Parent-Teen Communication about Sexual and Reproductive Health: Cohort Differences by Race/Ethnicity and Nativity

Abstract
:1. Introduction
2. Materials and Methods
2.1. Measures
2.2. Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- National Center for Health Statistics. Health, United States, 2016: With Chartbook on Long-Term Trends in Health; National Center for Health Statistics: Hyattsville, MD, USA, 2017.
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.K.; Driscoll, A.K.; Drake, P. Births: Final Data for 2016; National Center for Health Statistics: Hyattsville, MD, USA, 2018.
- Child Trends Databank. Sexually Transmitted Infections (STIs); Child Trends Databank: Bethesda, MD, USA, 2018. [Google Scholar]
- Centers for Disease Control and Prevention. STDs in Adolescents and Young Adults. Available online: https://www.cdc.gov/std/stats16/adolescents.htm (accessed on 17 December 2018).
- Breuner, C. Talking about Sex: AAP Recommends Evidence-Based Education, with Pediatricans’ Help. Available online: http://www.aappublications.org/news/2016/07/18/SexEd071816 (accessed on 8 January 2019).
- The Society for Adolescent Health and Medicine. Abstinence-Only-Until-Marriage Policies and Programs: An Updated Position Paper of the Society for Adolescent Health and Medicine. J. Adolesc. Health 2017, 61, 400–403. [Google Scholar]
- American Public Health Association. Sexuality Education as Part of a Comprehensive Health Education Program in K to 12 Schools; American Public Health Association: Washington, DC, USA, 2014. [Google Scholar]
- Widman, L.; Choukas-Bradley, S.; Noar, S.M.; Nesi, J.; Garrett, K. Parent-adolescent sexual communication and adolescent safer sex behavior: A meta-analysis. JAMA Pediatr. 2016, 170, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Commendador, K.A. Parental influences on adolescent decision making and contraceptive use. Pediatr. Nurs. 2010, 36, 147–156, 170. [Google Scholar] [PubMed]
- Hicks, M.S.; McRee, A.-L.; Eisenberg, M.E. Teens talking with their partners about sex: The role of parent communication. Am. J. Sex. Educ. 2013, 8, 1–17. [Google Scholar] [CrossRef]
- Miller, K.S.; Levin, M.L.; Whitaker, D.J.; Xu, X. Patterns of condom use among adolescents: The impact of mother-adolescent communication. Am. J. Public Health 1998, 88, 1542–1544. [Google Scholar] [CrossRef] [PubMed]
- Weiss, D.M. Parental Communication: Determinants of Sexual Activity in Later Life. Ph.D. Thesis, Purdue University, West Lafayette, IN, USA, 2011. [Google Scholar]
- Wikkeling-Scott, L.F. An Examination of the Influence of Mother-Child Communication and Maternal Monitoring on Sexual Behavior in African American High School Students. Dr.P.H. Thesis, Morgan State University, Baltimore, MD, USA, 2011. [Google Scholar]
- Guilamo-Ramos, V.; Bouris, A.; Lee, J.; McCarthy, K.; Michael, S.L.; Pitt-Barnes, S.; Dittus, P. Paternal influences on adolescent sexual risk behaviors: A structured literature review. Pediatrics 2012, 130, e1313–e1325. [Google Scholar] [CrossRef] [PubMed]
- Franzini, L.; Ribble, J.; Keddie, A. Understanding the Hispanic paradox. Ethnicity Dis. 2001, 11, 496–518. [Google Scholar]
- Albert, B. With One Voice 2012: America’s Adults and Teens Sound Off about Teen Pregnancy; The National Campaign to Prevent Teen and Unplanned Pregnancy: Washington, DC, USA, 2012. [Google Scholar]
- Meneses, L.M.; Orrell-Valente, J.K.; Guendelman, S.R.; Oman, D.; Irwin, C.E. Racial/ethnic differences in mother-daughter communication about sex. J. Adolesc. Health 2006, 39, 128–131. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, M.K. The influence of sexual risk communication between parents and daughters on sexual risk behaviors. Fam. Relat. 2002, 51, 238–247. [Google Scholar] [CrossRef]
- Somers, C.L.; Vollmar, W.L. Parent-adolescent relationships and adolescent sexuality: Closeness, communication, and comfort among diverse U.S. adolescent samples. Soc. Behav. Personal. 2006, 34, 451–460. [Google Scholar] [CrossRef]
- Healthy People 2020. Family Planning. Available online: http://www.healthypeople.gov/2020/topics-objectives/topic/family-planning (accessed on 28 September 2016).
- Office of Adolescent Health. Replicating Evidence-Based Teen Pregnancy Prevention Programs to Scale in Communities with the Greatest Need (Tier 1B); Office of Adolescent Health: Rockville, MD, USA, 2015.
- Office of Adolescent Health. FY18 Announcement of the Availability of Funds for Phase I New and Innovative Strategies (Tier 2) to Prevent Teenage Pregnancy and Promote Healthy Abstinence; Office of Adolescent Health: Rockville, MD, USA, 2018.
- Office of Adolescent Health. FY18 Announcement of Availability of Funds for Phase I Replicating Programs (Tier 1) Effective in the Promotion of Healthy Adolescence and the Reduction of Teenage Pregnancy and Associated Risk Behaviors; Office of Adolescent Health: Rockville, MD, USA, 2018.
- Zief, S.; Shapiro, R.; Strong, D. The Personal Responsibility Education Program (PREP): Launching a Nationwide Adolescent Pregnancy Prevention Effort; Office of Planning Research and Evaluation, Administration for Children and Families, U.S. Department of Health and Human Services: Washington, DC, USA, 2013.
- Office of Adolescent Health. About the Teen Pregnancy Prevention (TPP) Program; Office of Adolescent Health: Rockville, MD, USA, 2017.
- Centers for Disease Control and Prevention. Teen Pregnancy Prevention Evidence Review: Families Talking Together; U.S. Department of Health and Human Services: Washington, DC, USA, 2017.
- DeVore, E.R.; Ginsburg, K.R. The protective effects of good parenting on adolescents. Curr. Opin. Pediatr. 2005, 17, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Isasi, C.; Rastogi, D.; Molina, K. Health issues in Hispanic/Latino youth. J. Latinx Psychol. 2016, 4, 67–82. [Google Scholar] [CrossRef] [PubMed]
- Granados, G.; Puvvula, J.; Berman, N.; Dowling, P. Health care for Latino children: Impact of child and parental birthplace on insurance status and access to health services. Am. J. Public Health 2001, 91, 1806–1807. [Google Scholar] [CrossRef] [PubMed]
- Bray, I.; Gunnell, D.; Smith, G.D. Advanced paternal age: How old is too old? J. Epidemiol. Community Health 2006, 60, 851–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wight, D.; Fullerton, D. A review of interventions with parents to promote the sexual health of their children. J. Adolesc. Health 2013, 52, 4–27. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, L.D.; Maddow-Zimet, I.; Boonstra, H. Changes in adolescents’ receipt of sex education, 2006–2013. J. Adolesc. Health 2016, 58, 621–627. [Google Scholar] [CrossRef] [PubMed]
- National Center for Health Statistics. National Survey on Family Growth Public Use Data and Documentation; CDC National Center for Health Statistics: Hyattsville, MD, USA, 2017.
- Breuner, C.; Mattson, G. Sexuality education for children and adolescents. Pediatrics 2016, 138. [Google Scholar] [CrossRef] [PubMed]
- Luquis, R.R.; Brelsford, G.M.; Rojas-Guyler, L. Religiosity, spirituality, sexual attitudes, and sexual behaviors among college students. J. Relig. Health 2012, 51, 601–614. [Google Scholar] [CrossRef] [PubMed]
- Simington, J. Rethinking sex ed: Meet youth where they are. In Urban Wire: Adolescents and Youth; Urban Institute: Washington, DC, USA, 2016. [Google Scholar]
- Akers, A.; Holland, C.; Bost, J. Interventions to improve parental communication about sex: A systematic review. Pediatrics 2011, 127, 494–510. [Google Scholar] [CrossRef] [PubMed]
- Robert, A.; Sonenstein, F. Adolescents’ reports of communication with their parents about sexually transmitted diseases and birth control: 1988, 1995, and 2002. J. Adolesc. Health 2010, 46, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, L.; Ku, L.; Sonenstein, F. Adolescent’s reports of reproductive health education, 1988 and 1995. Fam. Plan. Perspect. 2000, 32, 220–226. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Teen Pregnancy in the United States. Available online: https://www.cdc.gov/teenpregnancy/about/index.htm (accessed on 17 December 2018).
- Gonzalez-Barrera, A. Chapter 1: Migration Flows Between the U.S. and Mexico Have Slowed and Turned Toward Mexico; Pew Research Center: Washington, DC, USA, 2015. [Google Scholar]
- Mark Mather. What’s Driving the Decline in U.S. Population Growth? Population Reference Bureau: Washington, DC, USA, 2013.
- Wilson, E.K. Differences in contraceptive use accross generations of migration among women of Mexican origin. Mater. Child Health J. 2009, 13, 641–651. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control. STDs in Racial and Ethnic Minorities. Available online: https://www.cdc.gov/std/stats15/minorities.htm (accessed on 6 November 2017).
- Guzman, L.; Golub, E.; Caal, S.; Hickman, S.; Ramos, M. Let’s (Not) Talk about Sex: Communication and Teen Pregnancy Prevention within Hispanic Families; Child Trends: Bethesda, MD, USA, 2013. [Google Scholar]
- Manlove, J.; Logan, C.; Moore, K.; Ikramullah, E. Pathways from family religiosity to adolescent sexual activity and contraceptive use. Perspect. Sex. Reprod. Health 2008, 40, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Vasilenko, S.A.; Duntzee, C.; Zheng, Y.; Lefkowitz, E.S. Testing two process models of religiosity and sexual behavior. J. Adolesc. 2013, 36, 667–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grossman, J.; Jenkins, L.; Richer, A. Parents’ perspectives on family sexuality communication from middle school to high school. Int. J. Environ. Res. Public Health 2018, 15, 107. [Google Scholar] [CrossRef] [PubMed]
- Office of Adolescent Health. Evidence-Based Programs. Available online: http://www.hhs.gov/ash/oah/oah-initiatives/teen_pregnancy/db/ (accessed on 17 December 2018).
- Pantin, H.; Guillermo, P.; Lopez, B.; Huang, S.; Tapia, M.I.; Schwartz, S.J.; Sabillon, E.; Brown, C.H.; Branchini, J. A randomized controlled trial of Familias Unidas for Hispanic adolescents with behavior problems. Psychosom. Med. 2009, 71, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Dilorio, C.; McCarty, F.; Resnicow, K.; Lehr, S.; Denzmore, P. REAL men: A group-randomized trial of an HIV prevention intervention for adolescent boys. Am. J. Public Health 2007, 97, 1084–1089. [Google Scholar] [CrossRef] [PubMed]
- Guilamo-Ramos, V.; Bouris, A.; Jaccard, J.; Gonzalez, B.; McCoy, W.; Aranda, D. A parent-based intervention to reduce sexual risk behavior in early adolescence: Building alliances between physicians, social workers and parents. J. Adolesc. Health 2011, 48, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Family & Youth Services Bureau. Competitive Personal Responsibility Education Program Fact Sheet. Available online: https://www.acf.hhs.gov/fysb/resource/competitive-prep-fact-sheet (accessed on 17 December 2018).
- Shtarksall, R.; Santelli, J.; Hirsch, J. Sex education and sexual socialization: Roles for educators and parents. Perspect. Sex. Reprod. Health 2007, 39, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Child Trends. Reducing Teen Childbearing among Latinos: An Innovative Anti-Poverty Strategy; Child Trends: Bethesda, MD, USA, 2013. [Google Scholar]
- Klein, J.D.; Sabaratnam, P.; Pazos, B.; Matos Auerbach, M.; Graff Havens, C.; Brach, M.J. Evaluation of the parents as primary sexuality educators program. J. Adolesc. Health 2005, 37, S94–S99. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Females in Cohort 1: 2006–2010 | Females in Cohort 2: 2011–2015 | Sig. Change across Cohorts | Males in Cohort 1: 2006–2010 | Males in Cohort 2: 2011–2015 | Sig. Change across Cohorts | |
|---|---|---|---|---|---|---|
| Percentage in Each Cohort | 52.9 | 47.1 | 52.7 | 47.3 | ||
| Race/ethnicity | ||||||
| White | 63.5 | 58.2 | 63.4 | 58.2 | ||
| Black | 16.5 | 16.2 | 16.1 | 16.1 | ||
| Hispanic | 20.0 | 25.6 | 20.5 | 25.8 | ||
| High religiosity | 39.0 | 39.8 | 32.1 | 29.2 | ||
| Disconnected (Neither working nor in school) | 10.1 | 7.4 | * | 9.1 | 7.2 | |
| Mother’s education | ||||||
| Less than high school | 15.9 | 15.7 | 13.3 | 16.2 | * | |
| High school graduate or GED | 31.1 | 28.1 | 34.1 | 27.6 | ||
| Some college or BA | 53.1 | 56.2 | 52.6 | 56.2 | ||
| Family structure at age 14 | ||||||
| Lived with two parents (biological or adopted) | 61.3 | 58.8 | 62.2 | 60.6 | ||
| Age | ||||||
| 15–17 | 55.1 | 58.0 | 60.5 | 60.9 | ||
| 18–19 | 44.9 | 42.0 | 39.5 | 39.1 | ||
| Ever had sex | 43.0 | 44.7 | 42.9 | 46.1 | ||
| Total Sample Size (N) | 2076 | 1834 | 2148 | 1871 |
| Talk to Parents about… | Any SRH Topic | How to Say No to Sex | Contraception | STIs | How to Use a Condom | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 2006–2010 | 2011–2015 | 2006–2010 | 2011–2015 | 2006–2010 | 2011–2015 | 2006–2010 | 2011–2015 | 2006–2010 | 2011–2015 | |||||
| Total | 79.0 | 78.5 | 62.4 | 62.4 | 55.8 | 56.4 | 58.0 | 60.0 | 30.4 | 36.8 | * | ||||
| Race/ethnicity | |||||||||||||||
| White | 79.9 | 78.2 | 62.9 | 63.6 | 58.4 | 60.9 | 56.0 | 56.7 | 29.0 | 33.7 | |||||
| Black | 82.0 | 79.6 | 67.8 | 63.2 | 56.2 | 51.0 | 68.7 | 68.3 | 44.4 | 43.9 | |||||
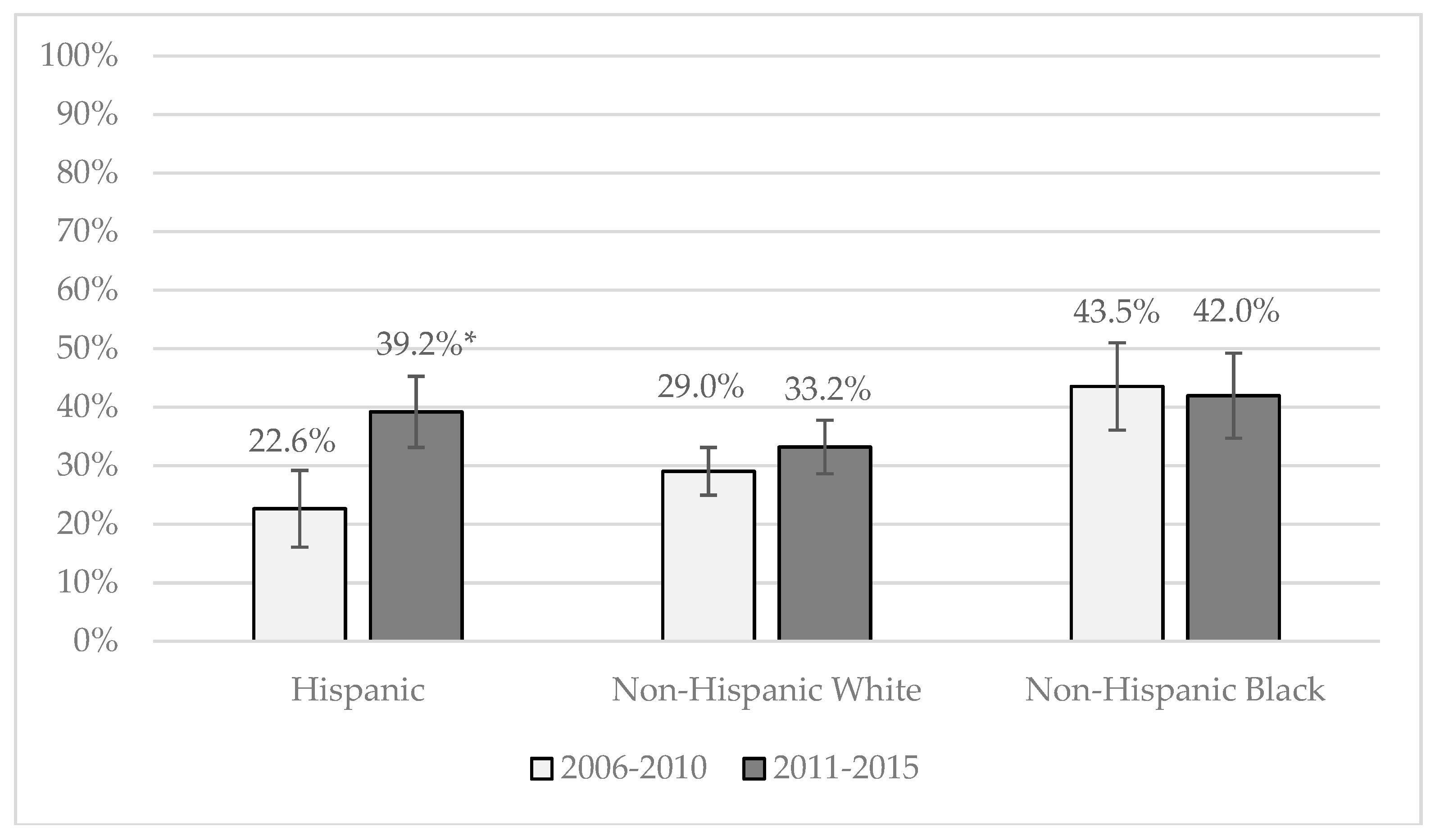
| Hispanic | 73.8 | 78.6 | 56.6 | 59.2 | 47.2 | 49.6 | 55.5 | 62.2 | 23.3 | 39.5 | * | ||||
| a | a | a | a | a | a | a | |||||||||
| Nativity of Hispanics | |||||||||||||||
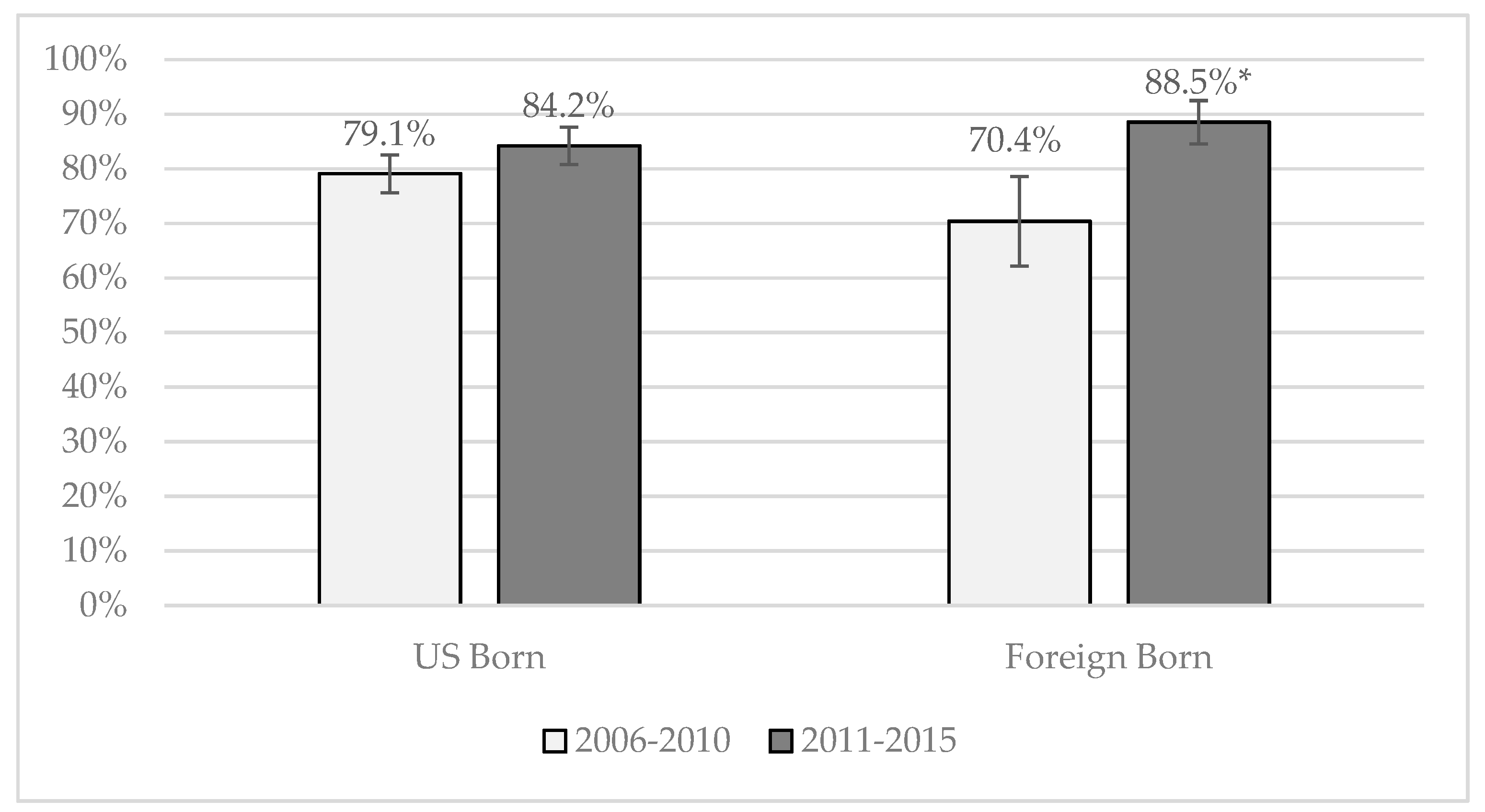
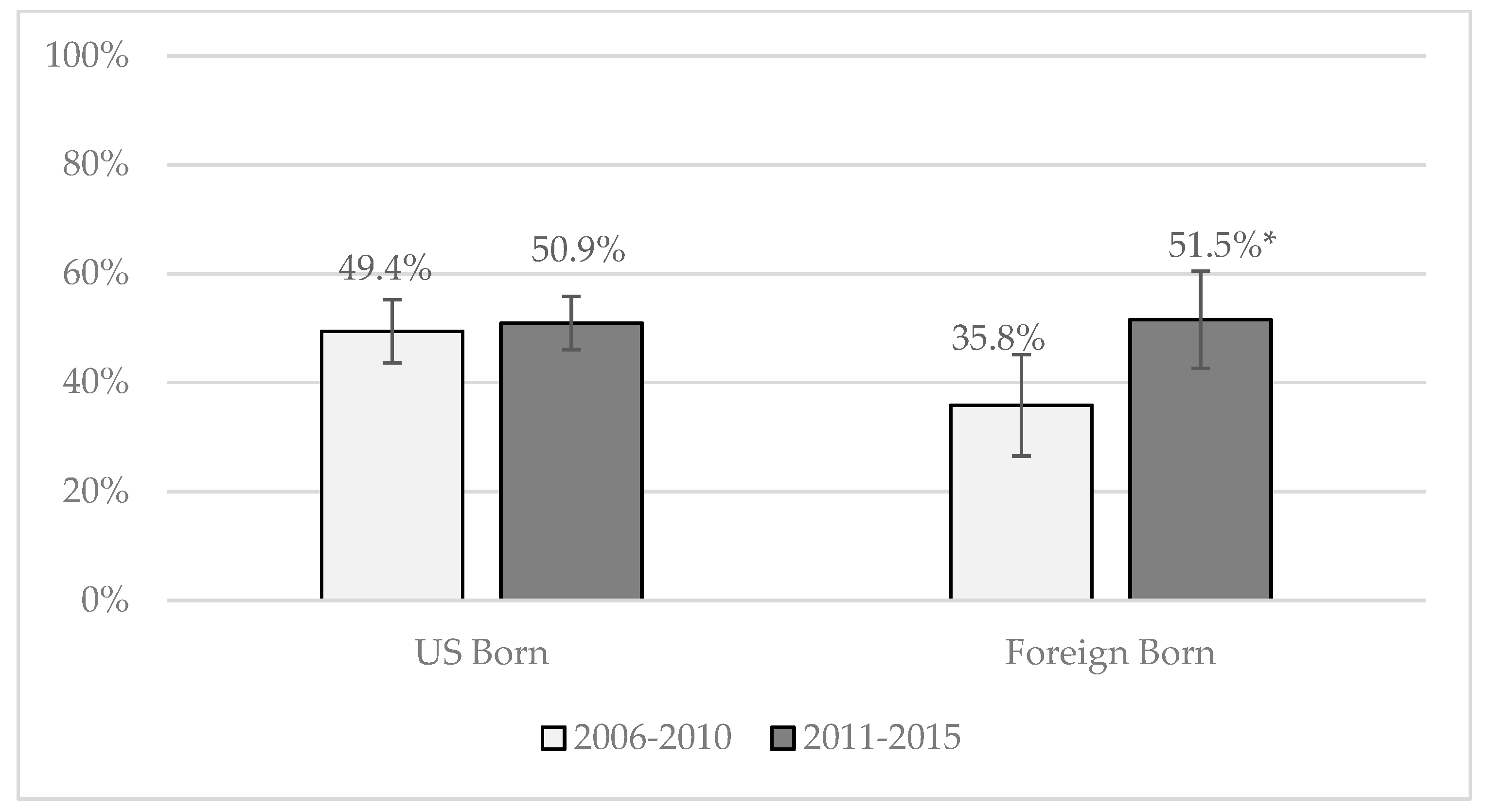
| U.S.-born | 76.4 | 78.8 | 59.0 | 59.4 | 49.3 | 50.6 | 58.3 | 62.4 | 24.5 | 39.1 | * | ||||
| Foreign-born | 63.7 | 77.5 | 47.3 | 58.1 | 38.8 | 44.6 | 44.1 | 61.0 | * | 18.7 | 41.1 | * | |||
| b | b | ||||||||||||||
| Male | 2006–2010 | 2011–2015 | 2006–2010 | 2011–2015 | 2006–2010 | 2011–2015 | 2006–2010 | 2011–2015 | 2006–2010 | 2011–2015 | |||||
| Total | 69.5 | 84.5 | * | 41.7 | 44.5 | 31.9 | 36.8 | * | 53.0 | 59.4 | * | 37.6 | 45.4 | * | |
| Race/ethnicity | |||||||||||||||
| White | 66.7 | 83.0 | * | 45.3 | 47.1 | 33.5 | 38.9 | 48.7 | 55.6 | * | 33.6 | 41.7 | * | ||
| Black | 78.2 | 86.5 | * | 43.3 | 46.5 | 28.0 | 34.6 | 65.7 | 66.4 | 50.5 | 58.7 | ||||
| Hispanic | 71.0 | 86.4 | * | 29.4 | 37.6 | * | 30.0 | 33.5 | 56.4 | 63.5 | * | 39.8 | 45.2 | ||
| a | a | a | a | a | a | a | |||||||||
| Nativity of Hispanics | |||||||||||||||
| U.S.-born | 74.2 | 85.1 | * | 33.8 | 37.8 | 31.0 | 32.1 | 58.2 | 63.8 | 40.8 | 44.7 | ||||
| Foreign-born | 62.1 | 90.4 | * | 17.1 | 36.9 | * | 27.0 | 37.7 | 51.0 | 62.5 | 37.1 | 46.8 | |||
| b | b | ||||||||||||||
| Talk to Parents about… | Any SRH Topic | How to Say No to Sex | Contraception | STIs | How to Use a Condom |
|---|---|---|---|---|---|
| VARIABLES | Adjusted Odds Ratio | Adjusted Odds Ratio | Adjusted Odds Ratio | Adjusted Odds Ratio | Adjusted Odds Ratio |
| 2011–2015 Cohort (ref: 2006–2010 cohort) | 0.9 | 1.0 | 1.0 | 1.0 | 1.3 * |
| (0.7–1.2) | (0.8–1.2) | (0.8–1.2) | (0.9–1.3) | (1.1–1.6) | |
| Race/ethnicity (ref: white) | |||||
| Hispanic | 1.0 | 0.9 | 0.7 *** | 1.2 | 1.0 |
| (0.8–1.2) | (0.7–1.1) | (0.5–0.8) | (0.9–1.4) | (0.8–1.3) | |
| Black | 1.1 | 1.1 | 0.8 * | 1.6 ** | 1.7 *** |
| (0.8–1.6) | (0.8–1.4) | (0.6–1.0) | (1.2–2.1) | (1.3–2.2) | |
| High religiosity (ref: religion is less important) | 1.2 | 1.4 ** | 0.8 * | 1.2 | 0.7 ** |
| (0.9–1.5) | (1.1–1.7) | (0.6–0.9) | (1.0–1.5) | (0.6–0.9) | |
| Disconnected (ref: in-school or working) | 0.5 *** | 0.6 ** | 0.7 * | 0.7 * | 1.1 |
| (0.4–0.7) | (0.5–0.9) | (0.5–1.0) | (0.5–1.0) | (0.7–1.5) | |
| Lived with two parents at age 14 (ref: none or 1) | 1.0 | 1.0 | 0.8 | 0.9 | 0.7 *** |
| (0.8–1.3) | (0.8–1.2) | (0.7–1.0) | (0.7–1.1) | (0.6–0.9) | |
| Mother’s education (ref: less than high school) | |||||
| High school graduate | 1.3 | 1.0 | 1.2 | 1.1 | 1.1 |
| (0.9–1.7) | (0.7–1.3) | (0.9–1.7) | (0.8–1.4) | (0.8–1.5) | |
| Some college or BA | 1.3 | 1.3 * | 1.2 | 1.1 | 1.0 |
| (1.0–1.7) | (1.0–1.6) | (0.9–1.5) | (0.9–1.5) | (0.8–1.4) | |
| Age | 0.8 | 0.9 | 1.0 | 0.8 * | 0.9 |
| (0.7–1.1) | (0.7–1.1) | (0.8–1.1) | (0.6–1.0) | (0.8–1.2) | |
| Ever had sex | 1.8 *** | 1.1 | 2.5 *** | 1.8 *** | 2.1 *** |
| (1.4–2.2) | (0.9–1.3) | (2.1–3.1) | (1.5–2.2) | (1.7–2.6) | |
| Constant | 2.6 *** | 1.4 * | 1.1 | 1.0 | 0.4 *** |
| (1.8–3.7) | (1.0–1.9) | (0.8–1.6) | (0.7–1.4) | (0.3–0.5) |
| Talk to Parents about… | Any SRH Topic | How to Say No to Sex | Contraception | STIs | How to Use a Condom |
|---|---|---|---|---|---|
| VARIABLES | Adjusted Odds Ratio | Adjusted odds ratio | Adjusted Odds Ratio | Adjusted Odds Ratio | Adjusted Odds Ratio |
| 2011–2015 Cohort (ref: 2006–2010 cohort) | 2.2 *** | 1.2 | 1.2 | 1.2 * | 1.3 ** |
| (1.7–2.9) | (1.0–1.4) | (1.0–1.5) | (1.0–1.5) | (1.1–1.6) | |
| Race/ethnicity (ref: white) | |||||
| Hispanic | 1.4 ** | 0.7 ** | 0.9 | 1.5 *** | 1.2 |
| (1.1–1.8) | (0.5–0.9) | (0.8–1.2) | (1.2–1.8) | (0.9–1.5) | |
| Black | 1.5 * | 0.9 | 0.7 | 1.6 *** | 1.7 *** |
| (1.1–2.0) | (0.7–1.1) | (0.6–1.0) | (1.3–2.0) | (1.3–2.2) | |
| High religiosity (ref: religion is less important) | 1.1 | 1.7 *** | 0.9 | 1.1 | 0.8 * |
| (0.9–1.4) | (1.4–2.1) | (0.7–1.1) | (0.9–1.3) | (0.6–1.0) | |
| Disconnected (ref: in-school or working) | 0.8 | 0.6 ** | 0.7 * | 1.0 | 1.1 |
| (0.6–1.1) | (0.4–0.8) | (0.5–0.9) | (0.7–1.3) | (0.8–1.6) | |
| Lived with two parents at age 14 (ref: none or 1) | 1.0 | 1.1 | 1.0 | 1.0 | 0.8 |
| (0.8–1.3) | (0.9–1.3) | (0.8–1.3) | (0.8–1.2) | (0.7–1.0) | |
| Mother’s education (ref: less than high school) | |||||
| High school graduate | 1.2 | 1.3 | 1.4 * | 1.1 | 1.1 |
| (0.8–1.6) | (1.0–1.7) | (1.0–1.9) | (0.9–1.5) | (0.8–1.5) | |
| Some college or BA | 1.6 ** | 1.8 *** | 1.8 *** | 1.4 * | 1.1 |
| (1.1–2.2) | (1.4–2.4) | (1.4–2.4) | (1.0–1.8) | (0.8–1.4) | |
| Age | 0.8 | 0.9 | 1.3 * | 0.8 * | 0.8 * |
| (0.7–1.0) | (0.8–1.1) | (1.0–1.6) | (0.7–1.0) | (0.6–1.0) | |
| Ever had sex | 2.0 *** | 1.0 | 2.1 *** | 2.3 *** | 3.2 *** |
| (1.6–2.4) | (0.9–1.3) | (1.7–2.6) | (1.9–2.7) | (2.6–3.9) |
| Talk to Parents about… | Any SRH Topic | How to Say No to Sex | Contraception | STIs | How to Use a Condom |
|---|---|---|---|---|---|
| VARIABLES | Adjusted Odds Ratio | Adjusted Odds Ratio | Adjusted Odds Ratio | Adjusted Odds Ratio | Adjusted Odds Ratio |
| 2011–2015 Cohort (ref: 2006–2010 cohort) | 1.7 *** | 1.2 | 1.1 | 1.3 * | 1.5 ** |
| (1.3–2.2) | (0.9–1.6) | (0.9–1.4) | (1.0–1.6) | (1.1–2.1) | |
| Foreign Born (ref: Native born) | 0.9 | 0.8 | 1.0 | 0.8 | 1.1 |
| (0.6–1.3) | (0.6–1.0) | (0.8–1.3) | (0.6–1.1) | (0.8–1.4) | |
| Female (ref: male) | 0.9 | 2.7 *** | 2.2 *** | 0.9 | 0.6 *** |
| (0.7–1.1) | (2.2–3.3) | (1.7–2.7) | (0.8–1.2) | (0.5–0.8) | |
| High religiosity (ref: religion is less important) | 1.2 | 1.5 ** | 1.0 | 1.3 * | 0.8 |
| (1.0–1.6) | (1.2–2.0) | (0.8–1.3) | (1.0–1.7) | (0.6–1.0) | |
| Disconnected (ref: in school or working) | 0.5 ** | 0.4 *** | 0.6 ** | 0.5 *** | 0.7 * |
| (0.3–0.7) | (0.3–0.7) | (0.4–0.9) | (0.3–0.7) | (0.5–1.0) | |
| Lived with two parents at age 14 (ref: none or 1) | 0.9 | 1.0 | 0.9 | 1.0 | 0.7 * |
| (0.7–1.3) | (0.8–1.3) | (0.7–1.2) | (0.7–1.4) | (0.6–0.9) | |
| Mother’s education (ref: less than high school) | |||||
| High school graduate | 1.7 ** | 1.7 *** | 1.6 ** | 1.2 | 1.7 *** |
| (1.1–2.4) | (1.2–2.2) | (1.1–2.3) | (0.9–1.8) | (1.3–2.2) | |
| Some college or BA | 2.0 *** | 1.9 *** | 1.9 *** | 1.4 * | 1.2 |
| (1.4–2.7) | (1.4–2.4) | (1.4–2.6) | (1.1–1.9) | (0.9–1.6) | |
| Age | 0.7 * | 0.9 | 1.0 | 0.8 | 1.0 |
| (0.6–1.0) | (0.7–1.2) | (0.8–1.4) | (0.6–1.1) | (0.7–1.2) | |
| Ever had Sex | 1.7 *** | 0.8 | 1.9 *** | 1.8 *** | 1.8 *** |
| (1.2–2.3) | (0.6–1.1) | (1.5–2.5) | (1.4–2.4) | (1.4–2.4) | |
| Constant | 2.1 *** | 0.4 *** | 0.2 *** | 1.0 | 0.5 *** |
| (1.4–3.1) | (0.3–0.5) | (0.2–0.3) | (0.7–1.3) | (0.3–0.7) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lantos, H.; Manlove, J.; Wildsmith, E.; Faccio, B.; Guzman, L.; Moore, K.A. Parent-Teen Communication about Sexual and Reproductive Health: Cohort Differences by Race/Ethnicity and Nativity. Int. J. Environ. Res. Public Health 2019, 16, 833. https://doi.org/10.3390/ijerph16050833
Lantos H, Manlove J, Wildsmith E, Faccio B, Guzman L, Moore KA. Parent-Teen Communication about Sexual and Reproductive Health: Cohort Differences by Race/Ethnicity and Nativity. International Journal of Environmental Research and Public Health. 2019; 16(5):833. https://doi.org/10.3390/ijerph16050833
Chicago/Turabian StyleLantos, Hannah, Jennifer Manlove, Elizabeth Wildsmith, Bianca Faccio, Lina Guzman, and Kristin A. Moore. 2019. "Parent-Teen Communication about Sexual and Reproductive Health: Cohort Differences by Race/Ethnicity and Nativity" International Journal of Environmental Research and Public Health 16, no. 5: 833. https://doi.org/10.3390/ijerph16050833