Identifying Areas with Disproportionate Local Health Department Services Relative to Opioid Overdose, HIV and Hepatitis C Diagnosis Rates: A Study of Rural Illinois

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
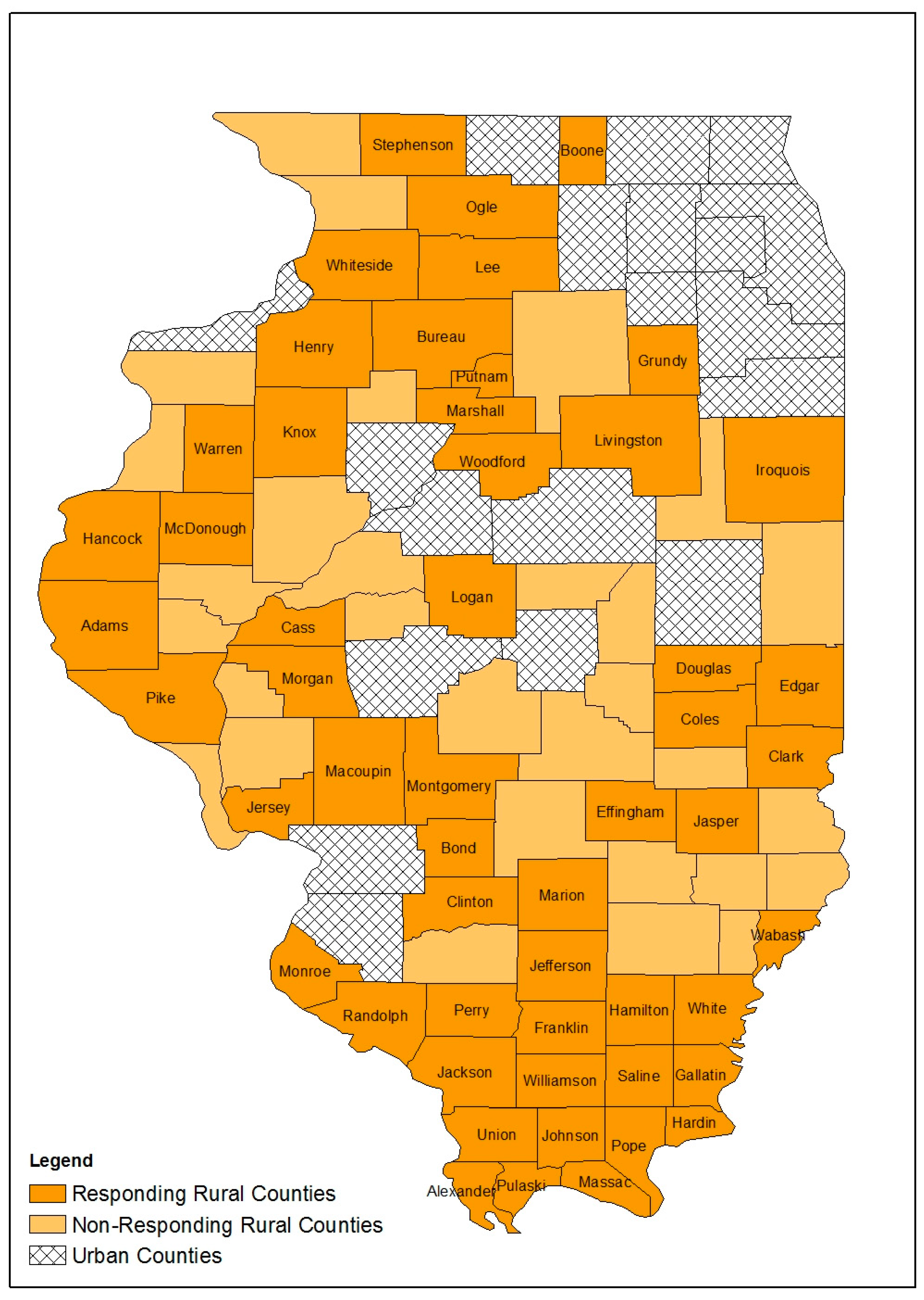
2.1. Overview
2.2. Local Health Department (LHD) Service Provision Survey
2.3. Survey Analysis
2.4. Disease Surveillance Data
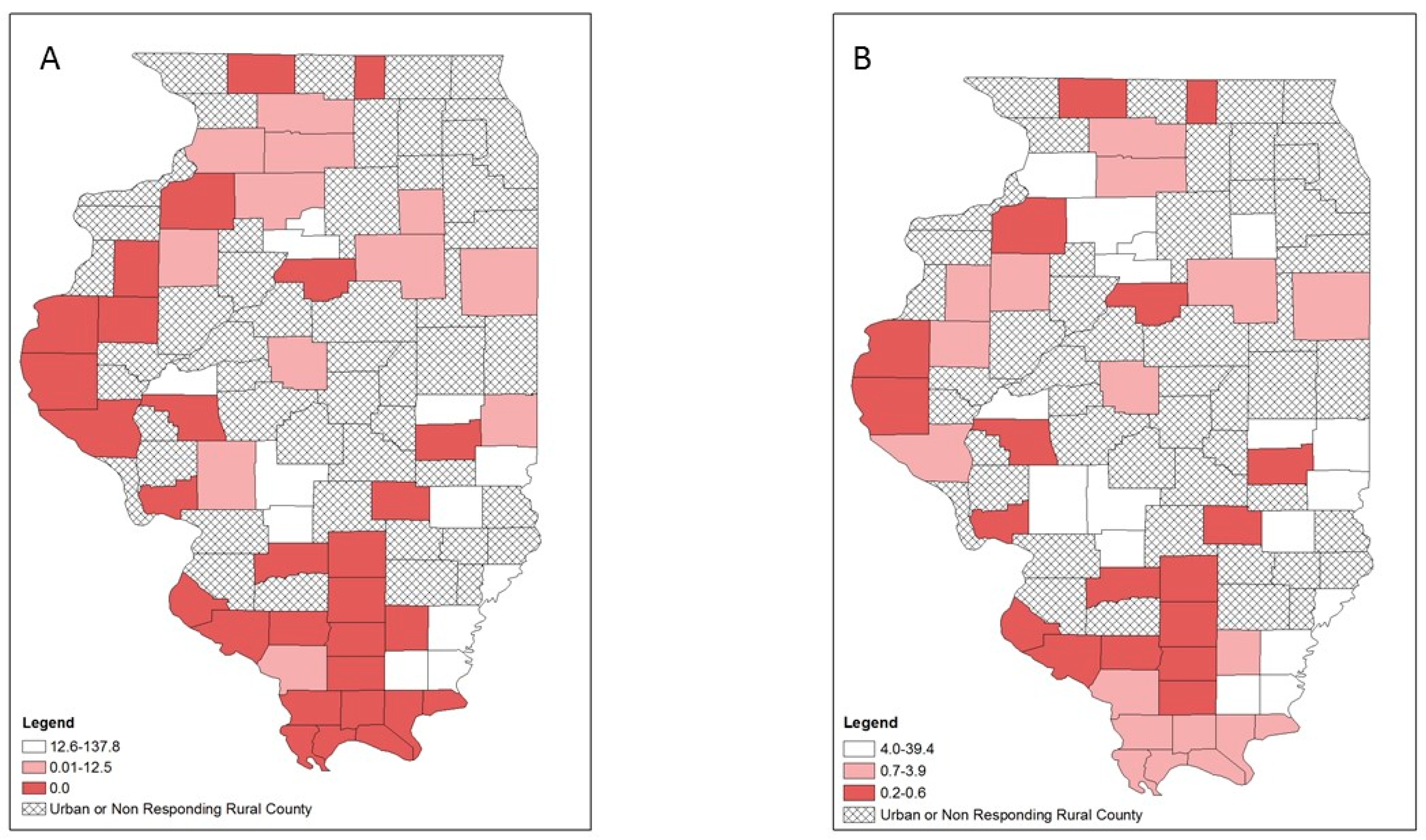
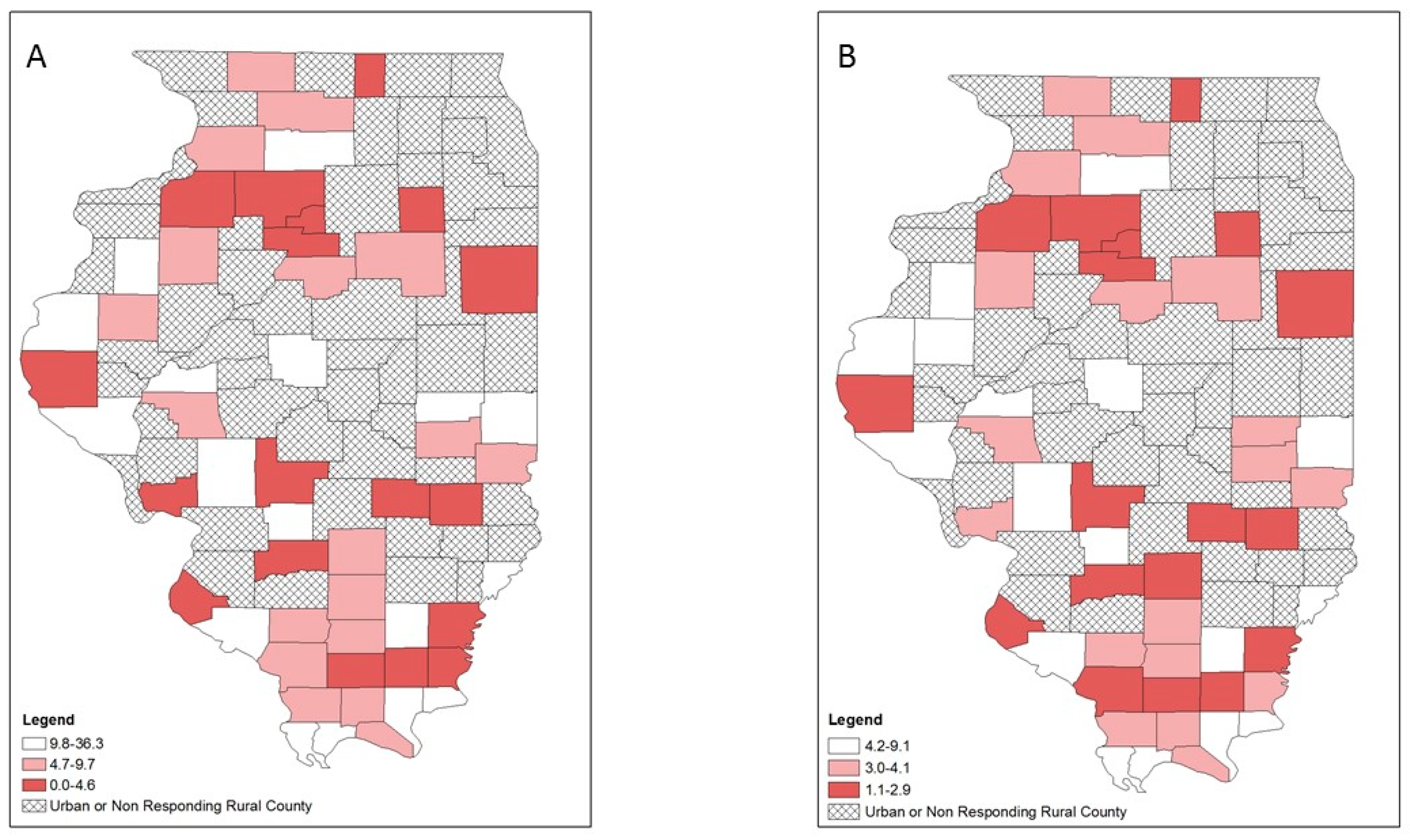
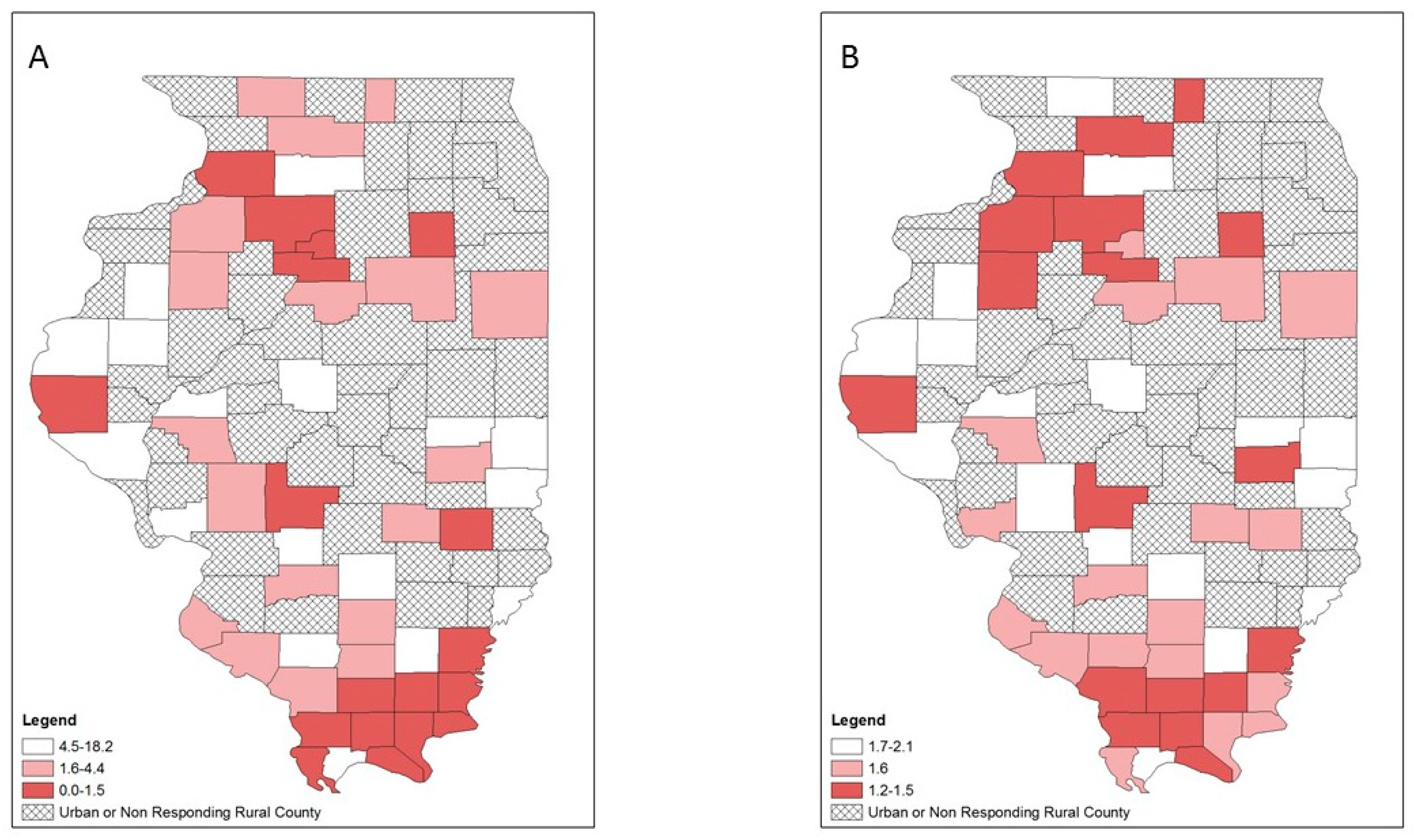
2.5. Choropleth Mapping
3. Results
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Disclaimer
Conflicts of Interest
References
- Perlman, D.C.; Jordan, A.E. The Syndemic of Opioid Misuse, Overdose, HCV, and HIV: Structural-Level Causes and Interventions. Curr. HIV/AIDS Rep. 2018, 15, 96–112. [Google Scholar] [CrossRef]
- National Association of County and City Health Officials. Statement of Policy: Opioid Epidemic. Available online: https://www.naccho.org/uploads/downloadable-resources/18-01-Opioid-Epidemic.pdf (accessed on 15 November 2018).
- Keyes, K.M.; Cerdá, M.; Brady, J.E.; Havens, J.R.; Galea, S. Understanding the rural-urban differences in nonmedical prescription opioid use and abuse in the United States. Am. J. Public Health 2014, 104, e52–e59. [Google Scholar] [CrossRef] [PubMed]
- Van Handel, M.M.; Rose, C.E.; Hallisey, E.J.; Kolling, J.L.; Zibbell, J.E.; Lewis, B.; Bohm, M.K.; Jones, C.M.; Flanagan, B.E.; Siddiqi, A.E.; et al. County-Level Vulnerability Assessment for Rapid Dissemination of HIV or HCV Infections Among Persons Who Inject Drugs, United States. J. Acquir. Immune Defic. Syndr. 2016, 73, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Peters, P.J.; Pontones, P.; Hoover, K.W.; Patel, M.R.; Galang, R.R.; Shields, J.; Duwve, J.M. HIV Infection Linked to Injection Use of Oxymorphone in Indiana, 2014–2015. N. Engl. J. Med. 2016, 375, 229–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. CDC’s Response to the Opioid Overdose Epidemic. Available online: https://www.cdc.gov/opioids/strategy.html (accessed on 15 November 2018).
- Illinois Department of Public Health. State of Illinois Opioid Action Plan. Available online: http://dph.illinois.gov/sites/default/files/publications/Illinois-Opioid-Action-Plan-Sept-6-2017-FINAL.pdf (accessed on 15 November 2018).
- Harris, J.K.; Beatty, K.; Leider, J.P.; Knudson, A.; Anderson, B.L.; Meit, M. The Double Disparity Facing Rural Local Health Departments. Annu. Rev. Public Health 2016, 37, 167–184. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Drug Overdose Death Data. Available online: https://www.cdc.gov/drugoverdose/data/statedeaths.html (accessed on 20 December 2018).
- Substance Abuse and Mental Health Services Administration. State Opioid Response Grants. Available online: https://www.samhsa.gov/grants/grant-announcements/ti-18-015 (accessed on 1 December 2018).
- Illinois Department of Human Services. IDHS/SUPR Initiatives in Response to the Opioid Crisis. Available online: http://www.dhs.state.il.us/page.aspx?item=105980 (accessed on 20 December 2018).
- Centers for Disease Control and Prevention. Public Health Emergency Preparedness (PHEP) Cooperative Agreement. Available online: https://www.cdc.gov/cpr/readiness/phep.htm (accessed on 30 November 2018).
- Centers for Disease Control and Prevention. Opioid Overdose: State Information. Available online: https://www.cdc.gov/drugoverdose/states/index.html (accessed on 24 January 2019).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inf. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Illinois Critical Access Hospital Network. Illinois Counties by Rural/Urban Classification. Available online: http://www.icahn.org/files/Rural_Health_Clinic/Rural_urban_counties.pdf (accessed on 15 November 2018).
- Illinois Department of Public Health. Death Statistics. Available online: http://www.dph.illinois.gov/data-statistics/vital-statistics/death-statistics/more-statistics (accessed on 1 November 2018).
- Illinois Department of Public Health. Discharge Data. Available online: http://dph.illinois.gov/topics-services/prevention-wellness/patient-safety-quality/discharge-Data (accessed on 1 November 2018).
- Illinois Department of Public Health. HIV Surveillance. Available online: http://www.dph.illinois.gov/topics-services/diseases-and-conditions/hiv-aids/hiv-surveillance/update-reports (accessed on 1 November 2018).
- Illinois Department of Public Health. Infectious Disease Reporting. Available online: http://www.dph.illinois.gov/topics-services/diseases-and-conditions/infectious-diseases/infectious-disease-reporting (accessed on 1 November 2018).
- United States Census Bureau. County Population Totals. Available online: https://www.census.gov/data/datasets/2017/demo/popest/counties-total.html (accessed on 1 November 2018).
- Cressie, N. Smoothing Regional Maps Using Empirical Bayes Motel. Geogr. Anal. 1992, 24, 75–95. [Google Scholar] [CrossRef]
- Devine, O.J.; Louis, T.A.; Halloran, M.E. Empirical Bayes Methods for Stabilizing Incidence Rates before Mapping. Epidemiology 1994, 5, 622–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brewer, C.A. Basic Mapping Principles for Visualizing Cancer Data Using Geographic Information Systems (GIS). Am. J. Prev. Med. 2006, 30, S25–S36. [Google Scholar] [CrossRef] [PubMed]
- Delta Regional Authority. About DRA. Available online: https://www.dra.gov/about-dra/mission-and-vision (accessed on 8 January 2019).
- Delta Regional Authority. Promoting a Healthy Delta. Available online: https://dra.gov/initiatives/promoting-a-healthy-delta (accessed on 8 January 2019).
- Nykiforuk, C.I.J.; Flaman, L.M. Geographic Information Systems (GIS) for Health Promotion and Public Health: A Review. Health Promot. Pract. 2011, 12, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Dubowitz, T.; Williams, M.; Steiner, E.D.; Weden, M.M.; Miyashiro, L.; Jacobson, D.; Lurie, N. Using geographic information systems to match local health needs with public health services and programs. Am. J. Public Health AJPH 2011, 101, 1664–1665. [Google Scholar] [CrossRef] [PubMed]
- Illinois Department of Public Health. IPLAN Standards and MAPP Crosswalk. Available online: https://iquery.illinois.gov/iquery/page.aspx?item=139 (accessed on 26 November 2018).
- Williams, M.V.; Dubowitz, T.; Jacobson, D.; Leuschner, K.J.; Kraus, L.; Steiner, E.D.; Weden, M. Mapping the Gaps: Ideas for Using GIS to Enhance Local Health Department Priority Setting and Program Planning; RAND Corporation: Santa Monica, CA, USA, 2011; Available online: https://www.rand.org/pubs/technical_reports/TR1146.html (accessed on 1 November 2018).
- Curtis, A.B.; Kothari, C.; Paul, R.; Connors, E. Using GIS and secondary data to target diabetes-related public health efforts. Public health reports. Public Health Rep. 2013, 128, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Health Resource and Services Administration. Data Portal. Available online: https://data.hrsa.gov/hdw/tools/dataportal.aspx (accessed on 4 January 2019).
- Substance Abuse and Mental Health Services Administration. Legislation, Regulations, and Guidelines. Available online: https://www.samhsa.gov/programs-campaigns/medication-assisted-treatment/legislation-regulations-guidelines (accessed on 24 January 2019).
- Lucchesi, L.R.; Wikle, C.K. Visualizing uncertainty in areal data with bivariate choropleth maps, map pixelation and glyph rotation. Stat 2017, 6, 292–302. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Service | N (%) | Disease-Specific Service Group |
|---|---|---|
| HIV testing | HIV prevention and treatment services | |
| 0 | 16 (30.2%) | |
| 1 | 33 (62.3%) | |
| 2+ | 4 (7.5%) | |
| Hepatitis C testing | Hepatitis C prevention and treatment services | |
| 0 | 20 (37.7%) | |
| 1 | 29 (54.7%) | |
| 2+ | 4 (7.6%) | |
| Pre-exposure Prophylaxis (PrEP) Clinic | HIV prevention and treatment services | |
| 0 | 46 (86.8%) | |
| 1 | 6 (11.3%) | |
| 2+ | 1 (1.9%) | |
| Naloxone Administration | OUD treatment services | |
| 0 | 38 (71.7%) | |
| 1 | 13 (24.5%) | |
| 2+ | 2 (3.8%) | |
| Naloxone Distribution | OUD treatment services | |
| 0 | 41 (77.4%) | |
| 1 | 11 (20.8%) | |
| 2+ | 1 (1.9%) | |
| Syringe Exchange | HIV & hepatitis C prevention and treatment services | |
| 0 | 50 (94.3%) | |
| 1 | 3 (5.7%) | |
| 2+ | 0 (0%) | |
| Syringe Disposal | HIV & hepatitis C prevention and treatment services | |
| 0 | 45 (84.9%) | |
| 1 | 8 (15.1%) | |
| 2+ | 0 (0%) | |
| Adult Mental Health | OUD treatment services | |
| 0 | 37 (69.8%) | |
| 1 | 13 (24.5%) | |
| 2+ | 3 (5.7%) | |
| Youth Mental Health | OUD treatment services | |
| 0 | 38 (71.7%) | |
| 1 | 12 (22.6%) | |
| 2+ | 3 (5.7%) | |
| Adult Substance Use | OUD treatment services | |
| 0 | 41 (77.4%) | |
| 1 | 10 (18.9%) | |
| 2+ | 2 (3.8%) | |
| Youth Substance Use | OUD treatment services | |
| 0 | 41 (77.4%) | |
| 1 | 10 (18.9%) | |
| 2+ | 2 (3.8%) | |
| Medication-Assisted Therapy | OUD treatment services | |
| 0 | 48 (86.8%) | |
| 1 | 6 (11.3%) | |
| 2+ | 1 (1.9%) |
| Disease-Specific Service Group | Mean (SD) | Median (Range) |
|---|---|---|
| Opioid Use Disorder (OUD) treatment services | 1.9 (2.8) | 0 (0–13) |
| HIV prevention and treatment services | 2.0 (1.6) | 2 (0–9) |
| Hepatitis C prevention and treatment services | 0.9 (0.8) | 1 (0–3) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McLuckie, C.; Pho, M.T.; Ellis, K.; Navon, L.; Walblay, K.; Jenkins, W.D.; Rodriguez, C.; Kolak, M.A.; Chen, Y.-T.; Schneider, J.A.; et al. Identifying Areas with Disproportionate Local Health Department Services Relative to Opioid Overdose, HIV and Hepatitis C Diagnosis Rates: A Study of Rural Illinois. Int. J. Environ. Res. Public Health 2019, 16, 989. https://doi.org/10.3390/ijerph16060989
McLuckie C, Pho MT, Ellis K, Navon L, Walblay K, Jenkins WD, Rodriguez C, Kolak MA, Chen Y-T, Schneider JA, et al. Identifying Areas with Disproportionate Local Health Department Services Relative to Opioid Overdose, HIV and Hepatitis C Diagnosis Rates: A Study of Rural Illinois. International Journal of Environmental Research and Public Health. 2019; 16(6):989. https://doi.org/10.3390/ijerph16060989
Chicago/Turabian StyleMcLuckie, Colleen, Mai T. Pho, Kaitlin Ellis, Livia Navon, Kelly Walblay, Wiley D. Jenkins, Christofer Rodriguez, Marynia A. Kolak, Yen-Tyng Chen, John A. Schneider, and et al. 2019. "Identifying Areas with Disproportionate Local Health Department Services Relative to Opioid Overdose, HIV and Hepatitis C Diagnosis Rates: A Study of Rural Illinois" International Journal of Environmental Research and Public Health 16, no. 6: 989. https://doi.org/10.3390/ijerph16060989