Relationships between Social Capital, Social Capital Satisfaction, Self-Esteem, and Depression among Elderly Urban Residents: Analysis of Secondary Survey Data


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Research Participants
2.2. Instruments
2.2.1. Depression
2.2.2. Social Capital
2.2.3. Social Capital Satisfaction
2.2.4. Self-Esteem
2.3. Statistical Analysis
3. Results
3.1. Sociodemographic Differences in Social Capital Satisfaction, Self-Esteem, and Depression
3.2. Measurement Model
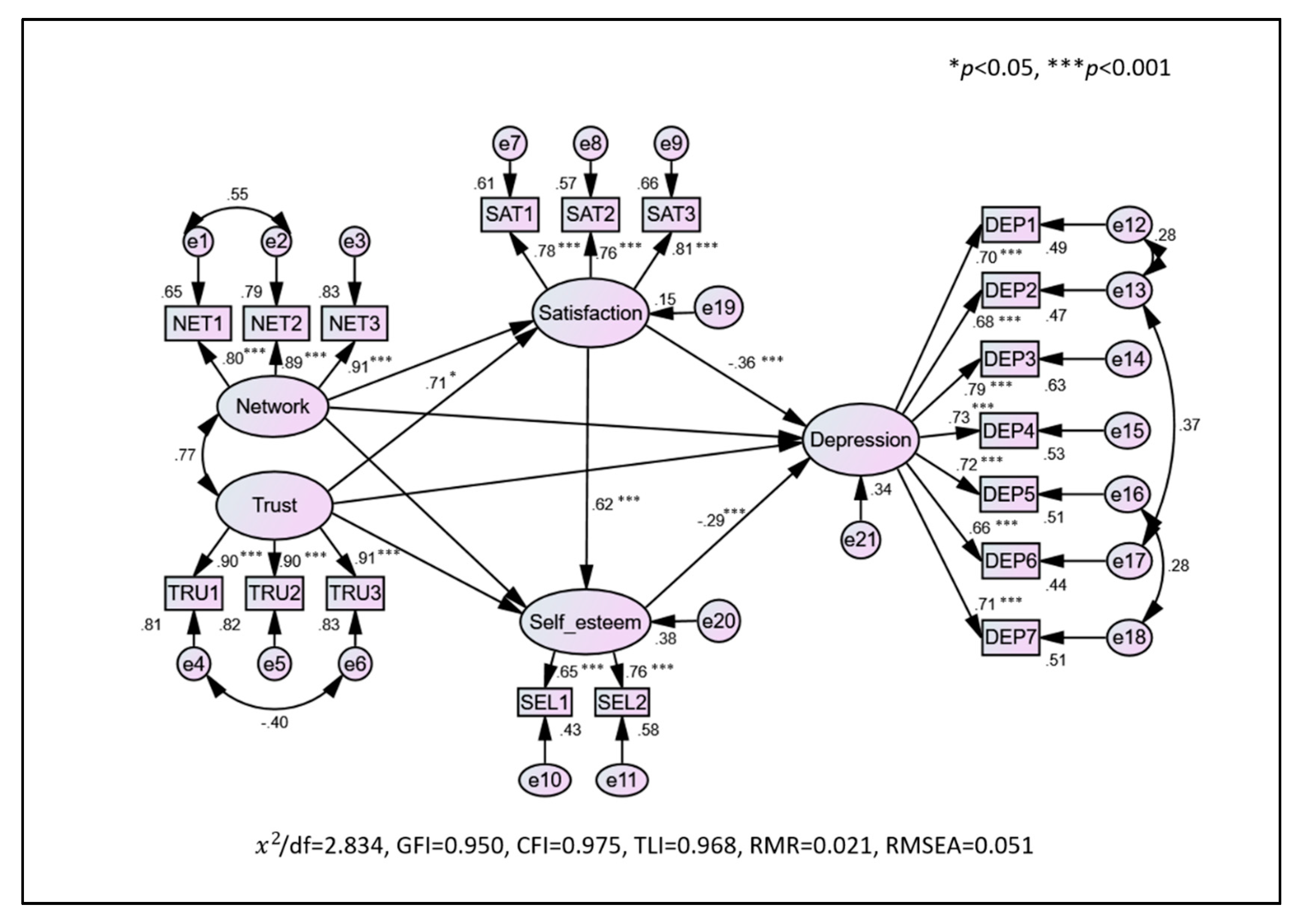
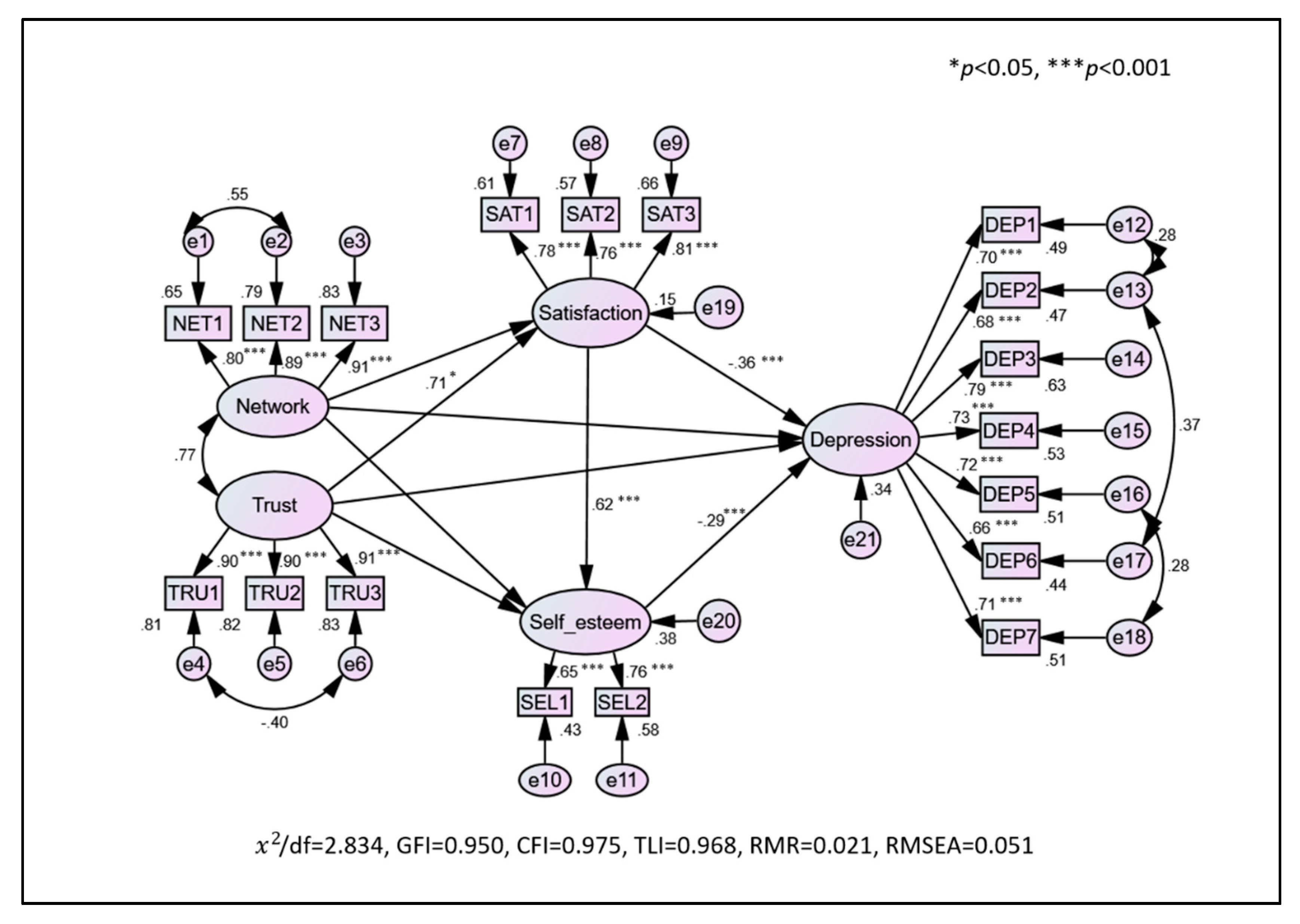
3.3. Structural Model
3.4. Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| DEP2 | DEP3 | DEP4 | DEP5 | DEP6 | DEP7 | DEP8 | DEP9 | DEP10 | DEP11 | |
|---|---|---|---|---|---|---|---|---|---|---|
| DEP1 | −0.629 ** | 0.551 ** | 0.537 ** | 0.486 ** | 0.484 ** | −0.479 ** | 0.376 ** | 0.334 ** | 0.295 ** | 0.296 ** |
| SEL2 | SEL3 | SEL4 | SEL5 | SEL6 | SEL7 | SEL8 | SEL9 | SEL10 | |
|---|---|---|---|---|---|---|---|---|---|
| SEL1 | 0.496 ** | 0.341 ** | 0.382 ** | 0.310 ** | 0.374 ** | 0.312 ** | 0.219 ** | 0.388 ** | 0.168 ** |
References
- Okkels, N.; Kristiansen, C.B.; Munk-Jørgensen, P.; Sartorius, N. Urban mental health: Challenges and perspectives. Curr. Opin. Psychiatry 2018, 31, 258–264. [Google Scholar] [CrossRef]
- Korean Statistical Information Service Urban Population Status. 2017. Available online: http://kosis.kr (accessed on 7 August 2018).
- Korea Institute for Health and Social Affairs. 2017 Survey of the Elderly; KIHASA: Sejong, Korea, 2017; pp. 29–62. ISBN 1113520000. [Google Scholar]
- Tiemeier, H. Biological risk factors for late life depression. Eur. J. Epidemiol. 2003, 18, 745–750. [Google Scholar] [CrossRef]
- Lee, H.J.; Son, S.A. Psychological and Physical Effects of 10 Weeks Urban Forest Therapy Program on Dementia Prevention in Low-Income Elderly Living Alone. J. People Plants Environ. 2018, 21, 557–564. [Google Scholar] [CrossRef]
- Deckers, K.; van Boxtel, M.P.J.; Schiepers, O.J.G.; de Vugt, M.; Muñoz Sánchez, J.L.; Anstey, K.J.; Brayne, C.; Dartigues, J.-F.; Engedal, K.; Kivipelto, M.; et al. Target risk factors for dementia prevention: A systematic review and Delphi consensus study on the evidence from observational studies. Int. J. Geriatr. Psychiatry 2015, 30, 234–246. [Google Scholar] [CrossRef] [PubMed]
- Langa, K.M. Is the risk of Alzheimer’s disease and dementia declining? Alzheimers. Res. Ther. 2015, 7, 34. [Google Scholar] [CrossRef] [PubMed]
- Min, K.B.; Kim, H.J.; Kim, H.J.; Min, J.Y. Parks and green areas and the risk for depression and suicidal indicators. Int. J. Public Health 2017, 62, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Wimo, A.; Guerchet, M.; Ali, G.-C.; Wu, Y.-T.; Prina, A.M.; Winblad, B.; Jönsson, L.; Liu, Z.; Prince, M. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimer’s Dement. 2017, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mental health action and innovation: The evidence-based case for investment. In Investing in Mental Health: Evidence for Action; World Health Organization: Geneva, Switzerland, 2013; pp. 14–22. ISBN 9789241564618. [Google Scholar]
- Girardi, P.; Pompili, M.; Innamorati, M.; Mancini, M.; Serafini, G.; Mazzarini, L.; Del Casale, A.; Tatarelli, R.; Baldessarini, R.J. Duloxetine in acute major depression: Review of comparisons to placebo and standard antidepressants using dissimilar methods. Hum. Psychopharmacol. Clin. Exp. 2009, 24, 177–190. [Google Scholar] [CrossRef]
- Serafini, G.; Pompili, M.; Belvederi Murri, M.; Respino, M.; Ghio, L.; Girardi, P.; Fitzgerald, P.B.; Amore, M. The effects of repetitive transcranial magnetic stimulation on cognitive performance in treatment-resistant depression. A systematic review. Neuropsychobiology 2015, 71, 125–139. [Google Scholar] [CrossRef]
- Kerling, A.; Tegtbur, U.; Gützlaff, E.; Kück, M.; Borchert, L.; Ates, Z.; von Bohlen, A.; Frieling, H.; Hüper, K.; Hartung, D.; et al. Effects of adjunctive exercise on physiological and psychological parameters in depression: A randomized pilot trial. J. Affect. Disord. 2015, 177, 1–6. [Google Scholar] [CrossRef]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; et al. Physiological and psychological effects of forest therapy on middle-aged males with high-normal blood pressure. Int. J. Environ. Res. Public Health 2015, 12, 2532–2542. [Google Scholar] [CrossRef]
- Mingo, C.A.; Martin, K.R.; Shreffler, J.; Schoster, B.; Callahan, L.F. Individual and community socioeconomic status: Impact on mental health in individuals with arthritis. Arthritis 2014, 2014, 256498. [Google Scholar] [CrossRef]
- Murata, C.; Saito, T.; Saito, M.; Kondo, K.; Murata, C.; Saito, T.; Saito, M.; Kondo, K. The Association between Social Support and Incident Dementia: A 10-Year Follow-Up Study in Japan. Int. J. Environ. Res. Public Health 2019, 16, 239. [Google Scholar] [CrossRef]
- Padayachey, U.; Ramlall, S.; Chipps, J. Depression in older adults: Prevalence and risk factors in a primary health care sample. South Afr. Fam. Pract. 2017, 59, 61–66. [Google Scholar] [CrossRef]
- Lee, H.J.; Lee, D.K. Do Sociodemographic Factors and Urban Green Space Affect Mental Health Outcomes Among the Urban Elderly Population? Int. J. Environ. Res. Public Health 2019, 16, 789. [Google Scholar] [CrossRef]
- Kong, F.; Xu, L.; Kong, M.; Li, S.; Zhou, C.; Li, J.; Sun, L.; Qin, W.; Kong, F.; Xu, L.; et al. The Relationship between Socioeconomic Status, Mental Health, and Need for Long-Term Services and Supports among the Chinese Elderly in Shandong Province—A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 526. [Google Scholar] [CrossRef]
- Lee, H.-Y.; Yu, C.-P.; Wu, C.-D.; Pan, W.-C.; Lee, H.-Y.; Yu, C.-P.; Wu, C.-D.; Pan, W.-C. The Effect of Leisure Activity Diversity and Exercise Time on the Prevention of Depression in the Middle-Aged and Elderly Residents of Taiwan. Int. J. Environ. Res. Public Health 2018, 15, 654. [Google Scholar] [CrossRef]
- Cohen-Cline, H.; Turkheimer, E.; Duncan, G.E. Access to green space, physical activity and mental health: A twin study. J. Epidemiol. Community Health 2015, 69, 523–529. [Google Scholar] [CrossRef]
- Orstad, S.L.; McDonough, M.H.; James, P.; Klenosky, D.B.; Laden, F.; Mattson, M.; Troped, P.J. Neighborhood walkability and physical activity among older women: Tests of mediation by perceptions and moderation by depressive symptoms. Prev. Med. (Baltim) 2018, 116, 60–67. [Google Scholar] [CrossRef]
- Dadvand, P.; Bartoll, X.; Basagaña, X.; Dalmau-Bueno, A.; Martinez, D.; Ambros, A.; Cirach, M.; Triguero-Mas, M.; Gascon, M.; Borrell, C.; et al. Green spaces and General Health: Roles of mental health status, social support, and physical activity. Environ. Int. 2016, 91, 161–167. [Google Scholar] [CrossRef]
- Kim, J.; Song, Y.-L.-A. Social Support: An Effective Resource for Reducing the Disparities in Depression across Socioeconomic Strata. Korean J. Sociol. 2006, 45, 175–197. [Google Scholar]
- Kim, D.B.; Sohn, U.S. A Meta-analysis of the Variables Related to Depression in Elderly. J. Korean Gerontol. Soc. 2005, 25, 167–187. [Google Scholar]
- Hassanzadeh, J.; Asadi-lari, M.; Baghbanian, A.; Ghaem, H. Association between social capital, health-related quality of life, and mental health: A structural-equation modeling approach. Croat. Med. J. 2016, 57, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Yoo, C.; Lee, S. Neighborhood Built Environments Affecting Social Capital and Social Sustainability in Seoul, Korea. Sustainability 2016, 8, 1346. [Google Scholar] [CrossRef]
- Coleman, J.S. Social Capital in the Creation of Human Capital. Am. J. Sociol. 1988, 94, S95–S120. [Google Scholar] [CrossRef]
- Putnam, R.D.; Leonardi, R.; Nanetti, R. Social capital and institutional success. In Making Democracy Work: Civic Traditions in Modern Italy; Princeton University Press: Princeton, NJ, USA, 1993; pp. 167–170. ISBN 140082074X. [Google Scholar]
- Cao, W.; Li, L.; Zhou, X.; Zhou, C. Social capital and depression: Evidence from urban elderly in China. Aging Ment. Health 2015, 19, 418–429. [Google Scholar] [CrossRef]
- Pollack, C.E.; von dem Knesebeck, O. Social capital and health among the aged: Comparisons between the United States and Germany. Health Place 2004, 10, 383–391. [Google Scholar] [CrossRef]
- House, J.S.; Landis, K.R.; Umberson, D. Social relationships and health. Science 1988, 241, 540–545. [Google Scholar] [CrossRef]
- Teo, A.R.; Choi, H.; Valenstein, M. Social Relationships and Depression: Ten-Year Follow-Up from a Nationally Representative Study. PLoS ONE 2013, 8, e62396. [Google Scholar] [CrossRef]
- Evenson, K.R.; Jones, S.A.; Holliday, K.M.; Cohen, D.A.; McKenzie, T.L. Park characteristics, use, and physical activity: A review of studies using SOPARC (System for Observing Play and Recreation in Communities). Prev. Med. (Baltim) 2016, 86, 153–166. [Google Scholar] [CrossRef]
- Liu, L.; Gou, Z.; Zuo, J. Social support mediates loneliness and depression in elderly people. J. Health Psychol. 2016, 21, 750–758. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.; Heim, D.; Hunter, S.; Ellaway, A. Health & Place The relative infl uence of neighbourhood incivilities, cognitive social capital, club membership and individual characteristics on positive mental health. Health Place 2014, 28, 187–193. [Google Scholar] [CrossRef]
- Han, S. Social capital and perceived stress: The role of social context. J. Affect. Disord. 2019, 250, 186–192. [Google Scholar] [CrossRef]
- Kim, B.J.; Linton, K.F.; Lum, W. Social capital and life satisfaction among Chinese and Korean elderly immigrants. J. Soc. Work 2015, 15, 87–100. [Google Scholar] [CrossRef]
- Bjørnskov, C. The happy few: Cross-country evidence on social capital and life satisfaction. Kyklos 2003, 56, 3–16. [Google Scholar] [CrossRef]
- Pavot, W.; Diener, E.; Colvin, C.R.; Sandvik, E. Further validation of satesfaction with life scale.pdf. J. Personal. Assess. 1991, 57, 149–161. [Google Scholar] [CrossRef]
- Kim, K.-H.; Kim, J.-H. The effects of elderly depression on life satisfaction. Fam. Cult. 2008, 20, 95–116. [Google Scholar]
- Korea Institute for Health and Social Affairs (KIHASA) 12th Korea Welfare Panel Study: User’s Guide. Available online: https://www.koweps.re.kr:442/eng/data/guide/list.do (accessed on 25 February 2019).
- Korea Institute for Health and Social Affairs (KIHASA) 12th Korea Welfare Panel Study. Available online: https://www.koweps.re.kr:442/eng/main.do (accessed on 25 February 2019).
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Gellis, Z.D. Assessment of a brief CES-D measure for depression in homebound medically ill older adults. J. Gerontol. Soc. Work 2010, 53, 289–303. [Google Scholar] [CrossRef] [PubMed]
- Chon, K.K.; Rhee, M.K. Preliminary Development of Korean Version of CES-D. Korean J. Clin. Psychol. 1992, 11, 65–76. [Google Scholar]
- Choi, M.-Y.; Kwak, H.-K.; Park, H.-S. The Effect of Community Social Capital on the Elderly’s Subjective Quality of Life: Focusing on the Mediating Effect of the Elderly Depression Mi-Young. J. Welf. Aged Vol. 2014, 66, 307–328. [Google Scholar]
- Cho, D.-H.; Yeo, C.-W.; Seo, Y.-H. Estimation of Life Satisfaction and Development of Welfare Policy using Welfare Panel Data. J. Korean Political Sci. Assoc. 2018, 26, 177–195. [Google Scholar]
- Rosenberg, M. The measurment of self-esteem. In Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965; pp. 16–36. ISBN 1400876133. [Google Scholar]
- Medsker, G.J.; Williams, L.J.; Holahan, P.J. A Review of Current Practices for Evaluating Causal Models in Organizational Behavior and Human Resources Management Research. J. Manage. 1994, 20, 439–464. [Google Scholar] [CrossRef]
- Shrout, P.E.; Bolger, N. Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychol. Methods 2002, 7, 422–445. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative Ways of Assessing Model Fit. In Testing Structural Equation Models; Bollen, K.A., Long, J.S., Eds.; Sage Publications: Newbury Park, CA, USA, 1993; pp. 136–139. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. SEM: An Introduction. In Multivariate Data Analysis: A Global Perspective; Pearson Prentice Hall: Upper New Jersey River, NJ, USA, 2010; pp. 664–672. [Google Scholar]
- Hutchinson, D.B.; Singh, J.; Svensson, G.; Mysen, T. Towards a model of conscientious corporate brands: A Canadian study. J. Bus. Ind. Mark. 2013, 28, 687–695. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Lockwood, C.M.; Williams, J. Confidence Limits for the Indirect Effect: Distribution of the Product and Resampling Methods. Multivar. Behav. Res. 2004, 39, 99–128. [Google Scholar] [CrossRef]
- Borge, L.-E.; Rattsø, J. Understanding generational conflict. In Young and Old Competing for Public Welfare Services; CESifo Working Paper Series No. 2223. CESifo Group: Munich, Germany, 2008; pp. 3–4. [Google Scholar]
- Walker, A.; Martimo, K. Ageing and intergenerational relations in Britain. In Comparing Social Policies: Exploring New Perspectives in Britain and Japan; The Policy Press: Bristol, UK, 2003; p. 49. [Google Scholar]
- Larson, R. Building Intergenerational Bonds Through the Arts. Generations 2006, 30, 38–41. [Google Scholar]
- Pinquart, M.; Sörensen, S. Influences of socioeconomic status, social network, and competence on subjective well-being in later life: A meta-analysis. Psychol. Aging 2000, 15, 187–224. [Google Scholar] [CrossRef]
- Kaplan, M.S. School-Based Intergenerational Programs; UNESCO Institute for Education: Hamburg, Germany, 2001. [Google Scholar]
- Mannion, G. Intergenerational Education and Learning: We Are in a New Place. In Families, Intergenerationality, and Peer Group Relations; Springer: Singapore, 2018; pp. 307–327. [Google Scholar]
- Daatland, S.O.; Lowenstein, A. Intergenerational solidarity and the family-welfare state balance. Eur. J. Ageing 2005, 2, 174–182. [Google Scholar] [CrossRef]
- Lowenstein, A. Intergenerational family relations and social support. Z. Gerontol. Geriatr. 1999, 32, 398–406. [Google Scholar] [CrossRef]
- Kropf, N.P.; Burnette, D. Grandparents as family caregivers: Lessons for intergenerational education. Educ. Gerontol. 2003, 29, 361–372. [Google Scholar] [CrossRef]
- Mamplekou, E.; Bountziouka, V.; Psaltopoulou, T.; Zeimbekis, A.; Tsakoundakis, N.; Papaerakleous, N.; Gotsis, E.; Metallinos, G.; Pounis, G.; Polychronopoulos, E.; et al. Urban environment, physical inactivity and unhealthy dietary habits correlate to depression among elderly living in eastern Mediterranean islands: The MEDIS (MEDiterranean ISlands elderly) study. J. Nutr. Health Aging 2010, 14, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.M.; Mak, K.K.; Watanabe, H.; Jeong, J.; Kim, D.; Bahar, N.; Ramos, M.; Chen, S.H.; Cheng, C. The mediating role of Internet addiction in depression, social anxiety, and psychosocial well-being among adolescents in six Asian countries: A structural equation modelling approach. Public Health 2015, 129, 1224–1236. [Google Scholar] [CrossRef]
- Kim, Y.; Paik, J. The Effects of Family Conflict, Social Support and Self-Esteem on Life Satisfaction of the Aged. J. Digit. Converg. 2016, 14, 279–287. [Google Scholar] [CrossRef]
- Fox, K.R. The influence of physical activity on mental well-being. Public Health Nutr. 1999, 2, 411–418. [Google Scholar] [CrossRef]
- Simpson, J.A. Psychological foundations of trust. Curr. Dir. Psychol. Sci. 2007, 16, 264–268. [Google Scholar] [CrossRef]
- Li, T.; Fung, H.H. Age Differences in Trust: An Investigation Across 38 Countries. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2013, 68, 347–355. [Google Scholar] [CrossRef]
- Rempel, J.K.; Holmes, J.G.; Zanna, M.P. Trust in Close Relationships. J. Pers. Soc. Psychol. 1985, 49, 95–112. [Google Scholar] [CrossRef]
- Chow, W.S.; Chan, L.S. Social network, social trust and shared goals in organizational knowledge sharing. Inf. Manag. 2008, 45, 458–465. [Google Scholar] [CrossRef]
- Chu, H.S.; Tak, Y.R. Effects of Social Capital on Subjective Health in the Community Indwelling Elderly. J. Korean Acad. Community Health Nurs. 2018, 29, 184. [Google Scholar] [CrossRef]
- Lee, J.B. Social Capital in the Aged’s Life Long Education; Gacheon University: Seongnam, Korea, 2016. [Google Scholar]
- Oh, J.-H. Social Bonds and the Migration Intentions of Elderly Urban Residents: The Mediating Effect of Residential Satisfaction. Popul. Res. Policy Rev. 2003, 22, 127–146. [Google Scholar] [CrossRef]
- Lee, H.J.; Son, S.A. Qualitative Assessment of Experience on Urban Forest Therapy Program for Preventing Dementia of the Elderly Living Alone in Low-Income Class. J. People Plants Environ. 2018, 21, 565–574. [Google Scholar] [CrossRef]
| Latent Variable | Definition | Observed Variables | Categories |
|---|---|---|---|
| Depression | Depressive symptomatology felt in daily life during the past week | Poor appetite | (1) Extremely rarely (2) Rarely (3) Sometimes (4) Most of the time |
| Doing well | |||
| Depressed | |||
| Burden | |||
| Lonely | |||
| Happiness | |||
| Sadness | |||
| Network | Subjective recognition of the quantitative social network | Who can help in an emergency | |
| Who can make one comfortable | |||
| Who can share in joy and sorrow | |||
| Trust | Confidence in social relationships | Can get help | (1) Strongly disagree (2) Disagree (3) Neither (4) Agree (5) Strongly agree |
| Can depend on others when in trouble | |||
| Can talk about problems | |||
| Satisfaction | The extent to which an individual feels satisfaction | Satisfaction with social relationships | |
| Satisfaction with leisure | |||
| Satisfaction as a whole | |||
| Self-esteem | The extent to which an individual’s respects and approves of himself/herself | Positive attitude toward oneself | (1) Strongly disagree (2) Disagree (3) Agree (4) Strongly agree |
| Satisfaction with oneself |
| Sociodemographic Group | N | % | Satisfaction | Self-Esteem | Depression |
|---|---|---|---|---|---|
| M ± SD | M ± SD | M ± SD | |||
| Sex | |||||
| Men | 295 | 42.1 | 9.98 ± 1.87 | 4.90 ± 1.24 | 15.82 ± 5.98 |
| Women | 406 | 57.9 | 9.98 ± 1.92 | 4.78 ± 1.24 | 18.59 ± 6.79 |
| χ2 (p) | 0.13 (0.99) | 7.61 (0.27) | 31.35 (0.051) | ||
| Age group | |||||
| 65–70 | 206 | 29.4 | 9.93 ± 1.83 | 4.74 ± 1.21 | 10.76 ± 3.84 |
| 71–75 | 198 | 28.2 | 10.22 ± 1.85 | 4.96 ± 1.29 | 11.59 ± 4.77 |
| 76–80 | 198 | 28.2 | 9.92 ± 1.97 | 4.78 ± 1.27 | 11.46 ± 4.28 |
| >80 | 99 | 14.1 | 9.72 ± 1.95 | 4.83 ± 1.13 | 12.61 ± 4.39 |
| χ2 (p) | 45.47 (0.13) | 11.15 (0.89) | 64.68 (0.32) | ||
| Educational level | |||||
| <Primary school | 494 | 70.5 | 9.92 ± 1.91 | 4.78 ± 1.24 | 11.69 ± 4.32 |
| Middle or high school | 181 | 25.8 | 10.03 ± 1.91 | 4.91 ± 1.25 | 11.08 ± 4.50 |
| >College | 26 | 3.7 | 10.73 ± 1.40 | 5.23 ± 1.18 | 9.58 ± 3.00 |
| χ2 (p) | 20.46 (0.67) | 17.00 (0.15) | 28.12 (0.92) | ||
| Household type | |||||
| Solitary | 245 | 35 | 9.76 ± 1.92 | 4.71 ± 1.18 | 12.58 ± 4.62 |
| Elderly spouse | 453 | 64.6 | 10.12 ± 1.85 | 4.89 ± 1.27 | 10.81 ± 4.00 |
| Multi-generation | 3 | 0.4 | 7.33 ± 3.21 | 4.33 ± 1.53 | 17.00 ± 9.85 |
| χ2 (p) | 100.78 (0.00 **) | 9.38 (0.67) | 176.13 (0.00 **) | ||
| Health status | |||||
| Good | 289 | 41.2 | 10.45 ± 1.65 | 5.16 ± 1.24 | 10.32 ± 3.71 |
| Bad | 412 | 58.8 | 9.65 ± 1.99 | 4.60 ± 1.19 | 12.25 ± 4.59 |
| χ2 (p) | 42.38 (0.00 **) | 41.00 (0.00 **) | 51.34 (0.00 **) | ||
| Income status | |||||
| Low-income class | 509 | 72.6 | 9.78 ± 1.95 | 4.72 ± 1.24 | 11.88 ± 4.59 |
| Middle class | 192 | 27.4 | 10.50 ± 1.63 | 5.11 ± 1.21 | 10.32 ± 3.38 |
| χ2 (p) | 27.15 (0.01 *) | 20.68 (0.00 **) | 39.59 (0.01 *) | ||
| Latent Variable | Item | Convergent Validity | ||||
|---|---|---|---|---|---|---|
| λ | OE. | CR | AVE | |||
| Social Capital | Network | NET1 | 0.80 | 0.38 | 0.90 | 0.75 |
| NET2 | 0.89 | 0.22 | ||||
| NET3 | 0.91 | 0.17 | ||||
| Trust | TRU1 | 0.90 | 0.18 | 0.93 | 0.82 | |
| TRU2 | 0.90 | 0.18 | ||||
| TRU3 | 0.91 | 0.17 | ||||
| Satisfaction | SAT1 | 0.78 | 0.21 | 0.90 | 0.75 | |
| SAT2 | 0.76 | 0.27 | ||||
| SAT3 | 0.82 | 0.16 | ||||
| Self-esteem | SEL1 | 0.65 | 0.24 | 0.80 | 0.67 | |
| SEL2 | 0.76 | 0.26 | ||||
| Depression | DEP1 | 0.70 | 0.36 | 0.92 | 0.61 | |
| DEP2 | 0.68 | 0.39 | ||||
| DEP3 | 0.79 | 0.20 | ||||
| DEP4 | 0.73 | 0.38 | ||||
| DEP5 | 0.72 | 0.27 | ||||
| DEP6 | 0.66 | 0.48 | ||||
| DEP7 | 0.71 | 0.20 | ||||
| Variable | Social Capital | Satisfaction | Self-Esteem | Depression | ||
|---|---|---|---|---|---|---|
| Network | Trust | |||||
| Social capital | Network | 0.75 | ||||
| Trust | 0.59 | 0.82 | ||||
| Social capital satisfaction | 0.17 | 0.15 | 0.75 | |||
| Self-esteem | 0.08 | 0.07 | 0.39 | 0.67 | ||
| Depression | 0.05 | 0.05 | 0.29 | 0.26 | 0.61 | |
| Variable | Total (Direct, Indirect) | |||
|---|---|---|---|---|
| Trust | Network | Satisfaction | Self-Esteem | |
| Social capital satisfaction | 0.71 * (0.71 *, 0.00) | −0.31 (−0.31, 0.00) | ||
| Self-esteem | 0.80 (0.36, 0.44) | −0.53 (−0.34, −0.19) | 0.62 ** (0.62 **, 0.00) | |
| Depression | −0.44 (0.04, −0.49 *) | 0.22 (−0.04, 0.27) | −0.54 ** (−0.36 **, −0.18 **) | −0.29 ** (−0.29 **, 0.00) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.J.; Lee, D.K.; Song, W. Relationships between Social Capital, Social Capital Satisfaction, Self-Esteem, and Depression among Elderly Urban Residents: Analysis of Secondary Survey Data. Int. J. Environ. Res. Public Health 2019, 16, 1445. https://doi.org/10.3390/ijerph16081445
Lee HJ, Lee DK, Song W. Relationships between Social Capital, Social Capital Satisfaction, Self-Esteem, and Depression among Elderly Urban Residents: Analysis of Secondary Survey Data. International Journal of Environmental Research and Public Health. 2019; 16(8):1445. https://doi.org/10.3390/ijerph16081445
Chicago/Turabian StyleLee, Hyun Jin, Dong Kun Lee, and Wonkyong Song. 2019. "Relationships between Social Capital, Social Capital Satisfaction, Self-Esteem, and Depression among Elderly Urban Residents: Analysis of Secondary Survey Data" International Journal of Environmental Research and Public Health 16, no. 8: 1445. https://doi.org/10.3390/ijerph16081445