Perception of Environmental Risks and Behavioral Changes during Pregnancy: A Cross-Sectional Study of French Postpartum Women

 , ,
, ,
Abstract
:1. Introduction
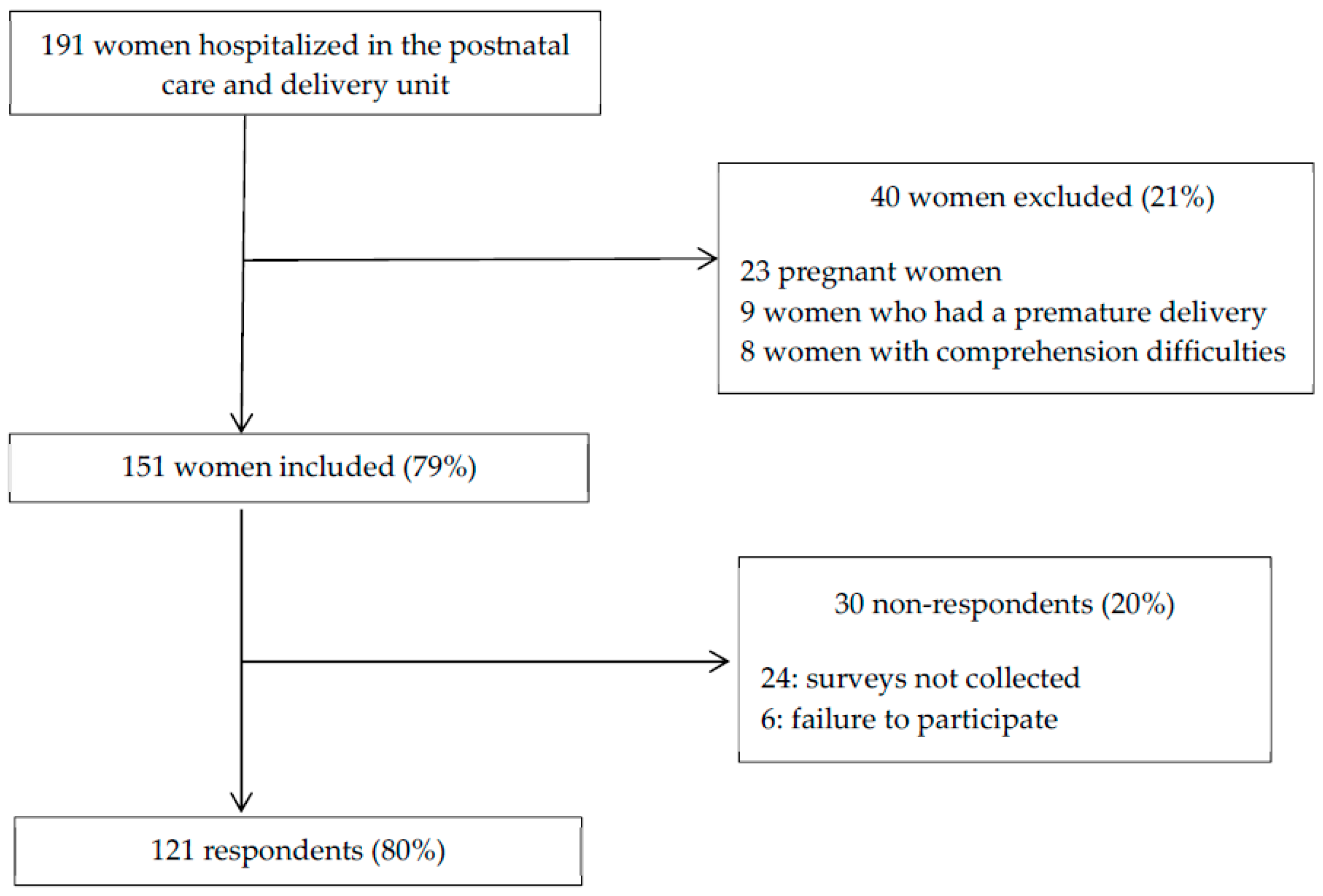
2. Materials and Methods
3. Results
3.1. Characteristics of the Study Population
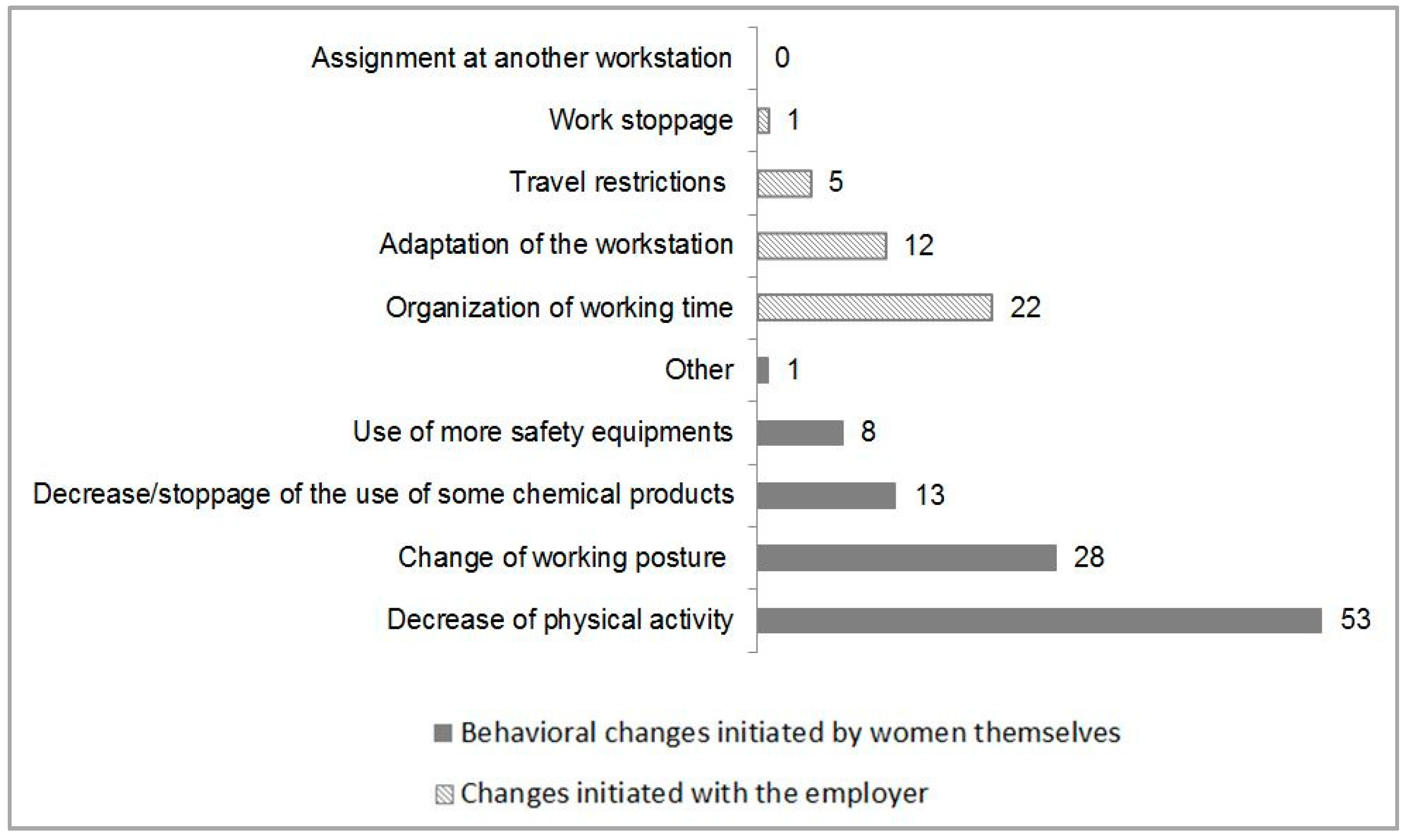
3.2. Perception of Environmental Risks and Behavioral Changes at the Workplace
3.3. Perceptions of Environmental Risks in the Non-Occupational Environment
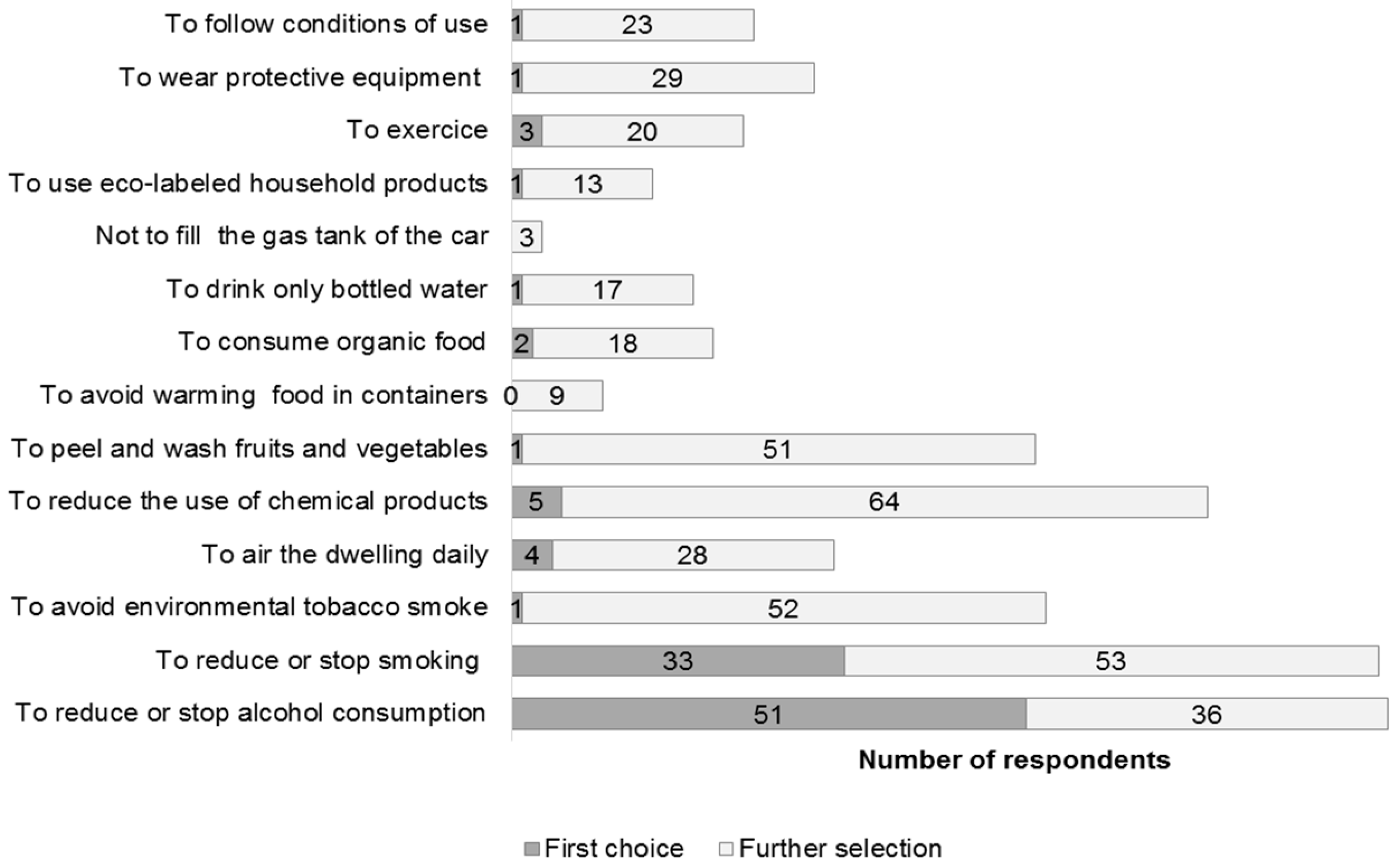
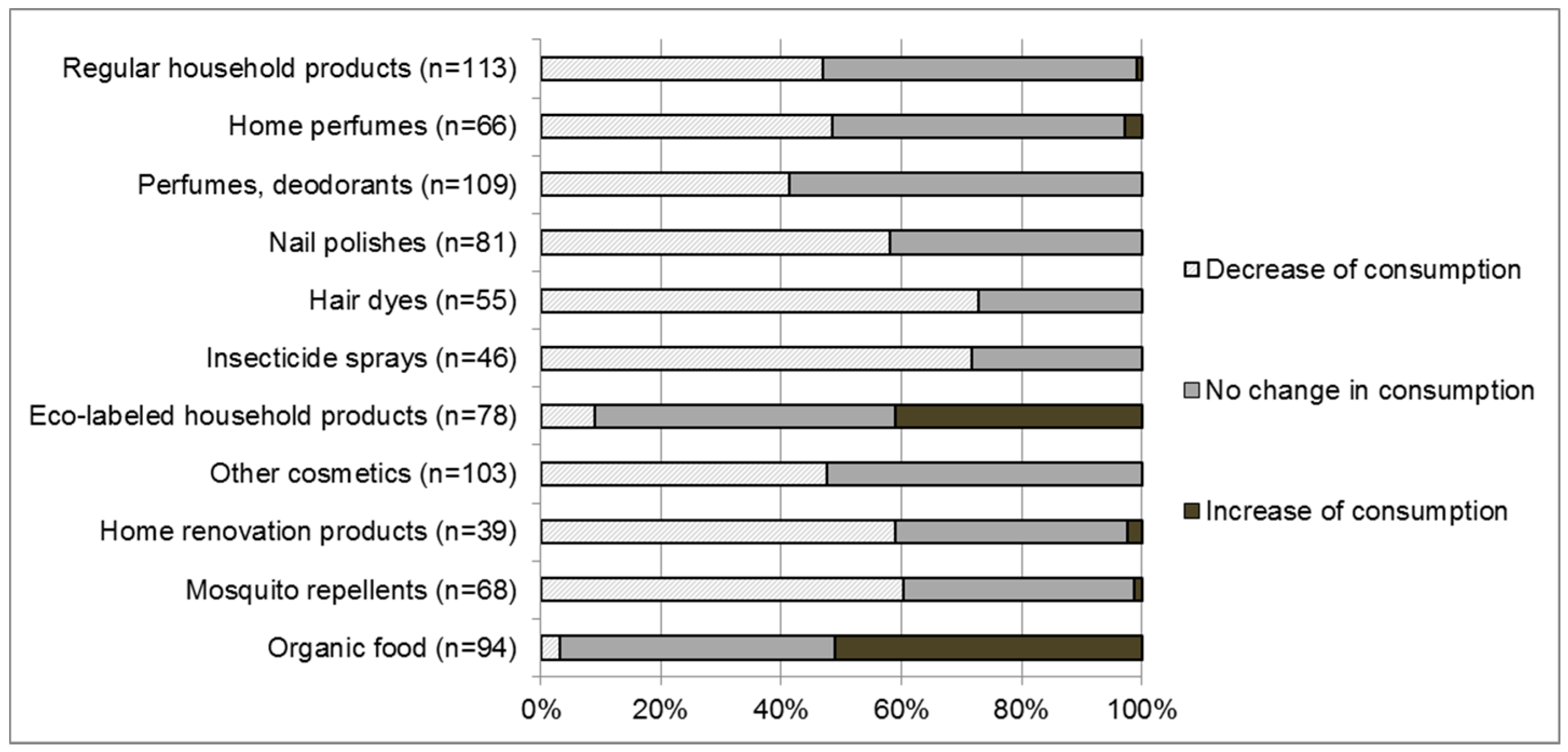
3.4. Behavioral Changes in the Non-Occupational Environment
3.5. Source of Information about the Environment
4. Discussion
4.1. Perceptions of Environmental Risks and Behavioral Changes at Work
4.2. Knowledge and Behavior Concerning Alcohol and Tobacco
4.3. Knowledge and Behavior Concerning the Daily Use of Products
4.4. Source of Information about the Environment
4.5. Strengths and Weaknesses of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Scott-Goodwin, A.C.; Puerto, M.; Moreno, I. Toxic effects of prenatal exposure to alcohol, tobacco and other drugs. Reprod. Toxicol. 2016, 61, 120–130. [Google Scholar] [CrossRef] [PubMed]
- Vrijheid, M.; Casas, M.; Gascon, M.; Valvi, D.; Nieuwenhuijsen, M. Environmental pollutants and child health-A review of recent concerns. Int. J. Hyg. Environ. Health 2016, 219, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Slama, R.; Cordier, S. Impact of chemical and physical environmental factors on the course and outcome of pregnancy. J. Gynecol. Obstet. Biol. Reprod. (Paris) 2013, 42, 413–444. [Google Scholar] [CrossRef]
- Hanke, W.; Jurewicz, J. The risk of adverse reproductive and developmental disorders due to occupational pesticide exposure: an overview of current epidemiological evidence. Int. J. Occup. Med. Environ. Health 2004, 17, 223–243. [Google Scholar]
- Jørgensen, K.T.; Jensen, M.S.; Toft, G.V.; Larsen, A.D.; Bonde, J.P.; Hougaard, K.S. Risk of cryptorchidism among sons of horticultural workers and farmers in Denmark. Scand. J. Work. Environ. Health 2014, 40, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Quansah, R.; Jaakkola, J.J. Occupational exposures and adverse pregnancy outcomes among nurses: A systematic review and meta-analysis. J. Womens Health 2010, 19, 1851–1862. [Google Scholar] [CrossRef] [PubMed]
- Lawson, C.C.; Rocheleau, C.M.; Whelan, E.A.; Lividoti Hibert, E.N.; Grajewski, B.; Spiegelman, D.; Rich-Edwards, J.W. Occupational exposures among nurses and risk of spontaneous abortion. Am. J. Obstet. Gynecol. 2012, 206, 327.e1–327.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronda, E.; Moen, B.E.; García, A.M.; Sánchez-Paya, J.; Baste, V. Pregnancy outcomes in female hairdressers. Int. Arch. Occup. Environ. Health 2010, 83, 945–951. [Google Scholar] [CrossRef]
- Henrotin, J.-B.; Picot, C.; Bouslama, M.; Collot-Fertey, D.; Radauceanu, A.; Labro, M.; Larroque, B.; Roudot, A.-C.; Sater, N.; Elhkim, M.O.; et al. Reproductive disorders in hairdressers and cosmetologists: A meta-analytical approach. J. Occup. Health 2015, 57, 485–496. [Google Scholar] [CrossRef]
- Halliday-Bell, J.A.; Gissler, M.; Jaakkola, J.J.K. Work as a hairdresser and cosmetologist and adverse pregnancy outcomes. Occup. Med. Oxf. Engl. 2009, 59, 180–184. [Google Scholar] [CrossRef] [Green Version]
- Di Renzo, G.C.; Conry, J.A.; Blake, J.; DeFrancesco, M.S.; DeNicola, N.; Martin, J.N.; McCue, K.A.; Richmond, D.; Shah, A.; Sutton, P.; et al. International Federation of Gynecology and Obstetrics opinion on reproductive health impacts of exposure to toxic environmental chemicals. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2015, 131, 219–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemsing, N.; Greaves, L.; Poole, N. Preconception health care interventions: A scoping review. Sex. Reprod. Healthc. 2017, 14, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Thompson, E.L.; Vázquez-Otero, C.; Vamos, C.A.; Marhefka, S.L.; Kline, N.S.; Daley, E.M. Rethinking Preconception Care: A Critical, Women’s Health Perspective. Matern. Child Health J. 2017, 21, 1147–1155. [Google Scholar] [CrossRef] [PubMed]
- Addati, L.; Cassirer, N.; Gilchrist, K. Maternity and Paternity at Work—Law and Practice across the World; International Labour Office: Geneva, Switzerland, 2014. [Google Scholar]
- Toivonen, K.I.; Oinonen, K.A.; Duchene, K.M. Preconception health behaviours: A scoping review. Prev. Med. 2017, 96, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Chabert, M.-C.; Perrin, J.; Berbis, J.; Bretelle, F.; Adnot, S.; Courbiere, B. Lack of information received by a French female cohort regarding prevention against exposure to reprotoxic agents during pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 205, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Rouillon, S.; Deshayes-Morgand, C.; Enjalbert, L.; Rabouan, S.; Hardouin, J.-B.; Group DisProSE; Migeot, V.; Albouy-Llaty, M. Endocrine Disruptors and Pregnancy: Knowledge, Attitudes and Prevention Behaviors of French Women. Int. J. Environ. Res. Public Health 2017, 14, 1021. [Google Scholar] [CrossRef] [PubMed]
- Henrotin, J.-B.; Vaissière, M.; Etaix, M.; Dziurla, M.; Malard, S.; Lafon, D. Occupational risks during pregnancy: Feedback from occupational medical services. Gynecol. Obstet. Fertil. Senol. 2018, 46, 20–27. [Google Scholar]
- Dean, A.; Arner, T.; Sunki, G.; Friedman, R.; Lantinga, M.; Sangam, S.; Zubieta, J.; Sullivan, K.; Brendel, K.; Gao, Z.; et al. Epi InfoTM, a Database and Statistics Program for Public Health Professionals; CDC: Atlanta, GA, USA, 2011. Available online: https://wwwn.cdc.gov/ (accessed on 11 February 2019).
- UNESCO Institute for Statistics International Standard Classification of Education ISCED 2011. Available online: http://uis.unesco.org/sites/default/files/documents/international-standard-classification-of-education-isced-2011-en.pdf (accessed on 11 February 2019).
- Teysseire, R.; Brochard, P.; Sentilhes, L.; Delva, F. Identification and Prioritization of Environmental Reproductive Hazards: A First Step in Establishing Environmental Perinatal Care. Int. J. Environ. Res. Public Health 2019, 16. [Google Scholar] [CrossRef]
- International Labour Organization International Standard Classification of Occupations Structure, Group Definitions and Correspondence Tables 2012. Available online: https://www.ilo.org/public/english/bureau/stat/isco/docs/groupdefn08.pdf (accessed on 11 February 2019).
- Shettle, J. Pregancy, Maternity and Work—Legal Aide-Memoire 2018. Available online: http://www.inrs.fr/dms/inrs/CataloguePapier/ED/TI-TJ-14/tj14.pdf (accessed on 11 February 2019).
- Barouki, R.; Gluckman, P.D.; Grandjean, P.; Hanson, M.; Heindel, J.J. Developmental origins of non-communicable disease: implications for research and public health. Environ. Health Glob. Access Sci. Source 2012, 11, 42. [Google Scholar] [CrossRef]
- Romano, D.; Moreno, N. Barriers for the prevention of chemical exposures in pregnant and breast-feeding workers? J. Epidemiol. Community Health 2010, 64, 193. [Google Scholar] [CrossRef]
- Frey, K.A.; Files, J.A. Preconception Healthcare: What Women Know and Believe. Matern. Child Health J. 2006, 10, 73–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamy, S.; Thibaut, F. Psychoactive substance use during pregnancy: A review. L’Encephale 2010, 36, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Ingall, G.; Cropley, M. Exploring the barriers of quitting smoking during pregnancy: a systematic review of qualitative studies. Women Birth J. Aust. Coll. Midwives 2010, 23, 45–52. [Google Scholar] [CrossRef] [PubMed]
- General Commission for Sustainable Development. French Lifestyles and Environmental Practices; General Commission for Sustainable Development: New York, NY, USA, 2018; p. 100. [Google Scholar]
- Massaquoi, L.D.; Edwards, N.C. A Scoping Review of Maternal and Child Health Clinicians Attitudes, Beliefs, Practice, Training and Perceived Self-Competence in Environmental Health. Int. J. Environ. Res. Public Health 2015, 12, 15769–15781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marie, C.; Lémery, D.; Vendittelli, F.; Sauvant-Rochat, M.-P. Perception of Environmental Risks and Health Promotion Attitudes of French Perinatal Health Professionals. Int. J. Environ. Res. Public Health 2016, 13, 1255. [Google Scholar] [CrossRef] [PubMed]
- Stotland, N.E.; Sutton, P.; Trowbridge, J.; Atchley, D.S.; Conry, J.; Trasande, L.; Gerbert, B.; Charlesworth, A.; Woodruff, T.J. Counseling patients on preventing prenatal environmental exposures—A mixed-methods study of obstetricians. PLoS ONE 2014, 9, e98771. [Google Scholar] [CrossRef] [PubMed]
- Sunyach, C.; Antonelli, B.; Tardieu, S.; Marcot, M.; Perrin, J.; Bretelle, F. Environmental Health in Perinatal and Early Childhood: Awareness, Representation, Knowledge and Practice of Southern France Perinatal Health Professionals. Int. J. Environ. Res. Public Health 2018, 15, 2259. [Google Scholar] [CrossRef]
- Blondel, B.; Coulm, B.; Bonnet, C.; Goffinet, F.; Le Ray, C. Trends in perinatal health in metropolitan France from 1995 to 2016: Results from the French National Perinatal Surveys. J. Gynecol. Obstet. Hum. Reprod. 2017, 46, 701–713. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 121) | Workers (n = 90) | Unemployed (n = 31) | p-Value * | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Age | 0.03 | ||||||
| < 25 | 15 | 12.4 | 7 | 7.8 | 8 | 25.8 | |
| 25–35 | 69 | 57.0 | 52 | 57.8 | 17 | 54.9 | |
| > 35 | 37 | 30.6 | 31 | 34.4 | 6 | 19.3 | |
| Education level | 0.02 | ||||||
| Level 0 to 4 | 52 | 43.0 | 33 | 36.7 | 19 | 61.3 | |
| Level 5 to 8 | 69 | 57.0 | 57 | 63.3 | 12 | 38.7 | |
| Living with a partner 1 | 111 | 94.1 | 83 | 95.4 | 28 | 90.3 | 1 |
| Planned pregnancy 2 | 91 | 75.2 | 70 | 77.8 | 21 | 67.7 | 0.28 |
| Primigravid women | 37 | 30.6 | 26 | 28.9 | 11 | 35.5 | 0.49 |
| Knowledge of pregnancy 3 | 0.34 | ||||||
| 0–1 month | 110 | 91.7 | 82 | 92.1 | 28 | 90.3 | |
| 1–3 months | 9 | 7.5 | 7 | 7.9 | 2 | 6.5 | |
| 3–4 months | 1 | 0.8 | 0 | 0 | 1 | 3.2 | |
| Group of Profession | n (n = 90) | % |
|---|---|---|
| Technicians and associate professionals | 30 | 33.3 |
| Professionals | 21 | 23.3 |
| Service and sales workers | 11 | 12.2 |
| Managers | 10 | 11.1 |
| Clerical support workers | 7 | 7.8 |
| Elementary occupations | 6 | 6.7 |
| Skilled agricultural, forestry, and fishery workers | 2 | 2.2 |
| Total 1 | 87 | 96.6 |
| Total (n = 90) | Exposed (n = 42) | Unexposed (n = 48) | p-Value * | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Pregnancy declaration date to the employer 1 | 0.75 | ||||||
| 0–3 months | 39 | 46.4 | 19 | 51.4 | 20 | 42.6 | |
| 3–4 months | 30 | 35.7 | 13 | 35.1 | 17 | 36.2 | |
| 4–6 months | 13 | 15.5 | 4 | 10.8 | 9 | 19.1 | |
| 6–9 months | 2 | 2.4 | 1 | 2.7 | 1 | 2.1 | |
| Cessation of work 2 | 0.27 | ||||||
| 0–3 months | 5 | 6.0 | 1 | 2.6 | 4 | 8.7 | |
| 3–4 months | 6 | 7.1 | 4 | 10.5 | 2 | 4.3 | |
| 4–6 months | 27 | 32.1 | 15 | 39.5 | 12 | 26.1 | |
| 6–9 months | 46 | 54.8 | 18 | 47.4 | 28 | 60.9 | |
| Behavioral change at the work station by women 2 | 60 | 71.4 | 30 | 78.9 | 30 | 65.2 | 0.17 |
| Change made by the employer at the work station 3 | 34 | 40.5 | 13 | 34.2 | 21 | 45.7 | 0.29 |
| No change made at the workstation | 17 | 18.9 | 5 | 11.9 | 12 | 25 | 0.11 |
| Medical visit with the occupational health physician 4 | 8 | 10.3 | 3 | 9.4 | 5 | 10.9 | 1 |
| Total (n = 121) | Level 0 to 4 of Qualification (n = 52) | Level 5 to 8 of Qualification (n = 69) | p-Value * | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Period of alcohol consumption dangerous for pregnancy 1 | 0.78 | ||||||
| As soon as the period of conception | 28 | 23.7 | 11 | 22.4 | 17 | 24.6 | |
| As soon as the beginning of pregnancy | 90 | 76.3 | 38 | 77.6 | 52 | 75.4 | |
| Period of tobacco consumption dangerous for pregnancy 2 | 0.23 | ||||||
| As soon as the period of conception | 54 | 46.2 | 19 | 39.6 | 35 | 50.7 | |
| As soon as the beginning of pregnancy | 63 | 53.8 | 29 | 60.4 | 34 | 49.3 | |
| Women who consider there to be no level of alcohol consumption that is safe for pregnancy 1 | 116 | 98.3 | 48 | 98.0 | 68 | 98.6 | 1 |
| Women who consider there to be no level of tobacco consumption that is safe for pregnancy 3 | 104 | 90.4 | 42 | 91.3 | 62 | 89.9 | 1 |
| First action considered by women to guaranty a healthy pregnancy | |||||||
| To reduce or stop alcohol consumption | 51 | 42.1 | 13 | 25.0 | 38 | 55.1 | <0.001 |
| To cut down on or stop smoking | 33 | 27.3 | 16 | 30.8 | 17 | 24.6 | 0.45 |
| Actions considered by women to guaranty a healthy pregnancy with no notion of ranking | |||||||
| To reduce or stop alcohol consumption | 87 | 71.9 | 30 | 57.7 | 57 | 82.6 | 0.002 |
| To cut down on or stop smoking | 86 | 71.1 | 32 | 61.5 | 54 | 78.3 | 0.04 |
| Total (n = 121) | Level 0 to 4 of Qualification (n = 52) | Level 4 to 8 Qualification (n = 69) | p-Value * | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Smoking status before knowledge of pregnancy 1 | 0.003 | ||||||
| Non-smoker | 98 | 82.4 | 35 | 70.0 | 63 | 91.3 | |
| Smoker | 21 | 17.6 | 15 | 30.0 | 6 | 8.7 | |
| Daily consumption of cigarettes among smokers before knowledge of pregnancy | 0.44 | ||||||
| [1,2,3,4,5,6,7,8,9,10] | 5 | 23.8 | 3 | 20.0 | 2 | 33.3 | |
| [10,11,12,13,14,15,16,17,18,19,20] | 11 | 52.4 | 7 | 46.7 | 4 | 66.7 | |
| ≥ 20 | 5 | 23.8 | 5 | 33.3 | 0 | 0.0 | |
| Behavioral changes during pregnancy among smokers | 0.15 | ||||||
| Stopped smoking during pregnancy | 8 | 38.1 | 4 | 26.7 | 4 | 66.7 | |
| Cut down on smoking during pregnancy | 13 | 61.9 | 11 | 73.3 | 2 | 33.3 | |
| Daily consumption of cigarettes among smokers during pregnancy | 0.58 | ||||||
| [1,2,3,4,5] | 4 | 30.8 | 4 | 36.4 | 0 | 0 | |
| [5,6,7,8,9,10] | 8 | 61.5 | 6 | 54.5 | 2 | 100 | |
| [10,11,12,13,14,15] | 1 | 7.7 | 1 | 9.1 | 0 | 0 | |
| Daily number of alcohol units consumed before pregnancy 2 | 0.75 | ||||||
| 0 | 106 | 90.6 | 47 | 92.2 | 59 | 89.4 | |
| 1 | 11 | 9.4 | 4 | 7.8 | 7 | 10.6 | |
| Daily number of alcohol units during pregnancy 3 | 1 | ||||||
| 0 | 118 | 100 | 51 | 100 | 67 | 100 | |
| Total | ||
|---|---|---|
| n (n = 121) | % | |
| Women who considered that they were sufficiently informed about the environment 1 | ||
| No/Do not know | 82 | 70.1 |
| Yes | 35 | 29.9 |
| Women who have been informed about the environment during pregnancy by physicians | 54 | 44.6 |
| Principal sources of information | ||
| Internet | 100 | 82.6 |
| Television | 69 | 57.0 |
| Midwife | 52 | 43.0 |
| Magazines | 48 | 39.7 |
| Entourage | 44 | 36.4 |
| Gynecologist | 44 | 36.4 |
| Maternity | 30 | 24.8 |
| General practitioner | 30 | 24.8 |
| Relevant sources of information identified by women | ||
| Midwives | 99 | 81.8 |
| Gynecologists and obstetricians | 88 | 72.7 |
| General practitioner | 45 | 37.2 |
| Occupational physician | 11 | 9.1 |
| Other: Primary Sickness Insurance Fund | 2 | 1.7 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teysseire, R.; Lecourt, M.; Canet, J.; Manangama, G.; Sentilhes, L.; Delva, F. Perception of Environmental Risks and Behavioral Changes during Pregnancy: A Cross-Sectional Study of French Postpartum Women. Int. J. Environ. Res. Public Health 2019, 16, 565. https://doi.org/10.3390/ijerph16040565
Teysseire R, Lecourt M, Canet J, Manangama G, Sentilhes L, Delva F. Perception of Environmental Risks and Behavioral Changes during Pregnancy: A Cross-Sectional Study of French Postpartum Women. International Journal of Environmental Research and Public Health. 2019; 16(4):565. https://doi.org/10.3390/ijerph16040565
Chicago/Turabian StyleTeysseire, Raphaëlle, Marion Lecourt, Jim Canet, Guyguy Manangama, Loïc Sentilhes, and Fleur Delva. 2019. "Perception of Environmental Risks and Behavioral Changes during Pregnancy: A Cross-Sectional Study of French Postpartum Women" International Journal of Environmental Research and Public Health 16, no. 4: 565. https://doi.org/10.3390/ijerph16040565