Mediterranean Built Environment and Precipitation as Modulator Factors on Physical Activity in Obese Mid-Age and Old-Age Adults with Metabolic Syndrome: Cross-Sectional Study

 ,
,  , ,
, , 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
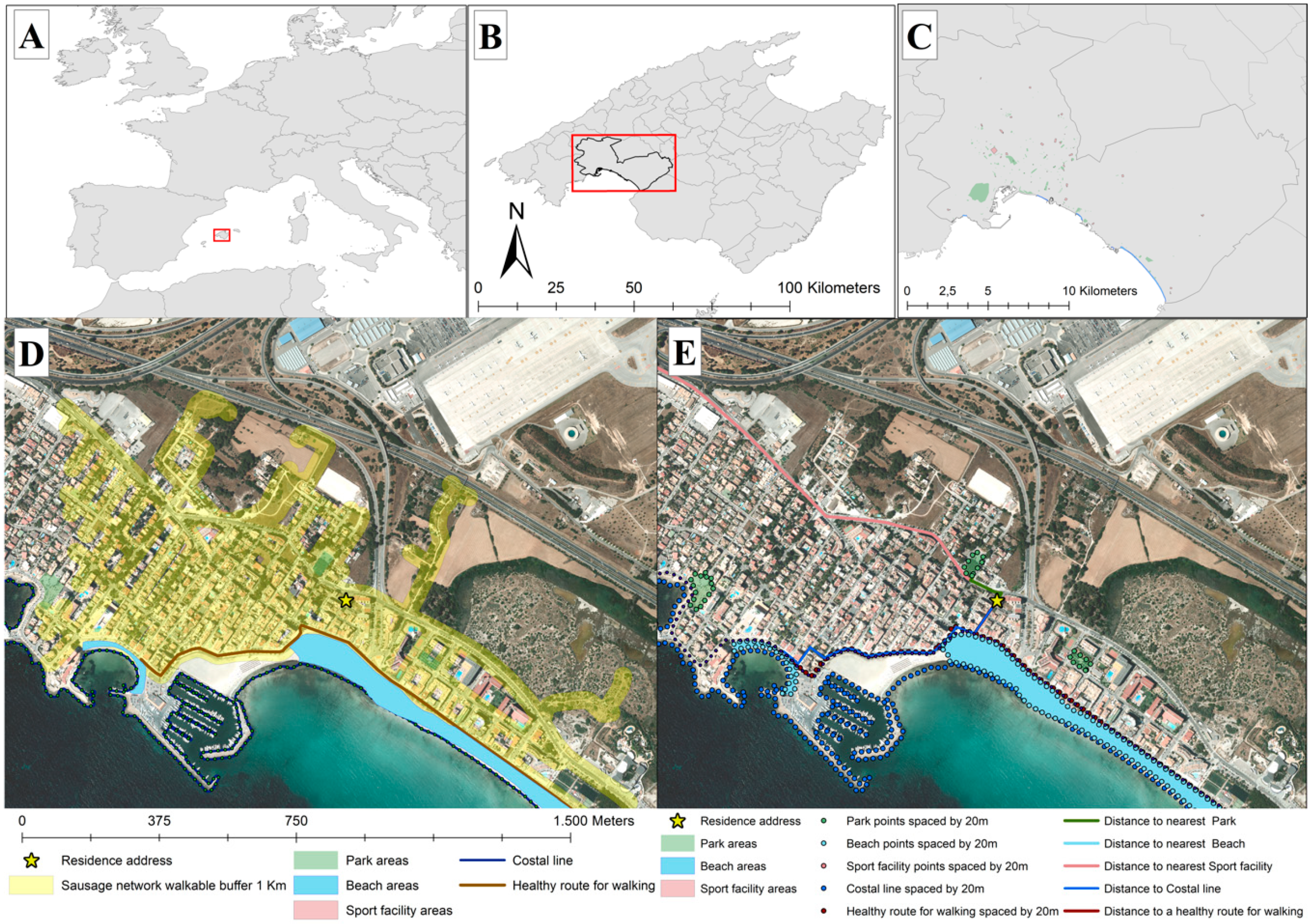
2.2. Neighborhood Exposure to Walk-Friendly Routes and Public Open Spaces (POS)
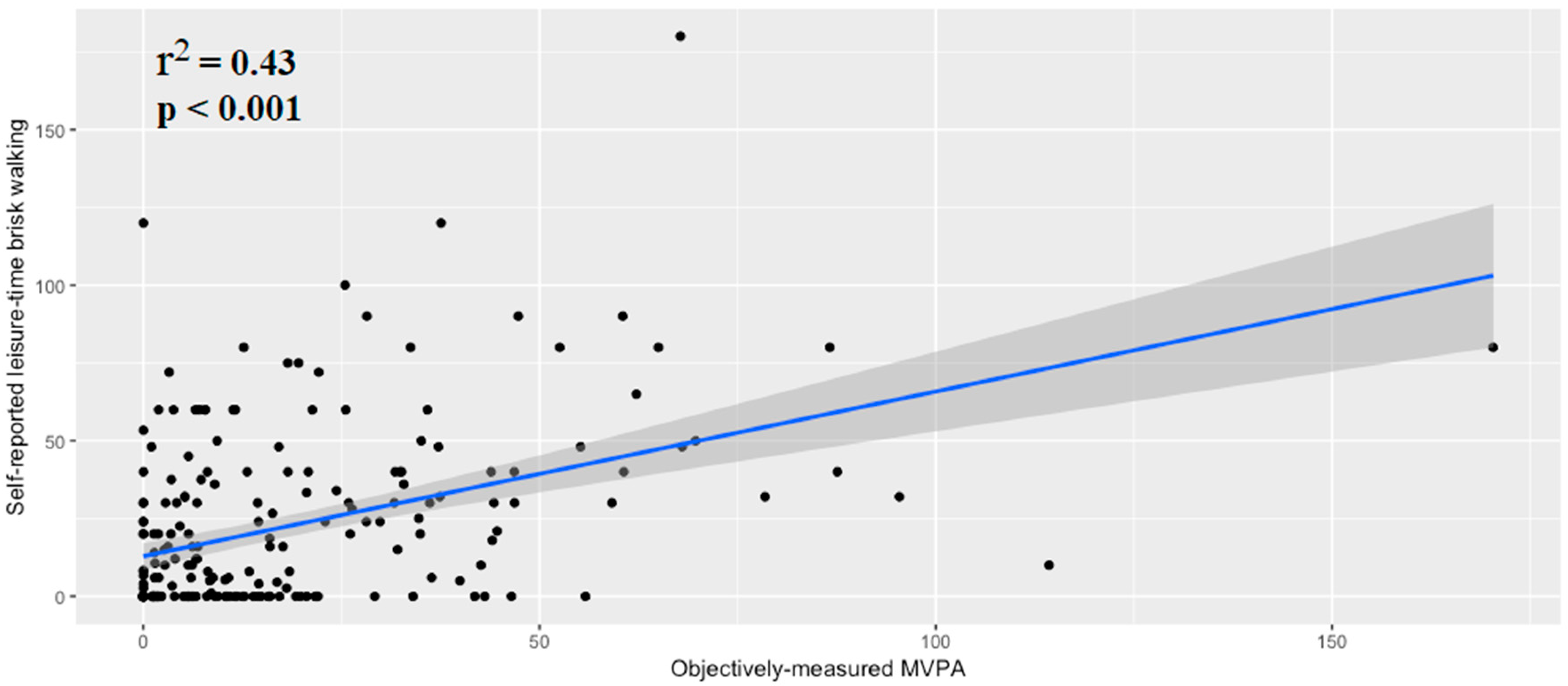
2.3. Outcome Measure: Physical Activity
2.4. Covariate Assessment
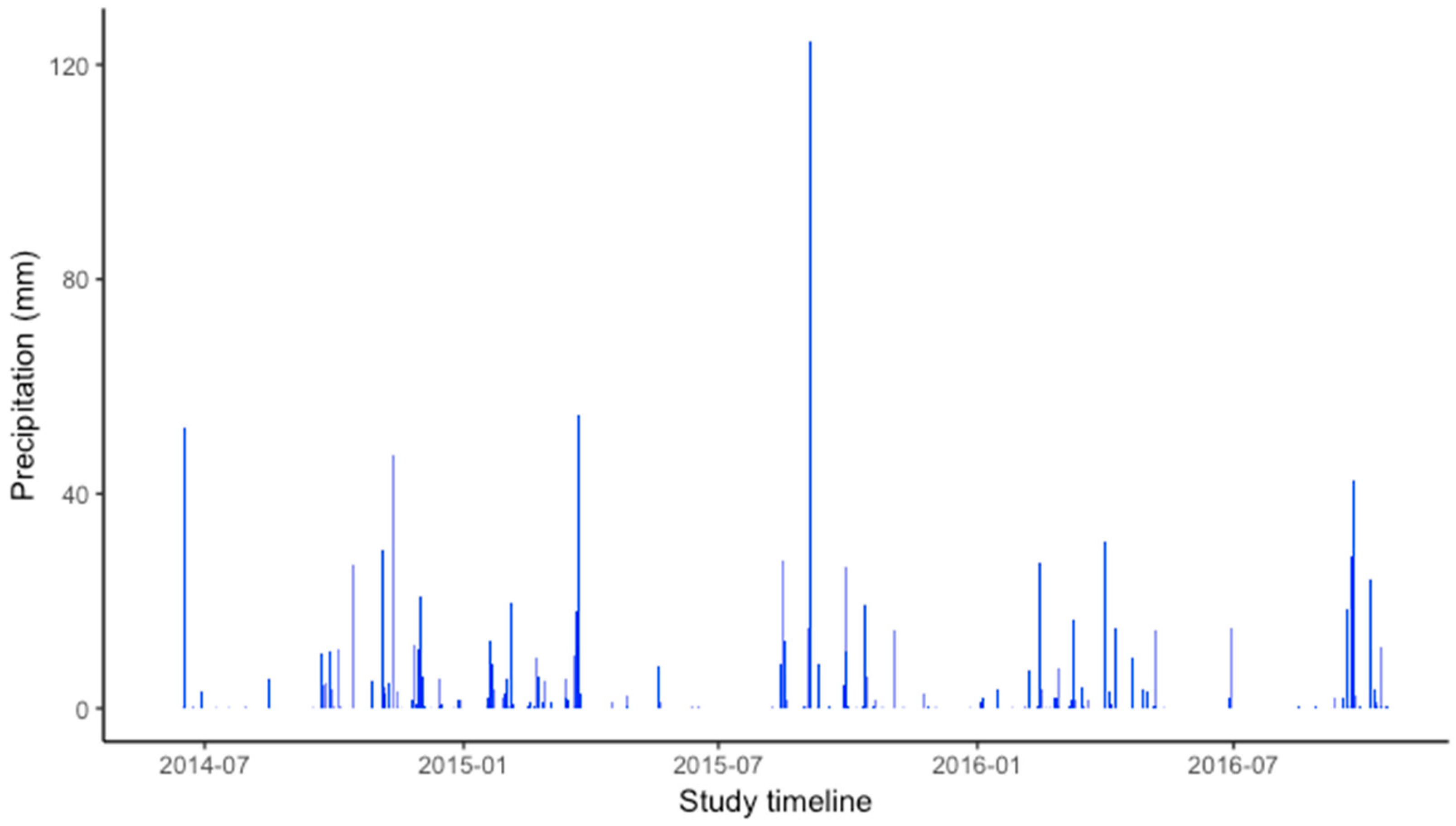
2.5. Weather Assessment
2.6. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Associations of POS with Self-Reported Leisure-Time Brisk Walking and OM-MVPA
4. Discussion
4.1. Main Findings
4.2. Built Environment, Weather, and Physical Activity in Older Adults
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet. Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; van Mechelen, W.; Pratt, M.; Lancet Physical Activity Series 2 Executive Committee. The economic burden of physical inactivity: A global analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef]
- Sallis, J.F.; Bull, F.; Guthold, R.; Heath, G.W.; Inoue, S.; Kelly, P.; Oyeyemi, A.L.; Perez, L.G.; Richards, J.; Hallal, P.C.; et al. Progress in physical activity over the Olympic quadrennium. Lancet 2016, 388, 1325–1336. [Google Scholar] [CrossRef]
- United Nations. Department of Economic and Social Affairs, Population Division. In World Population Ageing 2017; The United Nations: New York, NY, USA, 2017. [Google Scholar]
- Marengoni, A.; Angleman, S.; Melis, R.; Mangialasche, F.; Karp, A.; Garmen, A.; Meinow, B.; Fratiglioni, L. Aging with multimorbidity: A systematic review of the literature. Ageing Res. Rev. 2011, 10, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Garin, N.; Olaya, B.; Perales, J.; Moneta, M.V.; Miret, M.; Ayuso-Mateos, J.L.; Haro, J.M. Multimorbidity patterns in a national representative sample of the Spanish adult population. PLoS ONE 2014, 9, e84794. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015; p. 246. [Google Scholar]
- Van Cauwenberg, J.; Nathan, A.; Barnett, A.; Barnett, D.W.; Cerin, E.; Environment, T.C.O.; Council on Environment and Physical Activity (CEPA)-Older Adults Working Group. Relationships Between Neighbourhood Physical Environmental Attributes and Older Adults’ Leisure-Time Physical Activity: A Systematic Review and Meta-Analysis. Sports Med. 2018, 380, 1–26. [Google Scholar] [CrossRef]
- Barnett, D.W.; Barnett, A.; Nathan, A.; Van Cauwenberg, J.; Cerin, E.; Council on Environment and Physical Activity (CEPA)—Older Adults working group. Built environmental correlates of older adults’ total physical activity and walking: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 103. [Google Scholar] [CrossRef]
- Wu, Y.-T.; Luben, R.; Wareham, N.; Griffin, S.; Jones, A.P. Weather, day length and physical activity in older adults: Cross-sectional results from the European Prospective Investigation into Cancer and Nutrition (EPIC) Norfolk Cohort. PLoS ONE 2017, 12, e0177767. [Google Scholar] [CrossRef]
- Klenk, J.; Büchele, G.; Rapp, K.; Franke, S.; Peter, R.; ActiFE Study Group. Walking on sunshine: Effect of weather conditions on physical activity in older people. J. Epidemiol. Community Health 2012, 66, 474–476. [Google Scholar] [CrossRef]
- Witham, M.D.; Donnan, P.T.; Vadiveloo, T.; Sniehotta, F.F.; Crombie, I.K.; Feng, Z.; McMurdo, M.E.T. Association of Day Length and Weather Conditions with Physical Activity Levels in Older Community Dwelling People. PLoS ONE 2014, 9, e85331. [Google Scholar] [CrossRef] [PubMed]
- Loyen, A.; Van Hecke, L.; Verloigne, M.; Hendriksen, I.; Lakerveld, J.; Steene-Johannessen, J.; Vuillemin, A.; Koster, A.; Donnelly, A.; Ekelund, U.; et al. DEDIPAC consortium Variation in population levels of physical activity in European adults according to cross-European studies: A systematic literature review within DEDIPAC. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 72. [Google Scholar] [CrossRef] [PubMed]
- Colom, A.; Fiol, M.; Ruiz, M.; Compa, M.; Morey, M.; Moñino, M.; Romaguera, D. Association between Access to Public Open Spaces and Physical Activity in a Mediterranean Population at High Cardiovascular Risk. Int. J. Environ. Res. Public Health 2018, 15, 1285. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Buil-Cosiales, P.; Corella, D.; Bulló, M.; Fitó, M.; Vioque, J.; Romaguera, D.; Martinez, J.A.; Wärnberg, J.; Lopez-Miranda, J.; et al. PREDIMED-PLUS investigators Cohort Profile: Design and methods of the PREDIMED-Plus randomized trial. Int. J. Epidemiol. 2018, 41, 377. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed]
- Forsyth, A.; Van Riper, D.; Larson, N.; Wall, M.; Neumark-Sztainer, D. Creating a replicable, valid cross-platform buffering technique: The sausage network buffer for measuring food and physical activity built environments. Int. J. Health Geogr. 2012, 11, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forsyth, A.; Larson, N.; Lytle, L.; Mishra, N.; Neumark-Sztainer, D.; Noble, P.; Van Riper, D. LEAN-GIS protocols Local Environment for Activity and Nutrition-Geographic Information Systems. Available online: http://designforhealth.net/wp-content/uploads/2012/12/LEAN_Protocol_V2_1_010112rev.pdf (accessed on 23 April 2018).
- Frank, L.D.; Fox, E.H.; Ulmer, J.M.; Chapman, J.E.; Kershaw, S.E.; Sallis, J.F.; Conway, T.L.; Cerin, E.; Cain, K.L.; Adams, M.A.; et al. International comparison of observation-specific spatial buffers: Maximizing the ability to estimate physical activity. Int. J. Health Geogr. 2017, 16, 4. [Google Scholar] [CrossRef] [PubMed]
- Apparicio, P.; Seguin, A.-M. Measuring the Accessibility of Services and Facilities for Residents of Public Housing in Montreal. Urban Stud. 2006, 43, 187–211. [Google Scholar] [CrossRef]
- White, M.P.; Wheeler, B.W.; Herbert, S.; Alcock, I.; Depledge, M.H. Coastal proximity and physical activity: Is the coast an under-appreciated public health resource? Prev. Med. 2014, 69, 135–140. [Google Scholar] [CrossRef] [Green Version]
- Winters, M.; Buehler, R.; Götschi, T. Policies to Promote Active Travel: Evidence from Reviews of the Literature. Curr. Environ. Health Rep. 2017, 4, 278–285. [Google Scholar] [CrossRef]
- Molina, L.; Sarmiento, M.; Peñafiel, J.; Donaire, D.; Garcia-Aymerich, J.; Gomez, M.; Ble, M.; Ruiz, S.; Frances, A.; Schröder, H.; et al. Validation of the Regicor Short Physical Activity Questionnaire for the Adult Population. PLoS ONE 2017, 12, e0168148. [Google Scholar] [CrossRef] [PubMed]
- Elosua, R.; Marrugat, J.; Molina, L.; Pons, S.; Pujol, E. Validation of the Minnesota Leisure Time Physical Activity Questionnaire in Spanish men. The MARATHOM Investigators. Am. J. Epidemiol. 1994, 139, 1197–1209. [Google Scholar] [CrossRef] [PubMed]
- Elosua, R.; Garcia, M.; Aguilar, A.; Molina, L.; Covas, M.I.; Marrugat, J. Validation of the Minnesota Leisure Time Physical Activity Questionnaire in Spanish Women. Investigators of the MARATDON Group. Med. Sci. Sports Exerc. 2000, 32, 1431–1437. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010; Volume 60. [Google Scholar]
- Hart, T.L.; Swartz, A.M.; Cashin, S.E.; Strath, S.J. How many days of monitoring predict physical activity and sedentary behaviour in older adults? Int. J. Behav. Nutr. Phys. Act. 2011, 8, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freedson, P.S.; Miller, K. Objective monitoring of physical activity using motion sensors and heart rate. Res. Q. Exerc. Sport 2000, 71, S21–S29. [Google Scholar] [CrossRef] [PubMed]
- Hildebrand, M.; van Hees, V.T.; Hansen, B.H.; Ekelund, U. Age group comparability of raw accelerometer output from wrist- and hip-worn monitors. Med. Sci. Sports Exerc. 2014, 46, 1816–1824. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Tasigchana, R.F.; León-Muñoz, L.M.; López-García, E.; Banegas, J.R.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Mediterranean Diet and Health-Related Quality of Life in Two Cohorts of Community-Dwelling Older Adults. PLoS ONE 2016, 11, e0151596. [Google Scholar]
- Cerin, E.; Cain, K.L.; Conway, T.L.; Van Dyck, D.; Hinckson, E.; Schipperijn, J.; De Bourdeaudhuij, I.; Owen, N.; Davey, R.C.; Hino, A.A.F.; et al. Neighborhood environments and objectively measured physical activity in 11 countries. Med. Sci. Sports Exerc. 2014, 46, 2253–2264. [Google Scholar] [CrossRef]
- Wood, S.N. Generalized Additive Models: An Introduction with R, 2nd ed.; Chapman and Hall/CRC: London, UK, 2006. [Google Scholar]
- Burnham, K.P.; Anderson, D.R. Model Selection and Multimodel Inference: A Practical Information-Theoretic Approach; Springer Science & Business Media: Berlin, Germany, 2003. [Google Scholar]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Wood, S.; Scheipl, F. Gamm4: Generalized Additive Mixed Models Using Mgcv and Lme4. R Package Version 0.2-3. 2014. Available online: https://cran.r-project.org/web/packages/gamm4/index.html (accessed on 25 September 2018).
- Barnett, I.; van Sluijs, E.M.F.; Ogilvie, D. Physical activity and transitioning to retirement: A systematic review. Am. J. Prev. Med. 2012, 43, 329–336. [Google Scholar] [CrossRef]
- Barnett, I.; van Sluijs, E.; Ogilvie, D.; Wareham, N.J. Changes in household, transport and recreational physical activity and television viewing time across the transition to retirement: Longitudinal evidence from the EPIC-Norfolk cohort. J. Epidemiol. Community Health 2014, 68, 747–753. [Google Scholar] [CrossRef]
- Lim, K.; Taylor, L. Factors associated with physical activity among older people—A population-based study. Prev. Med. 2005, 40, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Harris, T.J.; Owen, C.G.; Victor, C.R.; Adams, R.; Cook, D.G. What factors are associated with physical activity in older people, assessed objectively by accelerometry? Br. J. Sports Med. 2009, 43, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.B.; Ryan, D.A. Assessing the effects of weather conditions on physical activity participation using objective measures. Int. J. Environ. Res. Public Health 2009, 6, 2639–2654. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef] [PubMed]
- Franco, M.; Bilal, U.; Diez-Roux, A.V. Preventing non-communicable diseases through structural changes in urban environments. J. Epidemiol. Community Health 2015, 69, 509–511. [Google Scholar] [CrossRef] [PubMed]
- Chippendale, T.; Boltz, M. The Neighborhood Environment: Perceived Fall Risk, Resources, and Strategies for Fall Prevention. Gerontologist 2015, 55, 575–583. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Individual/Demographic | Time Physical Activity (min/day) | ||||
|---|---|---|---|---|---|
| n (%) | Self-Reported Leisure-Time Brisk Walking | p | Objectively-Measured MVPA 10-min Bouts | p | |
| All | 218 (100) | 22.0 (28.4) | 17.3 (23.0) | ||
| Sex | 0.599 | <0.001 | |||
| Men | 106 (48.6) | 23.0 (26.9) | 23.0 (28.1) | ||
| Women | 112 (51.4) | 21.0 (29.8) | 11.8 (15.1) | ||
| Age (years) | 0.879 | 0.123 | |||
| >65 | 102 (46.8) | 22.3 (31.0) | 14.7 (18.8) | ||
| ≤65 | 116 (53.2) | 21.7 (25.9) | 19.5 (26.1) | ||
| Educational level | 0.238 | 0.118 | |||
| Primary school or less | 132 (60.6) | 20.2 (29.9) | 15.3 (19.1) | ||
| Secondary school or higher | 86 (39.4) | 24.8 (25.7) | 20.3 (27.9) | ||
| Self-rated health | 0.010 | <0.001 | |||
| Excellent/very good/good | 145 (67.1) | 24.6 (27.9) | 20.2 (25.8) | ||
| Fair/poor | 71 (32.9) | 14.8 (21.7) | 10.5 (13.1) | ||
| Precipitation (mm) | 0.731 | 0.237 | |||
| Non-rainy period | 119 | 21.4 (28.5) | 18.9 (26.4) | ||
| Rainy period | 99 | 22.7 (28.3) | 15.2 (18.2) | ||
| Objectively-Assessed POS | Mean (SD) | n Zeros (%) |
|---|---|---|
| Distance to coast (km) | 2.98 (1.71) | 0 (0.00) |
| Distance to walk-friendly route (km) | 0.45 (0.58) | 0 (0.00) |
| Distance to nearest sports facility (km) | 0.85 (0.66) | 0 (0.00) |
| Distance to nearest beach (km) | 3.89 (1.55) | 0 (0.00) |
| Distance to nearest park (km) | 0.28 (0.4) | 0 (0.00) |
| Coastline contained or intersected by buffer (km) | 0.04 (0.12) | 193 (88.53) |
| Walk-friendly routes contained or intersected by buffer (km) | 4.24 (3.15) | 22 (10.09) |
| No. sports facilities contained or intersected by buffer | 1.49 (1.34) | 66 (30.28) |
| Area of sports facilities contained or intersected by buffer (km2) | 0.02 (0.03) | 66 (30.28) |
| No. parks contained or intersected by buffer | 8.5 (5.09) | 9 (4.13) |
| Areas of parks contained or intersected by buffer (km2) | 0.16 (0.25) | 9 (4.13) |
| No. beaches contained or intersected by buffer | 0.04 (0.19) | 210 (96.33) |
| Areas of beaches contained or intersected by buffer (km2) | 0 (0) | 210 (96.33) |
| No. POS contained or intersected by buffer | 10.03 (5.91) | 9 (4.13) |
| Areas of POS contained or intersected by buffer (km2) | 0.17 (0.25) | 9 (4.13) |
| Predictor Variable | a Self-Reported Leisure-Time Brisk Walking (Minutes/Day) (n = 216) | b Engaging in ≥ 150 min/week Self-Reported Leisure-Time Brisk Walking (Yes = 83 (38.4%); No = 133 (61.6%)) | ||||
|---|---|---|---|---|---|---|
| β | 95% CI | p | OR | 95% CI | p | |
| Distance to the coast (km) | 2.063 | −0.005–4.131 | 0.052 | 1.095 | 0.924–1.298 | 0.294 |
| Healthy routes contained or intersected by buffer (km) | 2.374 | −3.762–8.51 | 0.449 | 0.917 | 0.558–1.504 | 0.73 |
| Distance to nearest sports facility (km) | −2.541 | −7.836–2.754 | 0.348 | 0.96 | 0.625–1.473 | 0.85 |
| Distance to nearest beach (km) | 0.518 | −1.742–2.778 | 0.654 | 0.959 | 0.798–1.152 | 0.651 |
| Distance to nearest park (km) | 3.134 | −5.662–11.929 | 0.486 | 1.124 | 0.557–2.267 | 0.744 |
| Walk-friendly routes contained or intersected by buffer (km) | −0.133 | −1.246–0.98 | 0.815 | 1.015 | 0.928–1.11 | 0.751 |
| No. sports facilities contained or intersected by buffer | 0.339 | −2.266–2.944 | 0.799 | 0.956 | 0.774–1.18 | 0.676 |
| No. parks contained or intersected by buffer | −0.215 | −0.905–0.475 | 0.542 | 0.995 | 0.941–1.052 | 0.867 |
| Areas of parks contained or intersected by buffer (km2) | −12.685 | −26.678–1.309 | 0.077 | 0.54 | 0.163–1.793 | 0.315 |
| No. POS contained or intersected by buffer | −0.123 | −0.716–0.469 | 0.684 | 0.995 | 0.949–1.044 | 0.851 |
| Areas of POS contained or intersected by buffer (km2) | −11.579 | −25.545–2.388 | 0.106 | 0.58 | 0.178–1.891 | 0.368 |
| Predictor Variable | a Objectively-Measured MVPA 10 Min Bouts (Minutes/Day) (n = 216) | b Engaging in ≥ 150 min/wk Objectively-Measured MVPA 10 Min Bouts(Yes = 60 (27.8%) No = 156 (72.2%)) | ||||
|---|---|---|---|---|---|---|
| β | 95% CI | p | OR | 95% CI | p | |
| Distance to coast (km) | 0.106 | −1.9–2.113 | 0.917 | 1.055 | 0.876–1.273 | 0.571 |
| Distance to walk-friendly route (km) | 1.088 | 0.647–1.828 | 0.752 | 1.088 | 0.647–1.828 | 0.752 |
| Distance to nearest sports facility (km) | −1.137 | −6.173–3.898 | 0.658 | 1.037 | 0.651–1.649 | 0.881 |
| Distance to nearest beach (km) | −1.099 | −3.234–1.035 | 0.314 | 0.938 | 0.764–1.152 | 0.542 |
| Distance to nearest park (km) | −3.56 | −12.956–5.835 | 0.459 | 0.875 | 0.404–1.894 | 0.735 |
| Walk-friendly routes contained or intersected by buffer (km) | 0.981 | −0.004–1.966 | 0.052 | 1.031 | 0.933–1.139 | 0.548 |
| No. sports facilities contained or intersected by buffer | 0.994 | −1.275–3.264 | 0.391 | 1.055 | 0.839–1.327 | 0.645 |
| No. parks contained or intersected by buffer | 0.485 | −0.132–1.102 | 0.125 | 1.016 | 0.955–1.082 | 0.609 |
| Areas of parks contained or intersected by buffer (km2) | −3.86 | −15.756–8.036 | 0.525 | 0.695 | 0.189–2.558 | 0.585 |
| No. POS contained or intersected by buffer | 0.398 | −0.132–0.928 | 0.143 | 1.014 | 0.962–1.069 | 0.599 |
| Areas of POS contained or intersected by buffer (km2) | −3.751 | −15.597–8.095 | 0.536 | 0.724 | 0.199–2.632 | 0.624 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colom, A.; Ruiz, M.; Wärnberg, J.; Compa, M.; Muncunill, J.; Barón-López, F.J.; Benavente-Marín, J.C.; Cabeza, E.; Morey, M.; Fitó, M.; et al. Mediterranean Built Environment and Precipitation as Modulator Factors on Physical Activity in Obese Mid-Age and Old-Age Adults with Metabolic Syndrome: Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 854. https://doi.org/10.3390/ijerph16050854
Colom A, Ruiz M, Wärnberg J, Compa M, Muncunill J, Barón-López FJ, Benavente-Marín JC, Cabeza E, Morey M, Fitó M, et al. Mediterranean Built Environment and Precipitation as Modulator Factors on Physical Activity in Obese Mid-Age and Old-Age Adults with Metabolic Syndrome: Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2019; 16(5):854. https://doi.org/10.3390/ijerph16050854
Chicago/Turabian StyleColom, Antoni, Maurici Ruiz, Julia Wärnberg, Montserrat Compa, Josep Muncunill, Francisco Javier Barón-López, Juan Carlos Benavente-Marín, Elena Cabeza, Marga Morey, Montserrat Fitó, and et al. 2019. "Mediterranean Built Environment and Precipitation as Modulator Factors on Physical Activity in Obese Mid-Age and Old-Age Adults with Metabolic Syndrome: Cross-Sectional Study" International Journal of Environmental Research and Public Health 16, no. 5: 854. https://doi.org/10.3390/ijerph16050854