1. Introduction
According to the Joint Monitoring Program (JMP) on Water, Sanitation and Hygiene [
1], approximately 844 million people lacked basic drinking water and 2.3 billion were without basic sanitation in 2015 with significant disparities across regions. Although sub-Saharan Africa (SSA) made modest progress in water and sanitation access between 1990 and 2015, 72% of its population are without basic sanitation at the end of the Millennium Development Goals (MDG) period [
1]. Poor sanitation has overwhelmingly been approached as a health concern related to the consumption of water and food contaminated with fecal bacteria. Diarrhoeal disease accounts for about 8.6% of under-five mortality worldwide [
2], and inadequate water and sanitation have been associated with diarrhoea [
3,
4].
For decades, sanitation approaches adopted by governmental and non-governmental organizations assessed the sanitation needs of households and provided either free or subsidized latrines [
5]. These approaches did not address the issues of sanitation behaviour change and community empowerment that could promote sustained access to improved sanitation [
6,
7]. Following these results, Community-Led Total Sanitation (CLTS) was adopted. This approach focuses on behavioural change to create “open defecation free (ODF) communities” [
8]. CLTS approaches open defecation as a collective health hazard, triggers communities for change, and inspires local innovation and mutual support for latrine construction and latrine use.
Although CLTS has significantly facilitated the process of stopping open defecation [
9], the 75% latrine coverage threshold required for improved health has not yet been reached [
10,
11,
12], and problems persist with the long-term sustainability of latrines [
13]. In general, research has shown that the adoption and sustained use of latrines is largely rooted in the social norms and networks of communities [
14,
15] and the rate of adoption of sanitation behaviours varies amongst households [
16]. Therefore, households’ decision to construct and use a latrine may be influenced by the social norms of the community. While research on CLTS in developing countries has been extensive [
10,
13,
16], few studies examine why people change their behaviour from a psychosocial perspective. However, understanding the mechanisms underlying behaviour change interventions is germane to improving its effectiveness [
17].
To understand latrine completion and use decisions among households, we used the Risks, Attitudes, Norms, Abilities, and Self-regulation (RANAS) model of behaviour change [
18] as a conceptual guide. The RANAS model underscores the importance of psychosocial factors in determining households’ sanitation behaviours [
13,
19,
20,
21,
22]. The risk factors represent a person’s understanding of the health risk of open defecation, the person’s perceived perception of his or her risk of contracting diarrhoea, and his or her perception of the severity of diarrhoea and its consequences. The attitude factors are a person’s beliefs about the costs (money and time/effort) and benefits (good health, greater respect, personal safety) of constructing a latrine and his or her positive feelings about owning a latrine. Norm factors represent the perceived social pressure to construct a latrine. They describe a person’s observation and awareness of others’ behaviour, his or her perception as to which behaviours are typically practised. Norm factors also describe a person’s perception as to which behaviours are typically practised approved or disapproved by relatives, friends, or neighbours. This includes the awareness of the dos and don’ts expressed by a village, tribe, or religious leaders and other institutions. The ability factors take three forms: confidence in performance (a person’s perceived ability to organize and execute latrine construction), confidence in continuation (a person’s perceived ability to continue latrine construction and ability in being able to deal with barriers that arise), and confidence in recovering (a person’s perceived ability to recover from setbacks, to continue the construction and after disruptions). Self-regulation factors denote a person’s strategies for constructing a latrine; his or her plans for overcoming potential barriers in the course of latrine construction; and monitoring to keep construction on track.
The psychosocial factors are embedded in contextual landscapes that may also influence latrine construction decisions. Psychosocial characteristics include social, physical, and personal factors. The social context represents the cultural and social relations, policies and laws, economic conditions (household’s income), and the information environment (including sanitation campaigns such as CLTS). Jenkins and Scott [
23] argue that the cost of household latrines is a significant constraint on latrine construction. Yet, researchers [
24,
25] have stated that the policies and legislation on sanitation are least accessible to marginalized groups in ways that limit their ability to switch to latrine use. In CLTS, social relations and cohesion among community members are key for collective actions and mutual support in latrine construction [
20].
The physical context includes the natural and built environment. For instance, whether the soil is loose or firm has to be considered when choosing the best fit design for latrine substructure so as to prevent latrine collapse. Finally, the personal context is framed by socio-demographic factors such as age, sex, religion, and education. Some studies [
26,
27,
28] have shown that latrine construction and use is associated with households’ educational status, though Oljira and Berkessa [
29] proposed a contrary view.
In a study commissioned by the World Health Organisation (WHO), Garn et al. [
11] reported that latrine coverage and ownership do not necessarily translate into latrine use. Even among households with latrines, open defecation is often still practised [
30,
31]. However, little is known about the households that have not been able to complete the construction of their latrines during CLTS interventions. In addition, the existing literature has not examined how level of latrine completion is associated with defecation habits among households. Achieving the Sustainable Development Goals (SDGs) is likely to be aided by better understanding of the factors associated with levels of latrine completion and consequent latrine use. This can inform effective targeting of interventions to increase sanitation coverage and subsequently improve health. Consequently, this study addresses the following questions:
- (1)
How do the levels of latrine completion relate to latrine use?
- (2)
How are socio-demographic characteristics of households linked to levels of latrine completion?
- (3)
What factors may deter households of different latrine completion levels from using their latrines?
- (4)
How do psychosocial factors differ between households’ latrine completion levels?
- (5)
How do reported reasons for latrine building differ between households’ latrine completion levels?
2. Methods
2.1. Research Context and Sampling
This study was conducted in two neighbouring districts: Bole district and Sawla-Tuna-Kalba district in the Northern Region of Ghana. The Ghana Multi Indicator Cluster Survey (MICS) conducted in 2012 [
32] revealed that about 71.9% of residents in the Northern Region practiced open defecation. At the district levels, similar results were observed with about 69.2% and 91.6% of the population defecating openly in Bole and Sawla-Tuna-Kalba Districts, respectively [
33]. To address the sanitation menace, Global Communities, a Non-Governmental Organisation in collaboration with the local governments of the two districts implemented CLTS in the last quarter of 2016. Baseline data was collected prior to the intervention and a follow-up survey was conducted 4–6 months after the intervention was implemented. End-line data for the intervention was collected 14–16 months after the intervention from February to March, 2018. During the baseline, 25 households were randomly selected from each community following Hoffmeyer-Zlotnik [
34] random route method. Equal chances were given to both men and women to participate in the survey, because both might be involved in decisions concerning latrine construction. Respondents for the baseline survey were interviewed again in the follow-up surveys. Every participant gave informed written consent to participate in the interviews. The ethical board of the University of Zurich, Switzerland and the Ethical Review Committee of the Ghana Health Service (GHS-ERC: 05/01/2016) approved this research trial.
2.2. Data Collection
A team of three supervisors and 33 local data collectors were recruited for data collection. The unit of study was the household, defined in this context as a person or group of people who live together in a dwelling and share housekeeping and cooking arrangements. Before data collection, one week of training was organized for the three field supervisors. After training the field supervisors, the data collectors were trained for another week. The training included discussing and interpreting and translating the survey questions into the various local languages (Brefo, Dagare, Gonja, Safalba, Twi, Mo and Waali) spoken in the study area to ensure the team understood the questions and the study. During the training, data collectors were grouped by language to rehearse the questions and to help each language group to adopt uniform words and terminologies. This was followed by role-plays at both the language group and general group levels to test data collectors’ interview and communication skills. The questionnaire was pretested in two days in four communities, and debriefing took place after every day of the pretest to share field experiences and adapt the instrument as necessary. The survey and questionnaire asked about socio-demographic characteristics, open-defecation habits, latrine construction and latrine use, psychosocial determinants of latrine construction and latrine use of households, and the physical and social context of the communities. The survey included some observations, which were recorded by the data collectors based on their individual judgement and joint decisions taken during training. The research manager and the field supervisors monitored the data collectors closely when the questionnaire was administered. Every data collector was assigned five respondents daily, and the research manager crosschecked the interviews for data quality after every day of data collection.
2.3. Measures
2.3.1. Latrine Construction
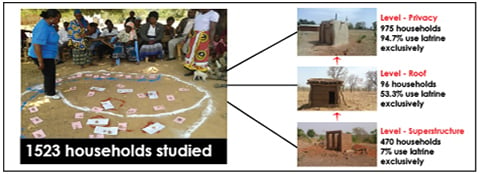
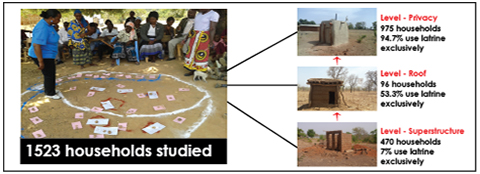
Latrine construction was derived from the question ‘Does your household have its own latrine?’ and coded as 0 = no household latrine; and 1 = household latrine. Since our focus is on households latrine construction levels and corresponding use, we dropped those with no household latrine. This resulted in an analytical sample of 1523 households.
2.3.2. Latrine Usage
Latrine use of respondents was measured by a series of questions that sought to assess respondents’ defecation habits in the morning, midday, and evening of the 7 days prior to the interview. For open defecation, the question ‘how many of the last 7 mornings did you defecate in the open?’ was asked. Respondents were also asked ‘how many of the last 7 mornings did you defecate in the latrine?’ to assess their latrine use in the previous 7 days. Based on the responses given, data collectors were asked to decide whether to code the respondent 1 = use latrine exclusively, 2 = defecate in the open exclusively and 3 = use latrine and does open defecation. For this analysis we added the mixed users to the open defecation group.
2.3.3. Socio-Demographic Factors
Socio-economic and demographic factors included in the study were individual monthly income, highest formal education attainment, marital status and age. Household characteristics included household size, number of children, number of children under 5 years, and number of adult men and women (above 17 years).
2.3.4. Psychosocial Determinants
These were assessed using the RANAS approach [
12,
18]. All questions were answered on a 5-point Likert scale. We used a visual scale of 5 black points of varying sizes to guide respondents select one of answering options. Data collectors read out every option to the respondent while indicating it on the visual scale.
2.3.5. Level of Latrine Construction
Level of latrine construction was reported by respondents and physically verified by data collectors. We categorised construction into five levels. Level 1: Only pit is dug; Level 2: Pit is dug and superstructure constructed; Level 3: Pit is dug, superstructure constructed, and latrine is roofed; Level 4: Pit is dug, superstructure constructed, latrine is roofed and has door; and Level 5: Pit is dug, superstructure constructed, latrines is roofed, and latrine has door and a vent pipe. These levels are described in the results.
2.4. Data Analysis Procedure
To answer the first research question, we classified households into five groups based on the stages of their latrines construction as described in the measures above. After this classification, we used Chi-square tests to determine the statistical difference in the latrine use and open defecation habits between the five levels. Using the results of the Chi-square test, we re-grouped the households into three levels based on the probable influencers of latrine use. These three levels are: (1) households that only dug the pit and constructed superstructure; (2) households that dug the pit, constructed superstructure, and roofed the latrine; and (3) households that dug the pit, constructed superstructure, roofed latrine, and fitted door and vent pipes. Two levels were compared at a time (Level 1 vs. Level 2 and Level 2 vs. Level 3).
To answer the remaining research questions, we again compared the three levels of latrine completion progressively. An ANOVA was used to test the socio-demographic factors, psychosocial factors, and other factors that may be linked to latrine construction and use between the three levels. For multiple response items, we did not test the statistical significance between the percentages but reported them relatively. All data analysis was carried out using SPSS version 22 (IBM SPSS Statistics for Windows, Version 22.0. IBM Corp, Armonk, NY, USA).
4. Discussion
In this study, we examined factors associated with levels of latrine completion and use in CLTS intervention communities in Northern Ghana. We found that households that roofed their latrines are more likely to switch from open defecation. Households would more likely switch from open defecation to latrine use if latrines protect their privacy. Existing literature on CLTS indicates that convenience, comfort, and health benefits are recurring reasons for latrine use [
19,
20]. Similarly, a study on rural sanitation showed that privacy and safety are the major reasons for latrine construction and use among women [
35]. Other possible reasons related to latrine use among the study households include the cleanliness of the latrine and its structural condition. However, having a latrine did not always translate into latrine use [
30]. We observed that about 5.3% (
Table 2) of households at level-privacy still practise open defecation. We also found that people are less likely to use latrines when they are dirty and damaged. Latrines that have roof and protect user privacy were also found to be cleaner. These structural characteristics that influence latrine use could be used as benchmarks against which constructed latrines could be measured in CLTS.
The factors influencing latrine construction and use are broadly classified into demographic and socio-economic factors, knowledge and attitudes, and social influence [
13,
15,
19,
20,
35,
36]. Although we did not find significant differences between household size, age, marital status or literacy rates among respondents across the levels of latrine completion, other research works have reported the influence of these factors on latrine construction and use [
36,
37,
38]. These socio-demographic factors could be further investigated in the study area. Research on economic predictors of latrine ownership in developing countries is not rare. Studies have shown that households with the highest incomes are the most likely to construct latrines [
16,
39,
40]. Household income affects the availability of resources for latrine construction. However, we found in this study that households with the highest incomes were at the lowest level of latrine construction (
Table 2). It has also been suggested that, despite the impact of income on latrine construction, other contextual factors drive latrine construction decisions [
16,
19,
20,
37].
The RANAS factors were used to examine the latrine construction behaviours of households that might have contributed to the construction of latrines in the study area. The perceived risk of diarrhoea was significantly higher for households who constructed only pit and superstructure, while the ownership of a complete latrine as well as latrine use reduced the perceived risk. The perceived risk of a practice has the potential to stimulate and shape households’ behaviours [
41,
42,
43]. However, though risk perception may evoke precautionary measures [
44], it is not a determinant of preventive health behaviours [
45]. The adoption of healthy behaviours is dependent upon the social process triggered by CLTS [
20], social norms [
13,
19], social networks, and social capital [
15,
36]. For example, one qualitative study conducted in Benin found prestige to be the main motivation for latrine construction, which had little to do with health risk [
46]. In our study, respondents expressed a general feeling of pride in latrine ownership, although those at level-superstructure perceived latrines to be very expensive to construct. CLTS processes produce norms and social networks between members of the community and also with their external environment. Through these social processes, individuals exchange knowledge and ideas and adopt the healthy behaviours of one another whilst strengthening social cohesion and inclusion. In this study, we found that the construction of latrines by relatives and kinsmen has a snowball effect that motivates other community members of the same kin to construct. This result supports previous findings by Shakya et al. [
36], which showed that latrine ownership among an individual’s caste is a significant influencer of an individual’s latrine ownership.
In the study, chiefs, opinion leaders, and family heads played an important role in establishing a norm of latrine construction and use and ending open defecation. Their collective actions brought authority and legitimacy to the whole process of CLTS in their communities and boosted the collective efforts of community members. In both study districts, communities that perceived strong approval of CLTS by their chiefs and opinion leaders had attained ODF status before the endline. Consistent with this finding, a study in Koassanga, Burkina Faso, showed that chiefs and community leaders played a significant role in ensuring collective actions for ending open defecation [
15]. In health promotion literature the active involvement of chiefs in the CLTS process enables communities to develop their own context-specific activities to end open defecation and the sustainability of community initiatives on sanitation [
15].
Although several researchers and practitioners of CLTS have argued that subsidies may undermine households’ motivation to construct latrines [
47,
48], our results revealed that subsidies were not a primary driver for latrine construction, however, they helped some households improved the structure and design quality of the latrines. Similarly, a cluster-randomized trial study in Bangladesh by Guiteras, Levinsohn, and Mobarak [
49] reported that CLTS latrine construction and latrine use was high among households that received subsidies. In addition to subsidies, monitoring the progress of latrine construction in follow-up visits has been found to have a positive impact on latrine construction and use. Follow-up visits motivate households and provide opportunities to seek technical guidance from field facilitators. Venkataramanan et al. [
12] amply acknowledged the influence of follow-up visits on latrine construction and latrine use.
Looking at the levels of latrine completion separately, households at level-superstructure are at the lowest stage of latrine construction, and open defecation is widely practised among these households. Households at level-superstructure generally expressed higher perceived risk of contracting diarrhoeal disease. They perceived latrine construction to be expensive although they recorded the highest average income. These households have the least clean latrines and would not defecate in their latrines when they are dirty, smelly, or damaged. They have fewer community members and relatives who constructed latrines. In addition, our results suggest that these households had less interaction with field facilitators and also received fewer subsidies than households in other levels of latrine construction. Similarly, a study by Slekiene and Mosler [
16] in rural Malawi revealed that households that slowly adopt the innovation of latrine ownership perceived latrine construction to be expensive, communicate less with people about latrines and also feel more vulnerable to contracting diarrheal diseases. Furthermore, Shakya et al. [
36] revealed that households social networks significantly influenced their latrine ownership and those with fewer networks are less likely to own latrines.
Different from households at level-superstructure, those at level-roof recorded the lowest average income and their latrines provide no privacy to users. Therefore, latrine use by households at this level is relatively low compared to level-privacy. Households at level-roof perceived they have more relatives and community members who constructed latrines than did households at level-superstructure. More households at this level reported they received a subsidy than in level-superstructure.
At level-privacy, households have completed latrines, and open defecation is less practised. Although household latrines at his level are clean, these households would not use latrines when they are dirty or smelly. Households at this level expressed less perceived risk of contracting diarrhoeal diseases but constructed latrines to improve household health and privacy during defecation. They perceived that they have more community members who constructed latrines than do level-roof households, and other important people like family, friends, chiefs and opinion leaders have a significant influence on their latrine construction. These households expressed strong commitment to complete latrine construction even when they encounter challenges. We also observed that level-privacy households had a great deal of interaction with field facilitators and also received more subsidy than households at the other levels.
The sustainability of latrine use is reported to be a great challenge, as it is common for people to abandon full-pit, damaged, or uncompleted latrines and return to open defecation [
13,
37,
50]. This study revealed that households were distributed across different levels of latrine completion and that latrine use varied amongst these levels. Although respondents expressed stronger commitment to complete latrine construction and continued latrine use, continued sensitization is required to sustain their new sanitation behaviour after the departure of project implementers. Scaling-up would therefore require the local planning and development authorities to enhance social marketing campaigns on sanitation to facilitate households to meet their sanitation needs, maintain good sanitation behaviours and create opportunities to act and overcome constraints [
46].
Some limitations are worth acknowledging, which readers should consider when interpreting the study findings. First, this study used reported family income for the analysis, which does not measure the wealth of households. Respondents may be biased in reporting their real income levels. Second, although we acknowledged the strong relationship between water and sanitation, and households’ health, our research did not discuss this relationship because the whole study was conceptualised on the impact of CLTS intervention on households latrine construction and use. Perhaps, latrine cleanliness may have been influenced by water access and availability. Fourth, all psychosocial determinants were self-reported and measured at endline. Future research should control for multiple comparison errors. Also, as the global community monitors progress on sanitation within the framework of the Sustainable Development Goals, an in-depth understanding of the barriers and complexities associated with sanitation access will inform policy. In this regard, we recommend future research on the relationship between gender, impairment and sanitation access (see [
51,
52,
53]).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}