Empirical Analysis of the Status and Influencing Factors of Catastrophic Health Expenditure of Migrant Workers in Western China


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sites and Participants
2.2. Data Collection
2.3. Ethics Statement
2.4. Indicator Calculation
2.5. Statistical Methods
3. Results
3.1. General Situation
3.2. Univariable Analysis of Different Migrant Workers’ Family Characteristics
3.3. Multivariate Analysis of CHE of Migrant Workers’ Families
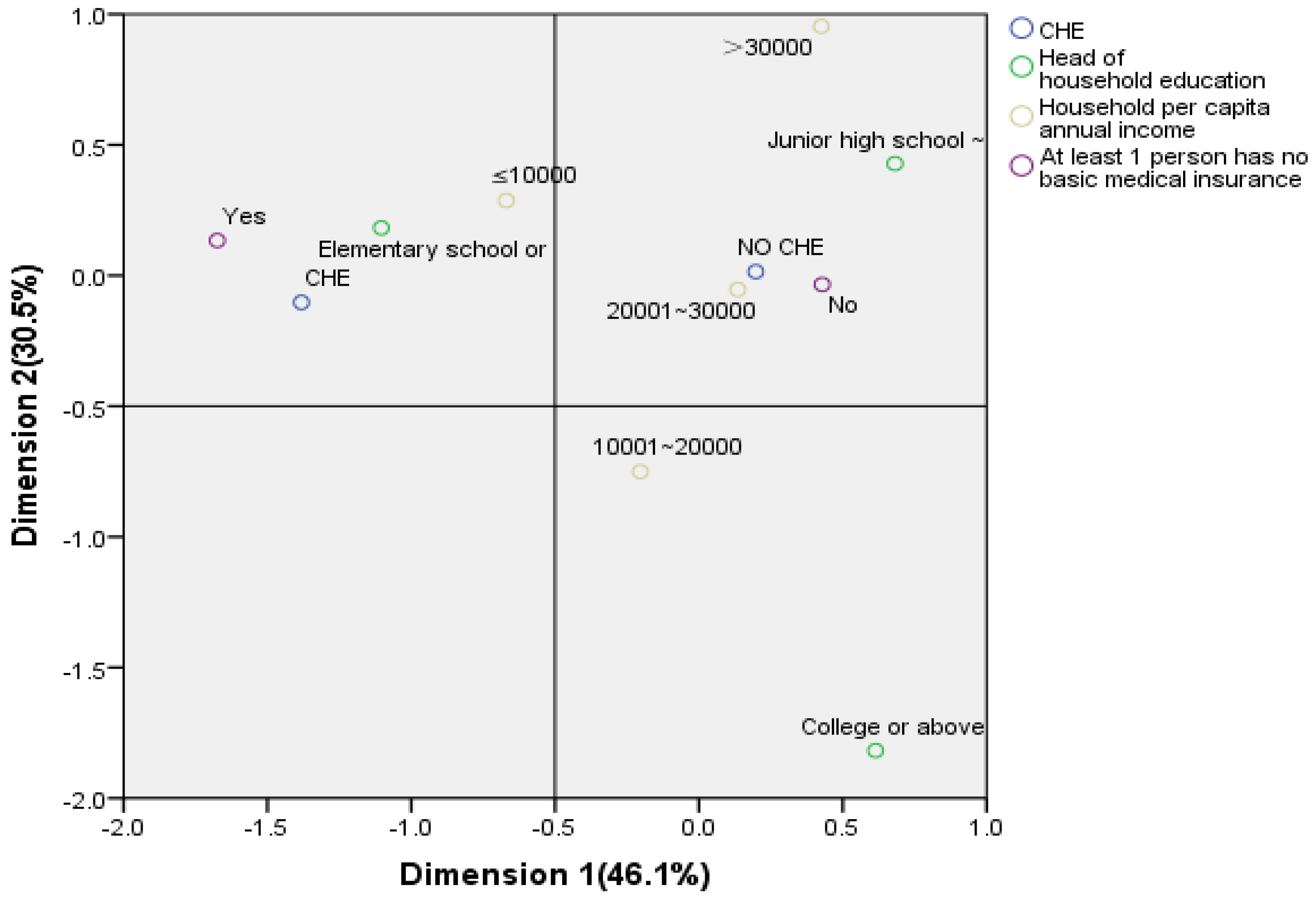
3.4. Multiple Correspondence Analysis between Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Heijink, R.; Xu, K.; Saksena, P.; Evans, D. Validity and Comparability of Out-of Pocket Health Expenditure from Household Surveys: A Review of the Literature and Current Survey Instruments; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Xu, K.; Evans, D.B.; Kawabata, K.; Zeramdini, R.; Klavus, J.; Murray, C.J. Household catastrophic health expenditure: A multicounty analysis. Lancet 2003, 362, 111–117. [Google Scholar] [CrossRef]
- Kawabata, K.; Xu, K.; Carrin, G. Preventing impoverishment through protection against catastrophic health expenditure. Bull. World Health Organ. 2002, 80, 612. [Google Scholar] [PubMed]
- Xu, K.; Evans, D.B.; Carrin, G.; Aguilar-Rivera, A.M.; Musgrove, P.; Evans, T. Protecting households from catastrophic health spending. Health Aff. 2007, 26, 972–983. [Google Scholar] [CrossRef] [PubMed]
- Tambor, M.; Pavlova, M.; Golinowska, S.; Sowada, C.; Groot, W. The formal–informal patient payment mix in European countries. Governance, economics, culture or all of these? Health Policy 2013, 113, 284–295. [Google Scholar] [CrossRef] [PubMed]
- Saksena, P.; Xu, K.; Durairaj, V. The Drivers of Catastrophic Expenditure: Outpatient Services, Hospitalization or Medicines; World Health Report; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Arsenijevic, J.; Pavlova, M.; Rechel, B.; Groot, W. Catastrophic HealthCare Expenditure among Older People with Chronic Diseases in 15 European Countries. PLoS ONE 2016, 11, e0157765. [Google Scholar] [CrossRef] [PubMed]
- National Bureau of Statistics. China Statistical Yearbook 2016; China Statistics Press: Beijing, China, 2016.
- Xu, K. Distribution of Health Payments and Catastrophic Expenditure Methodology; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Wang, Y.; Qiu, P.Y.; Tian, F. Catastrophic health expenditure and its influencing factors among rural families in Fushun county of Sichuan province. Chin. J. Public Health 2019, 1–4. Available online: http://kns.cnki.net/kcms/detail/21.1234.R.20180409.2102.024.html (accessed on 9 April 2018).
- Huang, S.S.; Yin, A.T. Household catastrophic health expenditure and its influencing factors among rural residents in Shangdong province. Chin. J. Public Health 2018, 34, 1221–1223. [Google Scholar]
- Huang, X.; Li, T.; Gu, X.; Wang, C.; Xiang, G. Empirical Analysis on the Status and Influencing Factors of Catastrophic Health Expenditure in Poor Urban Families. Chin. Health Econ. 2017, 36, 63–67. [Google Scholar]
- Yang, T.; Chu, J.; Zhou, C.; Medina, A.; Li, C.; Jiang, S.; Zheng, W.; Sun, L.; Liu, J. Catastrophic health expenditure: A comparative analysis of empty-nest and non-emptynest households with seniors in Shandong, China. BMJ Open 2016, 6, e010992. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Li, G. Study on catastrophic health expenditure of families with old people and its influencing factors. J. Shanghai Jiaotong Univ. (Med. Sci.) 2015, 35, 432–436. [Google Scholar]
- Wei, J.; Zhou, L.T. Discussing the Status of Medical Insurance System for Migrant Rural Workers and Its Mode Choice. Chin. Health Serv. Manag. 2010, 27, 31–33. [Google Scholar]
- Sirilak, S.; Okanurak, K.; Wattanagoon, Y.; Chatchaiyalerk, S.; Tornee, S.; Siri, S. Community participation of cross-border migrants for primary health care in Thailand. Health Policy Plan 2013, 28, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Castaneda, H.; Holmes, S.M.; Madrigal, D.S.; Young, M.E.D.; Beyeler, N.; Quesada, J. Immigration as a social determinant of health. Annu. Rev. Public Health 2015, 36, 375–392. [Google Scholar] [CrossRef] [PubMed]
- Malmus, D. Immigrants’ health and health inequality by type of integration policies in European countries. Eur. J. Public Health 2015, 25, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Nitika, A.L.; Nongkynrih, B.; Gupta, S.K. Migrants to urban India: Need for public health action. Indian J. Community Med. 2014, 399, 73–75. [Google Scholar]
- Li, J.; Chang, S.S.; Yip, P.S.F.; Li, J.; Jordan, L.P.; Tang, Y.G.; Hao, Y.T.; Huang, X.M.; Yang, N.; Chen, C.Q.; et al. Mental wellbeing amongst younger and older migrant workers in comparison to their urban counterparts in Guangzhou city, China: A crosssectional study. BMC Public Health 2014, 14, 1280. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.L. The Realistic Dilemma and Policy Analysis of the Citizenization of the New Generation Migrant Workers—Taking TaiYuan City as an Example. Econ. Trade 2019, 2, 19–21. [Google Scholar]
- Zhu, P.L.; Yang, Z.B. Multi-Dimensional Analysis on the Influence Factors of Migrant Workers’ Sense of Belonging. J. South China Agric. Univ. (Soc. Sci. Ed.) 2019, 1, 1–10. [Google Scholar]
- Liao, B.; Mao, X.; Liao, H. A Literature Review on Migrant Worker Citizenization under the Background of Urbanization. J. Xiangnan Univ. 2018, 39, 11–14. [Google Scholar]
- Boing, A.C.; Bertoldi, A.D.; de Barros, A.J.D.; Posenato, L.G.; Peres, K.G. Socioeconomic inequality in catastrophic health expenditure in Brazil. Rev. Saúde Pública 2014, 48, 632–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, K.; Evans, D.B.; Kadama, P.; Nabyonga, J.; Ogwal, P.O.; Nabukhonzo, P.; Aguilar, A.M. Understanding the impact of eliminating user fees. Utilization and catastrophic health expenditures in Uganda. Soc. Sci. Med. 2006, 62, 866–876. [Google Scholar] [CrossRef] [PubMed]
- Bakhtiar, P.; Ghobad, M.; Bijan, N.; Amjad, M.B. Hossein Safari. Catastrophic Health Expenditure After the Implementation of Health Sector Evolution Plan: A Case Study in the West of Iran. Int. J. Health Policy Manag. 2016, 5, 417–423. [Google Scholar]
- Zhang, W.T. Advanced Tutorial of SPSS Statistical Analysis; Higher Education Press: Beijing, China, 2004. [Google Scholar]
- Sourial, N.; Wolfson, C.; Zhu, B.; Quail, J.; Fletcher, J.; Karunananthan, S.; Bandeen-Roche, K.; Beland, F.; Bergman, H. Correspondence analysis is a useful tool to uncover the relationships among categorical variables. J. Clin. Epidemiol. 2010, 63, 638–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pei, H.B.; Wu, J.Q.; Zhou, Y. Multiple correspondence analysis of married women’s contraceptive methods related to their demographic characteristic. Chin. J. Health Stat. 2011, 5, 530–536. [Google Scholar]
- Li, B.H.; Dong, S.F.; Sun, Z.Q. An application of correspondence analysis method in the study of disease etiology. Chin. J. Epidemiol. 2007, 28, 914–917. [Google Scholar]
- Luo, S.; Ma, J.L.; Chen, J.W. The use of subgroup-correspondence analysis in epidemiology study. Chin. J. Health Stat. 2008, 25, 280–282. [Google Scholar]
- Wu, Q.H.; Li, Y.; Xu, L. Effect analysis on universal insurance coverage to reduce the incidence of catastrophic health expenditure in China. Chin. J. Health Policy 2012, 5, 62–66. [Google Scholar]
- Li, Y.; Wu, Q.H.; Gao, L.J. Analysis on causes of catastrophic health expenditure in rural China from perspective of system analysis. Chin. J. Health Policy 2012, 5, 55–59. [Google Scholar]
- Su, T.T.; Kouyaté, B.; Flessa, S. Catastrophic household expenditure for health care in a low-income society: A study from Nouna District, Burkina Faso. Bull. World Health Organ. 2006, 84, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Ekman, B. Catastrophic health payments and health insurance: Some counterintuitive evidence from one low-income country. Health Policy 2007, 83, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Woo, H.K.; Moon, O.R.; Park, J.H. The difference of health according to employment status and income level of wage-earners. Health Policy Manag. 2009, 19, 85–110. [Google Scholar] [CrossRef]
- Zhang, Q.; Li, W.; Li, Y.; Li, W.; Dong, X. Catastrophic health expenditure and related factors among rural inhabitants in Shenyang city. Chin. J. Public Health 2016, 32, 306–309. [Google Scholar]
- Kien, V.D.; Van Minh, H.; Giang, K.B.; Dao, A.; Tuan, L.T.; Ng, N. Socioeconomic inequalities in catastrophic health expenditure and impoverishment associated with non-communicable diseases in urban Hanoi, Vietnam. Int. J. Equity Health 2016, 15, 169. [Google Scholar] [CrossRef] [PubMed]
- Minh, H.V.; Phuong, N.T.K.; Saksena, P.; James, C.D.; Xu, K. Financial burden of household out-of pocket health expenditure in Viet Nam: Findings from the National Living Standard Survey 2002–2010. Soc. Sci. Med. 2013, 96, 258–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Wöhrmann, A.M.; Ler, J.; Wang, M. A mixed-method approach to postretirement career planning. J. Vocat. Behav. 2014, 84, 307–317. [Google Scholar] [CrossRef]
- Donghui, Z.; Wang, Z.; Yang, Z.; Jing, R.; Yang, J. Analysis on benefit level of rural under-five children in new cooperative medical scheme. Chin. Health Econ. 2012, 31, 33–35. [Google Scholar]
- Zhang, L.Y.; Cheng, X.M.; Tolhurst, R.; Tang, S.L.; Liu, X.Y. How effectively can the New Cooperative Medical Scheme reduce catastrophic health expenditure for the poor and non-poor in rural China? Trop. Med. Int. Health 2010, 15, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Kavosi, Z.; Keshtkaran, A.; Hayati, R.; Ravangard, R.; Khammarnia, M. Household financial contribution to the health System in Shiraz, Iran in 2012. Int. J. Health Policy Manag. 2014, 3, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Waters, H.R.; Anderson, G.F.; Mays, J. Measuring financial protection in health in the United States. Health Policy 2004, 69, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Thoa, N.T.; Thanh, N.X.; Chuc, N.T.; Lindholm, L. The impact of economic growth on health care utilization: A longitudinal study in rural Vietnam. Int. J. Equity Health 2013, 12, 19. [Google Scholar] [CrossRef] [PubMed]
- Kien, V.D.; Minh, H.V.; Ngoc, N.B.; Phuong, T.B.; Ngan, T.T.; Quam, M.B. Inequalities in Household Catastrophic Health Expenditure and Impoverishment Associated with Noncommunicable Diseases in Chi Linh, Hai Duong, Vietnam. Asia Pac. J. Public Health 2017, 29, 35S–44S. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Total (N = 1271) | CHE Households (N = 159) | χ2 | p Value |
|---|---|---|---|---|
| Family sizes (person) | 9.44 | 0.009 | ||
| 1–2 | 616 (48.5) | 60 (9.7) | ||
| 3–4 | 532 (41.9) | 77 (14.5) | ||
| ≥5 | 123 (9.7) | 22 (17.9) | ||
| Household per capita annual income (Yuan) | 24.96 | 0.000 | ||
| ≤10,000 | 141 (11.1) | 31 (22) | ||
| 10,001–20,000 | 464 (36.5) | 70 (15.1) | ||
| 20,001–30,000 | 325 (25.6) | 34 (10.5) | ||
| >30,000 | 341 (26.8) | 24 (7) | ||
| Head-of-household gender | 0.11 | 0.718 | ||
| Male | 735 (57.8) | 90 (12.2) | ||
| Female | 536 (42.2) | 69 (12.9) | ||
| Head-of-household age | 3.692 | 0.297 | ||
| ≤29 | 224 (17.6) | 20 (8.9) | ||
| 30–39 | 316 (24.9) | 40 (12.6) | ||
| 40–49 | 401 (31.5) | 53 (13.1) | ||
| ≥50 | 330 (26.0) | 47 (14.2) | ||
| Head-of-household education | 103.78 | 0.000 | ||
| Elementary school and below | 478 (37.6) | 67 (14) | ||
| Junior high school–high school | 603 (47.4) | 79 (13.1) | ||
| University and above | 190 (14.9) | 15 (7.9) | ||
| Elderly people over 65 years old | 15.18 | 0.000 | ||
| Yes | 252 (19.8) | 50 (19.9) | ||
| No | 1019 (80.2) | 108 (10.6) | ||
| Children under 5 years old | 13.09 | 0.000 | ||
| Yes | 78 (6.1) | 21 (27.1) | ||
| No | 1193 (93.9) | 138 (11.6) | ||
| At least 1 person has no basic medical insurance | 38.82 | 0.000 | ||
| Yes | 258 (20.3) | 62 (24) | ||
| No | 1013 (79.7) | 97 (9.5) | ||
| Chronically ill patients | 9.01 | 0.003 | ||
| Yes | 193 (15.2) | 37 (19.2) | ||
| No | 1078 (84.8) | 122 (11.3) | ||
| Hospitalized patients | 35.75 | 0.000 | ||
| Yes | 111 (8.7) | 34 (30.7) | ||
| No | 1160 (91.3) | 125 (10.8) |
| Variables | Reference Group | Wals χ2 | p Value | OR | 95% CI | |
|---|---|---|---|---|---|---|
| Family sizes (person) | 3–4 | 1–2 | 0.19 | 0.662 | 0.88 | 0.49–1.58 |
| ≥5 | 0.05 | 0.826 | 1.06 | 0.61–1.84 | ||
| Household per capita annual income (Yuan) | 20,001–30,000 | >30,000 | 2.42 | 0.120 | 1.54 | 0.89–2.67 |
| 10,001–20,000 | 11.80 | 0.001 | 2.35 | 1.44–3.82 | ||
| ≤10,000 | 20.05 | 0.000 | 3.72 | 2.09–6.62 | ||
| Head-of-household education | Junior high school–high school | University and above | 0.00 | 0.947 | 0.98 | 0.47–2.03 |
| Elementary school and below | 26.97 | 0.000 | 5.90 | 3.02–11.5 | ||
| Elderly people over 65 years old | Yes | No | 14.72 | 0.000 | 2.05 | 1.42–2.97 |
| Children under 5 years old | Yes | No | 12.26 | 0.000 | 2.61 | 1.53–4.48 |
| At least 1 person has no basic medical insurance | No | Yes | 36.31 | 0.000 | 2.96 | 2.08–4.23 |
| Chronically ill patients | Yes | No | 8.79 | 0.003 | 1.85 | 1.23–2.77 |
| Hospitalized patients | Yes | No | 32.13 | 0.000 | 3.61 | 2.31–5.62 |
| CHE | Household Per Capita Annual Income | Head-of-Household Education | Basic Medical Insurance |
|---|---|---|---|
| Head-of-household education | 11.22 ** | - | 39.65 ** |
| Basic medical insurance | 45.62 ** | 39.65 ** | - |
| CHE | 24.96 ** | 103.78 ** | 38.82 ** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, L.; Zhang, X.; Zhao, L.; Li, N. Empirical Analysis of the Status and Influencing Factors of Catastrophic Health Expenditure of Migrant Workers in Western China. Int. J. Environ. Res. Public Health 2019, 16, 738. https://doi.org/10.3390/ijerph16050738
Liu L, Zhang X, Zhao L, Li N. Empirical Analysis of the Status and Influencing Factors of Catastrophic Health Expenditure of Migrant Workers in Western China. International Journal of Environmental Research and Public Health. 2019; 16(5):738. https://doi.org/10.3390/ijerph16050738
Chicago/Turabian StyleLiu, Li, Xuewen Zhang, Longchao Zhao, and Ningxiu Li. 2019. "Empirical Analysis of the Status and Influencing Factors of Catastrophic Health Expenditure of Migrant Workers in Western China" International Journal of Environmental Research and Public Health 16, no. 5: 738. https://doi.org/10.3390/ijerph16050738