Work-Life Conflict among U.S. Long-Haul Truck Drivers: Influences of Work Organization, Perceived Job Stress, Sleep, and Organizational Support

 ,
, 
Abstract
:1. Introduction
- (1)
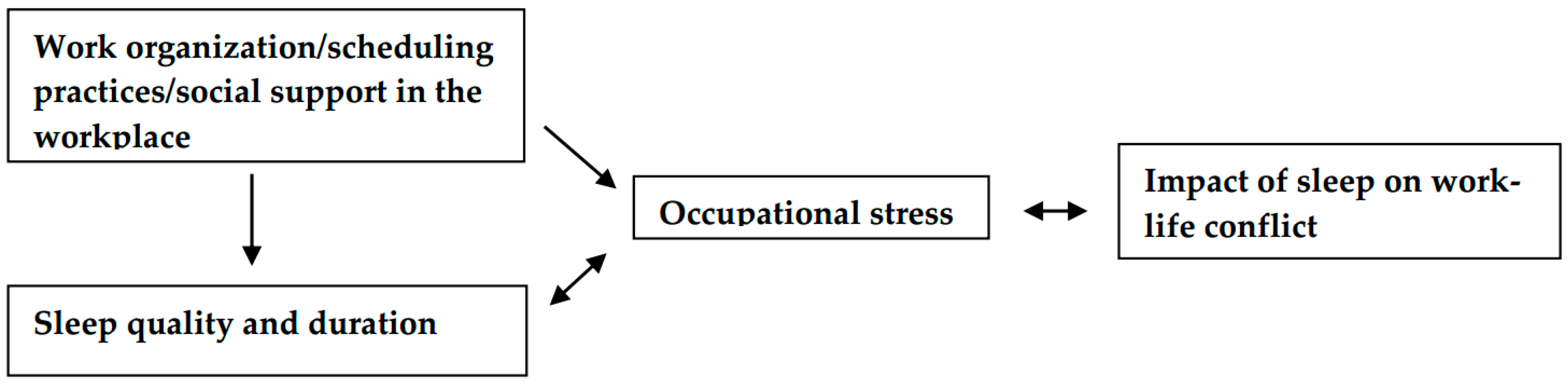
- that the combination of adverse work organization characteristics and an increased perceived job stress serve as a predictor of an increase in driver’ reporting of sleep negatively impacting their work-life balance;
- (2)
- and that the combination of adverse work organization characteristics and poorer sleep outcomes are predictors of higher perceived job stress.
- (3)
- we hypothesized that occupational stress mediates the relationship between on-the-job factors (scheduling, supervisor support), sleep, and subsequent work-life conflict.
2. Materials and Methods
2.1. Study Setting and Sample
2.2. Study Measures
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Connections between Work Organization, Sleep, Stress and Work-Life Balance
4.2. Recommendations to Improve Work-Life Balance
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Landsbergis, P.; Choi, B.; Dobson, M.; Sembajwe, G.; Slatin, C.; Delp, L.; Siqueira, C.; Schnall, P.; Baron, S. The Key Role of Work in Population Health Inequities. Am. J. Public Health 2018, 108, 296–297. [Google Scholar] [CrossRef] [PubMed]
- Alterman, T.; Luckhaupt, S.; Dahlhamer, J.; Ward, B.; Calvert, G. Job Insecurity, Work-Family Imbalance, and Hostile Work Environment: Prevalence Data from the 2010 National Health Interview Survey. Am. J. Ind. Med. 2013, 56, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N. Workers are People Too: Societal Aspects of Occupational Health Disparities—An Ecosocial Perspective. Am. J. Ind. Med. 2010, 53, 104–115. [Google Scholar] [CrossRef] [PubMed]
- Landsbergis, P. Assessing the Contribution of Working Conditions to Socioeconomic Disparities in Health: A Commentary. Am. J. Ind. Med. 2010, 53, 95–103. [Google Scholar] [CrossRef]
- Ahonen, E.; Fujishiro, K.; Cunningham, T.; Flynn, M. Work as an Inclusive Part of Population Health Inequities Research and Prevention. Am. J. Public Health 2018, 108, 306–311. [Google Scholar] [CrossRef]
- Clougherty, J.; Souza, K.; Cullen, M. Work and its role in shaping the social gradient in health. Ann. N. Y. Acad. Sci. 2010, 1186, 102–124. [Google Scholar] [CrossRef] [Green Version]
- Marmot, M. The Health Gap; Bloomsbury Press: London, UK, 2015. [Google Scholar]
- Landsbergis, P.; Grzywacz, J.; Montagne, A. Work Organization, Job Insecurity, and Occupational Health Disparities. Am. J. Ind. Med. 2014, 57, 495–515. [Google Scholar] [CrossRef]
- Burgard, S.; Lin, K. Bad Jobs, Bad Health? How Work and Working Conditions Contribute to Health Disparities. Am. Behav. Sci. 2013, 57, 1105–1127. [Google Scholar] [CrossRef] [Green Version]
- Siegrist, J.; Rodel, A. Work stress and health risk behavior. Scand. J. Work Environ. Health 2006, 32, 473–481. [Google Scholar] [CrossRef] [Green Version]
- LaMontagne, A. Invited Commentary: Job Strain and Health Behaviors—Developing a Bigger Picture. Am. J. Epidemiol. 2012, 176, 1090–1094. [Google Scholar] [CrossRef]
- Soloveiva, S.; Lalluka, T. Psychosocial factors at work, long work hours, and obesity: A systematic review. Scandanavian J. Work Environ. Health 2013, 39, 241–258. [Google Scholar] [CrossRef]
- Heraclides, A.; Chandola, T.; Witte, D.; Brunner, E. Work Stress, Obesity and The Risk of Type 2 Diabetes: Gender-Specific Bidirectional Effect in the Whitehall II Study. Obesity 2012, 20, 428–433. [Google Scholar] [CrossRef]
- Kivimaki, M.; Singh-Manoux, A.; Jokela, M.; Virtanen, M. Job strain and risk of obesity: A systematic review and meta-analysis of cohort studies. Int. J. Obes. 2015, 39, 1597–1600. [Google Scholar] [CrossRef]
- Schnall, P.; Dobson, M.; Landsbergis, P. Globalization, Work, and Cardiovascular Disease. Int. J. Health Serv. 2016, 46, 656–692. [Google Scholar] [CrossRef]
- Luckhaupt, S.; Cohen, M.; Li, J.; Calvert, G. Prevalence of Obesity Among U.S. Workers and Associations with Occupational Factors. Am. J. Prev. Med. 2014, 46, 237–248. [Google Scholar] [CrossRef] [Green Version]
- Yong, L.; Li, J.; Calvert, G. Sleep-related problems in the US working population: Prevalence and association with shiftwork status. Occup. Environ. Med. 2017, 74, 93–104. [Google Scholar] [CrossRef]
- Linton, S.; Kecklund, G.; Franklin, K.; Leissner, L.; Sivertsen, B.; Lindberg, E.; Svensson, A.; Hansson, S.; Sundin, O.; Hetta, J.; et al. The effect of the work environment on future sleep disturbances: A systematic review. Sleep Med. Rev. 2015, 23, 10–19. [Google Scholar] [CrossRef]
- Stansfeld, S.; Candy, B. Psychosocial work environment and mental health—A meta-analytic review. Scandanavian J. Work Environ. Health 2006, 32, 443–462. [Google Scholar] [CrossRef]
- Harvey, S.; Modini, M.; Joyce, S.; Milligan-Saville, J.; Tan, L.; Mykletun, A.; Bryant, R.; Christensen, H.; Mitchell, P. Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occup. Environ. Med. 2017, 74, 301–310. [Google Scholar] [CrossRef]
- BLS BoLS. Heavy and Tractor-trailer Truck Drivers. Available online: https://www.bls.gov/ooh/transportation-and-material-moving/heavy-and-tractor-trailer-truck-drivers.htm#tab-6 (accessed on 4 June 2018).
- Sieber, W.; Robinson, C.; Birdsey, J.; Chen, G.; Hitchcock, E.; Lincoln, J.; Nakata, A.; Sweeney, M. Obesity and Other Risk Factors: The National Survey of U.S. Long-Haul Truck Driver Health and Injury. Am. J. Ind. Med. 2014, 57, 615–626. [Google Scholar] [CrossRef] [Green Version]
- Apostolopoulos, Y.; Lemke, M.; Sonmez, S. Risks endemic to long-haul trucking in North America: Strategies to protect and promote driver well-being. New Solut. J. Environ. Occup. Health Policy 2014, 24, 57–80. [Google Scholar] [CrossRef]
- Belzer, M. Sweatshops on Wheels: Winners and Losers in Trucking Deregulation; Oxford University Press: Oxford, UK, 2000. [Google Scholar]
- Hege, A.; Lemke, M.; Apostolopoulos, Y.; Perko, M.; Sonmez, S.; Strack, R. US long-haul truck driver work organization and the association with cardiometabolic disease risk. Arch. Environ. Occup. Health 2017, 72, 303–310. [Google Scholar] [CrossRef]
- Lemke, M.; Apostolopoulos, Y.; Hege, A.; Sonmez, S.; Wideman, L. Understanding the role of sleep quality and sleep duration in commercial driving safety. Accid. Anal. Prev. 2016, 97, 79–86. [Google Scholar] [CrossRef]
- Chen, G.; Fang, Y.; Guo, F.; Hanowski, R. The influence of daily sleep patterns of commercial truck drivers on driving performance. Accid. Anal. Prev. 2016, 91, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Kelly, E.; Moen, P.; Oakes, J.; Fan, W.; Okechukwu, C.; Davis, K.; Hammer, L.; Kossek, E.; King, R.; Hanson, G.; et al. Changing Work and Work-Family Conflict: Evidence from the Work, Family, and Health Network. Am. Sociol. Rev. 2014, 79, 485–516. [Google Scholar] [CrossRef]
- Moen, P.; Kaduk, A.; Kossek, E.; Hammer, L.; Buxton, O.; O’Donnell, E.; Almeida, D.; Fox, K.; Tranby, E.; Oakes, J.; et al. Is work-family conflict a multilevel stressor linking job conditions to mental health? Evidence from the Work, Family and Health Network. In Work and Family in the New Economy; Emerald Group Publishing: Bingley, UK, 2015; pp. 177–217. [Google Scholar]
- Williams, J.; Berdahl, J.; Vandello, J. Beyond work-life “integration”. Annu. Rev. Psychol. 2016, 67, 515–539. [Google Scholar] [CrossRef]
- Buxton, O.; Lee, S.; Beverly, C.; Berkman, L.; Moen, P.; Kelly, E.; Hammer, L.; Almeida, D. Work-Family Conflict and Employee Sleep: Evidence from IT Workers in the Work, Family and Health Study. Sleep 2016, 39, 1911–1918. [Google Scholar] [CrossRef]
- Haar, J.; Sune, A.; Russo, M.; Ollier-Malaterre, A. A Cross-National Study on the Antecedents of Work-Life Balance from the Fit and Balance Perspective. Soc. Indic. Res. 2018. [Google Scholar] [CrossRef]
- Oshio, T.; Inoue, A.; Tsutsumi, A. Does work-to-family conflict really matter for health? Cross-sectional, prospective cohort and fixed-effect analyses. Soc. Sci. Med. 2017, 175, 36–42. [Google Scholar] [CrossRef]
- Sirgy, M.; Lee, D. Work-Life Balance: An Integrative Review. Appl. Res. Qual. Life 2018, 13, 229–254. [Google Scholar] [CrossRef]
- Lee, D.; Sirgy, M. What Do People Do to Achieve Work-Life Balance? A Formative Conceptualization to Help Develop a Metric for Large-Scale Quality-of-Life Surveys. Soc. Indic. Res. 2018, 138, 771–791. [Google Scholar] [CrossRef]
- Fujimura, Y.; Sekine, M.; Tatsuse, T. Sex differences in factors contributing to family-to-work and work-to-family conflict in Japanese civil servants. J. Occup. Health 2014, 56, 485–497. [Google Scholar] [CrossRef]
- Lunau, T.; Bambra, C.; Eikemo, T.; Wel, K.v.d.; Dragano, N. A balancing act? Work-life balance, health and well-being in European welfare states. Eur. J. Public Health 2014, 24, 422–427. [Google Scholar] [CrossRef]
- Lallukka, T.; Chandola, T.; Roos, E.; Cable, N.; Sekine, M.; Kagamimori, S.; Tatsuse, T.; Marmot, M.; Lahelma, E. Work-family conflicts and health behaviors among British, Finnish, and Japanese employees. Int. J. Behav. Med. 2010, 17, 134–142. [Google Scholar] [CrossRef]
- Leineweber, C.; Baltzer, M.; Hanson, L.M.; Westerlund, H. Work-family conflict and health in Swedish working women and men: A 2-year prospective analysis (the SLOSH study). Eur. J. Public Health 2013, 23, 710–716. [Google Scholar] [CrossRef]
- Dahlgren, A.; Tucker, P.; Gustavsson, P.; Rudman, A. Quick returns and night work as predictors of sleep quality, fatigue, work-family balance and satisfaction with work hours. Chronobiol. Int. 2016, 33, 759–767. [Google Scholar] [CrossRef]
- Mellner, C.; Kecklund, G.; Kompier, M.; Sariaslan, A.; Aronsson, G. Boundaryless Work, Psychological Detachment and Sleep: Does Workin ‘Anytime-Anywhere’ Equal Employees are ‘Always on’? In New Ways of Working Practices: Antecedents and Outcomes; Emerald Group Publishing Limited: Bingley, UK, 2016; pp. 29–47. [Google Scholar]
- Berkman, L.; Liu, Y.; Hammer, L.; Moen, P.; Klein, L.; Kelly, E.; Fay, M.; Davis, K.; Durham, M.; Karuntzos, G.; et al. Work-family conflict, cardiometabolic risk and sleep duration in nursing employees. J. Occup. Health Psychol. 2015, 20, 420–433. [Google Scholar] [CrossRef] [Green Version]
- Chandola, T.; Martikainen, P.; Bartley, M.; Lahelma, E.; Marmot, M.; Michikazu, S.; Nasermoaddeli, A.; Kagamimori, S. Does conflict between home and work explain the effect of multiple roles on mental health? A comparative study of Finland, Japan, and the UK. Int. J. Epidemiol. 2004, 33, 884–893. [Google Scholar] [CrossRef] [Green Version]
- Hammig, O.; Bauer, G. Work-life balance and mental health among male and female employees in Switzerland. Int. J. Public Health 2009, 54, 88–95. [Google Scholar] [CrossRef]
- Long, H. America has a massive truck driver shortage. Here’s why few want an $80,000 job. Washington Post, 28 May 2018. [Google Scholar]
- Oyedele, A. America’s biggest companies sound the alarm on truck driver shortage. Business Insider, 5 May 2018. [Google Scholar]
- Knudsen, H.; Ducharme, L.; Roman, P. Job stress and poor sleep quality: Data from an American sample of full-time workers. Soc. Sci. Med. 2007, 64, 1997–2007. [Google Scholar] [CrossRef]
- Burgard, S.; Ailshire, J. Putting work to bed: Stressful experiences on the job and sleep quality. J. Health Soc. Behav. 2009, 50, 476–492. [Google Scholar] [CrossRef]
- Berset, M.; Elfering, A.; Luthy, S.; Luthi, S.; Semmer, N. Work stressors and impaired sleep: Rumination as a mediator. Stress Health 2011, 27, e71–e82. [Google Scholar] [CrossRef]
- Fritz, C.; Crain, T. Recovery from Work and Employee Sleep: Understanding the Role of Experiences and Activities Outside of Work. In Work and Sleep: Research Insights for the Workplace; Barling, J., Barnes, C., Carleton, E., Wagner, D., Eds.; Oxford University Press: New York, NY, USA, 2016; pp. 55–76. [Google Scholar]
- Sonnentag, S.; Casper, A.; Pinck, A. Job Stress and Sleep. In Work and Sleep: Research Insights for the Workplace; Barling, J., Barnes, C., Carleton, E., Wagner, D., Eds.; Oxford University Press: New York, NY, USA, 2016; pp. 77–100. [Google Scholar]
- Williamson, A.; Bohle, P.; Quinlan, M.; Kennedy, D. Short Trips and Long Days: Safety and Health in Short-Haul Trucking. Ind. Labor Relat. Rev. 2009, 62, 415–429. [Google Scholar] [CrossRef]
- Puttonen, S.; Harma, M.; Hubin, C. Shift work and cardiovascular disease—Pathways from circadian stress to morbidity. Scand. J. Work Environ. Health 2010, 36, 96–108. [Google Scholar] [CrossRef]
- Crain, T.; Hammer, L.; Bodner, T.; Kossek, E.; Moen, P.; Lilienthal, R.; Buxton, O. Work-family conflict, family-supportive supervisor behaviors (FSSB), and sleep outcomes. J. Occup. Health Psychol. 2014, 19, 155. [Google Scholar] [CrossRef]
- Germeys, L.; Leineweber, C. Divergent concurrent and lagged effects of the reciprocal relation between work-nonwork interactions and sleep disturbance. Sleep 2018. [Google Scholar] [CrossRef]
- Holmgreen, L.; Tirone, V.; Gerhart, J.; Hobfoll, S. Conservation of resources theory. In The Handbook of Stress and Health: A Guide to Research and Practice; John Wiley & Sons: New York, NY, USA, 2017; pp. 443–457. [Google Scholar]
- Crain, T.; Hammer, L.; Bodner, T.; Olson, R.; Kossek, E.; Moen, P.; Buxton, O. Sustaining Sleep: Results from the Randomized Controlled Work, Family & Health Study. J. Occup. Health Psychol. 2019, 24, 180–197. [Google Scholar]
- Zohar, D.; Huang, Y.; Lee, J.; Robertson, M. A mediation model linking dispatcher leadership and work ownership with safety climate as predictors of truck driver safety performance. Accid. Anal. Prev. 2014, 62, 17–25. [Google Scholar] [CrossRef]
- Zohar, D.; Huang, Y.; Lee, J.; Robertson, M. Testing extrinsic and intrinsic motivation as explanatory variables for the safety climate-safety performance relationship among long-haul truck drivers. Transp. Res. Part F 2014, 30, 84–96. [Google Scholar] [CrossRef]
- Apostolopoulos, Y.; Lemke, M.; Hege, A.; Sonmez, S.; Sang, H.; Oberlin, D.; Wideman, L. Work and Chronic Disease: Comparison of Cardiometabolic Risk Markers Between Truck Drivers and the General US Population. J. Occup. Environ. Med. 2016, 58, 1098–1105. [Google Scholar] [CrossRef]
- Lemke, M.; Hege, A.; Apostolopoulos, Y.; Wideman, L.; Sonmez, S. Work and sleep among transport operators: Disparities and implications for safety. J. Transp. Health 2017, 7, 298–309. [Google Scholar] [CrossRef]
- Netzer, N.; Stoohs, R.; Netzer, C.; Clark, K.; Strohl, K. Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome. Ann. Intern. Med. 1999, 131, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Partinen, M.; Gislason, T. Basic Nordic Sleep Questionnaire (BNSQ): A quantitated measure of subjective sleep complaints. J. Sleep Res. 1995, 4, 150–155. [Google Scholar] [CrossRef] [PubMed]
- IBM. SPSS Statistics 23; IBM: New York, NY, USA, 2018. [Google Scholar]
- Wong, C.; Laschinger, H.S. The influence of frontline manager job strain on burnout, commitment, and turnover retention: A cross-sectional study. Int. J. Nurs. Stud. 2015, 52, 1824–1833. [Google Scholar] [CrossRef] [PubMed]
- Berglund, E.; Lytsy, P.; Westerling, R. The influence of locus of control on self-rated health in context of chronic disease: A structural equation modeling approach in a cross sectional study. BMC Public Health 2014, 14, 492. [Google Scholar] [CrossRef] [PubMed]
- Martinez, S.; Beebe, L.; Thompson, D.; Wagener, T.; Terrell, D.; Campbell, J. A structural equation modeling approach to understanding pathways that connect socioeconomic status and smoking. PLoS ONE 2018, 13, e0192451. [Google Scholar] [CrossRef]
- Côté-Lussier, C.; Mathieu, M.-È.; Barnett, T.A. Independent associations between child and parent perceived neighborhood safety, child screen time, physical activity and BMI: A structural equation modeling approach. Int. J. Obes. 2015, 39, 1475–1481. [Google Scholar] [CrossRef]
- Byrne, B. Structural Equation Modeling with Mplus: Basic Concepts, Applications, and Programming; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Bugge, A.; Möller, S.; Westfall, D.; Tarp, J.; Gejl, A.; Wedderkopp, N.; Hillman, C. Associations between waist circumference, metabolic risk and executive function in adolescents: A cross-sectional mediation analysis. PLoS ONE 2018, 13, e0199281. [Google Scholar] [CrossRef]
- Mplus. Structural Equation Modeling; Mplus: Los Angeles, CA, USA, 2018. [Google Scholar]
- Michel, J.; Kotrba, L.; Mitchelson, J.; Clark, M.; Baltes, B. Antecedents of work-family conflict: A meta-analytic review. J. Organ. Behav. 2011, 32, 689–725. [Google Scholar] [CrossRef]
- Kossek, E.; Pichler, S.; Bodner, T.; Hammer, L. Workplace social support and work-family conflict: A meta-analysis clarifying the influence of general and work-family specific supervisor and organizational support. Pers. Psychol. 2011, 64, 289–313. [Google Scholar] [CrossRef] [PubMed]
- Muthén, L.; Muthén, B. Mplus5; Muthén & Muthén: Los Angeles, CA, USA, 2007. [Google Scholar]
- Foundation, N.S. Sleep in America Polls. Available online: https://www.sleepfoundation.org/professionals/sleep-america-polls (accessed on 2 March 2019).
- Apostolopoulos, Y.; Sonmez, S.; Shattell, M.; Gonzales, C.; Fehrenbacher, C. Health survey of U.S. long-haul truck drivers: Work environment, physical health, and healthcare access. Work 2013, 46, 113–123. [Google Scholar]
- Lemke, M.K.; Apostolopoulos, Y.; Hege, A.; Newnam, S.; Sönmez, S. Can subjective sleep problems detect latent sleep disorders among commercial drivers? Accid. Anal. Prev. 2018, 115, 62–72. [Google Scholar] [CrossRef]
- Lemke, M.K.; Apostolopoulos, Y.; Hege, A.; Wideman, L.; Sönmez, S. Work, sleep, and cholesterol levels of U.S. long-haul truck drivers. Ind. Health 2017, 55, 149–161. [Google Scholar] [CrossRef]
- Lemke, M.K.; Apostolopoulos, Y.; Hege, A.; Wideman, L.; Sönmez, S. Work organization, sleep, and metabolic syndrome among long-haul truck drivers. Occup. Med. 2017, 67, 274–281. [Google Scholar] [CrossRef]
- Ferro, A.S. Remarks by Anne S. Ferro, FMCSA Administrator. In Proceedings of the Sleep Apnea and Trucking Conference, Baltimore, MD, USA, 11 May 2010. [Google Scholar]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2010, 33, S62–S69. [Google Scholar] [CrossRef]
- Krueger, G.P.; Belzer, M.H.; Alvarez, A.; Knipling, R.R.; Husting, E.L.; Brewster, R.M.; Siebert, J. Health and Wellness of Commercial Drivers; Transportation Research Board: Washington, DC, USA, 2007; pp. 58–91. [Google Scholar]
- Chalmers, T.; Lal, S. Assessing cardiovascular associations to affective states in Australian truck drivers. J. Australas. Coll. Road Saf. 2014, 25, 23. [Google Scholar]
- Cahalin, L.P.; Myers, J.; Kaminsky, L.; Briggs, P.; Forman, D.E.; Patel, M.J.; Pinkstaff, S.O.; Arena, R. Current trends in reducing cardiovascular risk factors in the United States: Focus on worksite health and wellness. Prog. Cardiovasc. Dis. 2014, 56, 476–483. [Google Scholar] [CrossRef]
- Sangaleti, C.T.; Trincaus, M.R.; Baratieri, T.; Zarowy, K.; Ladika, M.B.; Menon, M.U.; Miyahara, R.Y.; Raimondo, M.I.; Silveira, J.V.; Bortolotto, L.A.; et al. Prevalence of cardiovascular risk factors among truck drivers in the south of Brazil. BMC Public Health 2014, 14, 1063. [Google Scholar] [CrossRef]
- Apostolopoulos, Y.; Peachey, A.A.; Sonmez, S. The psychosocial environment of commercial driving: Morbidities, hazards, and productivity of truck and bus drivers. In Handbook of Stress in the Occupations; Langan-Fox, J., Cooper, C., Eds.; Edward Elgar: Northampton, UK, 2011. [Google Scholar]
- Ebrahimi, M.H.; Sadeghi, M.; Dehghani, M.; Niiat, K.S. Sleep habits and road traffic accident risk for Iranian occupational drivers. Int. J. Occup. Med. Environ. Health 2015, 28, 305–312. [Google Scholar] [CrossRef]
- Buxton, O.; Quintilliani, L.; Yang, M.; Ebbeling, C.; Stoddard, A.; Pereria, L.; Sorensen, G. Association of sleep adequacy with more healthful food chocies and positive workplace experiences among motor freight workers. Am. J. Public Health 2009, 99, S636–S643. [Google Scholar] [CrossRef]
- Guglielmi, O.; Magnavita, N.; Garbarino, S. Sleep quality, obstructive sleep apnea, and psychological distress in truck drivers: A cross-sectional study. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 53, 531–536. [Google Scholar] [CrossRef]
- Hege, A.; Perko, M.; Johnson, A.; Yu, C.H.; Sönmez, S.; Apostolopoulos, Y. Surveying the impact of work hours and schedules on commercial motor vehicle driver sleep. Saf. Health Work 2015, 6, 104–113. [Google Scholar] [CrossRef]
- Kanazawa, H.; Suzuki, M.; Onoda, T.; Yokozawa, N. Excess workload and sleep-related symptoms among commercial long-haul truck drivers. Sleep Biol. Rhythm. 2006, 4, 121–128. [Google Scholar] [CrossRef]
- Lemke, M.K.; Hege, A.; Perko, M.; Sönmez, S.; Apostolopoulos, Y. Work patterns, sleeping hours and excess weight in commercial drivers. Occup. Med. 2015. [Google Scholar] [CrossRef]
- De Pinho, R.S.N.; da Silva-Junior, F.P.; Bastos, J.P.C.; Maia, W.S.; de Mello, M.T.; de Bruin, V.M.S.; de Bruin, P.F.C. Hypersomnolence and accidents in truck drivers: A cross-sectional study. Chronobiol. Int. 2006, 23, 963–971. [Google Scholar] [CrossRef]
- Dobson, M.; Schnall, P.L. From stress to distress: The impact of work on mental health. In Unhealthy Work: Causes, Consequences, Cures; Schnall, P.L., Dobson, M., Rosskam, E., Eds.; Baywood: Amityville, NY, USA, 2009; pp. 113–132. [Google Scholar]
- Ross, G.F. Tourism industry employee workstress—A present and future crisis. J. Travel Tour. Mark. 2005, 19, 133–147. [Google Scholar] [CrossRef]
- Taylor, A.H.; Dorn, L. Stress. fatigue, health, and risk of road traffic accidents among professional drivers: The contribution of physical inactivity. Annu. Rev. Public Health 2006, 27, 371–391. [Google Scholar] [CrossRef]
- Apostolopoulos, Y.; Sonmez, S.; Lemke, M. Mapping U.S. long-haul truck drivers’ multiplex networks and risk topography in inner-city neighborhoods. Health Place 2015, 34, 9–18. [Google Scholar] [CrossRef]
- Apostolopoulos, Y.; Sönmez, S.; Hege, A.; Lemke, M.K. Work strain, social isolation and mental health of long-haul truckers. Occup. Ther. Ment. Health 2016, 32, 50–69. [Google Scholar] [CrossRef]
- Shattell, M.; Apostolopoulos, Y.; Sönmez, S.; Griffin, M. Occupational stressors and the mental health of truckers. Issues Ment. Health Nurs. 2010, 31, 561–568. [Google Scholar] [CrossRef]
- Orris, P.; Hartman, D.E.; Strauss, P.; Anderson, R.J.; Collins, J.; Knopp, C.; Xu, Y.; Melius, J. Stress among package truck drivers. Am. J. Ind. Med. 1997, 31, 202–210. [Google Scholar] [CrossRef]
- O’Neill, J.W.; Davis, K. Work stress and well-being in the hotel industry. Int. J. Hosp. Manag. 2011, 30, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Chiang, F.F.T.; Birtch, T.A.; Kwan, H.K. The moderating roles of job control and work-life balance practices on employee stress in the hotel and catering industry. Int. J. Hosp. Manag. 2010, 29, 25–32. [Google Scholar] [CrossRef]
- Damaske, S.; Zawadzki, M.J.; Smyth, J.M. Stress at work: Differential experiences of high versus low SES workers. Soc. Sci. Med. 2016, 156, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Wenger, J. Freedom isn’t free: Voices from the truck driving industry. New Solut. 2008, 18, 481–491. [Google Scholar] [CrossRef]
- Filiatrault, D.D.; Vavrik, J.; Kuzeljevic, B.; Cooper, P.J. The effect of rest-schedule orientation on sleep quality of commercial drivers. Traffic Inj. Prev. 2002, 3, 13–18. [Google Scholar] [CrossRef]
- Saltzman, G.M.; Belzer, M.H. Truck Driver Occupational Safety and Health 2003: Conference Report and Selective Literature Review. In Proceedings of the Truck Driver Occupational Safety and Health 2003, Wayne State University, Detroit, MI, USA, 24–25 April 2003. [Google Scholar]
- Brodie, L.; Lyndal, B.; Elias, I.J. Heavy vehicle driver fatalities: Learning’s from fatal road crash investigations in Victoria. Accid. Anal. Prev. 2009, 41, 557–564. [Google Scholar] [CrossRef]
- Lemke, M.K.; Meissen, G.J.; Apostolopoulos, Y. Overcoming barriers in unhealthy settings: A phenomenological study of healthy truck drivers. Glob. Qual. Nurs. Res. 2016, 3. [Google Scholar] [CrossRef] [PubMed]
- Karkoulian, S.; Srour, J.; Sinan, T. A gender perspective on work-life balance, perceived stress, and locus of control. J. Bus. Res. 2016, 69, 4918–4923. [Google Scholar] [CrossRef]
- Âkerstedt, T. Psychosocial stress and impaired sleep. Scand. J. Work Environ. Health 2006, 32, 493–501. [Google Scholar] [CrossRef]
- Darcy, C.; McCarthy, A.; Hill, J.; Grady, G. Work–life balance: One size fits all? An exploratory analysis of the differential effects of career stage. Eur. Manag. J. 2012, 30, 111–120. [Google Scholar] [CrossRef] [Green Version]
- Jensen, A.; Dahl, S. Truck drivers hours-of-service regulations and occupational health. Work 2009, 33, 363–368. [Google Scholar]
- Lemke, M.K.; Apostolopoulos, Y. Policy, work organization and sleep health and safety of commercial drivers: Introducing a complex systems paradigm. J. Ergon. 2016, 6, 152–156. [Google Scholar] [CrossRef]
- Newnam, S.; Goode, N.; Salmon, P.; Stevenson, M. Reforming the road freight transportation system using systems thinking: An investigation of Coronial inquests in Australia. Accid. Anal. Prev. 2017, 101, 28–36. [Google Scholar] [CrossRef]
- Salmon, P.M.; McClure, R.; Stanton, N.A. Road transport in drift? Applying contemporary systems thinking to road safety. Saf. Sci. 2012, 50, 1829–1838. [Google Scholar] [CrossRef]
- Olson, R.; Anger, W.K.; Elliot, D.L.; Wipfli, B.; Gray, M. A new health promotion model for lone workers: Results of the Safety & Health Involvement For Truckers (SHIFT) pilot study. J. Occup. Environ. Med. 2009, 51, 1233–1246. [Google Scholar]
- Wipfli, B.; Olson, R.; Koren, M. Weight-loss maintenance among SHIFT pilot study participants 30-months post-ntervention. J. Occup. Environ. Med. 2013, 55, 1. [Google Scholar] [CrossRef]
- Krueger, G.P.; Brewster, R.M.; Dick, V.R.; Inderbitzen, R.E.; Staplin, L. Health and Wellness Programs for Commercial Drivers; Transportation Research Board: Washington, DC, USA, 12 October 2007. [Google Scholar]
- Apostolopoulos, Y.; Lemke, M.K.; Sönmez, S.; Hege, A. The obesogenic environment of commerical trucking: A worksite environmental audit and implications for systems-based interventions. Am. J. Health Educ. 2016, 47, 85–93. [Google Scholar] [CrossRef]
- Lemke, M.; Apostolopoulos, Y. Health and wellness programs for commercial motor-vehicle drivers: Organizational assessment and new research directions. Workplace Health Saf. 2015, 63, 71–80. [Google Scholar] [CrossRef]
- Ropponen, A.; Harma, M.; Bergbom, B.; Natti, J.; Sallinen, M. The vicious cycle of working hours, sleep, and recovery in expert work. Int. J. Environ. Res. Public Health 2018, 15, 1361. [Google Scholar] [CrossRef]
- Lederer, W.; Paal, P.; Langen, D.v.; Sanwald, A.; Traweger, C.; Kinzl, J. Consolidation of working hours and work-life balance in anaesthesiologists—A cross-sectional national survey. PLoS ONE 2018, 13, e0206050. [Google Scholar] [CrossRef]
- Van der Holst, H.M.L.; Kerkhof, G.A. Shift work tolerance and the importance of sleep quality: A study of police officers. Biol. Rhythm Res. 2015, 46, 257–264. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age. Driver Years of Experience, Work Organization Characteristics | N (%) |
|---|---|
| Age | |
| 18–39 | 69 (26.5) |
| 40–49 | 73 (28.1) |
| 50 and older | 118 (45.4) |
| Years of Experience | |
| Less than 10 years | 97 (37.3) |
| 10–19 years | 79 (30.4) |
| 20 or more years | 84 (32.3) |
| Days on road per month | |
| 20 or less days | 40 (15.4) |
| 21–25 days | 110 (42.3) |
| 26 or more days | 110 (42.3) |
| Work hours per day | |
| Less than 11 h | 77 (29.8) |
| 11–13 h | 83 (32.1) |
| 13 or more hours | 99 (38.3) |
| Daily schedule | |
| Same each day | 45 (17.3) |
| Different each day | 215 (82.7) |
| Hours of day | |
| Same each day | 94 (36.2) |
| Different each day | 166 (63.8) |
| Days of week | |
| Same each week | 175 (67.6) |
| Different each week | 84 (32.4) |
| Fast pace of work | |
| Never or rarely | 83 (32.1) |
| Sometimes | 56 (21.6) |
| Often or always | 120 (46.4) |
| Coworker support | |
| Never or rarely | 57 (30.0) |
| Sometimes | 40 (21.1) |
| Often or always | 93 (48.9) |
| Supervisor support | |
| Never or rarely | 21 (8.4) |
| Sometimes | 38 (15.3) |
| Often or always | 189 (76.2) |
| Stress and Sleep Outcomes | Mean (SD) | Range | N (%) |
|---|---|---|---|
| Perceived stress | |||
| None–mild | 97 (37.3) | ||
| Moderate | 104 (40.0) | ||
| High or chronic | 59 (22.7) | ||
| Sleep duration in hours (Workdays) | 6.95 (1.62) | 3.0–13.0 | |
| Sleep duration in hours (Non-workdays) | 8.27 (2.12) | 3.5–16.0 | |
| Sleep duration needed for ‘highest function’ | 6.75 (1.53) | 1.0–13.0 | |
| Sleep quality (Workdays)—Frequency of ‘good night’s sleep’ | |||
| Never or rarely | 98 (38.2) | ||
| Almost or every night | 159 (61.8) | ||
| Sleep quality (Non-workdays)—Frequency of ‘good night’s sleep’ | |||
| Never or rarely | 39 (16.7) | ||
| Almost or every night | 194 (83.3) |
| Impact Outcomes | N (%) | Mean (SD) | Range |
|---|---|---|---|
| Impact on work | |||
| No impact | 48 (19.0) | ||
| Some impact | 111 (43.9) | ||
| Major impact | 94 (37.2) | ||
| Impact on social and leisure activities | |||
| No impact | 94 (41.4) | ||
| Some impact | 78 (34.4) | ||
| Major impact | 55 (24.2) | ||
| Impact on family and home responsibilities | |||
| No impact | 99 (40.9) | ||
| Some impact | 87 (36.0) | ||
| Major impact | 56 (23.1) | ||
| Impact on mood | |||
| No impact | 46 (18.0) | ||
| Some impact | 106 (41.6) | ||
| Major impact | 103 (40.4) | ||
| Impact on intimate and sexual relations | |||
| No impact | 122 (51.9) | ||
| Some impact | 66 (28.1) | ||
| Major impact | 47 (20.0) | ||
| Impact on physical health | |||
| No impact | 93 (37.1) | ||
| Some impact | 87 (34.7) | ||
| Major impact | 71 (28.3) | ||
| Impact on mental health | |||
| No impact | 94 (37.8) | ||
| Some impact | 87 (34.9) | ||
| Major impact | 68 (27.3) | ||
| Work-Life Conflict | 6.43 (4.30) | 0–14 | |
| None to minor impact (0–3) | 64 (30.5) | ||
| Mild impact (4–6) | 44 (21.0) | ||
| High impact (7–9) | 48 (22.9) | ||
| Major impact (10 or greater) | 54 (25.7) |
| Predictor Variables | Wald X2 | OR | 95% CI |
|---|---|---|---|
| 25 or less days on road/month (reference: 26 or more) | 0.97 | 0.76 | 0.44, 1.31 |
| 11 or less work hours per day (reference: more than 11) | 0.46 | 0.83 | 0.47, 1.44 |
| Same daily schedule (reference: different) | 1.49 | 0.63 | 0.30, 1.32 |
| Same hours per day (reference: different) | 0.38 | 0.84 | 0.47, 1.48 |
| Same days per week (reference: different) | 0.02 | 1.04 | 0.59, 1.83 |
| Frequency of fast pace of work | |||
| Never or rarely | 2.18 | 0.62 | 0.31, 1.18 |
| Sometimes | 0.02 | 1.05 | 0.53, 2.10 |
| Often or always (reference) | - | - | - |
| Supervisor support | |||
| Often or always | 0.22 | 1.32 | 0.43, 3.99 |
| Sometimes | 1.21 | 1.52 | 0.72, 3.23 |
| Never or rarely (reference) | - | - | - |
| Perceived Stress | |||
| None or mild (reference) | 4.18 | 0.45 * | 0.21, 0.97 |
| Moderate | 4.72 | 0.45 * | 0.22, 0.92 |
| High or chronic stress | - | - | - |
| Predictor Variables | Wald X2 | OR | 95% CI |
|---|---|---|---|
| 25 or less days on road/month (reference: 26 or more) | 0.01 | 1.03 | 0.52, 2.04 |
| 11 or less work hours per day (reference: more than 11) | 0.60 | 0.77 | 0.39, 1.50 |
| Same daily schedule (reference: different) | 0.14 | 1.18 | 0.51, 2.73 |
| Same hours per day (reference: different) | 1.22 | 1.48 | 0.74, 2.94 |
| Same days per week (reference: different) | 2.01 | 0.62 | 0.32, 1.20 |
| Frequency of fast pace of work | |||
| Never or rarely | 18.56 | 0.18 *** | 0.08, 0.39 |
| Sometimes | 11.59 | 0.24 *** | 0.11, 0.55 |
| Often or always (reference) | - | - | - |
| Supervisor support | |||
| Often or always | 0.02 | 0.91 | 0.23, 3.65 |
| Sometimes | 1.59 | 1.73 | 0.74, 4.07 |
| Never or rarely (reference) | - | - | - |
| Sleep Duration (workdays) | 14.62 | 0.60 *** | 0.47, 0.78 |
| Sleep Duration (non-workdays) | 7.00 | 1.27 ** | 1.06, 1.52 |
| Sleep Quality (workdays) | |||
| Almost or every night good sleep | 0.01 | 1.03 | 0.46, 2.30 |
| Never or rarely good sleep (reference) | - | - | - |
| Sleep Quality (non-workdays) | |||
| Almost or every night good sleep | 4.71 | 0.32 * | 0.11, 0.90 |
| Never or rarely good sleep (reference) | - | - | - |
| Work-Life Balance (influenced by work/sleep) | |||
| None to minor impact | 1.06 | 0.64 | 0.27, 1.50 |
| Mild impact | 0.52 | 0.71 | 0.28, 1.81 |
| High impact | 0.01 | 1.04 | 0.44, 2.46 |
| Very high impact | - | - | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hege, A.; Lemke, M.K.; Apostolopoulos, Y.; Whitaker, B.; Sönmez, S. Work-Life Conflict among U.S. Long-Haul Truck Drivers: Influences of Work Organization, Perceived Job Stress, Sleep, and Organizational Support. Int. J. Environ. Res. Public Health 2019, 16, 984. https://doi.org/10.3390/ijerph16060984
Hege A, Lemke MK, Apostolopoulos Y, Whitaker B, Sönmez S. Work-Life Conflict among U.S. Long-Haul Truck Drivers: Influences of Work Organization, Perceived Job Stress, Sleep, and Organizational Support. International Journal of Environmental Research and Public Health. 2019; 16(6):984. https://doi.org/10.3390/ijerph16060984
Chicago/Turabian StyleHege, Adam, Michael K. Lemke, Yorghos Apostolopoulos, Brian Whitaker, and Sevil Sönmez. 2019. "Work-Life Conflict among U.S. Long-Haul Truck Drivers: Influences of Work Organization, Perceived Job Stress, Sleep, and Organizational Support" International Journal of Environmental Research and Public Health 16, no. 6: 984. https://doi.org/10.3390/ijerph16060984