Improving Dietary Behavior Among Ethnic Minority Women in Denmark: A Feasibility Study Based on a Participatory and Culturally Adapted Intervention


Abstract
:1. Introduction
2. Materials and Methods
2.1. The Intervention
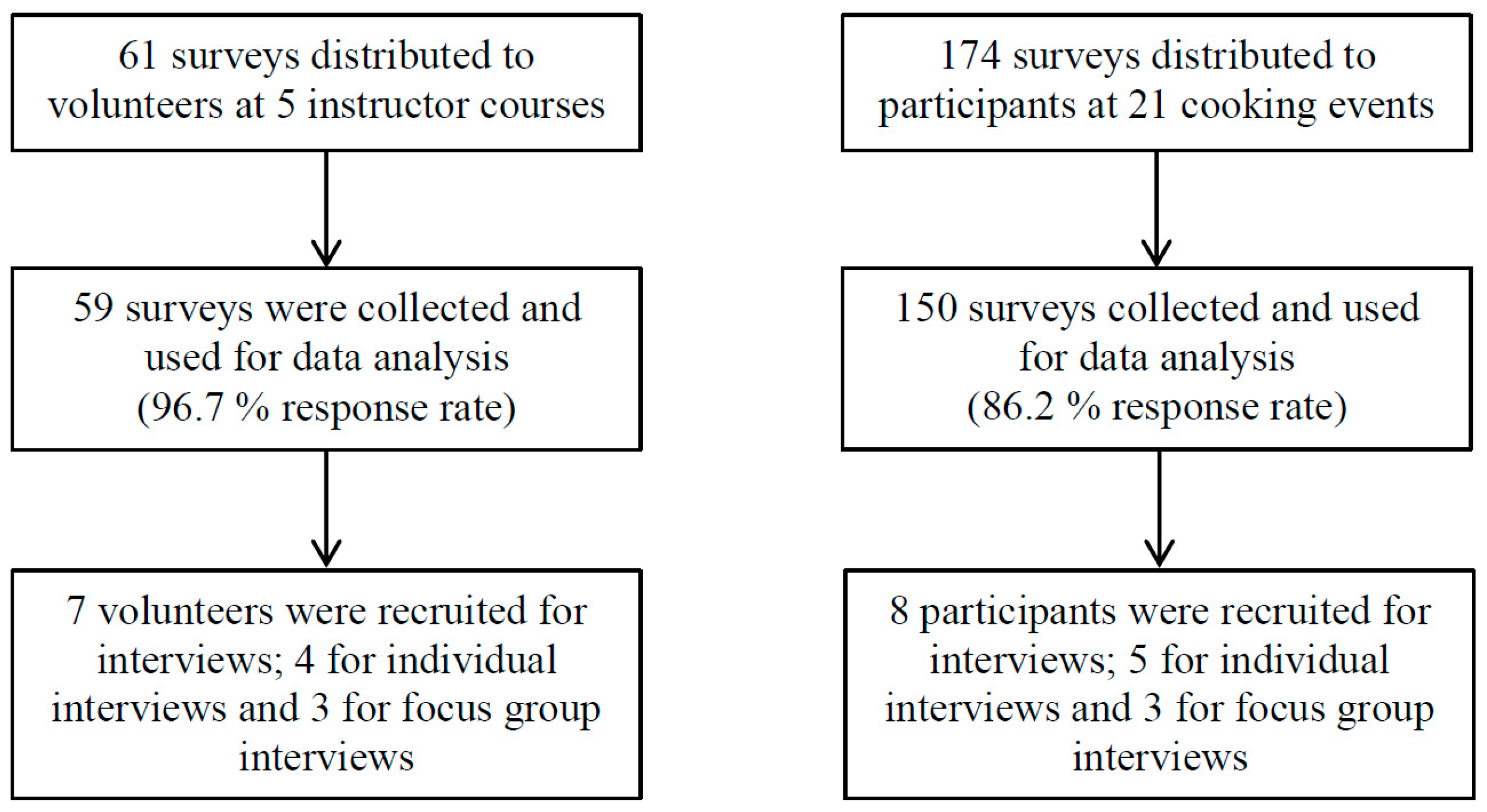
2.2. Study Design
2.3. Analysis
2.3.1. Motivating Healthy Dietary Behaviour
2.3.2. Cultural Adaption
2.4. Ethical Procedures
3. Results
3.1. Motivating Healthy Dietary Behaviour
3.2. Cultural Adaption
4. Discussion
4.1. Recruitment
4.2. Motivating Healthy Dietary Behaviour
4.3. Cultural Adaption
4.4. Strengths and Weaknesses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Estel, C.; Conti, C.R. Global burden of cardiovascular disease. Cardiovasc. Innov. Appl. 2016, 1, 369–377. [Google Scholar] [CrossRef]
- Mendis, S.; Puska, P.; Norrving, B. Global Atlas on Cardiovascular Disease Prevention and Control; World Health Organization in Collaboration with the World Heart Federation and the World Stroke Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Bo, A.; Zinckernagel, L.; Krasnik, A.; Petersen, J.H.; Norredam, M. Coronary heart disease incidence among non-Western immigrants compared to Danish-born people: Effect of country of birth, migrant status, and income. Eur. J. Prev. Cardiol. 2015, 22, 1281–1289. [Google Scholar] [CrossRef] [PubMed]
- Byberg, S.; Agyemang, C.; Zwisler, A.D.; Krasnik, A.; Norredam, M. Cardiovascular disease incidence and survival: Are migrants always worse off? Eur. J. Epidemiol. 2016, 31, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Bansal, N.; Fischbacher, C.M.; Bhopal, R.; Brown, H.; Steiner, M.; Capewell, S. Myocardial infarction incidence and survival by ethnic group: Scottish Health and Ethnicity Linkage retrospective cohort study. BMJ Open 2013, 3, e003415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norredam, M.; Agyemang, C.; Hansen, O.K.H.; Petersen, J.H.; Byberg, S.; Krasnik, A.; Kunst, A.E. Duration of residence and disease occurrence among refugees and family reunited immigrants: Test of the ‘Healthy Migrant Effect’ Hypothesis. Trop. Med. Int. Health 2014, 19, 958–967. [Google Scholar] [CrossRef] [PubMed]
- Davidson, E.M.; Liu, J.J.; Bhopal, R.; White, M.; Johnson, M.R.D.; Netto, G.; Wabnits, C.; Sheikh, A. Behavior change interventions to improve the health of racial and ethnic minority populations: A tool kit of adaptation approaches. Milbank Q. 2013, 91, 811–851. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, M.; Razum, O.; Tezcan-Güntekin, H.; Krasnik, A. Aging and health among migrants in a European perspective. Public Health Rev. 2016, 37, 20. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.J.; Davidson, E.; Bhopal, R.; White, M.; Johnson, M.; Netto, G.; Sheikh, A. Adapting health promotion interventions for ethnic minority groups: A qualitative study. Health Promot. Int. 2016, 31, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Lue Kessing, L.; Norredam, M.; Kvernrod, A.; Mygind, A.; Kristiansen, M. Contextualising migrants’ health behavior—A qualitative study of transnational ties and their implications for participation in mammography screening. BMC Public Health 2013, 13, 431. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, M.; Lue-Kessing, L.; Mygind, A.; Razum, O.; Norredam, M. Migration from low- to high-risk countries: A qualitative study of perceived risk of breast cancer and the influence on participation in mammography screening among migrant women in Denmark. Eur. J. Cancer Care 2014, 23, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Israel, B.A.; Schultz, A.J.; Parker, E.A. Community-based Participatory Research: Policy Recommendations for Promoting a Partnership Approach in Health Research. Educ. Health 2001, 14, 182–197. [Google Scholar]
- Dietary Recommendations. Available online: https://altomkost.dk/english/#c41067 (accessed on 25 January 2019).
- Cooking Videos: How to Make Heart Warm Food from All Over the World [Mad-Videoer: Sådan laver du Hjertevarm mad fra hele Verden]. Available online: https://hjerteforeningen.dk/2018/05/mad-videoer-saadan-laver-du-hjertevarm-mad-hele-verden/ (accessed on 25 January 2019).
- Castaneda-Gameros, D.; Redwood, S.; Thompson, J.L. Nutrient Intake and Factors Influencing Eating Behaviors in Older Migrant Women Living in the United Kingdom. Ecol. Food Nutr. 2017, 57, 50–68. [Google Scholar] [CrossRef] [PubMed]
- Garduño-Diaz, S.D.; Khokhar, S. Eating habits and nutrient intake of migrant South Asians in the UK. Public Health 2014, 128, 1043–1046. [Google Scholar] [CrossRef] [PubMed]
- Bhopal, R.S. Terminology and classifications for migrant, ethnic and racial groups: The centralty of census and population registers. In Migration, Ethnicity, Race, and Health in Multicultural Societies, 2nd ed.; Bhopal, R.S., Ed.; Oxford University Press: Oxford, UK, 2014; pp. 33–51. [Google Scholar]
- Divers, J.; Redden, D.T.; Rice, K.M.; Vaughan, L.K.; Padilla, M.A.; Allison, D.B.; Bluemke, D.A.; Young, H.J.; Arnett, D.K. Comparing Self-Reported Ethnicity to Genetic Background Measures in the Context of the Multi-Ethnic Study of Atherosclerosis (MESA). BMC Genet. 2011, 12, 28. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, S.; Hempler, N.; Krasnik, A. Issues to Consider When Measuring and Applying Socioeconomic Position Quantitatively in Immigrant Health Research. Int. J. Environ. Res. Public Health 2013, 10, 6354–6365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Danish Health Authority; The National Institute of Public Health Sundhedsstyrelsen. Danskernes Sundhed. Den Nationale Sundhedsprofil 2013—Fælles kernespørgsmål, 2013. [Health in Denmark. The National Health Profile 2013—Core Questions 2013]; The Danish Health Authority: Copenhagen, Denmark, 2013. [Google Scholar]
- Smailes, P.; Reider, C.; Hallarn, R.K.; Hafer, L.; Wallace, L.; Miser, W.F. Implementation of a Research Participant Satisfaction Survey at an Academic Medical Center. Clin. Res. 2016, 30, 42–47. [Google Scholar]
- Watanabe, T.; Berry, T.R.; Willows, N.D.; Bell, R.C. Assessing Intentions to Eat Low-Glycemic Index Foods by Adults with Diabetes Using a New Questionnaire Based on the Theory of Planned Behaviour. Can. J. Diabetes 2015, 39, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Diderichsen, F.; Andersen, I.; Manuel, C.; Andersen, A.N.; Bach, E.; Baadsgaard, M.; Brønnum-Hansen, H.; Hansen, F.K.; Jeune, B.; Jørgensen, T.; et al. Health inequality—Determinants and policies. Scand. J. Public Health 2012, 40, 12–105. [Google Scholar] [CrossRef] [PubMed]
- Patil, C.L.; Hadley, C.; Nahayo, P.D. Unpacking dietary acculturation among new Americans: Results from formative research with African refugees. J. Immigr. Minority Health 2009, 11, 342–358. [Google Scholar] [CrossRef] [PubMed]
- Lecerof, S.S.; Westerling, R.; Moghaddassi, M.; Östergren, P.O. Health information for migrants: The role of educational level in prevention of overweight. Scand. J. Public Health 2011, 39, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Park, M.H.; Falconer, C.L.; Croker, H.; Saxena, S.; Kessel, A.S.; Viner, R.M.; Kinra, S. Predictors of health-related behaviour change in parents of overweight children in England. Prev. Med. 2014, 62, 20–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sniehotta, F.F.; Scholz, U.; Schwarzer, R. Bridging the intention–behaviour gap: Planning, self-efficacy, and action control in the adoption and maintenance of physical exercise. Psychol. Health 2005, 20, 143–160. [Google Scholar] [CrossRef] [Green Version]
- Rechel, B.; Mladovsky, P.; Ingleby, D.; Mackenbach, J.P.; McKee, M. Migration and health in an increasingly diverse Europe. Lancet 2013, 381, 1235–1245. [Google Scholar] [CrossRef]
- Clark, L.; Hofsess, L. Acculturation. In Handbook of Immigrant Health; Loue, S., Ed.; Plenum Press: New York, NY, USA, 1998; pp. 37–59. [Google Scholar]
- Allen, J.D.; Caspi, C.; Yang, M.; Leyva, B.; Stoddard, A.M.; Tamers, S.; Tucker-Seeley, R.D.; Sorensen, G.C. Pathways between acculturation and health behaviors among residents of low-income housing: The mediating role of social and contextual factors. Soc. Sci. Med. 2014, 123, 26–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, L.B.; Sanbaek, A.; Thomsen, J.L.; Bjerregaard, A.L. Uptake of health checks by residents from the Danish social housing sector—A register-based cross-sectional study of patient characteristics in the ‘Your Life—Your Health’ program. BMC Public Health 2018, 18, 585. [Google Scholar] [CrossRef] [PubMed]
- Holmboe-Ottesen, G.; Wandel, M. Changes in dietary habits after migration and consequences for health: A focus on South Asians in Europe. Food Nutr. Res. 2012, 56, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, P.A.; Khokhar, S. Changing dietary habits of ethnic groups in Europe and implications for health. Nutr. Rev. 2008, 66, 203–215. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Volunteers (n = 59) Frequency (%) | Participants (n = 150) Frequency (%) |
|---|---|---|
| Age | ||
| 17–24 years | 2 (3.4%) | 9 (6.5%) |
| 25–34 years | 4 (6.9%) | 14 (10.1%) |
| 35–44 years | 19 (32.8%) | 41 (29.7%) |
| 45–54 years | 25 (43.1%) | 47 (34.1%) |
| 55–64 years | 5 (8.6%) | 18 (13.0%) |
| 65–74 years | 3 (5.2%) | 8 (5.8%) |
| 75–84 years | - | 1 (0.7%) |
| Missing | 1 | 12 |
| Continental region | ||
| Europe | 5 (8.6%) | 22 (15.0%) |
| North Africa | 6 (10.3%) | 15 (25.2%) |
| East Africa | 10 (17.2%) | 17 (11.6%) |
| Middle East | 27 (46.6%) | 70 (47.6%) |
| South Asia | 10 (17.2%) | 23 (15.6%) |
| Missing | 1 | 3 |
| Number of years in Denmark | ||
| 1–10 years | 9 (16.7%) | 22 (19.5%) |
| 11–20 years | 17 (31.5%) | 39 (34.5%) |
| 21+ years | 28 (51.9%) | 52 (46.0%) |
| Missing | 5 | 37 |
| Marital status | ||
| Married/living with partner | 33 (55.9%) | 96 (65.8%) |
| Divorced/separated | 15 (25.4%) | 18 (12.3%) |
| Unmarried/single | 9 (15.3%) | 16 (11.0%) |
| Widow | 2 (3.4%) | 14 (9.6%) |
| Other | - | 2 (1.4%) |
| Missing | 0 | 4 |
| Highest completed level of education | ||
| One or more shorter courses | 25 (47.2%) | 40 (35.1%) |
| Vocational education/skilled work | 5 (9.4%) | 20 (17.5%) |
| Short higher education | 11 (20.8) | 17 (14.9%) |
| Middle higher education | 5 (9.4%) | 24 (21.1%) |
| Long higher education | 3 (5.7%) | 7 (6.1%) |
| Another education | 4 (7.5%) | 6 (5.3%) |
| Missing | 6 | 36 |
| Employment status | ||
| Employed full-time | 7 (11.9%) | 15 (11.3%) |
| Employed part-time | 12 (20.3%) | 20 (15.0%) |
| Student | 8 (13.6%) | 28 (21.1%) |
| Retired | 9 (15.3%) | 29 (21.8%) |
| Unemployed | 14 (23.7%) | 22 (16.5%) |
| Other | 9 (15.3%) | 19 (14.3%) |
| Missing | 0 | 17 |
| Variable | Participants (n = 150) Frequency (%) |
|---|---|
| Number of identified healthy food principles | |
| 0 | 7 (4.9%) |
| 1 | 8 (5.6%) |
| 2 | 3 (2.1%) |
| 3 | 5 (3.5%) |
| 4 | 6 (4.2%) |
| 5 | 12 (8.5%) |
| 6 | 4 (2.8%) |
| 7 | 10 (7.0%) |
| 8 | 26 (18.3%) |
| 9 | 25 (17.6%) |
| 10 | 36 (25.4%) |
| Missing | 8 |
| Intention to cook healthy versions of traditional dishes in the future | |
| Yes | 120 (96.0%) |
| No | 5 (4.0%) |
| Missing | 25 |
| Intention to use measuring equipment in daily cooking routine | |
| Yes | 107 (84.3%) |
| No | 20 (15.7%) |
| Missing | 23 |
| Identify the Ten Healthy Food Principles. | Will You Use Measuring Equipment in Your Daily Cooking Routine? | Will You Cook Healthy Version of the Traditional Dishes in the Future? | ||||
|---|---|---|---|---|---|---|
| Yes | No | Significance | Yes | No | Significance | |
| Identified 8–10 | 72 (86.7%) | 11 (13.3%) | χ2: 1.1 p = 0.289 | 77 (97.5%) | 2 (2.5%) | χ2: 1.4 p = 0.237 |
| Identified 0–7 | 35 (79.5%) | 9 (20.5%) | 40 (93.0%) | 3 (7%) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pallesen, A.V.J.; Byberg, S.; Kristiansen, M. Improving Dietary Behavior Among Ethnic Minority Women in Denmark: A Feasibility Study Based on a Participatory and Culturally Adapted Intervention. Int. J. Environ. Res. Public Health 2019, 16, 795. https://doi.org/10.3390/ijerph16050795
Pallesen AVJ, Byberg S, Kristiansen M. Improving Dietary Behavior Among Ethnic Minority Women in Denmark: A Feasibility Study Based on a Participatory and Culturally Adapted Intervention. International Journal of Environmental Research and Public Health. 2019; 16(5):795. https://doi.org/10.3390/ijerph16050795
Chicago/Turabian StylePallesen, Anna Vera Jørring, Stine Byberg, and Maria Kristiansen. 2019. "Improving Dietary Behavior Among Ethnic Minority Women in Denmark: A Feasibility Study Based on a Participatory and Culturally Adapted Intervention" International Journal of Environmental Research and Public Health 16, no. 5: 795. https://doi.org/10.3390/ijerph16050795