Since the 1930s, there have been several famous atmospheric pollution events around the world, such as the Meuse Valley fog in Belgium, the photochemistry smoke event of Los Angeles, USA, the London smog episode in the United Kingdom and the asthma in Japan, which not only have caused huge economic losses, but also cost the health and lives of residents [
1]. Among various atmospheric pollutants, fine particulate matter (PM
2.5) is widely considered as the culprit causing health losses of residents due to its characteristics of small particle size, remote transmission distance, long duration, richness in toxic substances, and the ability to destroy the body’s blood circulation system [
2,
3,
4]. According to the global burden of disease study, PM
2.5 pollution caused approximately 4.2 million deaths, leading to 103 million losses of disability adjusted life years (DALYs) in 2015, and PM
2.5 has become the fifth leading cause of death [
5,
6]. With the rapid progress of industrialization and urbanization, China is also faced with a severe atmospheric pollution problem. Haze weather, which is typically represented by PM
2.5, occurs with a high frequency, a wide range and an unprecedented degree of harm, and it has become an important issue affecting China’s environmental quality, residents’ health and sustainable social development. It is estimated that PM
2.5 pollution in Beijing city caused more than 20,000 deaths and more than 1 million people to fall ill, resulting in direct economic losses of approximately
$147.62 million in 2013 [
7]. Therefore, it is of great significance to evaluate the health losses of residents induced by PM
2.5 pollution and to calculate their economic value for promoting the prevention of atmospheric pollution and implementing China’s health strategy.
Non-Chinese scholars’ studies on the health losses of atmospheric pollutants can be traced back to the 1960s. Ridker [
8] estimated that the economic value of residents’ health losses induced by SO
2 pollution in the United States in 1958 was
$80.2 billion using the human capital method, which became the beginning of quantitative assessment of the health effect of atmospheric pollutants. Dockery et al. [
9] used the cohort study method to track the PM
2.5 concentration and the health status of more than 8,000 residents in six cities in the United States, and they found that the death risk would increase by approximately 14% for every 10 μg/m
3 increase in PM
2.5 concentration. Based on the data of PM
2.5 concentration and health information of 552,138 adults in 151 large cities in the United States from 1982 to 1989, Pope et al. [
10] revealed that every 10 μg/m
3 increase in PM
2.5 concentration resulted in a 4.0% increase in all-cause mortality and an 8.0% increase in cardiopulmonary disease mortality, respectively. Katanoda et al. [
11] observed the health effects of concentration changes in various air pollutants in Japan on 63,520 respondents from 1983 to 1985, and they found that the increase in PM
2.5, SO
2, and NO
2 concentration lead to the increase in the death risk by lung cancer among residents. Among them, the death risk of lung cancer increased by 1.24% (95% CI: 1.12%, 1.37%) for every 10 μg/m
3 increase in PM
2.5 concentration; the death risk by lung cancer increased by 1.26% (95% CI: 1.07%, 1.48%) and 1.17% (95% CI: 1.10%, 1.26%) for each 10 ppb increase in SO
2 and NO
2 concentration. The study Atmospheric Pollution and Health: a European Approach (APHEA) showed that for every 10 μg/m
3 increase in PM
10 concentration, the hospitalization risk of asthma and chronic obstructive pulmonary disease (COPD) increased by 1.0% (95% CI: 0.4%, 1.5%) and by 0.5% (95% CI: 0.2%, 0.8%) for cardiovascular disease among people who were over 65 years old [
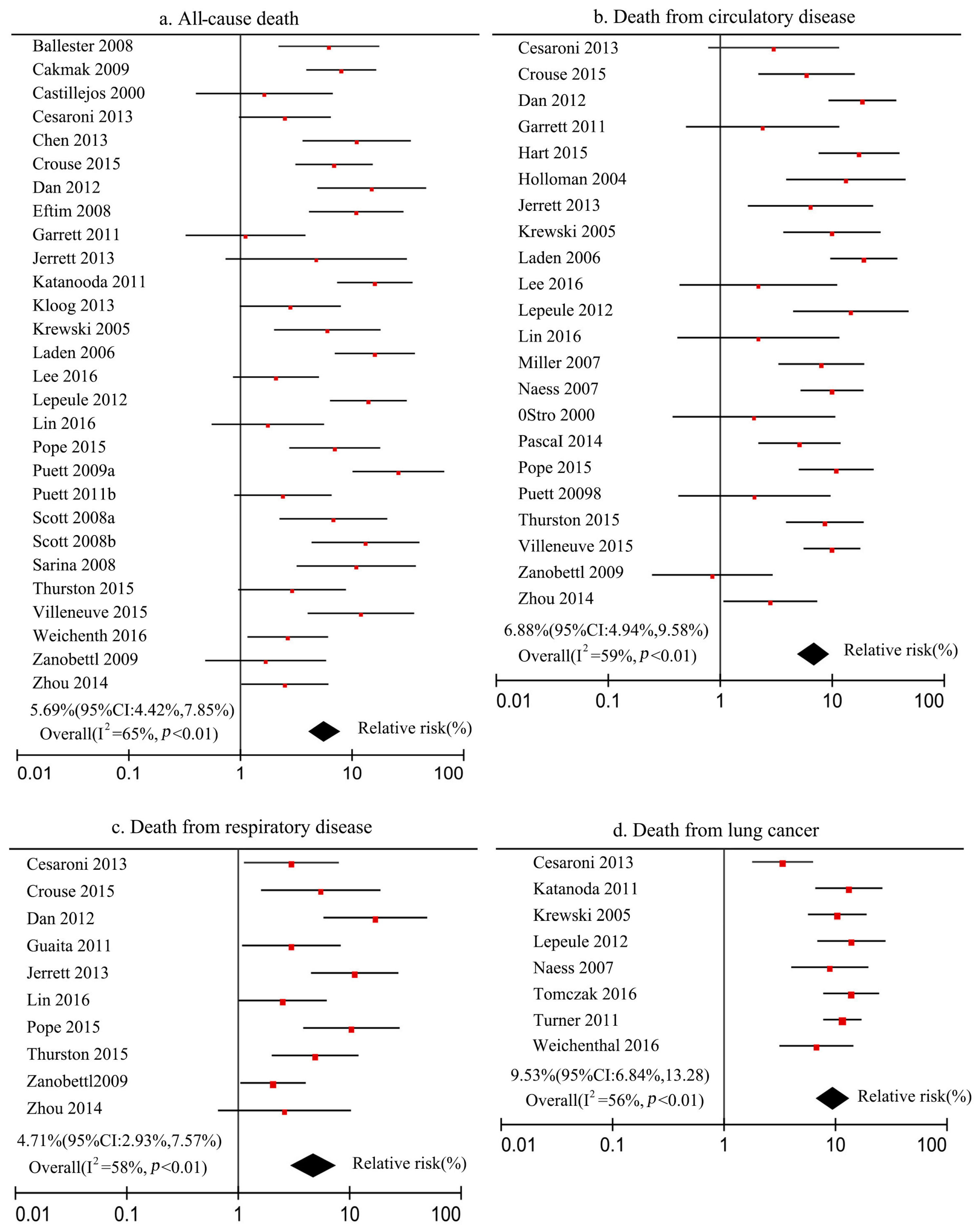
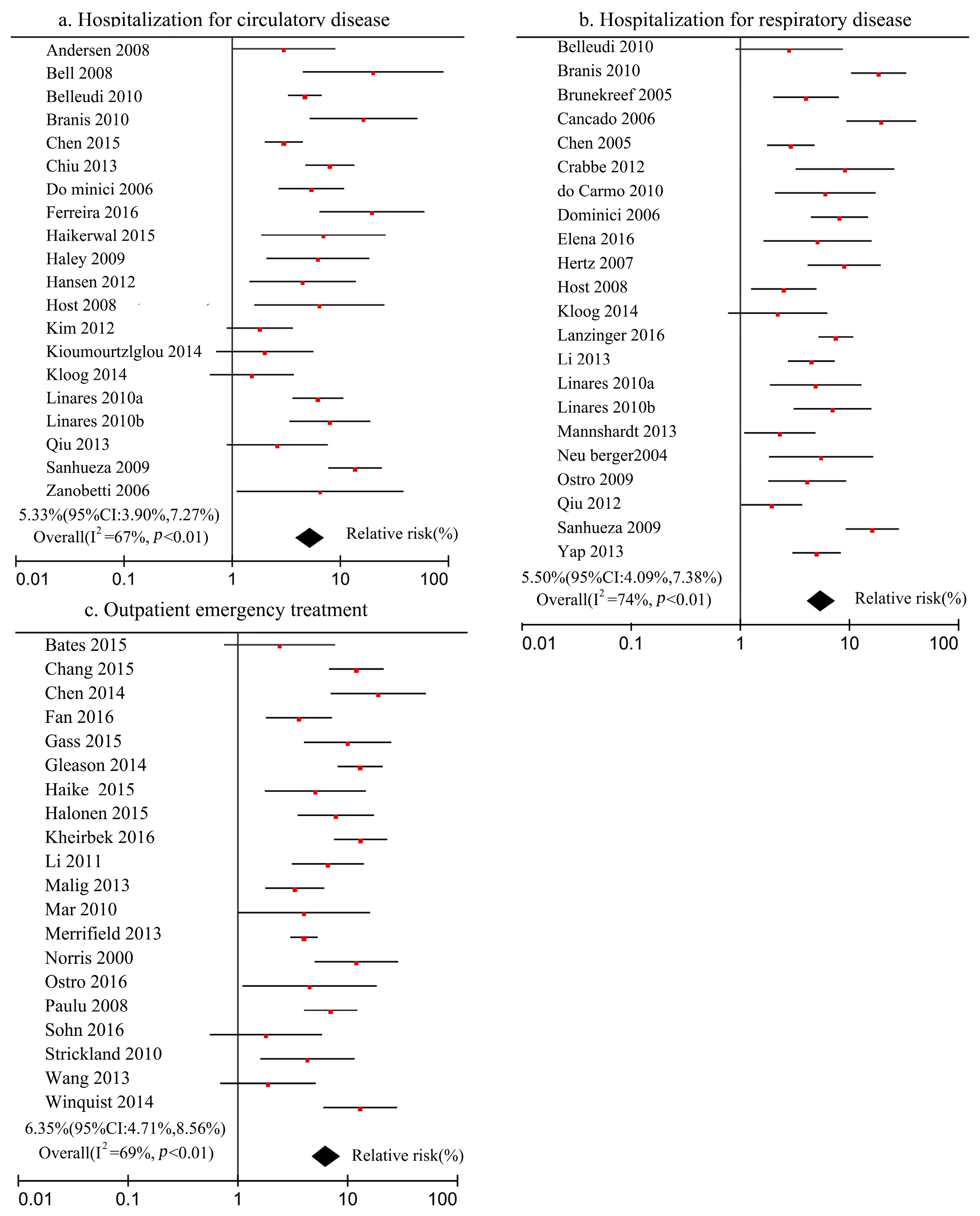
12]. The increase in epidemiological cases makes it possible to obtain the exposure–response coefficient outside the case area by using the meta-analysis method, which also lays a solid foundation for accounting for the health losses due to air pollutants. Seethaler et al. [
13] used the willingness-to-pay method to evaluate the economic value of health losses induced by PM
10 pollution in Austria, France and Sweden in 1996 as €27 billion, accounting for 1.7% of their GDP in the same year. Quah et al. [
14] used the environmental damage function and the dose–response method to estimate that the economic value of health losses caused by PM
10 pollution in Singapore in 1999 was
$3.662 billion, accounting for 4.31% of the GDP of that year. Chinese scholars started paying attention to the economic value of health losses caused by atmospheric pollution more recently; Guo et al. [
15] calculated the harm to human health due to SO
2 pollution in China in 1985 with the help of human capital approach, and they concluded that the health losses of residents were
$1.28 billion. Chen et al. [
16] estimated the health losses induced by PM
10 pollution and their economic value in 113 Chinese cities in 2006, and they found that PM
10 pollution caused 299,700 deaths, 254,900 hospitalizations and 7,625,100 medical outpatient visits, with an economic value of
$43.72 billion. Based on the calculation of the health losses of residents caused by PM
2.5 pollution in the Beijing–Tianjin–Hebei region, Huang et al. [
17] believed that the health benefits of controlling PM
2.5 pollution in this region could reach
$28.36 billion. In addition, some scholars believed that the above methods only included the direct value assessment of health losses, so they advocated including the labor losses and medical expenses caused by atmospheric pollution in the model, so as to estimate the indirect impact of atmospheric pollution on the macro economy [
18,
19]. Through reviewing relevant literature, it is found that the current research has the following problems: (1) The exposure–response coefficient is the key to calculating the health and economic losses of residents induced by PM
2.5 pollution. Due to the lack of epidemiological research cases in China, existing studies mostly refer to the results of the exposure–response coefficient in other countries [
20]. However, the difference in PM
2.5 pollution between China and other countries determines that using only foreign exposure–response coefficients will lead to a deviation of the evaluation results. (2) The current value assessment of health losses induced by PM
2.5 pollution focuses on the death effect, and it pays insufficient attention to the pathogenic effect of PM
2.5 pollution [
21,
22]. In fact, PM
2.5 pollution not only increases the number of deaths, but also greatly increases the number of patients at different health endpoints. Therefore, measuring health losses from the perspective of the death effect is a one-sided approach. (3) The statistical life value determined by using the willingness-to-pay method is the main method that measures the unit value of death loss; however, most of the existing studies directly refer to the investigation of the residents’ willingness to pay for reducing atmospheric pollution health hazards carried out in the early stage in China, which has the defect of poor timeliness, and this will eventually affect the values of the calculated health losses [
23,
24,
25,
26].
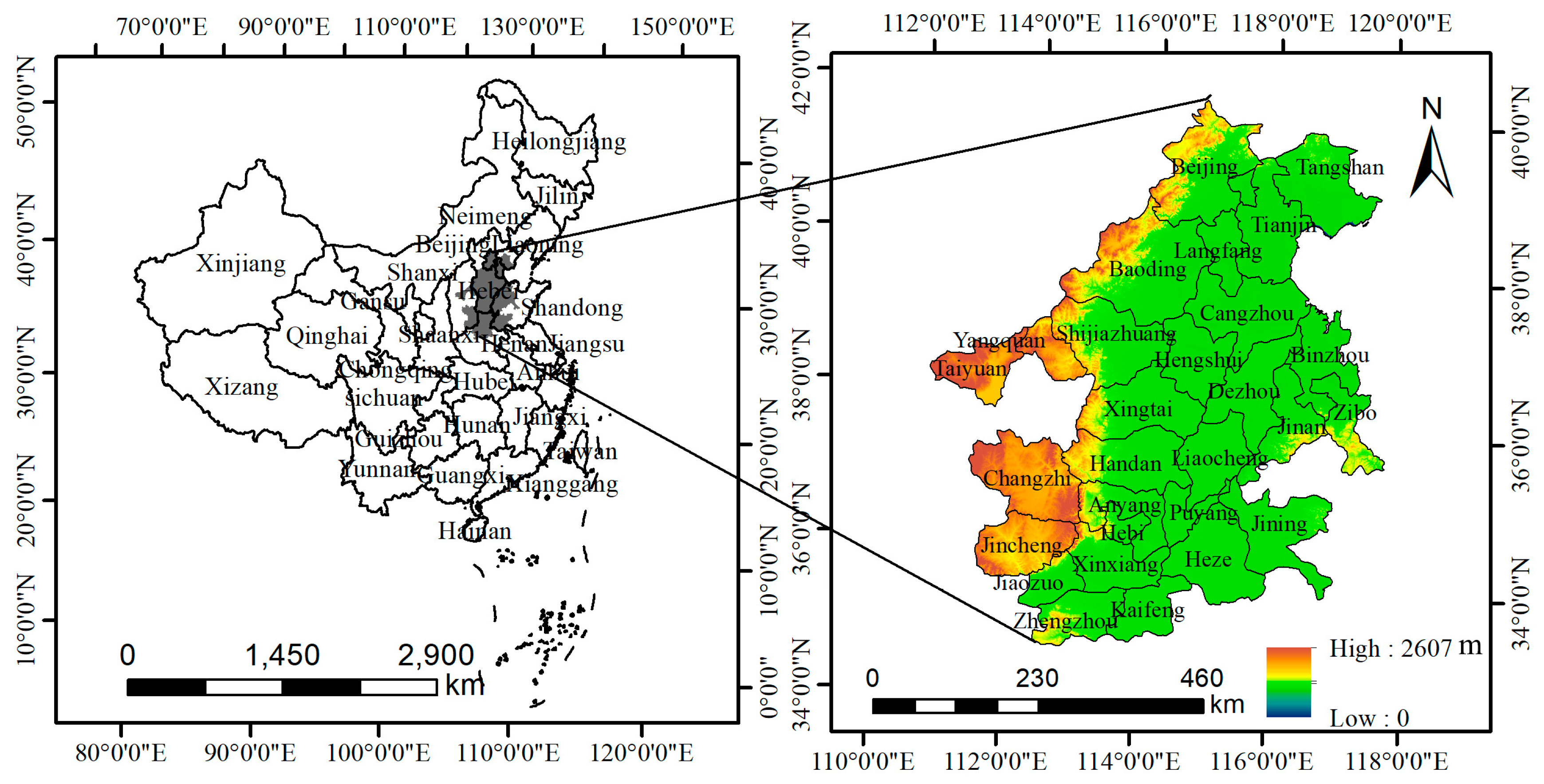
Work plan on atmospheric pollution prevention and control in the Beijing–Tianjin–Hebei region and surrounding areas issued by the Ministry of Environmental Protection of China and relevant departments in 2017 indicated that Beijing, Tianjin, Shijiazhuang, Tangshan, Langfang, Baoding, Cangzhou, Hengshui, Xingtai, Handan, Taiyuan, Yangquan, Changzhi, Jincheng, Jinan, Zibo, Jining, Dezhou, Liaocheng, Binzhou, Heze, Zhengzhou, Kaifeng, Anyang, Hebi, Xinxiang, Jiaozuo, and Puyang collectively constituted the atmospheric pollution transmission channel in the Beijing–Tianjin–Hebei region, which was identified as a key area for the prevention and control of atmospheric pollution (
Figure 1). According to data released by the Chinese City Statistical Yearbook, the population density of the region in 2016 was 701 persons/km
2, while the national average population density was 144 persons/km
2, so the region is a densely populated area in China [
27]. However, the PM
2.5 pollution in this region was extremely severe, with an average PM
2.5 concentration of 71 μg/m
3 in 2016, which was 7 times the guideline value issued by the World Health Organization, and posed a serious threat to the residents’ health [
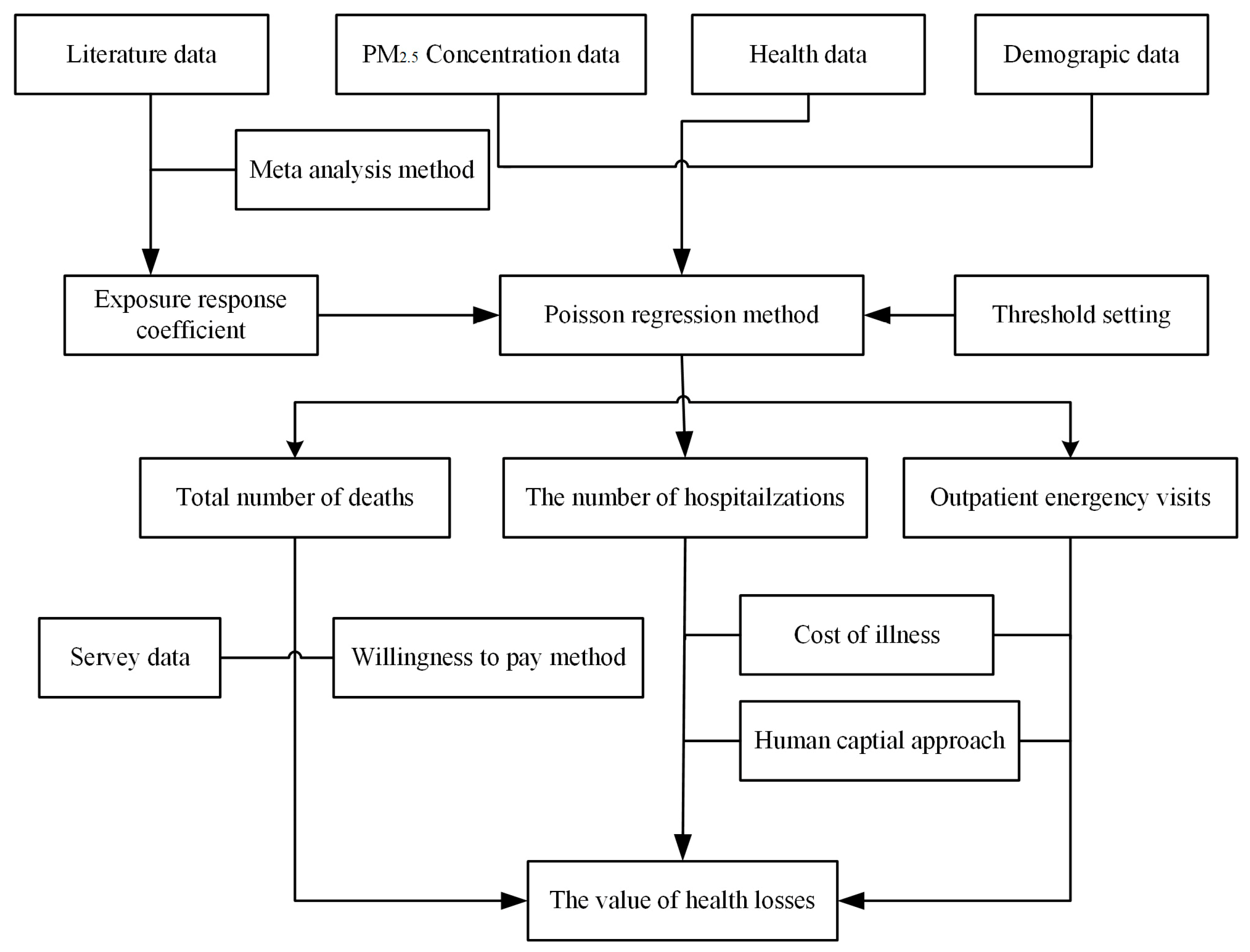
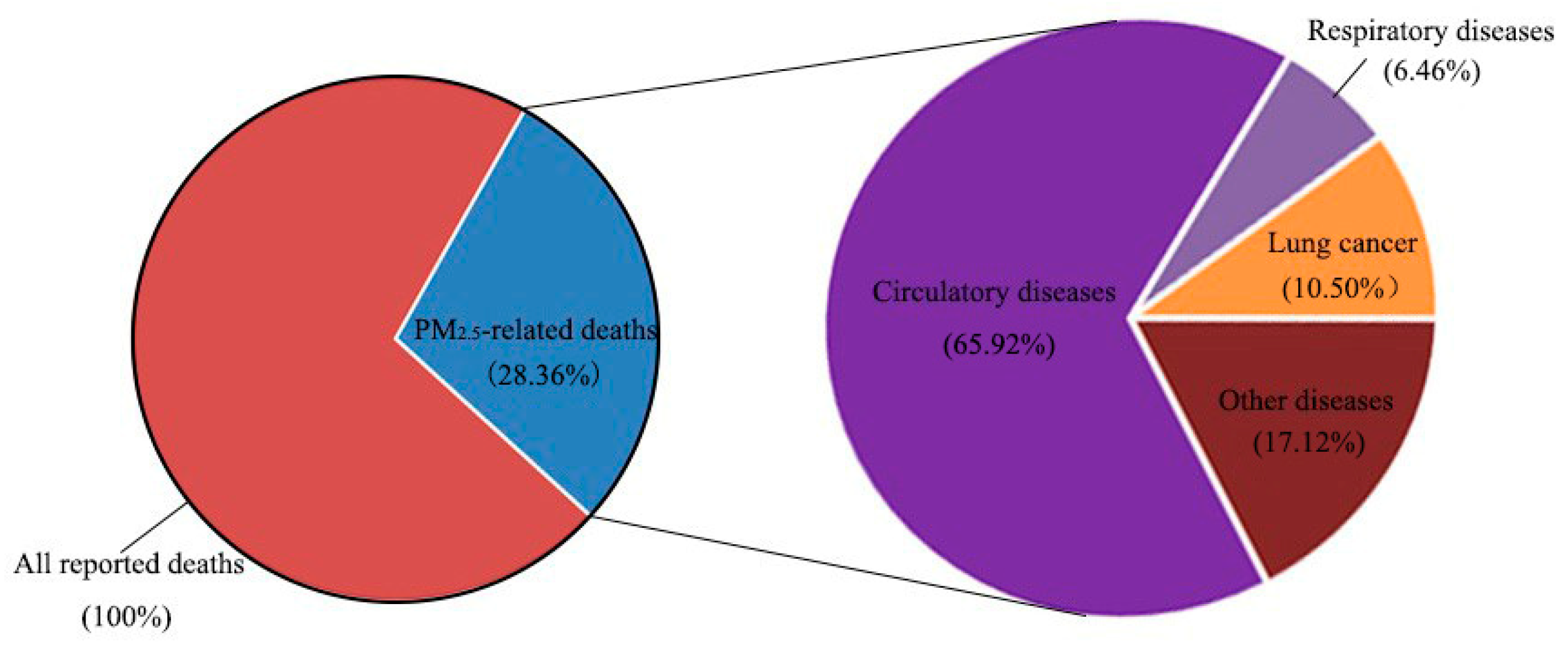
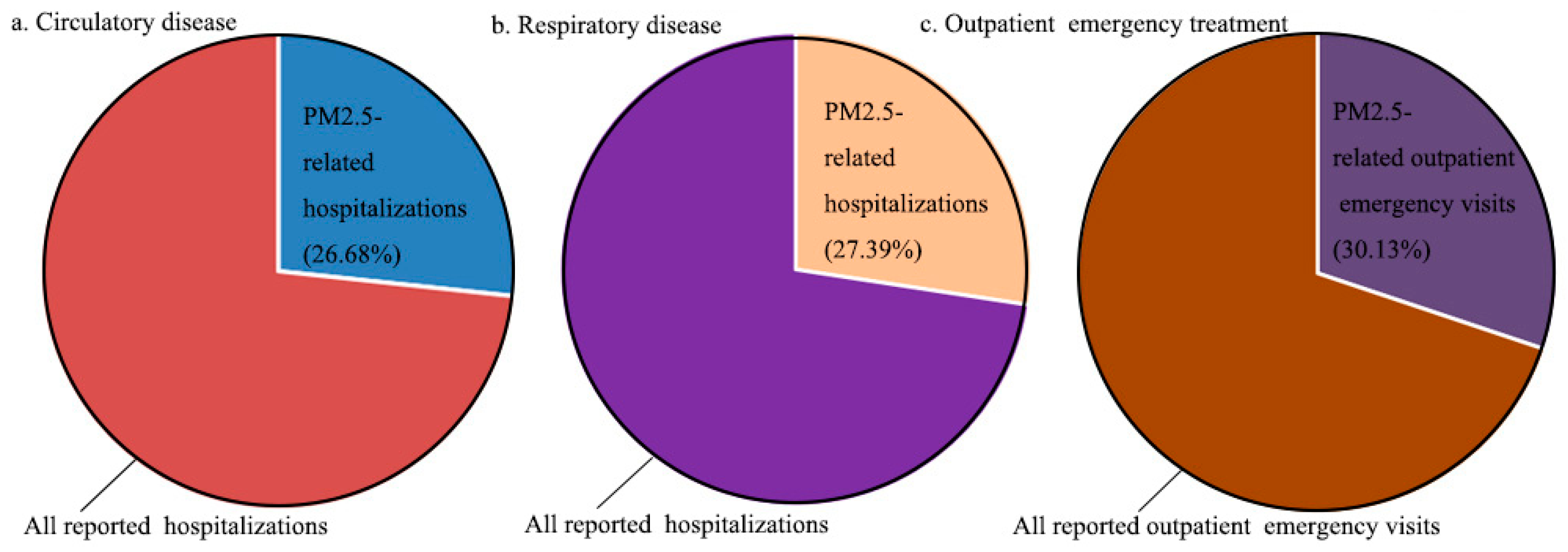
28]. Therefore, this paper uses the meta-analysis method and the Poisson regression model to estimate the number of deaths, hospitalizations, and outpatient emergency visits caused by PM
2.5 pollution in cities of atmospheric pollution transmission channel in the Beijing–Tianjin–Hebei region in 2016 based on the data from literature, remote sensing data, statistical data, and survey data. Besides, the environmental value evaluation method is used to calculate their economic value, which is beneficial to provide a reference for relevant departments that formulate environmental and health policy.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}