abstract
:1. Introduction
2. Materials and Methods
2.1. Conceptual Framework
2.2. Setting and Particularities of the National Context Explored
2.3. Study Design and Main Data Source
2.4. Study Population
2.5. Matching between Cases and Controls
2.6. Indicators of Healthcare Use
2.7. Analysis
3. Results
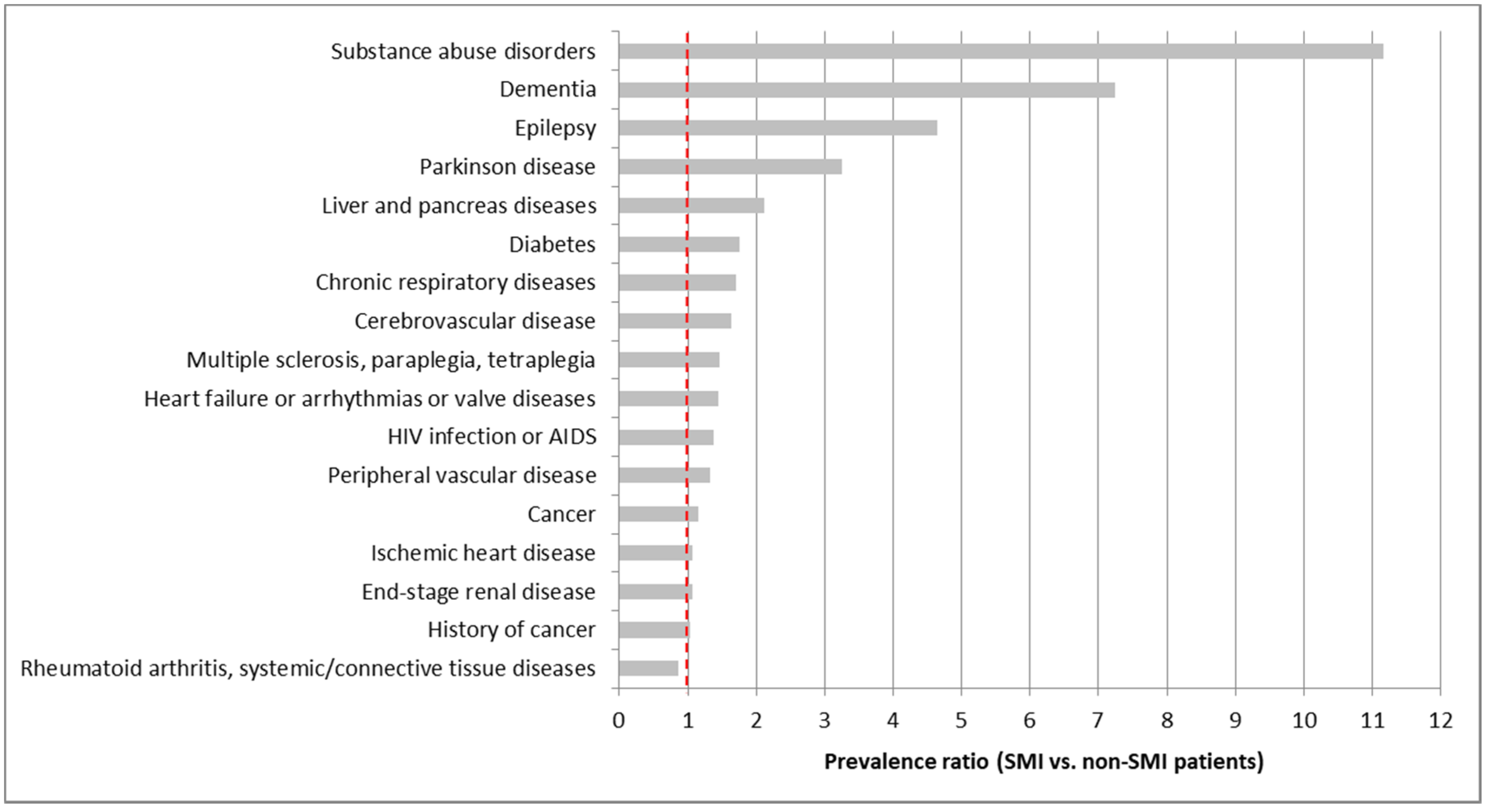
3.1. Study Population Characteristics
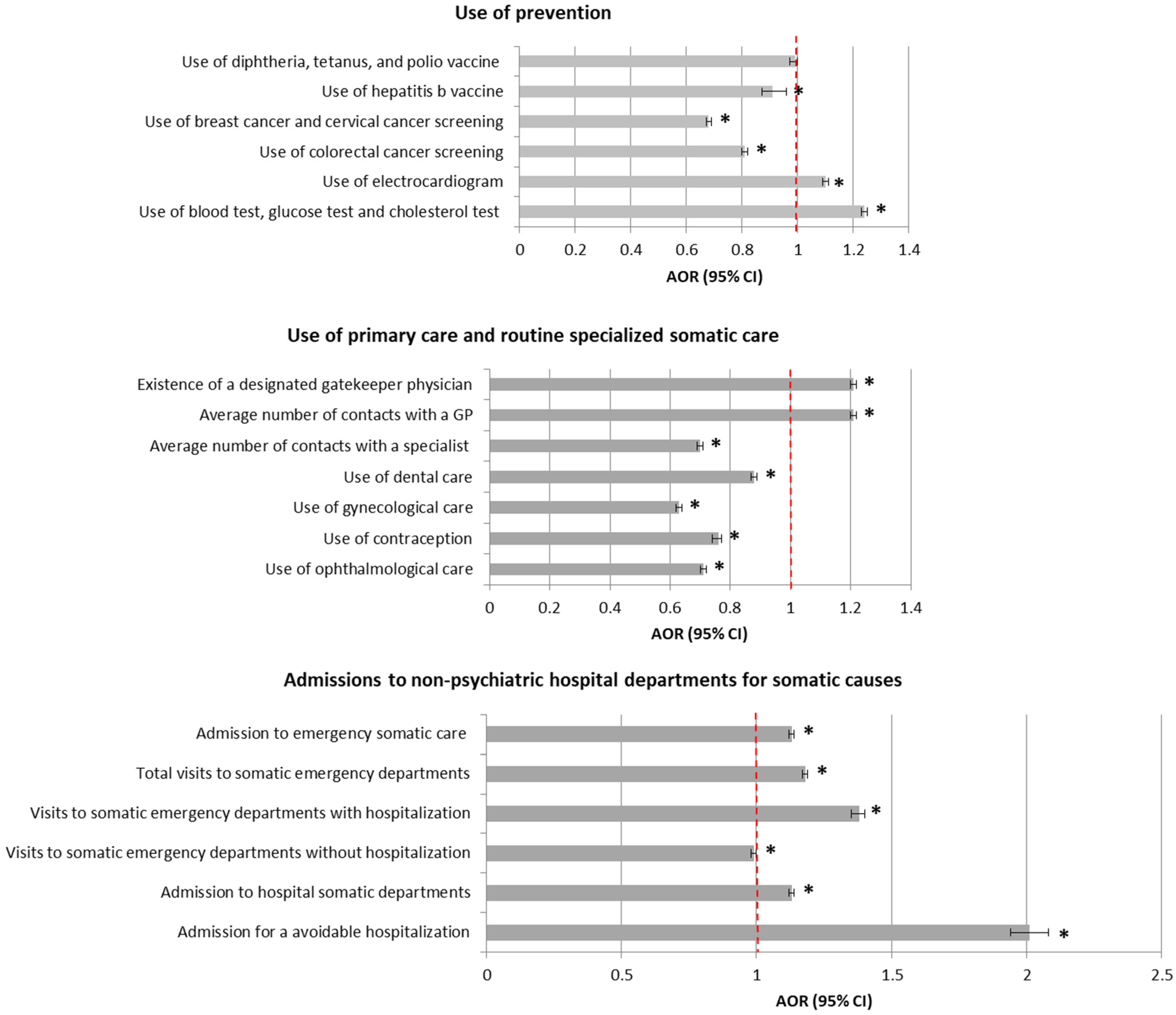
3.2. Comparisons of Patterns of Healthcare Use between Matched Cases and Controls
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fleury, M.-J.; Grenier, G. Etat de Situation sur la Santé Mentale au Québec et Réponse du Système de Santé et des Services Sociaux; Gouvernement du Québec: Québec, QC, Canada, 2012.
- Janssen, E.M.; McGinty, E.E.; Azrin, S.T.; Juliano-Bult, D.; Daumit, G.L. Review of the evidence: Prevalence of medical conditions in the United States population with serious mental illness. Gen. Hosp. Psychiatry 2015, 37, 199–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thornicroft, G. Physical health disparities and mental illness: The scandal of premature mortality. Br. J. Psychiatry 2011, 199, 441–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forsman, A.K.; Fredén, L.; Lindqvist, R.; Wahlbeck, K. Contribution of the Nordic School of Public Health to the public mental health research field: A selection of research initiatives, 2007–2014. Scand. J. Public Health 2015, 43, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Wahlbeck, K.; Westman, J.; Nordentoft, M.; Gissler, M.; Laursen, T.M. Outcomes of Nordic mental health systems: Life expectancy of patients with mental disorders. Br. J. Psychiatry 2011, 199, 453–458. [Google Scholar] [CrossRef]
- Krupchanka, D.; Mladá, K.; Winkler, P.; Khazaal, Y.; Albanese, E. Mortality in people with mental disorders in the Czech Republic: A nationwide, register-based cohort study. Lancet Public Health 2018, 3, e289–e295. [Google Scholar] [CrossRef]
- Coldefy, M.; Gandré, C. Persons with severe mental disorders: Life expectancy is greatly reduced and premature mortality has quadrupled. Quest. D’économie St. 2018, 237, 1–8. [Google Scholar]
- Oakley, P.; Kisely, S.; Baxter, A.; Harris, M.; Desoe, J.; Dziouba, A.; Siskind, D. Increased mortality among people with schizophrenia and other non-affective psychotic disorders in the community: A systematic review and meta-analysis. J. Psychiatr. Res. 2018, 102, 245–253. [Google Scholar] [CrossRef]
- Saxena, S. Excess mortality among people with mental disorders: A public health priority. Lancet Public Health 2018, 3, e264–e265. [Google Scholar] [CrossRef]
- World Health Organization. Mental Health Action Plan 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Mitchell, A.J.; Vancampfort, D.; Sweers, K.; van Winkel, R.; Yu, W.; De Hert, M. Prevalence of metabolic syndrome and metabolic abnormalities in schizophrenia and related disorders—A systematic review and meta-analysis. Schizophr. Bull. 2013, 39, 306–318. [Google Scholar] [CrossRef] [Green Version]
- DiMatteo, M.R.; Lepper, H.S.; Croghan, T.W. Depression is a risk factor for noncompliance with medical treatment: Meta-analysis of the effects of anxiety and depression on patient adherence. Arch. Intern. Med. 2000, 160, 2101–2107. [Google Scholar] [CrossRef]
- Berg, C.J.; Thomas, A.N.; Mertens, A.C.; Schauer, G.L.; Pinsker, E.A.; Ahluwalia, J.S.; Khuri, F.R. Correlates of continued smoking versus cessation among survivors of smoking-related cancers. Psychooncology 2013, 22, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Wahlbeck, K. Public mental health: The time is ripe for translation of evidence into practice. World Psychiatry 2015, 14, 36–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization, Regional office for Europe. Healthy, Prosperous Lives for All: The European Health Equity Status Report 2019; WHO Regional Office for Europe: Copenhagen, Denmark, 2019. [Google Scholar]
- Gierisch, J.M.; Beadles, C.; Shapiro, A.; McDuffie, J.R.; Cunningham, N.; Bradford, D.; Strauss, J.; Callahan, M.; Chen, M.; Hemminger, A.; et al. Health Disparities in Quality Indicators of Healthcare among Adults with Mental Illness; Department of Veterans Affairs (US): Washington, DC, USA, 2014.
- Wheeler, A.; McKenna, B.; Madell, D. Access to general health care services by a New Zealand population with serious mental illness. J. Prim. Health Care 2014, 6, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Pandurangi, A.; Smith, W. Disparities in breast and cervical cancer screening in women with mental illness: A systematic literature review. Am. J. Prev. Med. 2013, 44, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Björk Brämberg, E.; Torgerson, J.; Norman Kjellström, A.; Welin, P.; Rusner, M. Access to primary and specialized somatic health care for persons with severe mental illness: A qualitative study of perceived barriers and facilitators in Swedish health care. BMC Fam. Pract. 2018, 19, 12. [Google Scholar] [CrossRef] [Green Version]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef]
- Cook, B.L.; Hou, S.S.-Y.; Lee-Tauler, S.Y.; Progovac, A.M.; Samson, F.; Sanchez, M.J. A Review of Mental Health and Mental Health Care Disparities Research: 2011–2014. Med. Care Res. Rev. 2019, 76, 683–710. [Google Scholar] [CrossRef]
- Court of Auditors. L’organisation des Soins Psychiatriques, les Effets du Plan “Psychiatrie et Santé Mentale” (2005–2010); Court of Auditors: Paris, France, 2011. [Google Scholar]
- Legifrance Circulaire du 15 Mars 1960 Relative AU Programme D’Organisation et D’éQuipement des Départements en Matière de Lutte Contre Les Maladies Mentales. Available online: https://bdoc.ofdt.fr/doc_num.php?explnum_id=21540 (accessed on 11 May 2020).
- Coldefy, M. The evolution of psychiatric care systems in Germany, England, France and Italy: Similarities and differences. Quest. D’économie St. 2012, 180, 1–8. [Google Scholar]
- Ministry of Health. Comité Interministériel Pour La Santé Priorité Prevention—Rester en Bonne Santé Tout AU Long de sa Vie; Ministry of Health: Paris, France, 2018.
- Ministry of Health. Ministère de La Santé Feuille de Route Santé Mentale et Psychiatrie; Ministry of Health: Paris, France, 2018.
- Leboyer, M.; Llorca, P.-M. Psychiatrie: L’état D’urgence; Fayard: Paris, France, 2018. [Google Scholar]
- French Psychiatric Federation. Recommandation de Bonne Pratique en psyChiatrie: Comment Améliorer la Prise en Charge Somatique des Patients Ayant Une Pathologie Psychiatrique Sévère et Chronique; French Psychiatric Federation: Paris, France, 2015. [Google Scholar]
- France Assos Santé. Les Français et L’Accès Aux Soins; France Assos Santé: Paris, France, 2019. [Google Scholar]
- Lengagne, P.; Penneau, A.; Pichetti, S.; Sermet, C. L’accès Aux Soins Courants et Préventifs des Personnes en Situation de Handicap en France. Tome 1—Résultats de l’enquête Handicap-Santé Volet Ménages; Irdes: Paris, France, 2015. [Google Scholar]
- Rice, T.; Quentin, W.; Anell, A.; Barnes, A.J.; Rosenau, P.; Unruh, L.Y.; van Ginneken, E. Revisiting out-of-pocket requirements: Trends in spending, financial access barriers, and policy in ten high-income countries. BMC Health Serv. Res. 2018, 18, 371. [Google Scholar] [CrossRef] [Green Version]
- Dourgnon, P.; Or, Z.; Sorasith, C. The impact of the long-term illness scheme (LTI) on inequalities in the utilisation of ambulatory care between 1998 and 2008. Quest. D’économie St. 2013, 1, 1–6. [Google Scholar]
- Chevreul, K.; Berg Brigham, K.; Durand-Zaleski, I. France: Health system review. Health Syst. Transit. 2015, 17, 1–218. [Google Scholar] [PubMed]
- Durand-Zaleski, I. France: International Health Care System Profiles. Available online: http://international.commonwealthfund.org/countries/france/ (accessed on 24 February 2018).
- Tuppin, P.; Rudant, J.; Constantinou, P.; Gastaldi-Ménager, C.; Rachas, A.; de Roquefeuil, L.; Maura, G.; Caillol, H.; Tajahmady, A.; Coste, J.; et al. Value of a national administrative database to guide public decisions: From the système national d’information interrégimes de l’Assurance Maladie (SNIIRAM) to the système national des données de santé (SNDS) in France. Rev. Epidemiol. Sante Publique 2017, 65 (Suppl. 4), S149–S167. [Google Scholar] [CrossRef] [PubMed]
- Caisse Nationale D’assurance Maladie Méthode de Reprérage des Pathologies et D’affectation des Dépenses aux Pathologies. Available online: https://www.ameli.fr/l-assurance-maladie/statistiques-et-publications/etudes-en-sante-publique/cartographie-des-pathologies-et-des-depenses/methode.php (accessed on 6 March 2020).
- Legifrance. Décret n° 2016-1871 du 26 Décembre 2016 Relatif au Traitement de Données à Caractère Personnel Dénommé <Système National des Données de Santé>. Available online: https://www.legifrance.gouv.fr/affichTexte.do;jsessionid=C8519CDB2FDFB4598577E8449ACFA693.tpdila11v_1?cidTexte=JORFTEXT000033702840&dateTexte=&oldAction=rechJO&categorieLien=id&idJO=JORFCONT000033702240 (accessed on 7 February 2017).
- Bellass, S.; Taylor, J.; Han, L.; Prady, S.L.; Shiers, D.; Jacobs, R.; Holt, R.I.G.; Radford, J.; Gilbody, S.; Hewitt, C.; et al. Exploring Severe Mental Illness and Diabetes: Protocol for a Longitudinal, Observational, and Qualitative Mixed Methods Study. JMIR Res. Protoc. 2019, 8, 13407. [Google Scholar] [CrossRef] [PubMed]
- Barley, E.A.; Borschmann, R.D.; Walters, P.; Tylee, A. Interventions to encourage uptake of cancer screening for people with severe mental illness. Cochrane Database Syst. Rev. 2016, 9, CD009641. [Google Scholar] [CrossRef] [PubMed]
- Rey, G.; Jougla, E.; Fouillet, A.; Hémon, D. Ecological association between a deprivation index and mortality in France over the period 1997–2001: Variations with spatial scale, degree of urbanicity, age, gender and cause of death. BMC Public Health 2009, 9, 33. [Google Scholar] [CrossRef] [Green Version]
- Florida Agency for Health Care Administration. Ambulatory Care Sensitive Conditions Definitions and Data Source; Florida Agency for Health Care Administration: Tallahassee, FL, USA, 2018. [Google Scholar]
- Billings, J.; Zeitel, L.; Lukomnik, J.; Carey, T.S.; Blank, A.E.; Newman, L. Impact of socioeconomic status on hospital use in New York City. Health Aff. (Millwood) 1993, 12, 162–173. [Google Scholar] [CrossRef] [Green Version]
- Constantinou, P.; Tuppin, P.; Fagot-Campagna, A.; Gastaldi-Ménager, C.; Schellevis, F.G.; Pelletier-Fleury, N. Two morbidity indices developed in a nationwide population permitted performant outcome-specific severity adjustment. J. Clin. Epidemiol. 2018, 103, 60–70. [Google Scholar] [CrossRef] [Green Version]
- Agence Technique de L’information sur L’hospitalisation. Notice Technique n° CIM-MF 1234-4-2011 du 28 Décembre 2011; Agence Technique de L’information sur L’hospitalisation: Lyon, France, 2011. [Google Scholar]
- Ivory, V.; Witten, K.; Salmond, C.; Lin, E.-Y.; You, R.Q.; Blakely, T. The New Zealand Index of Neighbourhood Social Fragmentation: Integrating Theory and Data. Environ. Plan. A 2012, 44, 972–988. [Google Scholar] [CrossRef]
- Coldefy, M.; Nestrigue, C.; Paget, L.-M.; Younès, N. L’hospitalisation sans consentement en psychiatrie en 2010: Analyse et déterminants de la variabilité territoriale. Rev. Française Des Aff. Soc. 2016, 2, 253–273. [Google Scholar] [CrossRef]
- Chevillard, G.; Mousquès, J. Accessibilité aux soins et attractivité territoriale: Proposition d’une typologie des territoires de vie français. Cybergeo Eur. J. Geogr. 2018. [Google Scholar] [CrossRef]
- Insee. Base des Aires Urbaines. Available online: https://www.insee.fr/fr/information/2115011 (accessed on 6 March 2020).
- Caisse Nationale D’assurance Maladie. Caisse Nationale D’assurance Maladie Méthode Générale de la Cartographie des Pathologies, Version G5 (Années 2012 à 2016); Caisse Nationale D’assurance Maladie: Paris, France, 2018. [Google Scholar]
- Choron, G.; Lesage, F.-X.; Picy, L.; Courtet, P.; Olie, E. Somatic assessment of one hundred inpatients in a psychiatric crisis unit: A retrospective observational study. L’Encéphale 2019. [Google Scholar] [CrossRef] [PubMed]
- Denis, F.; Goueslard, K.; Siu-Paredes, F.; Amador, G.; Rusch, E.; Bertaud, V.; Quantin, C. Oral health treatment habits of people with schizophrenia in France: A retrospective cohort study. PLoS ONE 2020, 15, e0229946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gervaix, J.; Haour, G.; Michel, M.; Chevreul, K. Impact of mental illness on care for somatic comorbidities in France: A nation-wide hospital-based observational study. Epidemiol. Psychiatr. Sci. 2019, 28, 495–507. [Google Scholar] [CrossRef] [PubMed]
- Teng, P.-R.; Lin, M.-J.; Yeh, L.-L. Utilization of dental care among patients with severe mental illness: A study of a National Health Insurance database. BMC Oral. Health 2016, 16, 87. [Google Scholar] [CrossRef] [Green Version]
- Davydow, D.S.; Ribe, A.R.; Pedersen, H.S.; Fenger-Grøn, M.; Cerimele, J.M.; Vedsted, P.; Vestergaard, M. Serious Mental Illness and Risk for Hospitalizations and Rehospitalizations for Ambulatory Care-sensitive Conditions in Denmark: A Nationwide Population-based Cohort Study. Med. Care 2016, 54, 90–97. [Google Scholar] [CrossRef]
- Oud, M.J.T.; Schuling, J.; Groenier, K.H.; Verhaak, P.F.M.; Slooff, C.J.; Dekker, J.H.; Meyboom-de Jong, B. Care provided by general practitioners to patients with psychotic disorders: A cohort study. BMC Fam. Pract. 2010, 11, 92. [Google Scholar] [CrossRef] [Green Version]
- Chwastiak, L.A.; Rosenheck, R.A.; Kazis, L.E. Utilization of primary care by veterans with psychiatric illness in the National Department of Veterans Affairs Health Care System. J. Gen. Intern. Med. 2008, 23, 1835–1840. [Google Scholar] [CrossRef] [Green Version]
- Norton, J.; David, M.; Gandubert, C.; Bouvier, C.; Gutierrez, L.-A.; Frangeuil, A.; Macgregor, A.; Oude Engberink, A.; Mann, A.; Capdevielle, D. Ability of French General Practitioners to detect common mental disorders identified using the Patient Health Questionnaire: Has this changed with the introduction of gatekeeping and registration with a chosen doctor? Encephale 2016, 44, 22–31. [Google Scholar] [CrossRef]
- Bremer, D.; Lüdecke, D.; von dem Knesebeck, O. Social Relationships, Age and the Use of Preventive Health Services: Findings from the German Ageing Survey. Int. J. Environ. Res. Public Health 2019, 16, 4272. [Google Scholar] [CrossRef] [Green Version]
- Lake, J.; Turner, M.S. Urgent Need for Improved Mental Health Care and a More Collaborative Model of Care. Perm. J. 2017, 21, 17–024. [Google Scholar] [CrossRef] [Green Version]
- Kisely, S.; Baghaie, H.; Lalloo, R.; Siskind, D.; Johnson, N.W. A systematic review and meta-analysis of the association between poor oral health and severe mental illness. Psychosom. Med. 2015, 77, 83–92. [Google Scholar] [CrossRef] [PubMed]
- NHS England. Integrated Care and Support. Available online: https://www.england.nhs.uk/ourwork/part-rel/transformation-fund/ (accessed on 26 March 2020).
- World Health Organization. Framework on Integrated People-Centred Health Services; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients with SMI (n = 428,093) | Population without SMI (n = 33,225,644) | Prevalence Ratio |
|---|---|---|---|
| Mean (±SD) or n (%) | Mean (±SD) or n (%) | ||
| Demographic characteristics | |||
| Age | 45.27 (±11.53) | 41.08 (±13.36) | |
| Sex (female) | 198,887 (46.46) | 17,976,313 (54.10) | |
| Socio-economic characteristics at the individual level | |||
| Inclusion in the scheme covering healthcare costs for low-income groups (CMU-C) | 56,014 (13.08) | 2,990,454 (9.00) | |
| Missing values | 3399 (0.79) | 149,753 (0.45) | |
| Inclusion in the scheme providing financial assistance for the purchase of supplementary health insurance (ACS) | 79,953 (18.68) | 966,333 (2.91) | |
| Missing values | 3398 (0.79) | 149,746 (0.45) | |
| Characteristics of the living environment | |||
| Quintile of deprivation index (FDep) (from lower to higher deprivation) | |||
| 1st quintile | 74,727 (17.46) | 6,494,616 (19.55) | |
| 2nd quintile | 71,097 (16.61) | 6,351,714 (19.12) | |
| 3rd quintile | 91,747 (21.43) | 6,179,252 (18.60) | |
| 4th quintile | 82,810 (19.34) | 5,983,396 (18.01) | |
| 5th quintile | 81,711 (19.09) | 6,034,120 (18.16) | |
| Missing values 1 | 26,001 (6.07) | 2,182,546 (6.57) | |
| Social fragmentation | 3.49 (±2.65) | 2.38 (±2.73) | |
| Missing values | 18,236 (4.3) | 1,733,123 (5.2) | |
| Residency in an overseas territory | 14,000 (3.27) | 1,042,582 (3.14) | |
| Clinical characteristics | |||
| Comorbidity index | 1.73 (±3.15) | 0.67 (±2.04) | |
| Ischemic heart disease | 7789 (1.82) | 443,803 (1.34) | 1.36 |
| Cerebrovascular disease | 5062 (1.18) | 195,192 (0.59) | 2.00 |
| Heart failure or arrhythmias or valve diseases | 7466 (1.74) | 329,593 (0.99) | 1.76 |
| Peripheral vascular disease | 3312 (0.77) | 156,562 (0.47) | 1.64 |
| Diabetes | 34,432 (8.04) | 1,217,620 (3.66) | 2.20 |
| Cancer | 7139 (1.67) | 404,028 (1.22) | 1.37 |
| History of cancer | 8126 (1.90) | 520,134 (1.57) | 1.21 |
| Substance abuse disorders | 42,423 (9.91) | 212,744 (0.64) | 15.48 |
| Dementia (including Alzheimer’s disease) | 2538 (0.59) | 18,038 (0.05) | 11.80 |
| Parkinson disease | 1685 (0.39) | 32,631 (0.10) | 3.90 |
| Multiple sclerosis or paraplegia or tetraplegia | 2434 (0.57) | 115,839 (0.35) | 1.63 |
| Epilepsy | 10,308 (2.41) | 145,005 (0.44) | 5.48 |
| Chronic respiratory diseases (including asthma and COPD 2) | 31,928 (7.46) | 1,301,126 (3.92) | 1.90 |
| Rheumatoid arthritis or systemic and connective tissue diseases | 2139 (0.50) | 169,215 (0.51) | 0.98 |
| HIV infection or AIDS 3 | 2644 (0.62) | 106,911 (0.32) | 1.94 |
| End-stage renal disease | 617 (0.14) | 37,335 (0.11) | 1.27 |
| Liver and pancreas diseases (including chronic and acute failures) | 10,626 (2.48) | 293,445 (0.88) | 2.82 |
| Characteristic | Matched Patients with SMI (n = 413,437) | Matched Population without SMI (n = 1,240,311) |
|---|---|---|
| Mean (±SD) or n (%) | Mean (±SD) or n (%) | |
| Demographic characteristics | ||
| Age | 45.18 (±11.51) | 45.18 (±11.51) |
| Sex (female) | 192,242 (46.50) | 576,726 (46.50) |
| Socio-economic characteristics at the individual level | ||
| Inclusion in the scheme covering healthcare costs for low-income groups (CMU-C) | 55,492 (13.42) | 166,476 (13.42) |
| Inclusion in the scheme providing financial assistance for the purchase of supplementary health insurance (ACS) | 79,209 (19.16) | 42,375 (3.42) |
| Characteristics of the living environment | ||
| Quintile of deprivation index (FDep) (from lower to higher deprivation) | ||
| 1st quintile | 47,073 (17.92) | 222,219 (17.92) |
| 2nd quintile | 70,651 (17.09) | 211,953 (17.09) |
| 3rd quintile | 91,266 (22.07) | 273,798 (22,07) |
| 4th quintile | 82,342 (19.92) | 247,026 (19.92) |
| 5th quintile | 81,244 (19.65) | 243,732 (19.65) |
| Missing values 1 | 13,861 (3.35) | 41,583 (3.35) |
| Social fragmentation | 3.48 (±2.65) | 2.76 (±2.74) |
| Missing values | 6240 (1.51) | 21,660 (1.75) |
| Residency in an overseas territory | 18,864 (3.35) | 41,592 (3.35) |
| Taxonomy of French local geographical areas | ||
| 1: Suburban areas with a lower accessibility to healthcare and medium overall health status of the population | 54,769 (13.25) | 221,705 (17.87) |
| 2: Rural borders with a lower accessibility to healthcare | 39,161 (9.47) | 140,722 (11.35) |
| 3: Areas with a strong attraction for tourist and retired populations and the best accessibility to healthcare | 24,745 (5.99) | 86,553 (6.98) |
| 4: Deprived areas, urban and rural, with poor overall health status of the population | 41,223 (9.97) | 121,311 (9.78) |
| 5: Cities with abundant healthcare supply and heterogeneous socio-economic situations | 170,224 (41.17) | 415,723 (33.52) |
| 6: Wealthy cities and suburban areas | 65,754 (15.90) | 203,257 (16.39) |
| 7: Ad hoc category created for overseas territories which present similarities in terms of accessibility to healthcare | 13,823 (3.34) | 41,166 (3.32) |
| Missing values | 3738 (0.90) | 9874 (0.80) |
| Urban area zoning | ||
| Large urban center | 297,030 (71.84) | 782,746 (63.11) |
| Suburban municipality of a large urban center | 45,344 (10.97) | 196,074 (15.81) |
| Suburban municipality of several large urban centers | 13,077 (3.16) | 56,653 (4.57) |
| Average urban center | 13,264 (3.21) | 35,914 (2.90) |
| Suburban municipality of an average urban center | 1243 (0.30) | 5941 (0.48) |
| Small urban center | 13,453 (3.25) | 41,609 (3.35) |
| Suburban municipality of a small urban center | 550 (0.13) | 2825 (0.23) |
| Suburban municipality of several average or small urban centers | 12,142 (2.94) | 55,365 (4.46) |
| Isolated municipality located outside the sphere of influence of an urban center | 12,036 (2.91) | 44,459 (3.58) |
| Missing values | 5298 (1.28) | 18,725 (1.51) |
| Clinical characteristics | ||
| Comorbidity index | 1.73 (±3.16) | 0.82 (±2.27) |
| Ischemic heart disease | 7528 (1.82) | 21,097 (1.70) |
| Cerebrovascular disease | 4883 (1.18) | 8992 (0.72) |
| Heart failure or arrhythmias or valve diseases | 7191 (1.74) | 14,849 (1.20) |
| Peripheral vascular disease | 3206 (0.78) | 7364 (0.59) |
| Diabetes | 33,460 (8.09) | 57,041 (4.60) |
| Cancer | 6851 (1.66) | 17,855 (1.44) |
| History of cancer | 7817 (1.89) | 22,861 (1.84) |
| Substance abuse disorders | 41,066 (9.93) | 11,075 (0.89) |
| Dementia (including Alzheimer’s disease) | 2413 (0.58) | 933 (0.08) |
| Parkinson disease | 1628 (0.39) | 1480 (0.12) |
| Multiple sclerosis or paraplegia or tetraplegia | 2356 (0.57) | 4889 (0.39) |
| Epilepsy | 9997 (2.42) | 6491 (0.52) |
| Chronic respiratory diseases (including asthma and COPD 2) | 31,123 (7.53) | 55,126 (4.44) |
| Rheumatoid arthritis or systemic and connective tissue diseases | 2073 (0.50) | 7242 (0.58) |
| HIV infection or AIDS 3 | 2583 (0.62) | 5627 (0.45) |
| End-stage renal disease | 601 (0.15) | 1741 (0.14) |
| Liver and pancreas diseases (including chronic and acute failures) | 10,313 (2.49) | 14,610 (1.18) |
| Length of stay in inpatient psychiatric care over the two-year study period | ||
| 0 days | 301,650 (72.96) | 1,229,398 (99.12) |
| 1–60 days | 65,751 (15.90) | 8489 (0.68) |
| 61–180 days | 30,299 (7.33) | 1882 (0.15) |
| 181–365 days | 11,708 (2.83) | 417 (0.03) |
| >365 days | 4029 (0.97) | 125 (0.01) |
| Indicator of Healthcare Use | Matched Patients with SMI (n = 413,437) % or Mean (SD) | Matched Population without SMI (n = 1,240,311) % or Mean (SD) |
|---|---|---|
| Use of prevention * | ||
| Use of general preventive care services | ||
| Use of immunization (diphtheria, tetanus, and polio vaccine) (hepatitis b vaccine) | 6.76% | 7.07% |
| Use of immunization (hepatitis b vaccine) | 0.78% | 0.72% |
| Use of breast cancer and cervical cancer screening (for women only) | 47.93% | 60.98% |
| Use of colorectal cancer screening | 6.87% | 9.83% |
| Use of specific prevention targeting the adverse effects of antipsychotic drugs | ||
| Use of electrocardiogram | 13.81% | 10.36% |
| Use of blood test, glucose test and cholesterol test (all three) | 53.42% | 47.58% |
| Use of primary care and routine specialized somatic care * | ||
| Existence of a designated gatekeeper physician (GP or any other physician) | 78.56% | 76.45% |
| Average number of contacts with a GP | 13.37 (±15.99) | 10.13 (±14.36) |
| Average number of contacts with a specialist physician 1 | 2.57 (±4.45) | 3.77 (±6.82) |
| Use of dental care | 56.74% | 61.93% |
| Use of gynecological care (for women only) | 39.96% | 53.69% |
| Use of contraception (for women of child-bearing age only) | 38.03% | 45.06% |
| Use of ophthalmological care | 34.14% | 44.88% |
| Admissions to non-psychiatric hospital departments for somatic causes * | ||
| Admission to emergency somatic care (in emergency departments) | 42.58% | 28.10% |
| Average total number of visits to somatic emergency departments | 1.24 (±3.40) | 0.54 (±1.41) |
| Average number of visits to somatic emergency departments followed by a hospitalization | 0.32 (±1.13) | 0.10 (±0.50) |
| Average number of visits to somatic emergency departments not precursor to a subsequent hospitalization | 0.92 (±2.76) | 0.44 (±1.19) |
| Admission to hospital somatic departments 2 | 34.81% | 26.38% |
| Admission for an avoidable hospitalization 3 | 2.32% | 0.76% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gandré, C.; Coldefy, M. Disparities in the Use of General Somatic Care among Individuals Treated for Severe Mental Disorders and the General Population in France. Int. J. Environ. Res. Public Health 2020, 17, 3367. https://doi.org/10.3390/ijerph17103367
Gandré C, Coldefy M. Disparities in the Use of General Somatic Care among Individuals Treated for Severe Mental Disorders and the General Population in France. International Journal of Environmental Research and Public Health. 2020; 17(10):3367. https://doi.org/10.3390/ijerph17103367
Chicago/Turabian StyleGandré, Coralie, and Magali Coldefy. 2020. "Disparities in the Use of General Somatic Care among Individuals Treated for Severe Mental Disorders and the General Population in France" International Journal of Environmental Research and Public Health 17, no. 10: 3367. https://doi.org/10.3390/ijerph17103367