The Effects of Tai Chi on Markers of Atherosclerosis, Lower-limb Physical Function, and Cognitive Ability in Adults Aged Over 60: A Randomized Controlled Trial

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
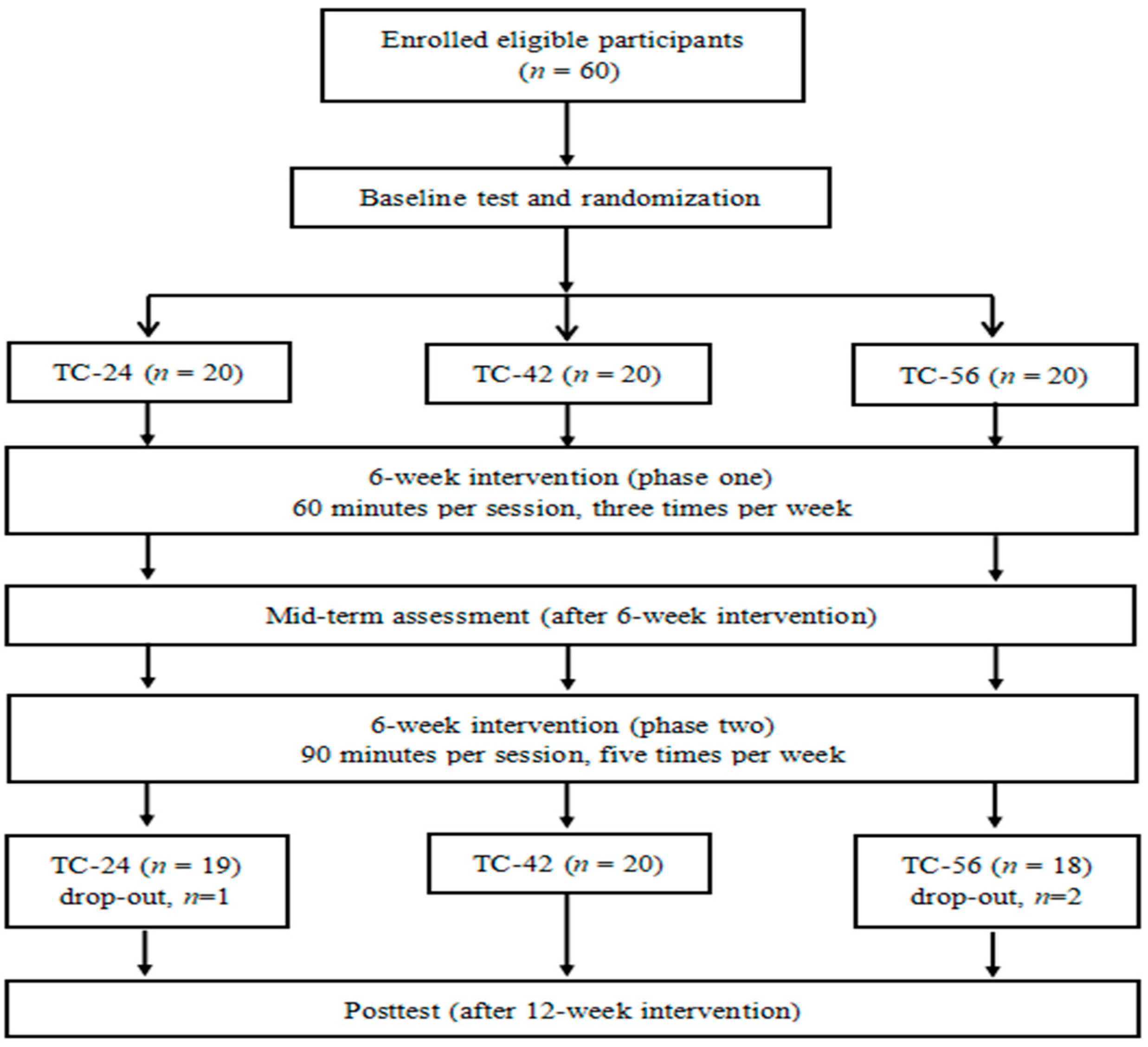
2.1. Study Participants
2.2. Three Different Styles of Tai Chi Intervention
2.3. Outcome Measures
2.3.1. Demographic and Anthropometric Information
2.3.2. Atherosclerosis
2.3.3. Cognitive Ability
2.3.4. Physical Function in Lower Limbs
Chair Rise Performance Test
Balance
The 6-Meter Walk Test (6MWT)
Timed Up and Go Test (TUG)
2.4. Data Analysis
3. Results
3.1. Baseline Data
3.2. Intervention Effects
3.2.1. Atherosclerosis
3.2.2. Cognitive Ability
3.2.3. Chair Rise Performance Test
3.2.4. Balance
3.2.5. MWT Test
3.2.6. TUG Test
4. Discussion
4.1. Ankle Brachial Index and Ankle Pulse Wave Velocity
4.2. Cognitive Ability
4.3. Physical Function in Lower Extremity
4.4. Strength and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Beard, J.R.; Officer, A.; De Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.M.E.E.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef]
- Pongiglione, B.; De Stavola, B.L.; Ploubidis, G.B. A systematic literature review of studies analyzing inequalities in health expectancy among the older population. PLoS One 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Suzman, R.; Beard, J.R.; Boerma, T.; Chatterji, S. Health in an ageing world—What do we know? Lancet 2015, 385, 484–486. [Google Scholar] [CrossRef]
- Stubbs, B.; Binnekade, T.; Eggermont, L.; Sepehry, A.A.; Patchay, S.; Schofield, P. Pain and the risk for falls in community-dwelling older adults: Systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2014, 95, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Palmefors, H.; DuttaRoy, S.; Rundqvist, B.; Börjesson, M. The effect of physical activity or exercise on key biomarkers in atherosclerosis - A systematic review. Atherosclerosis 2014, 235, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Loprinzin, P.D.; Crush, E.; Joyner, C. Cardiovascular disease biomarkers on cognitive function in older adults: Joint effects of cardiovascular disease biomarkers and cognitive function on mortality risk. Prev. Med. 2017, 94, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.N.; Gau, B.S.; Lou, M.F. The effectiveness of exercise on improving cognitive function in older people: A systematic review. J. Nurs. Res. 2011, 19, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Asteasu, M.L.S.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Casas-Herrero, Á.; Izquierdo, M. Role of physical exercise on cognitive function in healthy older adults: A systematic review of randomized clinical trials. Ageing Res. Rev. 2017, 37, 117–134. [Google Scholar] [CrossRef] [PubMed]
- Heyn, P.C.; Johnson, K.E.; Kramer, A.F. Endurance and strength training outcomes on cognitively impaired and cognitively intact older adults: A meta-analysis. J. Nutr. Health Aging 2008, 12, 401–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, R.C.C.; So, K.F. Use of anti-aging herbal medicine, Lycium barbarum, against aging-associated diseases. What do we know so far? Cell. Mol. Neurobiol. 2008, 28, 643–652. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; Wahl, H.W.; Matthews, J.T.; De Vito Dabbs, A.; Beach, S.R.; Czaja, S.J. Advancing the aging and technology agenda in gerontology. Gerontologist 2015, 55, 724–734. [Google Scholar] [CrossRef] [PubMed]
- Boot, C.W. Aging and information technology use: Potential and barriers. Curr. Direct. Psychol. Sci. 2009, 18, 253–258. [Google Scholar] [CrossRef]
- Reiner, M.; Niermann, C.; Jekauc, D. Long-term health benefits of physical activity—A systematic review of longitudinal studies. BMC Public Health 2013, 13, 813. [Google Scholar] [CrossRef] [PubMed]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Zhang, Y.J.; Liu, Y.; Tian, X.P.; Xiao, T.; Liu, X.L.; Yeung, A.; Liu, J.; Wang, X.Q.; Yang, Q. Effects of Tai Chi on lower limb proprioception in adults aged over 55: A systematic review and meta-analysis. Arch. Phys. Med. Rehab. 2018. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Zeng, N.; Wang, C.; Sun, L.; Thomas, G.A.; Wang, H. Effects of mind-body exercises for mood and functional capabilities in patients with stroke: An analytical review of randomized controlled trials. IJERPH 2018, 15, 721. [Google Scholar] [CrossRef] [PubMed]
- Cole, A.R.; Wijarnpreecha, K.; Chattipakorn, S.C. Effects of Tai Chi exercise on heart rate variability. Compl. Ther. Clin. Pract. 2016, 23, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Chen, X.; Wang, H. Baduanjin exercise for stroke rehabilitation: A systematic review with meta-analysis of randomized controlled trials. IJERPH 2018, 15, 600. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, C.; Zou, L.; Liu, X.; Song, W. The effects of mind-body exercise on cognitive performance in elderly: A systematic review and meta-analysis. IJERPH 2018, 15, 2791. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Sasaki, J.E.; Zeng, N.; Wang, C.; Sun, L. A systematic review with meta-analysis of mindful exercises on rehabilitative outcomes among poststroke patients. Arch. Phys. Med. Rehabil. 2018, 99, 2355–2364. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.M.; Maher, C.G.; Latimer, J. A randomized controlled trial of tai chi for long-term low back pain (TAI CHI): Study rationale, design, and methods. BMC Musculoskeletal Dis. 2009, 10, 55. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Piliae, R.E.; Coull, B.M. Community-based Yang-style Tai Chi is safe and feasible in chronic stroke: A pilot study. Clin. Rehabil. 2012, 26, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Sasaki, J.E.; Wei, G.-X.; Huang, T.; Yeung, A.S.; Neto, O.B.; Chen, K.W.; Hui, S.C. Effects of mind–body exercises (tai chi/yoga) on heart rate variability parameters and perceived stress: A systematic review with meta-analysis of randomized controlled trials. J. Clin. Med. 2018, 7, 404. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Li, C.; Wei, G.; Chen, K.; Kinser, P.; Chan, J. Effects of meditative movements on major depressive disorder: A systematic Review and meta-analysis of randomized controlled trials. J. Clin. Med. 2018, 7, 195. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Yeung, A.; Xiao, T.; Tian, X.; Kong, Z.; Zou, L.; Wang, X. Chen-Style Tai Chi for individuals (aged 50 years old or above) with chronic non-specific low back pain: a randomized controlled trial. Int. J. Environ. Res. Public Health 2019, 16, 517. [Google Scholar] [CrossRef] [PubMed]
- Blake, H.; Batson, M. Exercise intervention in brain injury: A pilot randomized study of Tai Chi Qigong. Clin. Rehab. 2009, 23, 589. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Chen, K.; Shu, Y.; Chen, X.; Luo, L.; Zhao, X. The effect of Tai Chi practice on attenuating bone mineral density loss: A systematic review and meta-analysis of randomized controlled trials. IJERPH 2017, 14, 1000. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Yu, D. Effect of a long-term modified Tai Chi-based intervention in attenuating bone mineral density in postmenopausal women in southeast China: Study protocol for a randomized controlled trial. Clin. Trial. Degen. Dis. 2017, 2, 46–52. [Google Scholar]
- Song, Q.H.; Zhang, Q.H.; Xu, R.M.; Ma, M.; Zhao, X.P.; Shen, G.Q.; Guo, Y.H.; Wang, Y. Effect of Tai-chi exercise on lower limb muscle strength, bone mineral density and balance function of elderly women. Int. J. Clin. Exp. Med. 2014, 7, 1569–1576. [Google Scholar] [PubMed]
- Zhang, Y.; Sun, J.; Li, N.; Su, Q. Effects of combined traditional chinese exercises on blood pressure and arterial function of adult female hypertensive patients. Res. Sport. Med. 2013, 21, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Piliae, R.E.; Hoke, T.M.; Hepworth, J.T.; Latt, L.D.; Najafi, B.; Coull, B.M. Effect of tai chi on physical function, fall rates and quality of life among older stroke survivors. Arch. Phys. Med. Rehabil. 2014, 95, 816–824. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Taylor, J.; Sanzo, P.; Zerpa, C. The effect of Tai Chi on functional lower extremity mobility and strength, ankle proprioception, and postural adaptation in older adults. Am. J. Med. Med. Sci. 2017, 7, 229–237. [Google Scholar] [CrossRef]
- Lu, X.; Hui-Chan, C.W.; Tsang, W.W. Tai Chi, arterial compliance, and muscle strength in older adults. Eur. J. Prev. Cardiol. 2013, 20, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.H.; Lee, Y.; Kim, S.G.; Choi, B.Y.; Lee, H.S.; Bang, S.Y. The beneficial effects of Tai Chi exercise on endothelial function and arterial stiffness in elderly women with rheumatoid arthritis. Arthritis Res. Ther. 2015, 17, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Piliae, R.E.; Newell, K.A.; Cherin, R.; Lee, M.J.; King, A.C.; Haskell, W.L. Effects of Tai Chi and western exercise on physical and cognitive functioning in healthy community-dwelling older adults. J. Aging Phys. Act. 2010, 18, 261–279. [Google Scholar] [CrossRef] [PubMed]
- Siu, M.; Lee, D.T.F. Effects of Tai Chi on cognition and instrumental activities of daily living in community dwelling older people with mild cognitive impairment. BMC Geriatr. 2018, 18, 37. [Google Scholar] [CrossRef] [PubMed]
- Maliha, G.; Townsend, R.R. A study of the VaSera arterial stiffness device in US patients. J. Clin. Hypertens (Greenwich) 2017, 19, 661–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loprinzi, P.D.; Abbott, K. Association of diabetic peripheral arterial disease and objectively-measured physical activity: NHANES 2003–2004. J. Iabet. & Metab. Dis. 2014, 13, 63. [Google Scholar]
- Matsushima, H.; Hosomi, N.; Hara, N.; Yoshimoto, T.; Neshige, S.; Kono, R.; Himeno, T.; Takeshima, S.; Takamatsu, K.; Shimoe, Y.; et al. Ability of the ankle brachial index and brachial-ankle pulse wave velocity to predict the 3-month outcome in patients with non-cardioembolic stroke. J. Ather. Thromb. 2017, 24, 1167–1173. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Li, D.; Li, F.; Zhou, A.; Wang, F.; Zuo, X.; Jia, X.F.; Song, H.; Jia, J. Montreal cognitive assessment in detecting cognitive impairment in Chinese elderly individuals: A population-based study. J. Geriat. Psy. Neur. 2011, 24, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.L.; Xu, Y.; Chu, A.Q.; Ding, D.; Liang, X.N.; Nasreddine, Z.S.; Dong, Q.; Hong, Z.; Zhao, Q.H.; Guo, Q.H. Validation of the chinese version of montreal cognitive assessment basic for screening mild cognitive impairment. J. Am. Geriatr. Soc. 2016, 64, e285–e290. [Google Scholar] [CrossRef] [PubMed]
- Hardy, R.; Cooper, R.; Shah, I.; Harridge, S.; Guralnik, J.; Kuh, D. Is chair rise performance a useful measure of leg power? Aging Clin. Experi. Res. 2010, 22, 412–418. [Google Scholar] [CrossRef] [Green Version]
- Michikawa, T.; Nishiwaki, Y.; Takebayashi, T.; Toyama, Y. One-leg standing test for elderly populations. J. Orthop. Sci. 2009, 14, 675–685. [Google Scholar] [CrossRef] [PubMed]
- Lyons, J.G.; Heeren, T.; Stuver, S.O.; Fredman, L. Assessing the agreement between 3-m and 6-m walk tests in 136 community-dwelling older adults. J. Aging Health 2015, 27, 594–605. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.P.; Si-Tou, J.I.; Tse, M.M.; Ng, S.S. Reliability and validity of the timed up and go test with a motor task in people with chronic stroke. Arch. Phys. Med. Rehabil. 2017, 98, 2213–2220. [Google Scholar] [CrossRef] [PubMed]
- Ato, D. Pitfalls in the ankle-brachial index and brachial-ankle pulse wave velocity. Vascul. Health Risk Manag. 2018, 14, 41–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Popele, N.M.; Grobbee, D.E.; Bots, M.L.; Asmar, R.; Topouchian, J.; Reneman, R.S. Association between arterial stiffness and atherosclerosis: The rotterdam study. Stroke 2001, 32, 454–460. [Google Scholar] [CrossRef]
- Schiffrin, E.L. Vascular stiffening and arterial compliance: Implications for systolic blood pressure. Amer. J. Hypert. 2004, 17, 39S–48S. [Google Scholar] [CrossRef] [PubMed]
- Herrington, W.; Lacey, B.; Sherliker, P.; Armitage, J.; Lewington, S. Epidemiology of atherosclerosis and the potential to reduce the global burden of atherothrombotic disease. Circ Res. 2016, 118, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Safar, M.E. Influence of lifestyle modification on arterial stiffness and wave reflections. Am. J. Hypert. 2005, 18, 137–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motivala, S.J.; Sollers, J.; Thayer, J.; Irwin, M.R. Tai Chi Chih acutely decreases sympathetic nervous system activity in older adults. J. Gerontol A Biol. Sci. Med. Sci. 2006, 61, 1177–1180. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Makita, S.; Uchida, R.; Ishihara, S.; Masuda, M. Effect of Tai Chi training on baroreflex sensitivity and heart rate variability in patients with coronary heart disease. Int. Heart, J. 2010, 51, 238–241. [Google Scholar] [CrossRef]
- Wayne, P.M.; Walsh, J.N.; Taylor-Piliae, R.E.; Wells, R.E.; Papp, K.V.; Donovan, N.J.; Yeh, G.Y. Effect of tai chi on cognitive performance in older adults: Systematic review and meta-analysis. J. Amer. Geriatr. Soc. 2014, 62, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G.; Liu, F.; Li, S.; Huang, M.; Tao, J.; Chen, L. Tai Chi and the protection of cognitive ability: A systematic review of prospective studies in healthy adults. Am. J. Prev. Med. 2015, 49, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Yin, W.; Wang, Y.T.; Elisabeth, O.; Burgessa, J. The effects of Tai Chi exercise on cognitive function in older adults: A meta-analysis. J. Sport Health Sci. 2013, 4, 193–203. [Google Scholar] [CrossRef]
- Wayne, P.M.; Yeh, G.; Mehta, D.H. Minding the mind-body literature: Aging and cognitive decline. J. Altern Complement Med. 2018, 24, 196–199. [Google Scholar] [CrossRef] [PubMed]
- Mortimer, J.A.; Ding, D.; Borenstein, A.R. Changes in brain volume and cognition in a randomized trial of exercise and social interaction in a community-based sample of non-demented chinese elders. J. Alzheimer’s Dis.: JAD 2012, 30, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Tangen, G.G.; Engedal, K.; Bergland, A.; Moger, T.A.; Mengshoel, A.M. Relationships between balance and cognition in patients with subjective cognitive impairment, mild cognitive impairment, and Alzheimer disease. Phys. Ther. 2014, 94, 1123–1134. [Google Scholar] [CrossRef] [PubMed]
- Simith-Ray, R.; Hughes, S.L.; Prohaska, T.R.; Little, D.M.; Jurivich, D.A.; Hedeker, D. Impact of cognitive training on balance and gait in older adults. J. Gerontol.: Series B 2015, 70, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Saverino, A.; Waller, D.; Rantell, K.; Parry, R.; Moriarty, A.; Playford, E.D. The role of ognitive factors in predicting balance and fall risk in a neuro-rehabilitation setting. PLoS ONE 2016, 11, e0153469. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| TC-24 Group (n = 19) | TC-42 Group (n = 20) | TC-56 Group (n= 18) | Statistics | |
|---|---|---|---|---|
| Demographic and anthropometric characteristics | ||||
| Age (year) | 67.4±5.9 | 64.9±3.5 | 64.5±3.6 | 2.393 |
| Sex (male/female, n) | 9/10 | 10/10 | 9/9 | 0.035 |
| BMI (kg/m2) | 23.4±2.9 | 24.6±2.3 | 25.0±2.6 | 2.250 |
| Resting heart rate (beats/minute) | 76.1±8.6 | 71.0±4.9 | 77.3±4.2 | 5.638 ** |
| Outcome variables | ||||
| ABI | ||||
| left side | 1.2±0.1 | 1.2±0.1 | 1.2±0.1 | 0.515 |
| right side | 1.2±0.1 | 1.1±0.1 | 1.2±0.1 | 0.962 |
| PWV | ||||
| left ankle | 7.2±1.3 | 6.1±0.7 | 6.2±0.8 | 6.762 ** |
| right ankle | 7.2±1.3 | 6.1±0.7 | 6.4±0.6 | 7.227 ** |
| MoCA | 26.5±1.5 | 26.0±1.4 | 25.8±1.5 | 1.107 |
| Chair rise performance test | 9.9±2.4 | 8.3±1.2 | 9.8±2.2 | 4.049 * |
| One leg standing test | ||||
| left leg | 4.7±3.0 | 1.9±1.1 | 3.0±1.7 | 9.070 *** |
| right leg | 3.3±2.7 | 2.3±1.8 | 3.7±2.2 | 2.028 |
| 6MWT | 5.6±1.4 | 4.8±0.5 | 5.0±0.5 | 4.666 * |
| TUG | 11.7±2.9 | 10.5±1.6 | 11.2±2.8 | 1.243 |
| TC-24 Group (n = 19) | TC-42 Group (n = 20) | TC-56 Group (n = 18) | F Value # | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 6-week | 12-week | 6-week | 12-week | 6-week | 12-week | Group | Time | Group X Time | |
| ABI | |||||||||
| left side | 1.2±0.1 | 1.2±0.1 | 1.1±0.1 | 1.2±0.1 | 1.2±0.1 | 1.1±0.1 | 0.239 | 1.134 | 2.632 * |
| right side | 1.1±0.1 | 1.1±0.1 | 1.1±0.1 | 1.1±0.2 | 1.1±0.1 | 1.1±0.1 | 0.218 | 0.065 | 0.453 |
| PWV | |||||||||
| left ankle | 7.1±1.2 | 6.8±1.0 | 6.1±0.7 | 5.9±0.6 | 6.1±0.7 | 5.9±0.6 | 3.951 * | 3.182 | 1.465 |
| right ankle | 7.1±1.2 | 6.9±1.2 | 6.0±0.7 | 5.9±0.7 | 6.3±0.6 | 6.0±0.5 | 1.699 | 1.423 | 1.796 |
| MoCA | 28.2±1.3 | 29.8±0.5 | 27.9±1.6 | 29.8±0.6 | 27.7±1.6 | 29.6±0.7 | 1.697 | 2.337 | 1.479 |
| Chair rise performance test | 9.5±2.3 | 8.8±1.7 | 7.9±1.2 | 7.6±1.0 | 9.2±2.0 | 8.9±1.8 | 0.168 | 0.480 | 2.013 |
| One leg standing test | |||||||||
| left leg | 5.5±3.0 | 5.7±3.3 | 2.4±1.2 | 3.2±1.0 | 4.2±2.3 | 5.3±1.8 | 15.628 *** | 1.160 | 4.888 * |
| right leg | 4.3±2.6 | 4.5±2.3 | 2.8±2.3 | 3.8±2.4 | 5.2±2.7 | 6.2±2.2 | 3.099 | 1.491 | 2.289 |
| 6MWT | 5.4±1.3 | 5.7±1.1 | 4.4±0.5 | 4.5±0.5 | 4.5±0.6 | 4.7±0.4 | 8.188 ** | 7.122 * | 3.137 |
| TUG | 11.3±2.8 | 10.4±2.1 | 10.0±1.5 | 9.0±1.3 | 10.7±2.7 | 9.3±1.9 | 1.024 | 5.581 ** | 1.052 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, S.; Zhang, Y.; Kong, Z.; Loprinzi, P.D.; Hu, Y.; Ye, J.; Liu, S.; Yu, J.J.; Zou, L. The Effects of Tai Chi on Markers of Atherosclerosis, Lower-limb Physical Function, and Cognitive Ability in Adults Aged Over 60: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 753. https://doi.org/10.3390/ijerph16050753
Zhou S, Zhang Y, Kong Z, Loprinzi PD, Hu Y, Ye J, Liu S, Yu JJ, Zou L. The Effects of Tai Chi on Markers of Atherosclerosis, Lower-limb Physical Function, and Cognitive Ability in Adults Aged Over 60: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2019; 16(5):753. https://doi.org/10.3390/ijerph16050753
Chicago/Turabian StyleZhou, Shengwen, Yanjie Zhang, Zhaowei Kong, Paul D. Loprinzi, Yang Hu, Jiajie Ye, Shijie Liu, Jane Jie Yu, and Liye Zou. 2019. "The Effects of Tai Chi on Markers of Atherosclerosis, Lower-limb Physical Function, and Cognitive Ability in Adults Aged Over 60: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 16, no. 5: 753. https://doi.org/10.3390/ijerph16050753