The Intervention Effect of SMS Delivery on Chinese Adolescent’s Physical Activity

 ,
,
Abstract
:1. Introduction
1.1. Physical Activity and Obesity
1.2. PA Intervention with Short Message Service (SMS)
1.3. The Theoretical Framework of the Study
1.4. Research Questions of the Study
- (1)
- What is the effect of the frequency and timing of the delivery of SMS impact on the quantity of adolescent’s PA?
- (2)
- Would the stages of motivational readiness for PA be affected as a result of the SMS intervention?
- (3)
- Would adolescents perceive a difference in benefits and barriers to PA as a result of the SMS intervention?
2. Materials and Methods
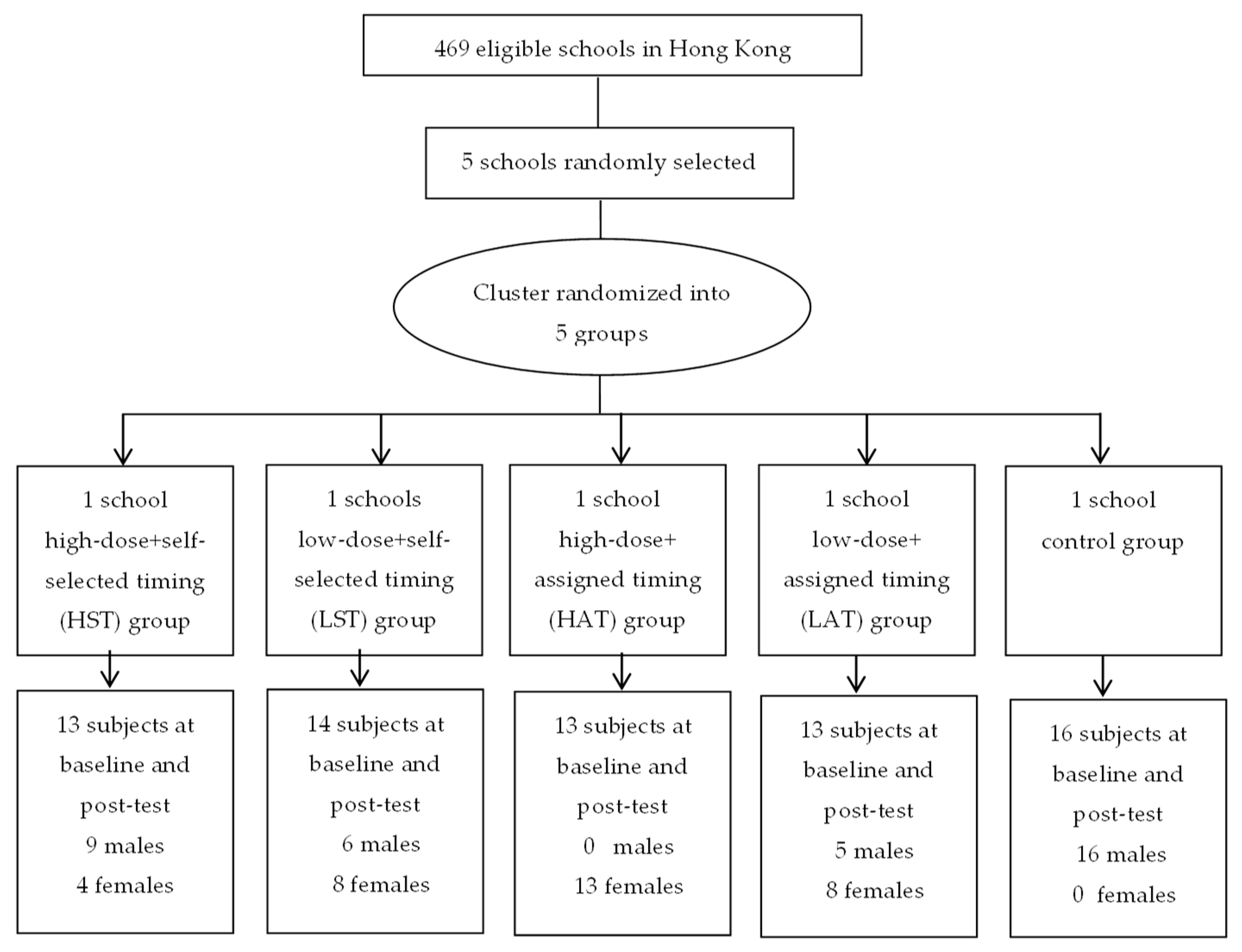
2.1. Participants
2.2. Procedures
- (1)
- High-frequency + self-selected timing (HST): Participants received five SMS per week (on weekdays). Self-determined timing for the receipt of SMS (before school/afterschool/after dinner).
- (2)
- Low-frequency + self-selected timing (LST): Participants received three SMS per week. Self-determined timing for the receipt of SMS.
- (3)
- High-frequency + assigned timing (HAT): Participants received five SMS per week. Assigned timing for the receipt of SMS (after school).
- (4)
- Low-frequency + assigned timing (LAT). Participants received three SMS per week. Assigned timing for the receipt of SMS (after school).
- (5)
- Control group (C). No treatment.
2.3. Measures
2.4. Intervention
2.5. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Intervention Effect on PA
3.3. Intervention Effect on Exercise Benefits and Barriers
4. Discussion
4.1. What Is the Effect of SMS Delivery Frequency and Timing on Chinese Adolescents’ PA?
4.2. Were the Stages of Motivational Readiness Affected As a Result of the SMS Intervention?
4.3. Was There a Difference in Perceived Benefits and Barriers As a Result of the SMS Intervention?
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mazurek, M.O.; Engelhardt, C.R. Video Game Use and Problem Behaviors in Boys with Autism Spectrum Disorders. Res. Autism Spectr. Disord. 2013. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T. Physical Activity, Sedentary Behavior, and Health: Paradigm Paralysis or Paradigm Shift? Diabetes 2010. [Google Scholar] [CrossRef] [PubMed]
- Müller, A.M.; Khoo, S.; Lambert, R. Review of Physical Activity Prevalence of Asian School-Age Children and Adolescents. Asia-Pac. J. Public Health 2013. [Google Scholar] [CrossRef]
- The Boys’ and Girls’ Clubs Association of Hong Kong. Exercise and Happiness-Survey on Hong Kong Children’s Happiness; The Boys’ and Girls’ Clubs Association of Hong Kong: Hong Kong, China, 2018. (In Chinese) [Google Scholar]
- Huang, W.Y.; Wong, S.H.S.; Sit, C.H.P.; Wong, M.C.S.; Sum, R.K.W.; Wong, S.W.S.; Yu, J.J. Results from the Hong Kong’s 2018 Report Card on Physical Activity for Children and Youth. J. Exerc. Sci. Fit. 2019, 17, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, T.; Cerin, E.; Baranowski, J. Steps in the Design, Development and Formative Evaluation of Obesity Prevention-Related Behavior Change Trials. Int. J. Behav. Nutr. Phys. Act. 2009. [Google Scholar] [CrossRef] [PubMed]
- Fanning, J.; Mullen, S.P.; Mcauley, E. Increasing Physical Activity with Mobile Devices: A Meta-Analysis. J. Med. Internet Res. 2012. [Google Scholar] [CrossRef] [PubMed]
- Free, C.; Phillips, G.; Galli, L.; Watson, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The Effectiveness of Mobile-Health Technology-Based Health Behaviour Change or Disease Management Interventions for Health Care Consumers: A Systematic Review. PLoS Med. 2013. [Google Scholar] [CrossRef] [PubMed]
- Orr, J.A.; King, R.J. Mobile Phone SMS Messages Can Enhance Healthy Behaviour: A Meta-Analysis of Randomised Controlled Trials. Health Psychol. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Vernig, P.M.; Repique, R.J.R. Short Message Service Can Be a Promising Tool for Psychiatric Patients and Clinicians. J. Am. Psychiatr. Nurses Assoc. 2015. [Google Scholar] [CrossRef] [PubMed]
- Bangure, D.; Chirundu, D.; Gombe, N.; Marufu, T.; Mandozana, G.; Tshimanga, M.; Takundwa, L. Effectiveness of Short Message Services Reminder on Childhood Immunization Programme in Kadoma, Zimbabwe—A Randomized Controlled Trial, 2013. BMC Public Health 2015. [Google Scholar] [CrossRef] [PubMed]
- Davis, D.R.; Abbitt, J.T. An Investigation of the Impact of an Intervention to Reduce Academic Procrastination Using Short Message Service (SMS) Technology. J. Interact. Online Learn. 2013, 12, 78–102. [Google Scholar]
- Noordam, A.C.; George, A.; Sharkey, A.B.; Jafarli, A.; Bakshi, S.S.; Kim, J.C. Assessing Scale-up of MHealth Innovations Based on Intervention Complexity: Two Case Studies of Child Health Programs in Malawi and Zambia. J. Health Commun. 2015. [Google Scholar] [CrossRef] [PubMed]
- Albino, S.; Tabb, K.M.; Requena, D.; Egoavil, M.; Pineros-Leano, M.F.; Zunt, J.R.; García, P.J. Perceptions and Acceptability of Short Message Services Technology to Improve Treatment Adherence amongst Tuberculosis Patients in Peru: A Focus Group Study. PLoS ONE 2014. [Google Scholar] [CrossRef] [PubMed]
- Markett, C.; Sánchez, I.A.; Weber, S.; Tangney, B. Using Short Message Service to Encourage Interactivity in the Classroom. Comput. Educ. 2006. [Google Scholar] [CrossRef]
- Beasley, R.E.; College, F. Short Message Service (SMS) Texting Symbols: A Functional Analysis of 10,000 Cellular Phone Text Messages. Matrix 2009, 9, 89–99. [Google Scholar]
- Daliot-Bul, M. Japan’s Mobile Technoculture: The Production of a Cellular Playscape and Its Cultural Implications. Media Cult. Soc. 2007. [Google Scholar] [CrossRef]
- Thulin, E.; Vilhelmson, B. Mobiles Everywhere: Youth, the Mobile Phone, and Changes in Everyday Practice. Young 2007. [Google Scholar] [CrossRef]
- Oksman, V.; Turtiainen, J. Mobile Communication as a Social Stage: Meanings of Mobile Communication in Everyday Life among Teenagers in Finland. New Media Soc. 2004. [Google Scholar] [CrossRef]
- Ferrer-Roca, O.; Cárdenas, A.; Diaz-Cardama, A.; Pulido, P. Mobile Phone Text Messaging in the Management of Diabetes. J. Telemed. Telecare 2004. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.R.; Yoo, S.K.; Jung, S.M.; Kwon, N.Y.; Hong, C.S. A Web-Based Mobile Asthma Management System. J. Telemed. Telecare 2005. [Google Scholar] [CrossRef] [PubMed]
- Neville, R.; Greene, A.; McLeod, J.; Tracey, A.; Surie, J. Mobile Phone Text Messaging Can Help Young People Manage Asthma. BMJ 2002. [Google Scholar] [CrossRef]
- Lim, M.S.C.; Hocking, J.S.; Hellard, M.E.; Aitken, C.K. SMS STI: A Review of the Uses of Mobile Phone Text Messaging in Sexual Health. Int. J. STD AIDS 2008. [Google Scholar] [CrossRef] [PubMed]
- Obermayer, J.L.; Riley, W.T.; Asif, O.; Jean-Mary, J. College Smoking-Cessation Using Cell Phone Text Messaging. J. Am. Coll. Heal. 2004. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, R.; Dorey, E.; Bramley, D.; Bullen, C.; Denny, S.; Elley, C.R.; Maddison, R.; McRobbie, H.; Parag, V.; Rodgers, A.; et al. A Theory-Based Video Messaging Mobile Phone Intervention for Smoking Cessation: Randomized Controlled Trial. J. Med. Internet Res. 2011. [Google Scholar] [CrossRef] [PubMed]
- Morak, J.; Schindler, K.; Goerzer, E.; Kastner, P.; Toplak, H.; Ludvik, B.; Schreier, G. A Pilot Study of Mobile Phone-Based Therapy for Obese Patients. J. Telemed. Telecare 2008. [Google Scholar] [CrossRef] [PubMed]
- Hurling, R.; Catt, M.; De Boni, M.; Fairley, B.W.; Hurst, T.; Murray, P.; Richardson, A.; Sodhi, J.S. Using Internet and Mobile Phone Technology to Deliver an Automated Physical Activity Program: Randomized Controlled Trial. J. Med. Internet Res. 2007. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, J.R.; Bauer, S.; Hamer, R.M.; Kordy, H.; Ward, D.; Bulik, C.M. Use of Text Messaging for Monitoring Sugar-Sweetened Beverages, Physical Activity, and Screen Time in Children: A Pilot Study. J. Nutr. Educ. Behav. 2008. [Google Scholar] [CrossRef] [PubMed]
- Newton, K.H.; Wiltshire, E.J.; Elley, C.R. Pedometers and Text Messaging to Increase Physical Activity: Randomized Controlled Trial of Adolescents with Type 1 Diabetes. Diabetes Care 2009. [Google Scholar] [CrossRef] [PubMed]
- Sirriyeh, R.; Lawton, R.; Ward, J. Physical Activity and Adolescents: An Exploratory Randomized Controlled Trial Investigating the Influence of Affective and Instrumental Text Messages. Br. J. Health Psychol. 2010. [Google Scholar] [CrossRef] [PubMed]
- Lau, P.W.C.; Lau, E.Y.; Wong, D.P.; Ransdell, L. A Systematic Review of Information and Communication Technology-Based Interventions for Promoting Physical Activity Behavior Change in Children and Adolescents. J. Med. Internet Res. 2011. [Google Scholar] [CrossRef] [PubMed]
- Nigg, C.R.; Geller, K.S.; Motl, R.W.; Horwath, C.C.; Wertin, K.K.; Dishman, R.K. A Research Agenda to Examine the Efficacy and Relevance of the Transtheoretical Model for Physical Activity Behavior. Psychol. Sport Exerc. 2011. [Google Scholar] [CrossRef] [PubMed]
- Umstattd, M.R.; Hallam, J. Use of Social Cognitive Theory Variables across Exercise Stages of Change of Employed Women. Am. J. Health Stud. 2006, 21, 44. [Google Scholar]
- Kim, Y. A Stage-Matched Intervention for Exercise Behaviour Change Based on the Transtheoretical Model. Psychol. Rep. 2008, 102, 939–950. [Google Scholar] [CrossRef] [PubMed]
- De Bourdeaudhuij, I.; Philippaerts, R.; Crombez, G.; Matton, L.; Wijndaele, K.; Balduck, A.L.; Lefevre, J. Stages of Change for Physical Activity in a Community Sample of Adolescents. Health Educ. Res. 2005. [Google Scholar] [CrossRef] [PubMed]
- Taymoori, P.; Niknami, S.; Berry, T.; Ghofranipour, F.; Kazemnejad, A. Application of the Health Promotion Model to Predict Stages of Exercise Behaviour in Iranian Adolescents. East. Mediterr. Heal. J. 2009. [Google Scholar] [CrossRef]
- Martins, J.; Marques, A.; Sarmento, H.; Carreiro Da Costa, F. Adolescents’ Perspectives on the Barriers and Facilitators of Physical Activity: A Systematic Review of Qualitative Studies. Health Educ. Res. 2014. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y. Differences in Physical Activity and Perceived Benefits and Barriers among Normal Weight, Overweight, and Obese Adolescents. Percept. Mot. Skills 2013. [Google Scholar] [CrossRef] [PubMed]
- Ransdell, L.B.; Detling, N.; Hildebrand, K.; Lau, P.; Moyer-Mileur, L.; Shultz, B. Can Physical Activity Interventions Change Perceived Exercise Benefits and Barriers? Am. J. Health Stud. 2004, 19, 195–204. [Google Scholar]
- Hall, A.; Cole-Lewis, H.; Bernhardt, J.M. Mobile Text Messaging for Health: A Systematic Review of Reviews. Annu. Rev. Public Health 2015. [Google Scholar] [CrossRef] [PubMed]
- Lau, E.Y.; Lau, P.W.C.; Chung, P.-K.; Ransdell, L.B.; Archer, E. Evaluation of an Internet–Short Message Service–Based Intervention for Promoting Physical Activity in Hong Kong Chinese Adolescent School Children: A Pilot Study. Cyberpsychology. Behav. Soc. Netw. 2012. [Google Scholar] [CrossRef] [PubMed]
- Crocker, P.R.E.; Bailey, D.A.; Faulkner, R.A.; Kowalski, K.C.; Mcgrath, R. Measuring General Levels of Physical Activity: Preliminary Evidence for the Physical Activity Questionnaire for Older Children. Med. Sci. Sports Exerc. 1997. [Google Scholar] [CrossRef]
- Wang, J.J.; Baranowski, T.; Lau, W.P.; Chen, T.A.; Pitkethly, A.J. Validation of the Physical Activity Questionnaire for Older Children (PAQ-C) among Chinese Children. Biomed. Environ. Sci. 2016. [Google Scholar] [CrossRef]
- The President’s Council on Physical Fitness and Sports Report. Physical Activity and Sport in the Lives of Girls; President’s Council on Physical Fitness and Sport: Rockville, MD, USA, 2003. [Google Scholar]
- Garcia, A.W.; Pender, N.J.; Antonakos, C.L.; Ronis, D.L. Changes in Physical Activity Beliefs and Behaviors of Boys and Girls across the Transition to Junior High School. J. Adolesc. Health 1998. [Google Scholar] [CrossRef]
- Hagger, M.; Chatzisarantis, N.L.D.; Hein, V.; Soós, I.; Karsai, I.; Lintunen, T.; Leemans, S. Teacher, Peer and Parent Autonomy Support in Physical Education and Leisure-Time Physical Activity: A Trans-Contextual Model of Motivation in Four Nations. Psychol. Health 2009. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, D.A.; Carlson, R.A.; Gilmore, R.O. Acquisition of Intellectual and Perceptual-Motor Skills. Annu. Rev. Psychol. 2001. [Google Scholar] [CrossRef] [PubMed]
- Grubbs, L.; Carter, J. The Relationship of Perceived Benefits and Barriers to Reported Exercise Behaviors in College Undergraduates. Fam. Community Health 2002. [Google Scholar] [CrossRef]
- Blanchard, C.M.; Fortier, M.; Sweet, S.; O’Sullivan, T.; Hogg, W.; Reid, R.D.; Sigal, R.J. Explaining Physical Activity Levels from a Self-Efficacy Perspective: The Physical Activity Counseling Trial. Ann. Behav. Med. 2007. [Google Scholar] [CrossRef]
- O’Dea, J.A. Why Do Kids Eat Healthful Food? Perceived Benefits of and Barriers to Healthful Eating and Physical Activity among Children and Adolescents. J. Am. Diet. Assoc. 2003. [Google Scholar] [CrossRef]
- Webb, T.L.; Joseph, J.; Yardley, L.; Michie, S. Using the Internet to Promote Health Behavior Change: A Systematic Review and Meta-Analysis of the Impact of Theoretical Basis, Use of Behavior Change Techniques, and Mode of Delivery on Efficacy. J. Med. Internet Res. 2010. [Google Scholar] [CrossRef] [PubMed]
- Buhi, E.R.; Trudnak, T.E.; Martinasek, M.P.; Oberne, A.B.; Fuhrmann, H.J.; McDermott, R.J. Mobile Phone-Based Behavioural Interventions for Health: A Systematic Review. Health Educ. J. 2013. [Google Scholar] [CrossRef]


{kind=link}
| Groups | n | Gender n (%) | Age (years) n (%) | Body Mass Index (kg/m2) Mean (SD) | ||
|---|---|---|---|---|---|---|
| Male | Female | 12–13 | 14–16 | |||
| HST | 13 | 9 (69.2) | 4 (30.8) | 8 (61.5) | 5 (38.5) | 20.32 (4.30) |
| LST | 14 | 6 (42.9) | 8 (57.1) | 3 (21.4) | 11 (78.6) | 20.07 (2.60) |
| HAT | 13 | 0 (0.0) | 13 (100.0) | 9 (69.2) | 4 (30.8) | 20.95 (2.95) |
| LAT | 13 | 5 (38.5) | 8 (61.5) | 6 (46.2) | 7 (53.8) | 20.92 (3.59) |
| Control | 16 | 16 (100.0) | 0 (0.0) | 2 (12.5) | 14 (87.5) | 20.51 (3.56) |
| Group | n | PAQ-C Total Score (Mean (SD)) | n | Stage Movement (n (%)) | |||
|---|---|---|---|---|---|---|---|
| Baseline | Post Test | Regression to a Lower Stage | Stable | Progression to a Higher Stage | |||
| HST | 13 | 16.46 (6.54) | 18.75 (10.57) | 13 | 1 (7.7) | 7 (53.8) | 5 (38.5) |
| LST | 14 | 21.31 (11.58) | 18.31 (12.99) | 14 | 3 (23.1) | 4 (30.8) | 6 (46.2) |
| HAT | 13 | 22.46 (12.84) | 20.38 (12.22) | 13 | 3 (23.1) | 5 (38.5) | 5 (38.5) |
| LAT | 13 | 19.69 (8.59) | 21.85 (8.68) | 13 | 2 (15.4) | 8 (61.5) | 3 (23.1) |
| Control | 13 | 27.18 (13.40) | 23.81 (13.34) | 16 | 5 (31.3) | 8 (50.0) | 3 (18.8) |
| Group | n | Exercise Benefit Score | Exercise Barrier Score | Benefits/Barriers Differential Score | |||
|---|---|---|---|---|---|---|---|
| Baseline | Post Test | Baseline | Post-Test | Baseline | Post-Test | ||
| HST | 13 | 27.54 (6.30) | 27.08 (4.82) | 28.80 (6.47) | 24.33 (7.90) | −1.23 (7.81) | 3.08 (8.48) |
| LST | 14 | 33.38 (5.92) | 36.69 (4.59) | 29.93 (6.62) | 30.62 (6.21) | 3.08 (8.64) | 5.25 (7.82) |
| HAT | 13 | 34.00 (5.35) | 35.00 (6.72) | 30.69 (8.37) | 27.15 (7.07) | 3.31 (8.13) | 7.85 (8.36) |
| LAT | 13 | 31.62 (4.81) | 30.42 (2.47) | 28.08 (5.17) | 26.08 (4.84) | 3.54 (6.35) | 3.67 (4.19) |
| Control | 16 | 35.69 (5.02) | 33.06 (5.77) | 25.94 (7.08) | 25.36 (8.56) | 9.75 (10.61) | 7.50 (12.47) |
| Group | PAQ-C Total Score | |||||
|---|---|---|---|---|---|---|
| n | Pre-Test | Post-Test | p Value * | |||
| Mean | SD | Mean | SD | |||
| Intensity | ||||||
| High group | 19 | 19.42 | 10.97 | 20.68 | 11.54 | 0.043 |
| Low group | 21 | 18.76 | 9.12 | 19.14 | 11.39 | |
| Control group | 13 | 27.18 | 13.40 | 23.81 | 13.34 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lau, P.W.C.; Pitkethly, A.J.; Leung, B.W.C.; Lau, E.Y.; Wang, J.-J. The Intervention Effect of SMS Delivery on Chinese Adolescent’s Physical Activity. Int. J. Environ. Res. Public Health 2019, 16, 787. https://doi.org/10.3390/ijerph16050787
Lau PWC, Pitkethly AJ, Leung BWC, Lau EY, Wang J-J. The Intervention Effect of SMS Delivery on Chinese Adolescent’s Physical Activity. International Journal of Environmental Research and Public Health. 2019; 16(5):787. https://doi.org/10.3390/ijerph16050787
Chicago/Turabian StyleLau, Patrick W. C., Amanda J. Pitkethly, Beeto W. C. Leung, Erica Y. Lau, and Jing-Jing Wang. 2019. "The Intervention Effect of SMS Delivery on Chinese Adolescent’s Physical Activity" International Journal of Environmental Research and Public Health 16, no. 5: 787. https://doi.org/10.3390/ijerph16050787