Influence of Risk of Drug–Drug Interactions and Time Availability on Patient Trust, Satisfaction, and Cooperation with Clinical Pharmacists

Abstract
:1. Introduction
2. Literature Review
2.1. Drug–Drug Interaction (DDI) Risk and Trust in Clinical Pharmacists
2.2. Time Availability and Trust in Clinical Pharmacists
2.3. Trust and Cooperation between Patient and Clinical Pharmacist
2.4. Trust and Satisfaction toward Clinical Pharmacists
2.5. Satisfaction and Cooperation between Patient and Clinical Pharmacist
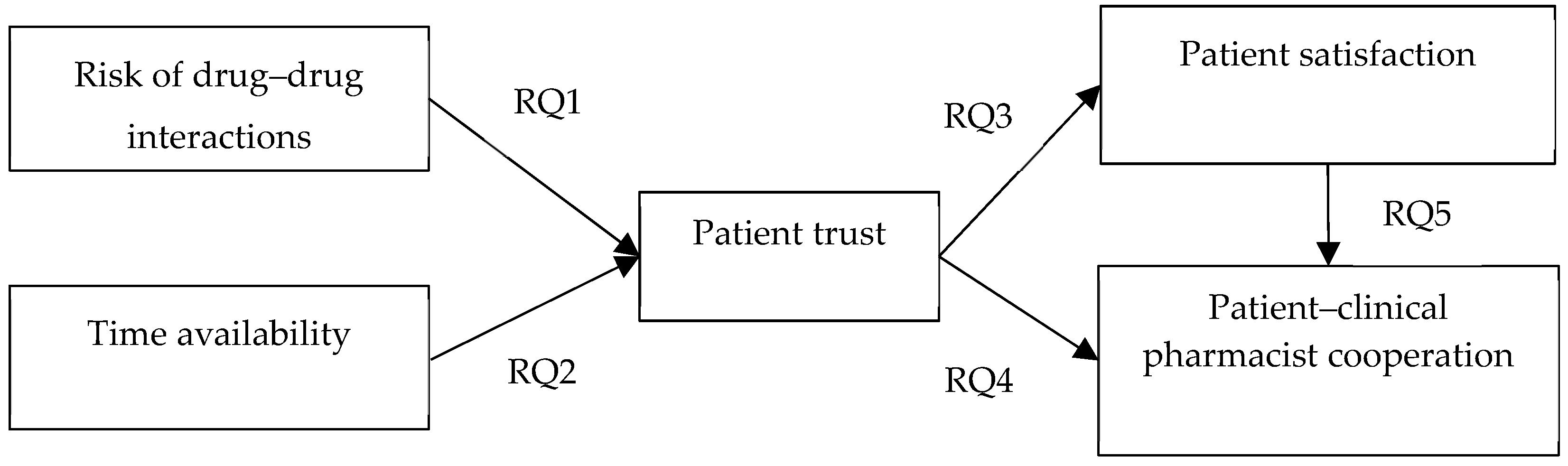
2.6. Research Questions
- RQ1: Does the risk of drug–drug interactions (DDIs) affect patient trust in clinical pharmacists?
- RQ2: Does time availability (communication time) affect patient trust in clinical pharmacists?
- RQ3: Does patient trust affect patient satisfaction toward clinical pharmacists?
- RQ4: Does patient’ trust affect cooperation between patients and clinical pharmacists?
- RQ5: Does patient satisfaction affect cooperation between patients and clinical pharmacists?
3. Methods
3.1. Sample and Data Collection
3.2. Measures
3.3. Analytical Method
4. Results
4.1. Descriptive Statistics
4.2. Confirmatory Factor Analysis
Reliability and Validity
4.3. Structural Equation Model
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Aparasu, R.; Pharm, R.; Aparasu, A. Clinically important potential drug-drug interactions in outpatient settings. Res. Soc. Adm. Pharm. 2007, 3, 426–437. [Google Scholar] [CrossRef]
- Herbert, K.; Urmie, J.; Newland, B. Prediction of pharmacist intention to provide Medi-care medication therapy management services using the theory of planned behavior. Res. Soc. Adm. Pharm. 2006, 2, 299–314. [Google Scholar] [CrossRef] [PubMed]
- Blake, K.; Madhavan, S.; Scott, V.; Meredith, B. Medication therapy management services in West Virginia: Pharmacists’ perceptions of educational and training needs. Res. Soc. Adm. Pharm. 2009, 5, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Chui, M.; Mott, D.; Maxwell, L. A qualitative assessment of a community pharmacy cognitive pharmaceutical services program, using a work system approach. Res. Soc. Adm. Pharm. 2012, 8, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Gupta, G.; Gelfand, J.; Lewis, J. Increased risk for demyelinating diseases in patients with inflammatory bowel disease. Gastroenterology 2005, 129, 819–826. [Google Scholar] [CrossRef]
- Tsai, K.; Chen, J.; Wen, C.; Kuo, H.; Lu, I.; Chiu, L. Medication adherence among geriatric outpatients prescribed multiple medications. Am. J. Geriatr. Pharmacother. 2012, 18, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Manias, E.; Williams, A.; Liew, D.; Rixon, S.; Braaf, S.; Finch, S. Effects of patient-, environment- and medication-related factors on high-alert medication incidents. Int. J. Qual. Health Care 2014, 26, 308–320. [Google Scholar] [CrossRef] [Green Version]
- Kinoshita, H.; Kobayashi, Y.; Fukuda, T. Duplicative medications in patients who visit multiple medical institutions among the insured of a corporate health insurance society in Japan. Health Policy 2008, 85, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Rollason, V.; Vogt, N. Reduction of poly pharmacy in the elderly a systematic review of the role of the pharmacist. Drugs Aging 2003, 20, 817–832. [Google Scholar] [CrossRef] [PubMed]
- Rivkin, A.; Yin, H. Evaluation of the role of the critical care pharmacist in identifying and avoiding or minimizing significant drug-drug interactions in medical intensive care patients. J. Crit. Care 2011, 2, e1–e6. [Google Scholar] [CrossRef]
- Carter, S.; Moles, R.; White, L.; Chen, T. Patients’ willingness to use a pharmacist-provided medication management service: The influence of outcome expectancies and communication efficacy. Res. Soc. Adm. Pharm. 2012, 8, 487–498. [Google Scholar] [CrossRef]
- Ngorsuraches, S. Development and validation of the patient trust in community pharmacists (TRUST-Ph) scale: Results from a study conducted in Thailand. Res. Soc. Adm. Pharm. 2007, 4, 272–283. [Google Scholar] [CrossRef]
- Ahituv, N.; Igbaria, M.; Sella, A. The effect of time pressure and completeness of information on decision making. J. Manag. Infor. Syst. 1998, 15, 153–172. [Google Scholar] [CrossRef]
- Janis, I. Groupthink Psychological Studies of Policy Decisions and Fiascoes; Houghton Mifflin: Boston, MA, USA, 1983. [Google Scholar]
- Iyer, E. Unplanned purchasing: Knowledge of shopping environment and time pressure. J. Retail. 1989, 65, 40–57. [Google Scholar]
- Svenson, L.; Edland, A.; Slovic, P. Choices and judgment of incompletely described decision alternatives under time pressure. Acta Psychol. 1990, 75, 153–169. [Google Scholar] [CrossRef]
- Payne, J.; Bettman, J.; Johnson, E. Adaptive strategy selection in decision making. J. Exp. Psychol. 1988, 14, 534–552. [Google Scholar] [CrossRef]
- Rajneesh, S.; Kent, B. The effects of time constraints on consumers’ judgments of prices and products. J. Consum. Res. 2003, 30, 92–104. [Google Scholar]
- Heikki, T.; Joseph, S.; Jeffrey, A. The effects of task complexity and time availability limitations on human performance in database query tasks. Int. J. Hum.-Comput. Stud. 2005, 62, 349–379. [Google Scholar]
- Caterinicchio, R. Testing plausible path models of interpersonal trust in patient-physician treatment relationships. Soc. Sci. Med. 1979, 13A, 81–99. [Google Scholar]
- Anderson, L.; Dedrick, R. Development of the trust in physician scale: a measure to assess interpersonal trust in patient-physician relationships. Psychol. Rep. 1990, 67, 1091–1100. [Google Scholar] [CrossRef] [PubMed]
- Dugan, E.; Trachtenberg, F.; Hall, M.A. Development of abbreviated measures to assess patient trust in a physician, a health insurer, and medical profession. BMC Health Serv. Res. 2005, 5, 1–7. [Google Scholar] [CrossRef]
- Alberta College of Pharmacists CoE. Healthy Albertans through Excellence in Pharmacy Practice. Available online: https://pharmacists.ab.ca/nCollege/default.aspx (accessed on 20 April 2015).
- Hall, M.; Dugan, E.; Zheng, B.; Mishra, A. Trust in physicians and medical institutions: What is it, can it be measured, and does it matter? Milbank Q. 2001, 79, 613–639. [Google Scholar] [CrossRef]
- Thom, D.; Hall, M.; Pawlson, L. Measuring patients’ trust in physicians when assessing quality of care. Qual. Care 2004, 23, 124–132. [Google Scholar] [CrossRef]
- Thom, D.; Kravitz, R.; Bell, R.; Krupat, E.; Azari, R. Patient trust in the physician: relationship to patient requests. Fam. Pract. 2002, 19, 476–483. [Google Scholar] [CrossRef] [Green Version]
- Verbeek, J.; de Boer, A.; van der Weide, W.; Piirainen, H.; Anema, J.; van Amstel, R. Patient satisfaction with occupational health physicians, development of a questionnaire. Occup. Environ. Med. 2005, 62, 119–123. [Google Scholar] [CrossRef] [Green Version]
- Pearson, S.; Raeke, L. Patients’ trust in physicians: Many theories, few measures, and little data. J. Gen. Intern. Med. 2000, 15, 509–513. [Google Scholar] [CrossRef]
- Crosby, L.A.; Evans, K.R.; Cowles, D. Relationship quality in services selling: An interpersonal influence perspective. J. Mark. 1990, 54, 68–81. [Google Scholar] [CrossRef]
- Homburg, C.; Giering, A. Personal characteristics as moderators of the relationship between customer satisfaction and loyalty—An empirical analysis. Psychol. Mark. 2001, 18, 43–66. [Google Scholar] [CrossRef]
- Lee, K.Y.; Huang, H.L.; Hsu, Y.C. Trust, satisfaction and commitment-on loyalty to international retail service brands. Asia Pac. Manag. Rev. 2007, 12, 161–169. [Google Scholar]
- Fang, Y.; Qureshi, I.; Sun, H.; McCole, P.; Ramsey, E.; Lim, K.H. Trust, satisfaction, and online repurchase intention: the moderating role of perceived effectiveness of ecommerce institutional mechanisms. MIS Q. 2014, 38, 407–427. [Google Scholar] [CrossRef]
- Donnally, C.J., III; Perez, J.R.; Cade II, W.H.; Munoz, J.; Page, C.L.; Best, T.M.; Kaplan, L.D.; Baraga, M.G. Novel approach to improve patient satisfaction in the outpatient clinic setting. J. Clin. Orthop. Trauma 2019, 10, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Garman, A.N.; Garcia, J.; Hargreaves, M. Patient satisfaction as a predictor of return-to-provider behavior: analysis and assessment of financial implications. Qual. Manag. Healthcare 2004, 13, 75–80. [Google Scholar] [CrossRef]
- De Paula, D.A.G.; Piatti, N.C.T.P.; Costa, L.M.; Chiavegato, L.D. Satisfaction levels with physical therapy in hospitalized patients. Braz. J. Phys. Ther. 2019. [Google Scholar] [CrossRef] [PubMed]
- Khomami, H.M. The dataset for relationship between the nurses to patients ratio and patients satisfaction with nursing care. Data Brief 2018, 21, 2149–2154. [Google Scholar] [CrossRef] [PubMed]
- Conti, A.A.; Humphris, G.M. Patient centred consultation, satisfaction and young patients: a cross-country analysis. Patient Educ. Couns. 2019, 102, 782–789. [Google Scholar] [CrossRef]
- Weingarten, N.; Issa, N.; Posluszny, J. Fellow-led SICU morbidity and mortality conferences address patient safety, quality improvement, interpersonal cooperation and ACGME milestones. Am. J. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Bosak, M.; Slowik, A.; Iwanska, A.; Lipinska, M.; Turaj, W. Co-medication and potential drug interactions among patients with epilepsy. Seizure 2019, 66, 47–52. [Google Scholar] [CrossRef]
- Gendelman, O.; Amital, H.; Bar-On, Y.; Shor, D.B.; Amital, D.; Tiosono, S.; Shalev, V.; Chodick, G.; Weitzman, D. Time to diagnosis of fibromyalgia and factors associated with delayed diagnosis in primary care. Best Pract. Res. Clin. Rheumatol. 2019. [Google Scholar] [CrossRef]
- Pozsgai, E.; Busa, C.; Fodor, D.; Bellyei, S.; Csikos, A. Wait times to diagnosis and treatment in patients with colorectal cancer in Hungary. Cancer Epidemiol. 2019, 59, 244–248. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; The Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Frequency | Percent |
|---|---|---|
| Gender | ||
| Female | 669 | 90.3% |
| Male | 72 | 9.7% |
| Age | ||
| Under 20 | 6 | 0.8% |
| 21–30 | 111 | 15.0% |
| 31–40 | 363 | 49.0% |
| 41–50 | 222 | 30.0% |
| 51 or above | 39 | 5.3% |
| Education | ||
| High school or below | 579 | 78.1% |
| College or University | 123 | 16.6% |
| Graduate or above | 39 | 5.3% |
| Marital status | ||
| Married | 696 | 93.9% |
| Not married | 45 | 6.1% |
| Income | ||
| Under 20,000 NT | 81 | 10.9% |
| 20,000–under 40,000 NT | 480 | 64.8% |
| 40,000 NT or above | 180 | 24.3% |
| Hospitalization or not | ||
| Yes | 489 | 66.0% |
| No | 242 | 34.0% |
| Variable | Mean | SD | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|---|---|
| 1. Risk of drug–drug interactions | 4.05 | 0.58 | 0.96 | ||||
| 2. Time availability | 4.03 | 0.55 | 0.17 ** | 0.94 | |||
| 3. Patient trust | 3.72 | 0.57 | 0.25 ** | 0.38 ** | 0.92 | ||
| 4. Patient satisfaction | 3.81 | 0.55 | 0.50 ** | 0.48 ** | 0.48 ** | 0.93 | |
| 5. Patient–clinical pharmacist cooperation | 3.73 | 0.61 | 0.35 ** | 0.52 ** | 0.37 ** | 0.56 ** | 0.94 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, Y.-C.; Dang, V.T.; Yen, H.-Y.; Lai, K.-M. Influence of Risk of Drug–Drug Interactions and Time Availability on Patient Trust, Satisfaction, and Cooperation with Clinical Pharmacists. Int. J. Environ. Res. Public Health 2019, 16, 1566. https://doi.org/10.3390/ijerph16091566
Chou Y-C, Dang VT, Yen H-Y, Lai K-M. Influence of Risk of Drug–Drug Interactions and Time Availability on Patient Trust, Satisfaction, and Cooperation with Clinical Pharmacists. International Journal of Environmental Research and Public Health. 2019; 16(9):1566. https://doi.org/10.3390/ijerph16091566
Chicago/Turabian StyleChou, Ying-Chyi, Van Thac Dang, Hsin-Yi Yen, and Kuan-Ming Lai. 2019. "Influence of Risk of Drug–Drug Interactions and Time Availability on Patient Trust, Satisfaction, and Cooperation with Clinical Pharmacists" International Journal of Environmental Research and Public Health 16, no. 9: 1566. https://doi.org/10.3390/ijerph16091566