Is a One Health Approach Utilized for Q Fever Control? A Comprehensive Literature Review


Abstract
:
1. Introduction
2. Materials and Methods
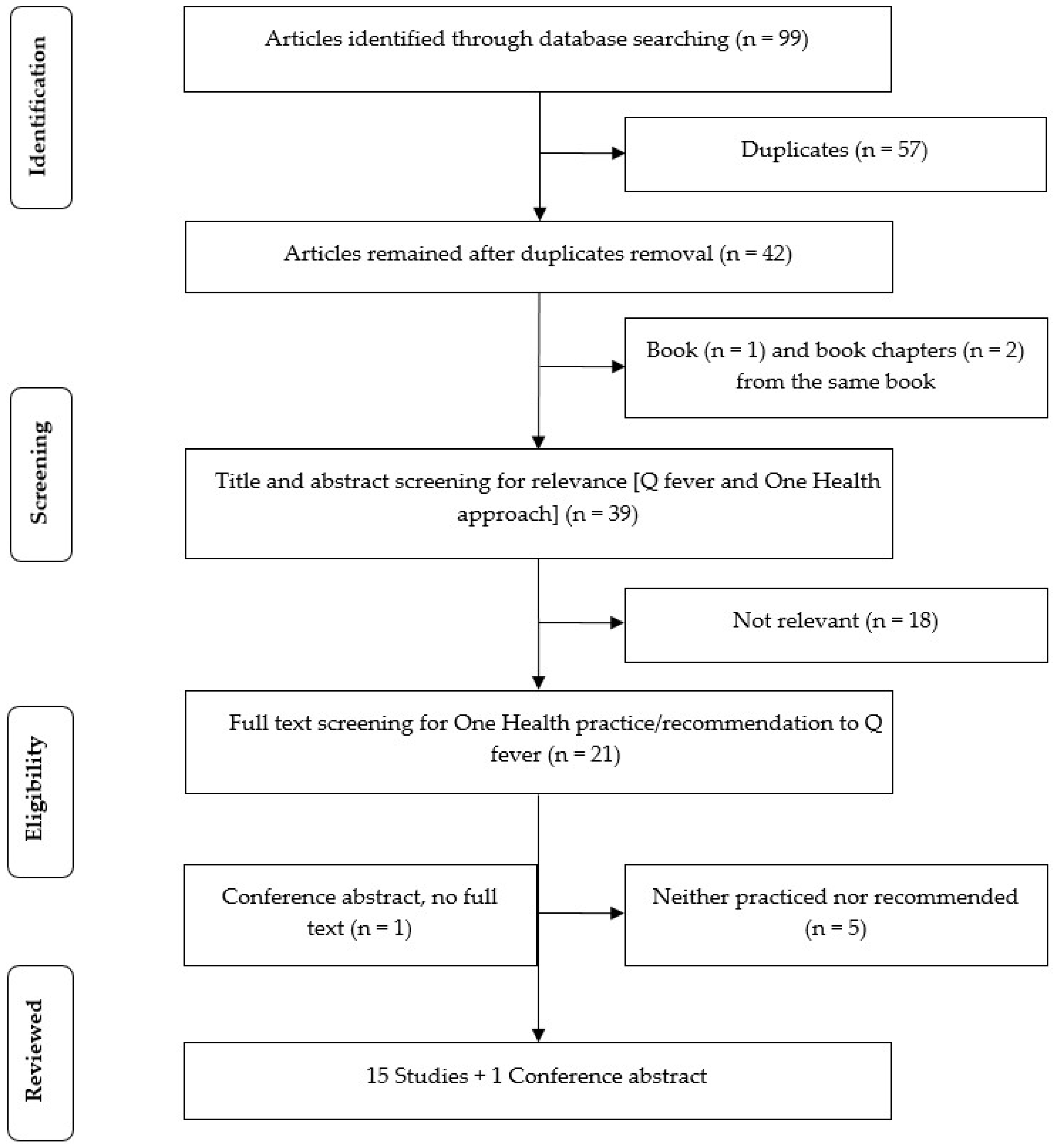
2.1. Search Strategy
2.2. Eligibility Criteria
- Studies that described the practice of one or more components of One Health in Q fever prevention and control;
- Studies that did not practice but recommended a One Health approach to Q fever prevention and control.
2.3. One Health Practice, Recommendation, and Observed and Expected Outcomes
3. Results
3.1. Q Fever Risks to Humans
3.2. Human and Animal Serology
3.2.1. Human
3.2.2. Animal
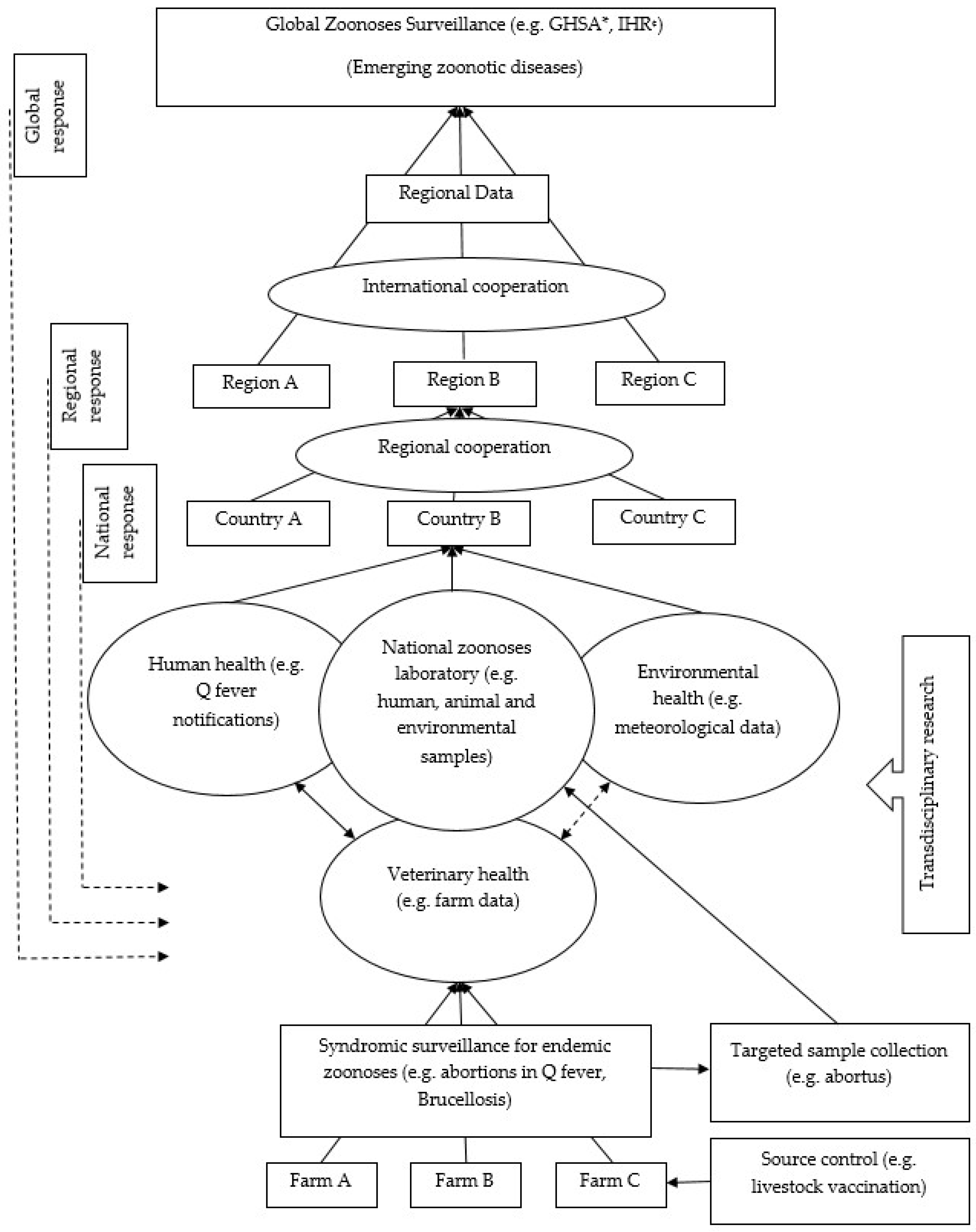
3.3. Integrated Q Fever Surveillance
3.4. Vaccination
3.5. Environmental Management
3.6. Multi-Sectoral Collaboration Including Joint Research
3.6.1. Policy and Practice Guideline Development
3.6.2. Information Sharing and Intelligence Exchange
3.6.3. Risk Communication
3.6.4. Joint Intervention
3.6.5. Evaluation
3.7. Education and Training Including Community Engagement
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Terheggen, U.; Leggat, P.A. Clinical manifestations of Q fever in adults and children. Travel Med. Infect. Dis. 2007, 5, 159–164. [Google Scholar] [CrossRef] [PubMed]
- McQuiston, J.H.; Childs, J.E. Q fever in humans and animals in the United States. Vector Borne Zoonotic Dis. 2002, 2, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Australian Government, Department of Health. National Notifiable Diseases Surveillance System. Available online: http://www9.health.gov.au/cda/source/cda-index.cfm (accessed on 20 February 2019).
- Anderson, A.; Bijlmer, H.; Fournier, P.E.; Graves, S.; Hartzell, J.; Kersh, G.J.; Limonard, G.; Marrie, T.J.; Massung, R.F.; McQuiston, J.H.; et al. Diagnosis and Management of Q Fever—United States, 2013: Recommendations from CDC and the Q Fever Working Group; CDC—National Center for Emerging and Zoonotic Infectious Diseases: Atlanta, GA, USA, 2013; pp. 1–28. [Google Scholar]
- Burke, R.L.; Kronmann, K.C.; Daniels, C.C.; Meyers, M.; Byarugaba, D.K.; Dueger, E.; Klein, T.A.; Evans, B.P.; Vest, K.G. A review of zoonotic disease surveillance supported by the armed forces health surveillance center. Zoonoses Public Health 2012, 59, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Van Asseldonk, M.A.P.M.; Bontje, D.M.; Backer, J.A.; van Roermund, H.J.W.; Bergevoet, R.H.M. Economic aspects of Q fever control in dairy goats. Prev. Vet. Med. 2015, 121, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Palmer, C.; McCall, B.; Jarvinen, K.; Krause, M.; Heel, K. “The dust hasn’t settled yet”: The national Q fever management program, missed opportunities for vaccination and community exposures. Aust. N. Z. J. Public Health 2007, 31, 330–332. [Google Scholar] [CrossRef] [PubMed]
- Kermode, M.; Yong, K.; Hurley, S.; Marmion, B. An economic evaluation of increased uptake in Q fever vaccination among meat and agricultural industry workers following implementation of the national Q fever management program. Aust. N. Z. J. Public Health 2003, 27, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Lower, T.; Corben, P.; Massey, P.; Depczynski, J.; Brown, T.; Stanley, P.; Osbourn, M.; Durrheim, D. Farmers’ knowledge of Q fever and prevention approaches in New South Wales. Aust. J. Rural Health 2017, 25, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Garner, M.G.; Longbottom, H.M.; Cannon, R.M.; Plant, A.J. A review of Q fever in Australia 1991–1994. Aust. N. Z. J. Public Health 1997, 21, 722–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dantas-Torres, F.; Chomel, B.B.; Otranto, D. Ticks and tick-borne diseases: A one health perspective. Trends Parasitol. 2012, 28, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Whitney, E.A.S.; Massung, R.F.; Candee, A.J.; Ailes, E.C.; Myers, L.M.; Patterson, N.E.; Berkelman, R.L. Seroepidemiologic and occupational risk survey for Coxiella burnetii antibodies among United States veterinarians. Clin. Infect. Dis. 2009, 48, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Noah, D.L.; Noah, D.L.; Crowder, H.R. Biological terrorism against animals and humans: A brief review and primer for action. J. Am. Vet. Med. Assoc. 2002, 221, 40–43. [Google Scholar] [CrossRef] [PubMed]
- CDC—National Center for Emerging and Zoonotic Infectious Diseases. One Health. Available online: https://www.cdc.gov/onehealth/index.html (accessed on 15 August 2018).
- Dorko, E.; Rimarova, K.; Pilipcinec, E. Influence of the environment and occupational exposure on the occurrence of Q fever. Cent. Eur. J. Public Health 2012, 20, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Simpson, G.J.G.; Quan, V.; Frean, J.; Knobel, D.L.; Rossouw, J.; Weyer, J.; Marcotty, T.; Godfroid, J.; Blumberg, L.H. Prevalence of selected zoonotic diseases and risk factors at a human-wildlife-livestock interface in Mpumalanga province, South Africa. Vector Borne Zoonotic Dis. 2018, 18, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Mori, M.; Roest, H.J. Farming, Q fever and public health: Agricultural practices and beyond. Arch. Public Health 2018, 76, 2. [Google Scholar] [CrossRef] [PubMed]
- Kanoute, Y.B.; Gragnon, B.G.; Schindler, C.; Bonfoh, B.; Schelling, E. Epidemiology of brucellosis, Q fever and rift valley fever at the human and livestock interface in northern Cote d’Ivoire. Acta Trop. 2017, 165, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Cleaveland, S.; Sharp, J.; Abela-Ridder, B.; Allan, K.J.; Buza, J.; Crump, J.A.; Davis, A.; Vilas, V.J.D.; de Glanville, W.A.; Kazwala, R.R.; et al. One health contributions towards more effective and equitable approaches to health in low- and middle-income countries. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2017, 372. [Google Scholar] [CrossRef] [PubMed]
- Candela, M.G.; Caballol, A.; Atance, P.M. Wide exposure to Coxiella burnetii in ruminant and feline species living in a natural environment: Zoonoses in a human-livestock-wildlife interface. Epidemiol. Infect. 2017, 145, 478–481. [Google Scholar] [CrossRef] [PubMed]
- Wardrop, N.A.; Thomas, L.F.; Cook, E.A.; de Glanville, W.A.; Atkinson, P.M.; Wamae, C.N.; Fevre, E.M. The sero-epidemiology of Coxiella burnetii in humans and cattle, western Kenya: Evidence from a cross-sectional study. PLoS Negl. Trop. Dis. 2016, 10, e0005032. [Google Scholar] [CrossRef] [PubMed]
- Van Leuken, J.P.G.; Swart, A.N.; Brandsma, J.; Terink, W.; Van de Kassteele, J.; Droogers, P.; Sauter, F.; Havelaar, A.H.; Van der Hoek, W. Human Q fever incidence is associated to spatiotemporal environmental conditions. One Health 2016, 2, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ndeereh, D.; Muchemi, G.; Thaiyah, A. Knowledge, attitudes and practices towards spotted fever group rickettsioses and Q fever in Laikipia and Maasai Mara, Kenya. J. Public Health Afr. 2016, 7, 545. [Google Scholar] [CrossRef] [PubMed]
- Bond, K.A.; Vincent, G.; Wilks, C.R.; Franklin, L.; Sutton, B.; Stenos, J.; Cowan, R.; Lim, K.; Athan, E.; Harris, O.; et al. One health approach to controlling a Q fever outbreak on an Australian goat farm. Epidemiol. Infect. 2016, 144, 1129–1141. [Google Scholar] [CrossRef] [PubMed]
- Ladbury, G.A.F.; Van Leuken, J.P.G.; Swart, A.; Vellema, P.; Schimmer, B.; Ter Schegget, R.; Van der Hoek, W. Integrating interdisciplinary methodologies for one health: Goat farm re-implicated as the probable source of an urban Q fever outbreak, the Netherlands, 2009. BMC Infect. Dis. 2015, 15, 372. [Google Scholar] [CrossRef] [PubMed]
- Halliday, J.E.B.; Allan, K.J.; Ekwem, D.; Cleaveland, S.; Kazwala, R.R.; Crump, J.A. Endemic zoonoses in the tropics: A public health problem hiding in plain sight. Vet. Rec. 2015, 176, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Burniston, S.; Okello, A.L.; Khamlome, B.; Inthavong, P.; Gilbert, J.; Blacksell, S.D.; Allen, J.; Welburn, S.C. Cultural drivers and health-seeking behaviours that impact on the transmission of pig-associated zoonoses in Lao People’s Democratic Republic. Infect. Dis. Poverty 2015, 4, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greter, H.; Jean-Richard, V.; Crump, L.; Béchir, M.; Alfaroukh, I.O.; Schelling, E.; Bonfoh, B.; Zinsstag, J. The benefits of ‘one health’ for pastoralists in Africa. Onderstepoort J. Vet. Res. 2014, 81, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Biggs, H.M.; Turabelidze, G.; Todd, S.R.; Slifka, K.J.; Drexler, N.A.; Pratt, D.; McCurdy, G.; Lloyd, J.K.; Kato, C.Y.; Sun, D.; et al. Q fever outbreak on a large United States Goat and cattle dairy: A one health investigation. In 63rd Annual Meeting; American Society of Tropical Medicine and Hygiene: New Orleans, LA, USA, 2014; Volume 91, p. 199. [Google Scholar]
- Biggs, H.M.; Turabelidze, G.; Pratt, D.; Todd, S.R.; Jacobs-Slifka, K.; Drexler, N.A.; McCurdy, G.; Lloyd, J.; Evavold, C.L.; Fitzpatrick, K.A.; et al. Coxiella burnetii infection in a community operating a large-scale cow and goat dairy, Missouri, 2013. Am. J. Trop. Med. Hyg. 2016, 94, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Enserink, M. Humans, animals—it’s one health. Or is it? Science 2010, 327, 266–267. [Google Scholar] [CrossRef] [PubMed]
- Dunne, G.; Gurfield, N. Local veterinary diagnostic laboratory, a model for the one health initiative. Vet. Clin. North Am. Small Anim. Pract. 2009, 39, 373–384. [Google Scholar] [CrossRef] [PubMed]
- Gubernot, D.M.; Boyer, B.L.; Moses, M.S. Animals as early detectors of bioevents: Veterinary tools and a framework for animal-human integrated zoonotic disease surveillance. Public Health Rep. 2008, 123, 300–315. [Google Scholar] [CrossRef] [PubMed]
- Rodolakis, A. Zoonoses in goats: How to control them. Small Rumin. Res. 2014, 121, 12–20. [Google Scholar] [CrossRef]
- Van der Hoek, W.; Morroy, G.; Renders, N.H.; Wever, P.C.; Hermans, M.H.; Leenders, A.C.A.P.; Schneeberger, P.M. Epidemic Q fever in humans in the Netherlands. In Coxiella Burnetii: Recent Advances and New Perspectives in Research of the Q Fever Bacterium; Toman, R., Heinzen, R.A., Samuel, J.E., Mege, J.-L., Eds.; Springer: Dordrecht, The Netherlands, 2012; Volume 984, pp. 329–364. [Google Scholar]
- Australian Government. The Australian Immunisation Handbook, 10th ed.; Commonwealth of Australia: Canberra, Australia, 2015; pp. 355–362.
- Van Holland, B.J.; Soer, R.; de Boer, M.R.; Reneman, M.F.; Brouwer, S. Preventive occupational health interventions in the meat processing industry in upper-middle and high-income countries: A systematic review on their effectiveness. Int. Arch. Occup. Environ. Health 2015, 88, 389–402. [Google Scholar] [CrossRef] [PubMed]
- Gefenaite, G.; Munster, J.M.; van Houdt, R.; Hak, E. Effectiveness of the Q fever vaccine: A meta-analysis. Vaccine 2011, 29, 395–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marmion, B.P.; Ormsbee, R.A.; Kyrkou, M.; Wright, J.; Worswick, D.A.; Izzo, A.A.; Esterman, A.; Feery, B.; Shapiro, R.A. Vaccine prophylaxis of abattoir-associated Q fever: Eight years’ experience in Australian abattoirs. Epidemiol. Infect. 1990, 104, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Milazzo, A.; Featherstone, K.B.; Hall, R.G. Q fever vaccine uptake in South Australian meat processors prior to the introduction of the national Q fever management program. Commun. Dis. Intell. 2005, 29, 400–406. [Google Scholar]
- Schimmer, B.; Lenferink, A.; Schneeberger, P.; Aangenend, H.; Vellema, P.; Hautvast, J.; van Duynhoven, Y. Seroprevalence and risk factors for Coxiella burnetii (Q fever) seropositivity in dairy goat farmers’ households in the Netherlands, 2009–2010. PLoS ONE 2012, 7, e42364. [Google Scholar] [CrossRef] [PubMed]
- NASPHV. Compendium of Measures to Prevent Disease Associated with Animals in Public Settings, 2009: National Association of State Public Health Veterinarians, Inc. (NASPHV); RR-5; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2009; pp. 1–21. [Google Scholar]
- Cosic, G.; Djekic, J.; Duric, P.; Seguljev, Z.; Petrovic, M.; Rajcevic, S. Epidemiological characteristics of Q fever in Vojvodina province, Serbia, from 1985 to 2009. Arch. Biol. Sci. 2012, 64, 1363–1368. [Google Scholar] [CrossRef]
- Chiu, C.K.; Durrheim, D.N. A review of the efficacy of human Q fever vaccine registered in Australia. N. S. W. Public Health Bull. 2007, 18, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Ganter, M. Zoonotic risks from small ruminants. Vet. Microbiol. 2015, 181, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Graves, S.; Stenos, J. Rickettsioses in Australia. Ann. N. Y. Acad. Sci. 2009, 1166, 151–155. [Google Scholar] [CrossRef] [PubMed]
- CDC—Program Performance and Evaluation Office. Introduction to Program Evaluation for Public Health Programs: A Self-Study Guide. Available online: https://www.cdc.gov/eval/guide/index.htm (accessed on 10 August 2018).
- Lai, C.H.; Sun, W.; Lee, C.H.; Lin, J.N.; Liao, M.H.; Liu, S.S.; Chang, T.Y.; Tsai, K.F.; Chang, Y.C.; Lin, H.H.; et al. The epidemiology and characteristics of Q fever and co-infections with scrub typhus, murine typhus or leptospirosis in Taiwan: A nationwide database study. Zoonoses Public Health 2017, 64, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Ralph, A.; Markey, P.; Schultz, R. Q fever cases in the Northern Territory of Australia from 1991 to 2006. Commun. Dis. Intell. 2007, 31, 222–227. [Google Scholar]
- Sloan-Gardner, T.S.; Massey, P.D.; Hutchinson, P.; Knope, K.; Fearnley, E. Trends and risk factors for human Q fever in Australia, 1991–2014. Epidemiol. Infect. 2017, 145, 787–795. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study and Location | Study Type | One Health | Observed and/or Expected Outcomes | Comments |
|---|---|---|---|---|
| [16] South Africa | Cross-sectional | Practiced | ||
|
|
| ||
|
|
| ||
| Recommended | ||||
|
| |||
| [17] Europe/Belgium | Systematic review | Practiced | ||
|
|
| ||
| Recommended | ||||
|
| |||
| ||||
| [18] Côte d’Ivoire | Cross-sectional | Practiced | ||
|
|
| ||
| ||||
| Recommended | ||||
|
| |||
| [19] Africa/Tanzania | Review | Recommended | ||
|
|
| ||
|
| |||
|
| |||
|
| |||
| [20] Spain | Cross-sectional | Practiced | ||
|
|
| ||
| Recommended | ||||
|
| |||
| [21] Kenya | Cross-sectional | Practiced | ||
|
|
| ||
|
| |||
|
| |||
| Recommended | ||||
|
| |||
| [22] Netherlands | Ecological correlation | Practiced | ||
|
|
| ||
| Recommended | ||||
|
| |||
| [23] Kenya | Cross-sectional | Practiced | ||
|
|
| ||
| Recommended | ||||
|
| |||
| ||||
|
| |||
| [24] Australia | Outbreak investigation | Practiced | ||
|
|
| ||
|
| |||
|
| |||
|
| |||
| ||||
| ||||
| ||||
| Recommended | ||||
|
| |||
|
| |||
|
| |||
|
| |||
| [25] Netherlands | Ecological correlation | Practiced | ||
|
|
| ||
|
| |||
|
| |||
| Recommended | ||||
|
| |||
| ||||
| [26] Africa/Tanzania | Feature/Review | Recommended | ||
|
|
| ||
|
| |||
|
| |||
| [27] Lao People’s Democratic Republic (Laos) | Review | Practiced | ||
|
|
| ||
| Recommended | ||||
|
| |||
| ||||
|
| |||
| [28] Africa/Chad | Conference proceedings/Review | Practiced | ||
|
|
| ||
| Recommended | ||||
|
| |||
|
| |||
| [29] USA | Outbreak investigation | Practiced | ||
|
|
| ||
|
| |||
|
| |||
| Recommended | ||||
|
| |||
| [31] Netherlands | Review | Recommended | ||
|
|
| ||
|
| |||
|
| |||
| [32] USA | Review | Practiced | ||
|
|
| ||
| ||||
|
| |||
|
| |||
| ||||
|
| |||
| Recommended | ||||
|
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahaman, M.R.; Milazzo, A.; Marshall, H.; Bi, P. Is a One Health Approach Utilized for Q Fever Control? A Comprehensive Literature Review. Int. J. Environ. Res. Public Health 2019, 16, 730. https://doi.org/10.3390/ijerph16050730
Rahaman MR, Milazzo A, Marshall H, Bi P. Is a One Health Approach Utilized for Q Fever Control? A Comprehensive Literature Review. International Journal of Environmental Research and Public Health. 2019; 16(5):730. https://doi.org/10.3390/ijerph16050730
Chicago/Turabian StyleRahaman, Md Rezanur, Adriana Milazzo, Helen Marshall, and Peng Bi. 2019. "Is a One Health Approach Utilized for Q Fever Control? A Comprehensive Literature Review" International Journal of Environmental Research and Public Health 16, no. 5: 730. https://doi.org/10.3390/ijerph16050730
APA StyleRahaman, M. R., Milazzo, A., Marshall, H., & Bi, P. (2019). Is a One Health Approach Utilized for Q Fever Control? A Comprehensive Literature Review. International Journal of Environmental Research and Public Health, 16(5), 730. https://doi.org/10.3390/ijerph16050730