Internet-Delivered Cognitive Behavior Therapy for Young Taiwanese Female Nursing Students with Irritable Bowel Syndrome—A Cluster Randomized Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Eligibility criteria
2.2. Design and Procedure
2.3. Measures
2.4. Intervention
2.5. Analysis
3. Results
3.1. Characteristics of Participants
3.2. Results on Outcome Measures
4. Discussion
Study Limitations
5. Conclusion
Author Contributions
Funding
Conflicts of Interest
References
- Agrawal, A.; Whorwell, P.J. Irritable bowel syndrome: Diagnosis and management. BMJ Learn. 2006, 332, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Drossma, D.A. Functional gastrointestinal disorders: history, pathophysiology, clinical features and Rome IV. Gastroenterology 2016. [Google Scholar] [CrossRef] [PubMed]
- Chang, F.Y.; Lu, C.L. The clinical significances of irritable bowel syndrome in Taiwan. J. Gastroenterol. Hepatol. 2011, 26, 102–105. [Google Scholar] [CrossRef] [PubMed]
- Canavan, C.; West, J.; Card, T. The epidemiology of irritable bowel syndrome. Clin. Epidemiol. 2014, 6, 71–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heitkemper, M.M.; Jarrett, M.E.; Levy, R.L.; Cain, K.C.; Burr, R.L.; Feld, A.; Barney, P.; Weisman, P. Self-management for women with irritable bowel syndrome. Clin. Gastroenterol. Hepatol. 2004, 2, 585–596. [Google Scholar] [CrossRef]
- Lu, C.L.; Chen, C.Y.; Lang, H.C.; Luo, J.C.; Wang, S.S.; Chang, F.Y.; Lee, S.D. Current patterns of irritable bowel syndrome in Taiwan: The Rome II Questionnaire on a Chinese population. Aliment Pharmacol. Ther. 2003, 18, 1159–1169. [Google Scholar] [CrossRef] [PubMed]
- Weaver, K.R.; Melkus, G.D.; Henderson, W.A. Irritable Bowel Syndrome An evidence-based review of new diagnostic criteria and treatment recommendations. AJN 2017, 117, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.C.; Moayyedi, P.; Lacy, B.E.; Lembo, A.J.; Saito, Y.A.; Schiller, L.R.; Soffer, E.E.; Spiegel, B.M.R.; Quigley, E.M.M. American College of Gastroenterology Monograph on the Management of Irritable Bowel Syndrome and Chronic Idiopathic Constipation. Am. J. Gastroenterol. 2014, 109, S2–S26. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, E.B.; Lackner, J.M.; Jaccard, J.; Rowell, D.; Carosella, A.M.; Powell, C.; Sanders, K.; Krasner, S.; Kuhn, E. The role of stress in symptom exacerbation among IBS patients. J. Psychosom. Res. 2008, 64, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Drossman, D.A. The functional gastrointestinal disorders and the Rome III process. Gastroenterology 2006, 130, 1377–1390. [Google Scholar] [CrossRef] [PubMed]
- Fond, G.; Loundou, A.; Hamdani, N.; Boukouaci, W.; Dargel, A.; Oliveira, J.; Roger, M.; Tamouza, R.; Leboyer, M.; Boyer, L. Anxiety and depression comorbidities in irritable bowel syndrome (IBS): A systematic review and meta-analysis. Eur. Arch. Psychiatry Clin. Neurosci. 2014, 264, 651–660. [Google Scholar] [CrossRef] [PubMed]
- Spiller, R.; Aziz, Q.; Creed, F.; Emmanuel, A.; Houghton, L.; Hungin, P.; Jones, R.; Kumar, D.; Rubin, G.; Trudgill, N.; et al. Guidelines on the irritable bowel syndrome: Mechanisms and practical management. Gut 2007, 56, 1770–1798. [Google Scholar] [CrossRef] [PubMed]
- Herting, V.L.; Cain, K.C.; Jarrett, M.E.; Burr, M.E.; Heitkemper, M.M. Daily stress and gastrointestinal symptoms in women with irritable bowel syndrome. Nurs. Res. 2007, 56, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.A.; Locke, G.R., 3rd; Weaver, A.L.; Zinsmeister, A.R.; Talley, N.J. Diet and functional gastrointestinal disorders: A population-based case-control study. Am. J. Gastroenterol. 2005, 100, 2743–2748. [Google Scholar] [CrossRef] [PubMed]
- Zijdenbos, I.L.; de Wit, N.J.; van der Heijden, G.J.; Rubin, G.; Quartero, A.O. Psychological treatments for the management of irritable bowel syndrome. Cochrane Database Syst. Rev. 2009, 21. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.C.; Quigley, E.M.; Lacy, B.E.; Lembo, A.J.; Saito, Y.A.; Schiller, L.R.; Soffer, E.E.; Moayyedi, P.; Spiegel, B.M. Effect of antidepressants and psychological therapies, including hypnotherapy, in irritable bowel syndrome: systematic review and meta-analysis. Am. J. Gastroenterol. 2014, 109, 1350–1365. [Google Scholar] [CrossRef] [PubMed]
- Boyce, P.M.; Talley, N.J.; Balaam, B.; Koloski, N.A.; Truman, G.A. Randomized Controlled Trial of Cognitive Behavior Therapy, Relaxation Training, and Routine Clinical Care for the Irritable Bowel Syndrome. Am. J. Gastroenterol. 2003, 98, 2009–2218. [Google Scholar] [CrossRef] [PubMed]
- Laird, K.T.; Tanner-Smith, E.E.; Russell, A.C.; Hollon, S.D.; Walker, L.S. Comparative efficacy of psychological therapies for improving mental health and daily functioning in irritable bowel syndrome: A systematic review and meta-analysis. Clin. Psychol. Rev. 2017, 51, 142–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Xiong, L.; Zhang, S.; Yu, Q.; Chen, M. Cognitive–behavioral therapy for irritable bowel syndrome: A meta-analysis. J. Psychosom. Res. 2014, 77, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hedman, E.; Ljótsson, B.; Lindefors, N. Cognitive behavior therapy via the Internet: A systematic review of applications, clinical efficacy and cost–effectiveness. Expert Rev. Pharmacoecon. Outcomes Res. 2012, 12, 745–764. [Google Scholar] [CrossRef] [PubMed]
- Andersson, G. Internet interventions: Past, present and future. Internet Interv. 2018, 12, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Oerlemans, S.; van Cranenburgh, O.; Herremans, P.J.; Spreeuwenberg, P.; van Dulmen, S. Intervening on cognitions and behavior in irritable bowel syndrome: A feasibility trial using PDAs. J. Psychosom. Res. 2011, 70, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Vigerland, S.; Lenhard, F.; Bonnert, M.; Lalouni, M.; Hedman, E.; Ahlen, J.; Olén, O.; Serlachius, E.; Ljótsson, B. Internet-delivered cognitive behavior therapy for children and adolescents: A systematic review and meta-analysis. Clin. Psychol. Rev. 2016, 50, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laird, K.T.; Tanner-Smith, E.E.; Russell, A.C.; Hollon, S.D.; Walker, L.S. Short-term and long-term efficacy of psychological therapies for irritable bowel syndrome: A systematic review and meta-analysis. Clin Gastroenterol. Hepatol. 2016, 14, 937–947. [Google Scholar] [CrossRef] [PubMed]
- Halpert, A.; Rybin, D.; Doros, G. Expressive writing is a promising therapeutic modality for the management of IBS: A pilot study. Am. J. Gastroenterol. 2010, 105, 2440–2448. [Google Scholar] [CrossRef] [PubMed]
- Pennebaker, J.W.; Chung, C.K. Expressive writing and its links to mental and physical health. In Oxford Handbook of Health Psychology; Friedman, H.S., Ed.; Oxford University: New York, NY, USA, 2011; pp. 417–437. [Google Scholar]
- Reinhold, M.; Bürkner, P.C.; Holling, H. Effects of expressive writing on depressive symptoms—A meta-analysis. Clin. Psychol. Sci. Pract. 2018, 25, 1–13. [Google Scholar] [CrossRef]
- Pulido-Martos, M.; Augusto-Landa, J.M.; Lopez-Zafra, E. Sources of stress in nursing students: A systematic review of quantitative studies. Int. Nurs. Rev. 2011, 59, 15–25. [Google Scholar] [CrossRef]
- Lee, T.Y.; Tsai, C.H. Risk factors and self-management skills of irritable bowel syndrome in nursing students: A school-base study. J. Tzu Chi Coll. Technol. 2013, 21, 33–47. [Google Scholar]
- Longstreth, G.F.; Thompson, W.G.; Chey, W.D.; Houghton, L.A.; Mearin, F.; Spiller, R.C. Functional bowel disorders. Gastroenterology 2006, 130, 1480–1491. [Google Scholar] [CrossRef] [PubMed]
- Boyce, P.; Gilchrist, J.; Talley, N.J.; Rose, D. Cognitive-behaviour therapy as a treatmentfor irritable bowel syndrome: A pilot study. Aust. N. Z. J. Psychiatry 2000, 34, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Brislin, R.W. Back-Translation for Cross-Cultural Research. J. Cross-Cult. Psychol. 1970, 1, 185–216. [Google Scholar] [CrossRef]
- Zhong, S.C.; Long, C.F. Revision of the Situation and Trait Anxiety Scale. Annu. Rep. 1984, 31, 27–36. [Google Scholar]
- Spielberger, C.D.; Gorsuch, R.C.; Lushene, R.E.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists: Palo Alto, CA, USA, 1983. [Google Scholar]
- Chien, C.P.; Cheng, T.A. Depression in Taiwan: epidemiological survey utilizing CES-D. Seishin Shinkeigaku Zasshi 1985, 87, 335–338. [Google Scholar] [PubMed]
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Greenberger, D.; Padesky, C.A. Mind over Mood: Change How You Feel by Changing the Way You Think; Guilford Press: New York, NY, USA, 1996. [Google Scholar]
- Julian, L.J. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A). Arthritis Care Res. (Hoboken) 2011, 63, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.C.; Lacy, B.E.; Harris, L.A.; Quigley, E.M.M.; Moayyedi, P. Effect of Antidepressants and Psychological Therapies in Irritable Bowel Syndrome: An Updated Systematic Review and Meta-analysis. Am. J. Gastroenterol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Bonnert, M.; Ljótsson, B.; Hedman, E.; Andersson, J.; Arnell, H.; Benninga, M.A.; Simrén, M.; Thulin, H.; Thulin, U.; Vigerland, S.; et al. Internet-delivered cognitive behavior therapy for adolescents with functional gastrointestinal disorders—An open trial. Internet Interv. 2014, 1, 141–148. [Google Scholar] [CrossRef]
- Ljótsson, B.; Hedman, E.; Andersson, E.; Hesser, H.; Lindfors, P.; Hursti, T.; Rydh, S.; Rück, C.; Lindefors, N.; Andersson, G. Internet-delivered exposure-based treatment vs. stress management for irritable bowel syndrome: A randomized trial. Am. J. Gastroenterol. 2011, 106, 1481–1491. [Google Scholar] [CrossRef] [PubMed]
- Van Dessel, N.; Den Boeft, M.; van der Wouden, J.C.; Kleinstäuber, M.; Leone, S.S.; Terluin, B.; Numans, M.E.; van der Horst, H.E.; van Marwijk, H. Non-pharmacological interventions for somatoform disorders and medically-unexplained physical symptoms (MUPS) in adults. Cochrane Database Syst. Rev. 2014, 1, CD011142. [Google Scholar] [CrossRef]
- Bennett, E.J.; Piesse, C.; Palmer, K.; Badcock, C.A.; Tennant, C.C.; Kellow, J.E. Functional gastrointestinal disorders: Psychological, social, and somatic features. Gut 1998, 42, 414–420. [Google Scholar] [CrossRef]
- Drossman, D.A.; Camilleri, M.; Mayer, E.A.; Whitehead, W.E. AGA technical review on irritable bowel syndrome. Gastroenterology 2002, 123, 2108–2131. [Google Scholar] [CrossRef] [PubMed]
- Sykes, M.A.; Blanchard, E.B.; Lackner, J.; Keefer, L.; Krasner, S. Psychopathology in irritable bowel syndrome: Support for a psychophysiological model. J. Behav. Med. 2003, 26, 361–372. [Google Scholar] [CrossRef] [PubMed]
- Davidson, R.J.; McEwen, B.S. Social influences on neuroplasticity: Stress and interventions to promote well-being. Nat. Neurosci. 2012, 15, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Hedman, E.; Axelsson, E.; Görling, A.; Ritzman, C.; Ronnheden, M.; Alaoui, S.E.; Andersson, E.; Lekander, M.; Ljótsson, B. Internet-delivered exposure-based cognitive-behavioural therapy and behavioural stress management for severe health anxiety: Randomised controlled trial. Br. J. Psychiatry 2014, 205, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Chalah, M.A.; Ayache, S.S. Disentangling the Neural Basis of Cognitive Behavioral Therapy in Psychiatric Disorders: A Focus on Depression. Brian Sci. 2018, 8, 150. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.J.; Stein, D.J. A systematic review of the neural bases of psychotherapy for anxiety and related disorders. Dialogues Clin Neurosci. 2015, 17, 261–279. [Google Scholar]
- Kladnitski, N.; Smith, J.; Allen, A.; Andrews, G.; Newby, J.M. Online mindfulness-enhanced cognitive behavioural therapy for anxiety and depression: Outcomes of a pilot trial. Internet Interv. 2018, 13, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Niles, A.N.; Haltom, K.E.; Mulvenna, C.M.; Lieberman, M.D.; Stanton, A.L. Effects of Expressive Writing on Psychological and Physical Health: The Moderating Role of Emotional Expressivity. Anxiety Stress Coping 2014, 27, 1–19. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| IBS Symptoms (BSSS) | Anxiety (STAI-S) | Depression (CES-D) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Effect | wald x2 | df | P | wald x2 | df | P | wald x2 | df | P |
| Intercept | 41.68 | 1 | <0.001 | 27.53 | 1 | <0.001 | 18.49 | 1 | <0.001 |
| Group | 7.20 | 2 | 0.027 | 267.20 | 2 | <0.001 | 13.96 | 2 | <0.001 |
| Time | 54.06 | 1 | <0.001 | 112.04 | 1 | <0.001 | 79.98 | 1 | <0.001 |
| Group*Time | 12.22 | 2 | 0.002 | 35.01 | 2 | <0.001 | 194.87 | 2 | <0.001 |
| Baseline | 122.83 | 1 | <0.001 | 34.73 | 1 | <0.001 | 23.70 | 1 | <0.001 |
| T1 | T2 | T3 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Adjusted mean | β | SE | P | Post hoc | Adjusted mean | β | SE | P | Post hoc | Adjusted mean | β | SE | P | Post hoc |
| BSSS | |||||||||||||||
| ICBT | −4.66 | −1.66 | 1.74 | 0.341 | −2.24 | 4.49 | 2.26 | 0.049 | −9.90 | −2.87 | 1.91 | 0.136 | |||
| EW | −4.69 | −1.69 | 1.89 | 0.373 | −7.76 | −1.04 | 2.46 | 0.673 | −8.22 | −1.18 | 2.08 | 0.569 | |||
| Control | −3.00 | −6.72 | −7.04 | ||||||||||||
| Baseline | −0.35 | 0.05 | <0.001 | −0.427 | 0.065 | <0.001 | −0.441 | 0.055 | <0.001 | ||||||
| STAI-S | |||||||||||||||
| ICBT | −2.26 | −1.17 | 1.65 | 0.477 | −4.61 | 0.84 | 1.78 | 0.638 | −14.54 | −6.15 | 2.00 | 0.002 | 1 > 3 * | ||
| EW | −5.26 | −4.18 | 1.71 | 0.016 | 2 > 3 * | −10.16 | −4.71 | 1.85 | 0.012 | 2 > 1 * 2 > 3 * | −11.96 | −3.56 | 2.08 | 0.089 | |
| Control | −1.08 | −5.45 | −8.40 | ||||||||||||
| Baseline(ref.) | −0.331 | 0.077 | <0.001 | −0.502 | 0.083 | <0.001 | −0.677 | 0.093 | <0.001 | ||||||
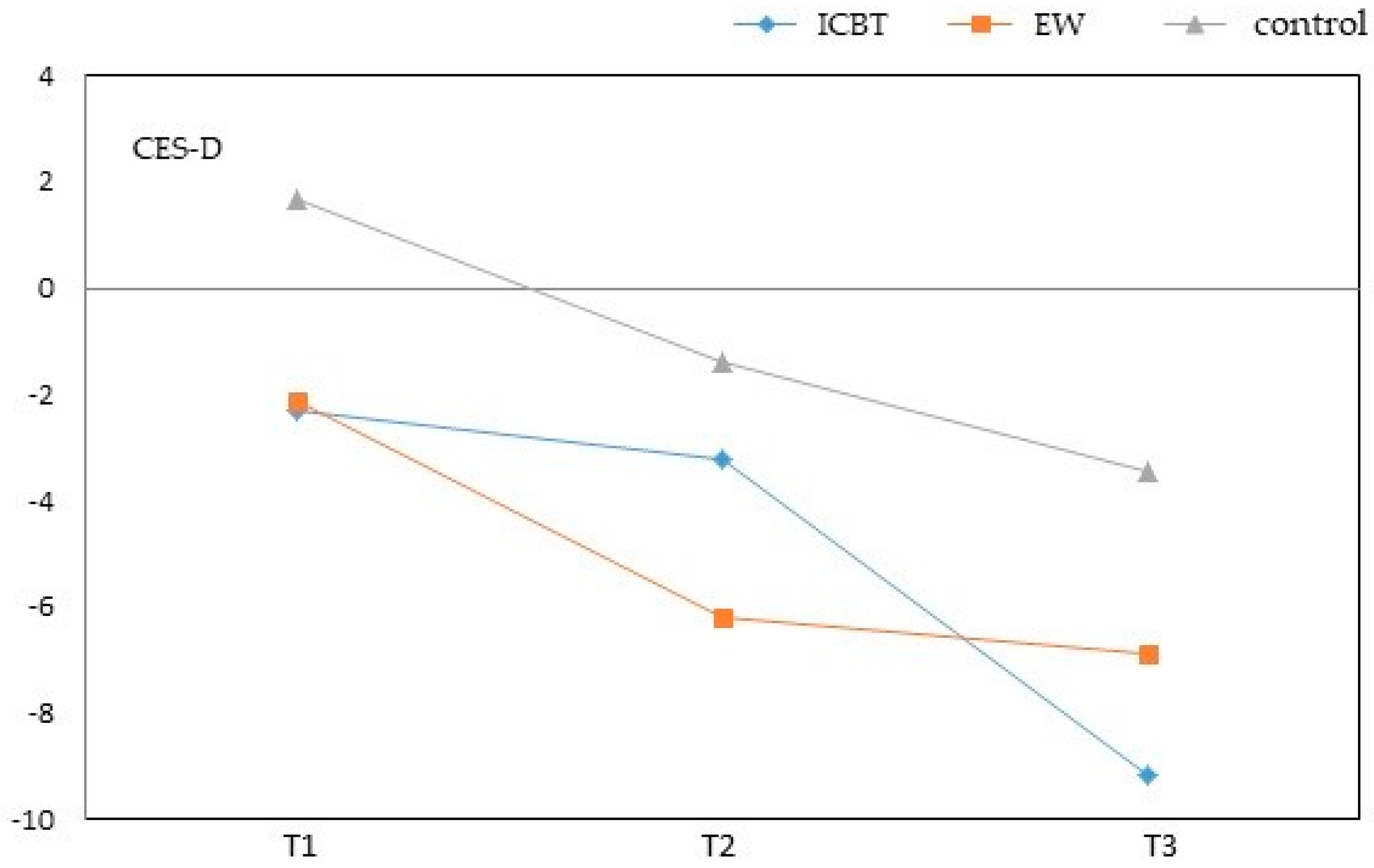
| CES-D | |||||||||||||||
| ICBT | −2.28 | −3.96 | 1.54 | 0.011 | 1 > 3* | −3.28 | −1.87 | 1.64 | 0.254 | −9.15 | −5.71 | 1.60 | <0.001 | 1 > 3 ** | |
| EW | −2.12 | −3.80 | 1.60 | 0.019 | −6.18 | −4.77 | 1.70 | 0.006 | 2 > 3 * | −6.88 | −3.44 | 1.67 | 0.041 | ||
| Control | 1.68 | −1.40 | −3.44 | ||||||||||||
| Baseline(ref.) | −0.323 | 0.063 | <0.001 | −0.438 | 0.067 | <0.001 | −0.621 | 0.065 | <0.001 | ||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, T.-Y.; Hsieh, T.-C.; Sung, H.-C.; Chen, W.-L. Internet-Delivered Cognitive Behavior Therapy for Young Taiwanese Female Nursing Students with Irritable Bowel Syndrome—A Cluster Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 708. https://doi.org/10.3390/ijerph16050708
Lee T-Y, Hsieh T-C, Sung H-C, Chen W-L. Internet-Delivered Cognitive Behavior Therapy for Young Taiwanese Female Nursing Students with Irritable Bowel Syndrome—A Cluster Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2019; 16(5):708. https://doi.org/10.3390/ijerph16050708
Chicago/Turabian StyleLee, Tzu-Ying, Tsung-Cheng Hsieh, Huei-Chuan Sung, and Wan-Lan Chen. 2019. "Internet-Delivered Cognitive Behavior Therapy for Young Taiwanese Female Nursing Students with Irritable Bowel Syndrome—A Cluster Randomized Controlled Trial" International Journal of Environmental Research and Public Health 16, no. 5: 708. https://doi.org/10.3390/ijerph16050708