Family Factors Associated with Selected Childhood Nutrition Aspects in Central Poland


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Characteristics of the Examined Mothers and Their Children
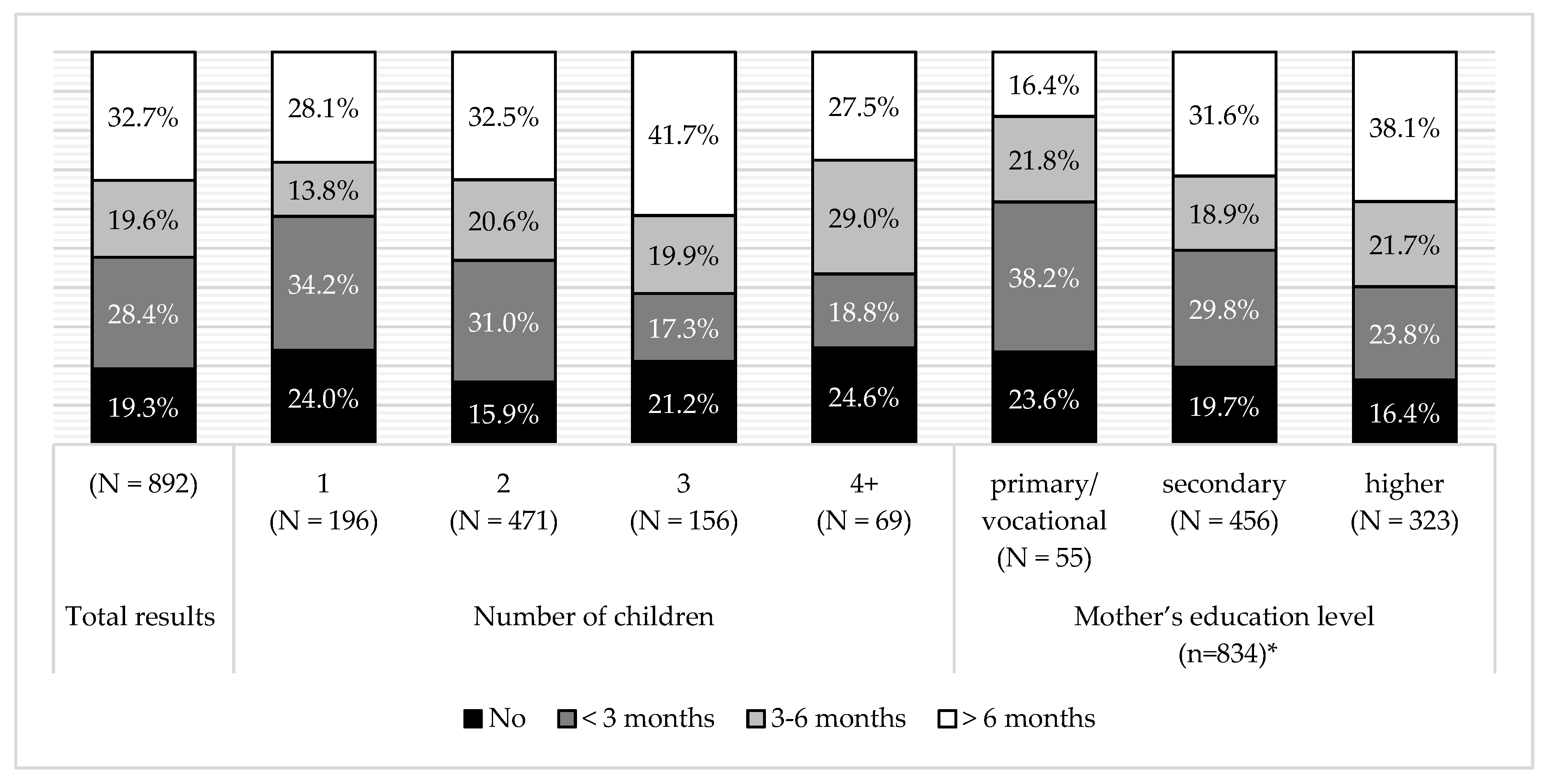
3.2. Breastfeeding
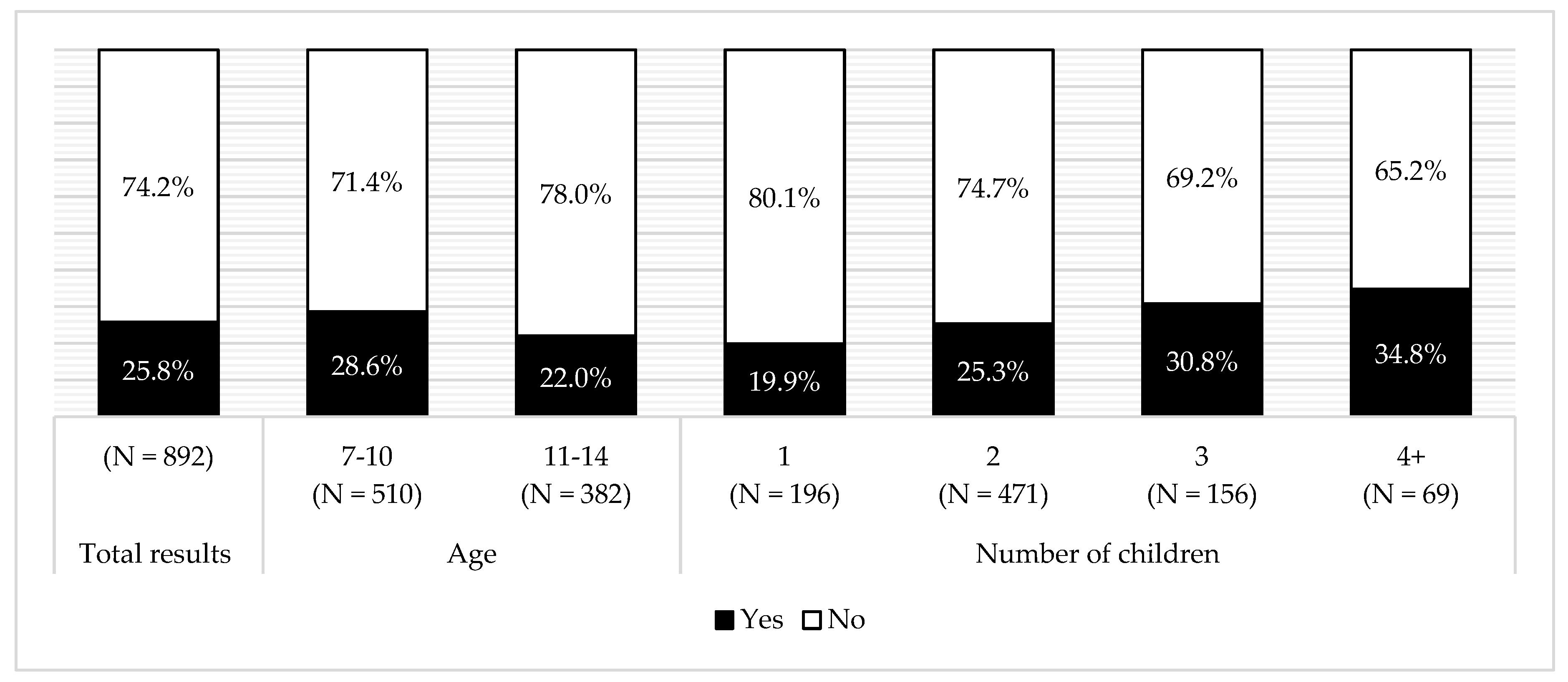
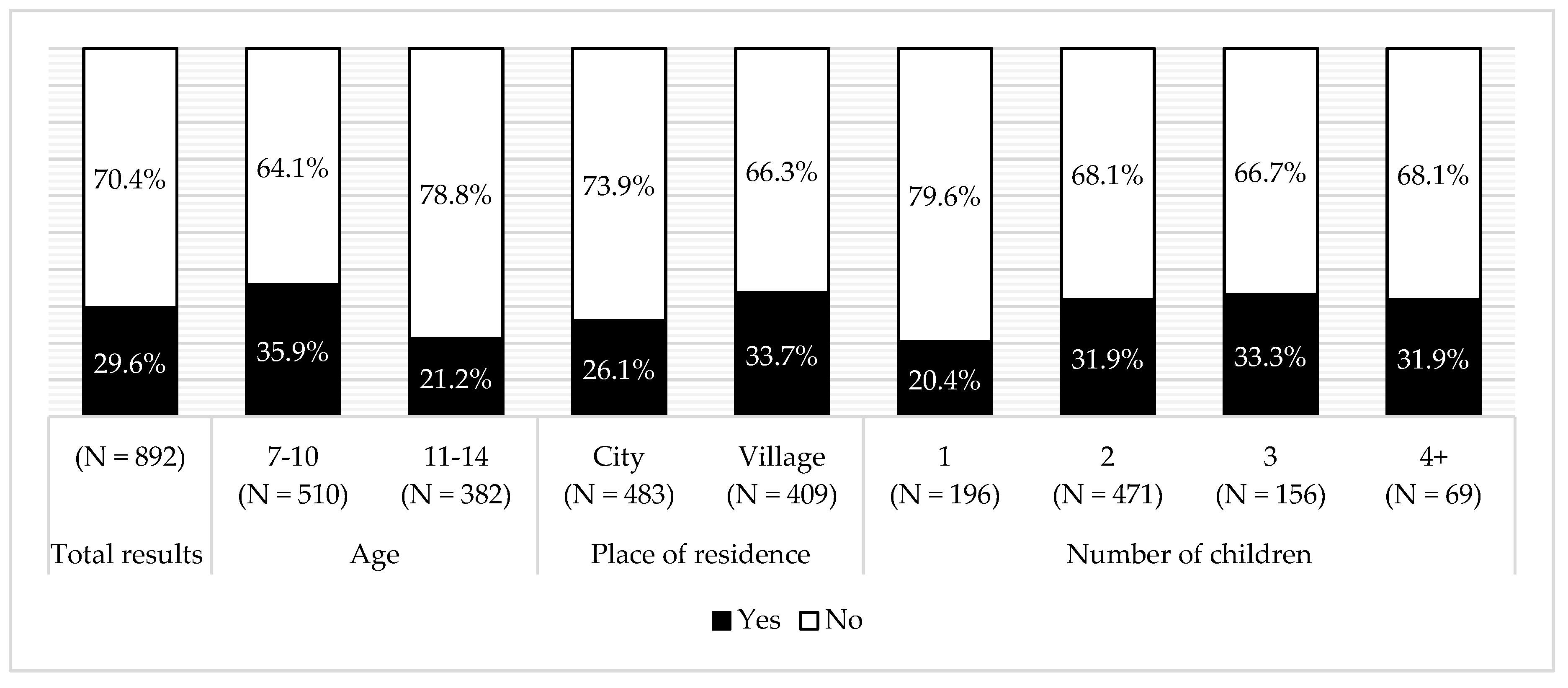
3.3. Using Sweets as a Reward and as a Check for the Prevalence of Dental Caries
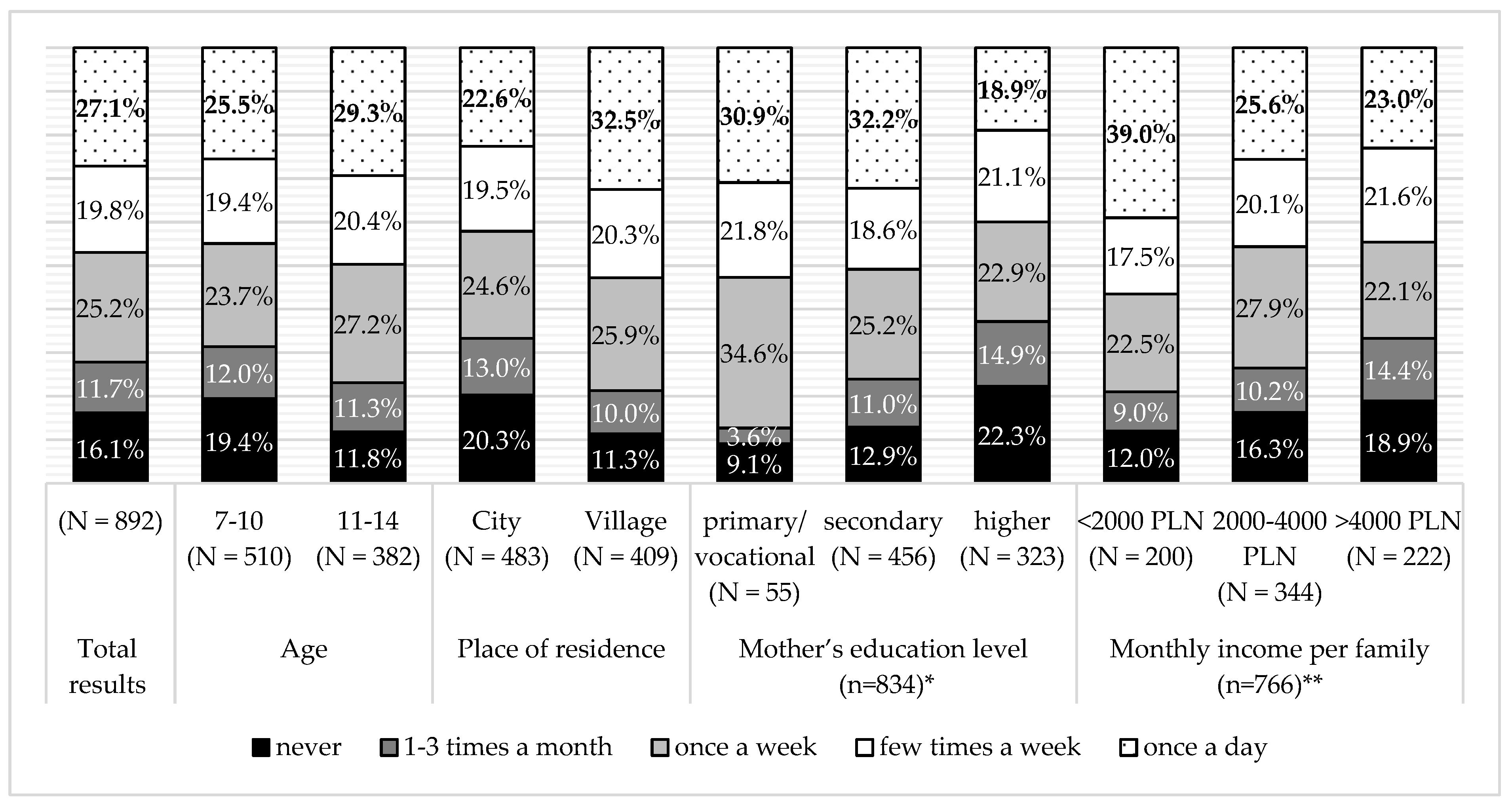
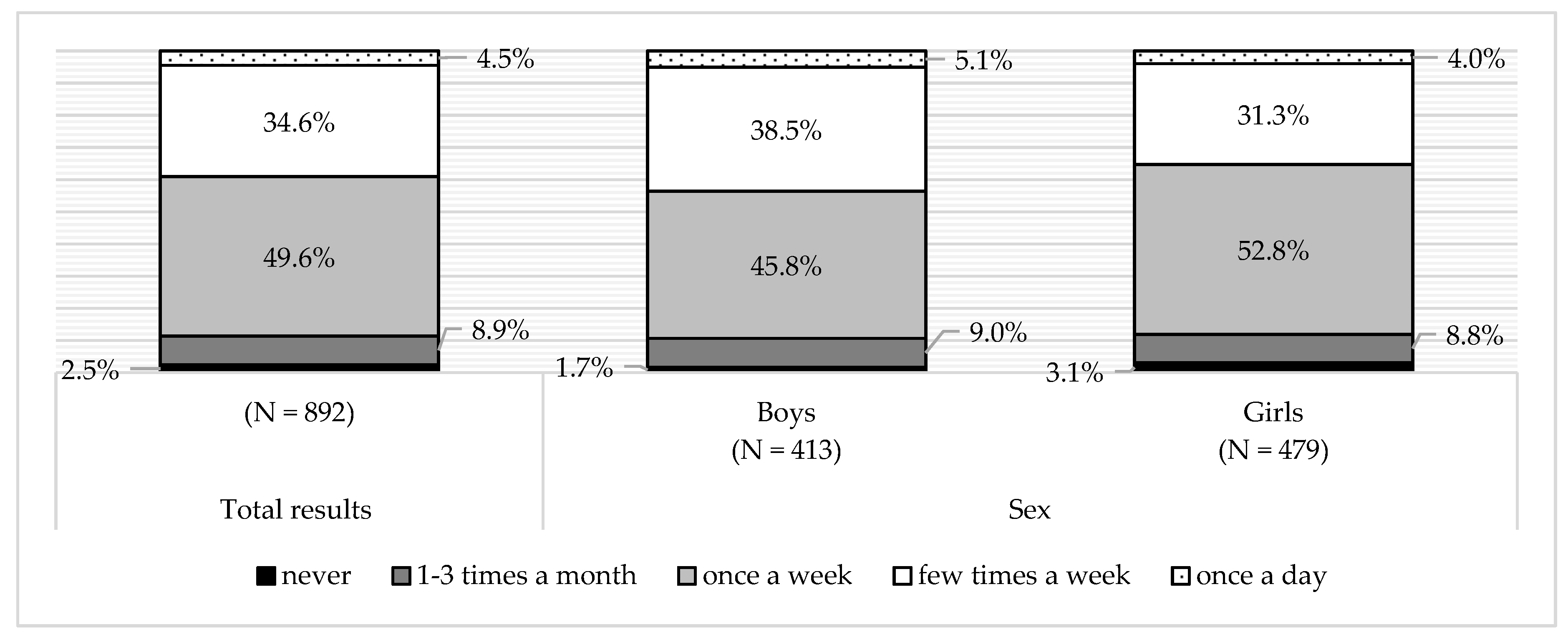
3.4. Sweets Beverage and Snack Consumption
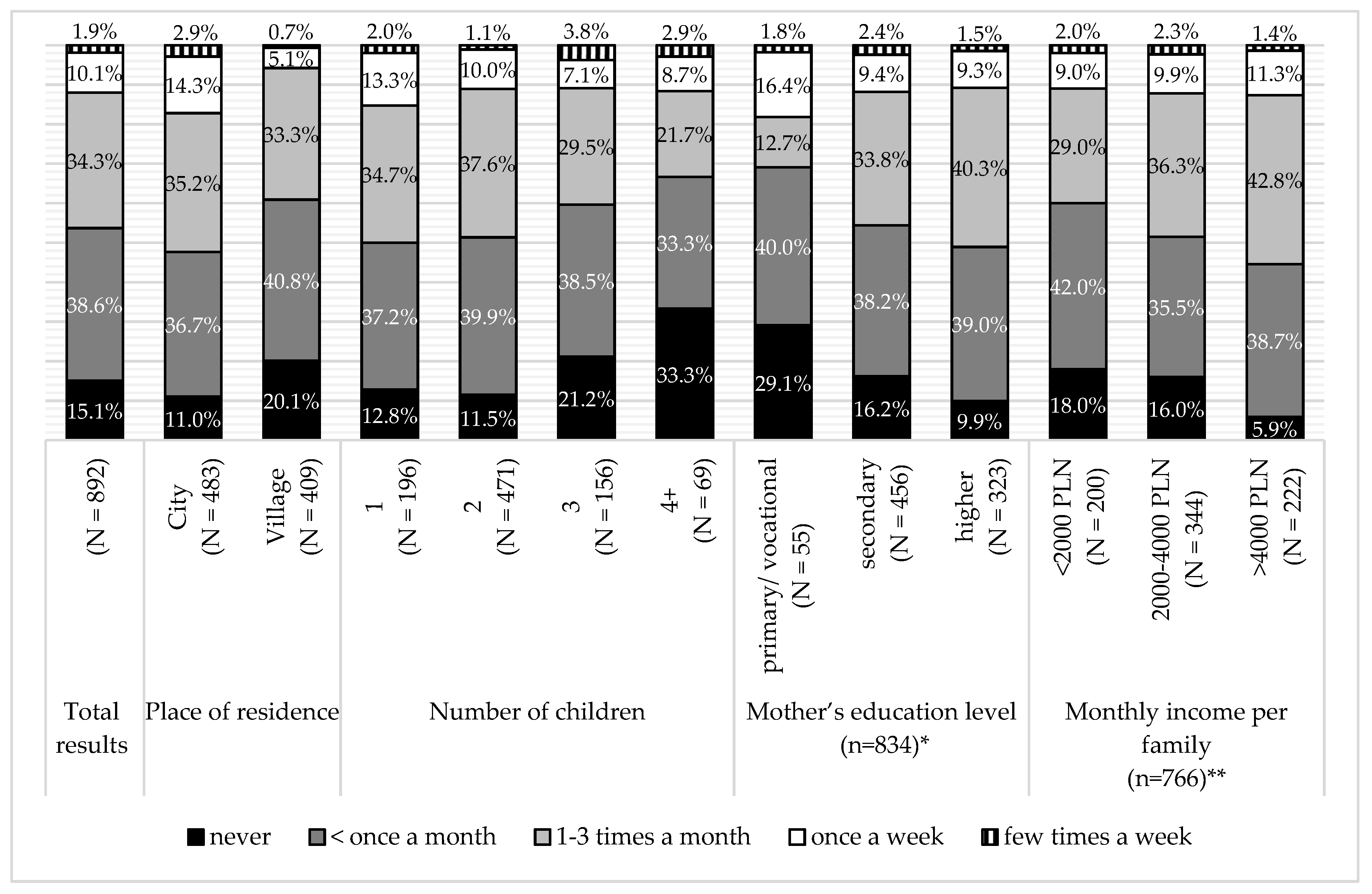
3.5. Fried Food and Fast Food Consumption
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kelishadi, R.; Farajian, S. The protective effects of breastfeeding on chronic non-communicable diseases in adulthood: A review of evidence. Adv. Biomed. Res. 2014, 3. [Google Scholar] [CrossRef] [PubMed]
- Scaglioni, S.; Salvioni, M.; Galimberti, C. Influence of parental attitudes in the development of children eating behaviour. Br. J. Nutr. 2008, 29, 22–25. [Google Scholar] [CrossRef] [PubMed]
- McHale, S.; Crouter, A.; McGuire, S.; Updegraff, K. Congruence between mothers’ and fathers’ differential treatment of siblings: Links with family relations and children’s well-being. Child Dev. 1995, 66, 116–128. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.M.; Ben-Shlomo, Y.; Gunnell, D.; Elwood, P.; Yamell, J.; Smith, G.D. Breast feeding and cardiovascular disease risk factors, incidence, and mortality: The Caerphilly study. J. Epidemiol. Community Health 2005, 59, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Owen, C.; Martin, R.; Whincup, P.; Smith, G.; Cook, D. Effect of Infant Feeding on the Risk of Obesity Across the Life Course: A Quantitative Review of Published Evidence. Pediatrics 2005, 115, 1367–1377. [Google Scholar] [CrossRef] [PubMed]
- Parsons, T.J.; Power, C.; Manor, O. Infant feeding and obesity through the lifecourse. Arch. Dis. Child. 2003, 88, 793–795. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, D.A.; Najman, J.M.; Sterne, J.; Williams, G.; Ebrahim, S.; Smith, G. Associations of parental, birth, and early life characteristics with systolic blood pressure at 5 years of age: Findings from the Mater-University study of pregnancy and its outcomes. Circulation 2004, 110, 2417–2423. [Google Scholar] [CrossRef]
- Leeson, C.P.M.; Kattenhorn, J.; Deanfield, A. Duration of breast feeding and arterial distensibility in early adult life: population based study. BMJ 2001, 322, 643–647. [Google Scholar] [CrossRef]
- Young, T.; Martens, P.; Taback, S.; Sellers, E.; Dean, H.; Cheang, M.; Flett, B. Type 2 Diabetes Mellitus in Children Prenatal and Early Infancy Risk Factors Among Native Canadians. Arch. Pediatr. Adolesc. Med. 2002, 156, 651–655. [Google Scholar] [CrossRef]
- Ravelli, A.C.; van der Meulen, J.H.; Osmond, C.; Barker, D.; Bleker, O. Infant feeding and adult glucose tolerance, lipid profile, blood pressure, and obesity. Arch. Dis. Child. 2000, 82, 248–252. [Google Scholar] [CrossRef]
- Tham, R.; Bowatte, G.; Dharmage, S.; Tan, D.; Lau, M.; Dai, X.; Allen, K.; Lodge, C. Breastfeeding and the risk of dental caries: A systematic review and meta-analysis. Acta Paediatr. Int. J. Paediatr. 2015, 104, 62–84. [Google Scholar] [CrossRef] [PubMed]
- Jarosz, M.; Wolnicka, K.; Kłosowska, J. Environmental factors associated with prevalence of overweight and obesity among children and adolescents. Postępy Nauk Med. 2011, 24, 770–777. [Google Scholar]
- Fisher, J.O.; Birch, L.L. Restricting access to foods and children’s eating. Appetite 1999, 32, 405–419. [Google Scholar] [CrossRef] [PubMed]
- Grimm, G.C.; Harnack, L.; Story, M. Factors associated with soft drink consumption in school-aged children. J. Am. Diet. Assoc. 2004, 104, 1244–1249. [Google Scholar] [CrossRef] [PubMed]
- Jarosz, M.; Rychlik, E. Carbonated sweetened beverages and their associations with diet related diseases. Stand. Med. 2007, 109–114. [Google Scholar]
- Wang, L.; Dalton, W.T.; Schetzina, K.E.; Fulton-Robinson, H.; Holt, N.; Ho, A.; Tudiver, F.; Wu, T. Home Food Environment, Dietary Intake, and Weight among Overweight and Obese Children in Southern Appalachia. South. Med. J. 2013, 106, 550–557. [Google Scholar] [CrossRef]
- Kantovitz, K.R.; Pascon, F.M.; Puppin Rontani, R.M.; Duarte Gavião, M. Obesity and dental caries in children: A systematic review and meta-analysis. Oral Health Prev. Dent. 2006, 4, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health of the Republic of Poland. Oral Health and Its Conditions in the Polish Population Aged 5, 7 and 12 in 2016; Ministry of Health of the Republic of Poland: Warsaw, Poland, 2016. [Google Scholar]
- Harton, A. Children’s nutrition behaviours in Poland. In Children and Youth in the Sociological Dimension; Szymbirski, J., Zatoński, W., Eds.; Wszechnica Polska Szkoła Wyższa w Warszawie: Warsaw, Poland, 2013; pp. 115–133. ISBN 9788389077202. [Google Scholar]
- Ghidurus, M.; Turtoi, M.; Boskou, G.; Niculita, P.; Stan, V. Nutritional and health aspects related to frying (I). Rom. Biotechnol. Lett. 2010, 15, 5675–5682. [Google Scholar]
- Wosje, K.; Khoury, P.; Claytor, R.; Copeland, K.; Hornung, R.; Daniels, S.; Kalkwarf, H. Dietary patterns associated with fat and bone mass in young children. Am J. Clin. Nutr. 2010, 92, 294–303. [Google Scholar] [CrossRef]
- Taveras, E.; Berkey, C.; Rifas-Shiman, S.; Ludwig, D.; Rockett, H.; Field, A.; Colditz, G.; Gillman, M. Association of Consumption of Fried Food Away From Home With Body Mass Index and Diet Quality in Older Children and Adolescents. Pediatrics 2005, 116, e518–e524. [Google Scholar] [CrossRef]
- Qi, Q.; Chu, A.; Kang, J.; Huang, J.; Rose, L.; Jensen, M.; Liang, L.; Curhan, G.; Pasquale, L.; Wiggs, J.; et al. Fried food consumption, genetic risk, and body mass index: gene-diet interaction analysis in three US cohort studies. BMJ 2014, 348, g1610. [Google Scholar] [CrossRef] [PubMed]
- Thompson, O.; Ballew, C.; Resnicow, K.; Must, A.; Bandini, L.; Cyr, H.; Dietz, W. Food purchased away from home as a predictor of change in BMI z-score among girls. Int. J. Obes. Relat. Metab. Disord. 2004, 28, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Zadka, K.; Pałkowska-Goździk, E.; Rosołowska-Huszcz, D. Relation between environmental factors and children’s health behaviors contributing to the occurrence of diet-related diseases in Central Poland. Int. J. Environ. Res. Public Health 2019, 16, 52. [Google Scholar] [CrossRef] [PubMed]
- Noel-Weiss, J.; Boersma, S.; Kujawa-Myles, S. Questioning current definitions for breastfeeding research. Int. Breastfeed. J. 2012, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Michaelsen, K.F.; Weaver, L.; Branca, F.; Robertson, A. Feeding and Nutrition of Infants and Young Children: Guidelines for the WHO European Region, with Emphasis on the Former Soviet Countries; WHO: Copenhagen, Denmark, 2003; ISBN 9289043407 0378-2255. [Google Scholar]
- Statement, P. Breastfeeding and the Use of Human Milk. Pediatrics 2012, 129, 827–841. [Google Scholar] [CrossRef]
- Report on Breastfeeding Status in Poland 2014. Available online: http://cnol.kobiety.med.pl/wp-content/uploads/2019/01/RAPORT-O-STANIE-KARMIENIA-PIERSIĄ-W-POLSCE-2014.pdf (accessed on 20 January 2019).
- Mikiel-Kostyra, K.; Mielniczuk, H.; Wojdan-Gode, E.; Borkowski, W.; Bołtruszko, I. Children nutrition in Poland in 1997. Pediatr. Pol. 1999, 74, 465–471. [Google Scholar]
- Zagórecka, E.; Motkowski, R.; Stolarczyk, A.; Socha, P.; Piotrowska-Jastrzębsa, J.; Socha, J. Breastfeeding in infants living in selected areas of Central and Eastern Poland: preliminary results of a multicenter study. Pediatr. Pol. 2007, 82, 538–549. [Google Scholar] [CrossRef]
- Bernatowicz-Łojko, U.; Wesołowska, A.; Wilińska, M. Share of human milk in feeding children to the second year of life in Poland on the example of Kuyavian-Pomeranian Voivodeship. Stand. Med. 2012, 9, 285–292. [Google Scholar] [CrossRef]
- Report on Breastfeeding Status in Poland 2015. Available online: http://cnol.kobiety.med.pl/wp-content/uploads/2019/01/Raport_Karmienie_Piersia_w_Polsce_20151.pdf (accessed on 20 January 2019).
- Victora, C.G.; Bahl, R.; Barros, A.J.D.; França, G.V.A.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef]
- Bień, A.; Kozak, A.; Rzońca, E.; Stadnicka, S. Opinions and attitudes of women towards breastfeeding. J. Educ. Health Sport 2017, 7, 1258–1271. [Google Scholar] [CrossRef]
- Dzbuk, E.; Bakalczuk, G.; Padała, O.; Orzeł, A.; Putowski, M.; Piróg, M.; Podgórniak, M.; Wdowiak, E.; Wdowiak, A. Knowledge of breastfeeding among women after childbirth. Med. Ogólna i Nauk. o Zdrowiu 2016, 22, 260–263. [Google Scholar] [CrossRef]
- Gebuza, G.; Gierszewska, M.; Kaźmierczak, M.; Michalska, E.; Kotzbach, R. Preparation of women for breast-feeding. Probl. Pielęgniarstwa 2010, 18, 406–412. [Google Scholar]
- Klejewski, A.; Urbaniak, T.; Baczyk, G.; Cichocka, E. Knowlege about breast feeding advantages among primiparas. Przeglad Lek. 2012, 69, 1021–1025. [Google Scholar]
- Cierpka, A.; Żuralska, R.; Olszewski, J.; Gaworska-Krzemińska, A. Knowledge of breastfeeding among midwives. Probl. Pielęgniarstwa 2007, 15, 172–178. [Google Scholar]
- Szostak-Wȩgierek, D.; Cybulska, B.; Zdrojewski, T.; Kopeć, G.; Podolec, P. Why fast food should be forbidden in Polish schools? Kardiol. Pol. 2009, 67, 337–343. [Google Scholar] [PubMed]
- Fisher, J.O.; Wright, G.; Herman, A.N.; Malhotra, K.; Serrano, E.L.; Foster, G.D.; Whitaker, R.C. “Snacks are not food”. Low-income, urban mothers’ perceptions of feeding snacks to their preschool-aged children. Appetite 2015, 84, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Rasińska, R.; Głowacka-Rębała, A. The influence of family behaviours on children’s nutritional behaviours. Pielęgniarstwo Pol. 2013, 1, 12–17. [Google Scholar]
- Wójcicka, A.; Zalewska, M.; Czerech, E.; Jabłoński, R.; Grabowska, S.; Maciorkowska, E. Dental caries of the developmental age as a civilization disease. Przegl. Epidemiol. 2012, 66, 705–711. [Google Scholar] [PubMed]
- Stodolak, A.; Fuglewicz, A. Prevention of caries in children and adolescents and oral health promotion—The role of health care professionals. Med. Ogólna i Nauk. o Zdrowiu 2014, 20, 76–81. [Google Scholar]
- Komosińska, K.; Woynarowska, B. Oral health behaviours among 11-15-year-old adolescents in Poland and other countries and trends between 1990–2002. Nowa Stomatol. 2004, 2, 62–72. [Google Scholar]
- Szczepańska, E.; Piórkowska, K.; Niedworok, E.; Muc-Wierzgoń, M. The consumption of sweets and sweetened beverages in terms of obesity occurrence on the example of children living in rural and urban environment. Endokrynol. Otyłość i Zaburzenia Przemiany Mater. 2010, 6, 78–84. [Google Scholar]
- James, J.; Thomas, P.; Cavan, D.; Kerr, D. Preventing childhood obesity by reducing consumption of carbonated drinks: cluster randomised controlled trial. BMJ 2004, 328, 1237. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; Fulgoni, V.L.; Cowan, A.E.; Gaine, P.C. Sources of added sugars in young children, adolescents, and adults with low and high intakes of added sugars. Nutrients 2018, 10, 102. [Google Scholar] [CrossRef] [PubMed]
- Mensink, G.B.M.; Kleiser, C.; Richter, A. Food consumption of children and adolescents in Germany. Results of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2007, 50, 609–623. [Google Scholar] [CrossRef] [PubMed]
- Mazur, J.; Małkowska-Szkutnik, A. Research results of HBSC 2010. The Technical Raport; Instytut Matki i Dziecka: Warsaw, Poland, 2011; ISBN 978-83-88767-58-6. [Google Scholar]
- Marcinkowska, U.; Gałeczka, M.; Kukowka, K.; Kania, M.; Lau, K.; Jośko-Ochojska, J. Changes in beverage consumption among youth. Probl. Hig. Epidemiol. 2014, 95, 907–911. [Google Scholar]
- Suliga, E. The frequency of the consumption of the first and the second breakfast among rural children. Rocz. Panstw. Zakl. Hig. 2003, 54, 213–220. [Google Scholar] [PubMed]
- Mazarello Paes, V.; Hesketh, K.; O’Malley, C.; Moore, H.; Summerbell, C.; Griffin, S.; van Sluijs, E.; Ong, K.; Lakshman, R. Determinants of sugar-sweetened beverage consumption in young children: A systematic review. Obes. Rev. 2015, 16, 903–913. [Google Scholar] [CrossRef]
- Wojtyła-Buciora, P.; Żukiewicz-Sobczak, W.; Wojtyła, K.; Marcinkowski, J. Nutrition of primary school children in Kalisz district—In children’s and their parents’ opinions. Probl. Hig. Epidemiol. 2015, 96, 245–253. [Google Scholar]
- Świderska-Kopacz, J.; Marcinkowski, J.T.; Jankowska, K. Health behaviour of secondary school pupils and its chosen determinants. Part IV. Nutritional habits. Probl. Hig. Epidemiol. 2008, 89, 241–245. [Google Scholar]
- Stefańska, E.; Falkowska, A.; Ostrowska, L. Selected Nutritional Habits Children and Teenagers Aged 10–15 Years. Rocz. Panstw. Zakl. Hig. 2012, 63, 91–98. [Google Scholar]
- Piernas, C.; Popkin, B.M. Trends in snacking among U.S. children. Health Aff. 2010, 29, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Sawicka, K.; Wawryniuk, A.; Łuczyk, R.J.; Krzyżanowska, E.; Szubiela, N.; Łuczyk, M.; Daniluk, J. Assessment of the state of nutritionality and method of food of children of furnishing to basic and gynal schools. J. Educ. Health Sport 2017, 7, 510–528. [Google Scholar] [CrossRef]
- Babicz-Zielińska, E.; Jeżewska-Zychowicz, M. Impact of the Environmental Factors on Food Choice and Consumption. Handel Wewnętrzny 2015, 2, 5–18. [Google Scholar]
- Platta, A.; Martul, A. The evaluation of parents knowledge with regard to the impact of dietary behaviorus on obesity development among children. Bromatol. i Chem. Toksykol. 2012, XLV, 1087–1091. [Google Scholar]
- Cruz, J.A.A. Dietary habits and nutritional status in adolescents over Europe—Southern Europe. Eur. J. Clin. Nutr. 2000, 54, S29–S35. [Google Scholar] [CrossRef] [PubMed]
- Bowman, S.; Gortmaker, S.; Ebbeling, C.; Pereira, M.; Ludwig, D. Effects of fast-food consumption on energy intake and diet quality among children in a national household survey. Pediatrics 2004, 113, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Fïto, M.; Covas, M.I. Association of fast food consumption with energy intake, diet quality, body mass index and the risk of obesity in a representative Mediterranean population. Br. J. Nutr. 2007, 98, 1274–1280. [Google Scholar] [CrossRef] [PubMed]
- Kośmider, A.; Gronowska-Senger, A. Popularity of “fast-food” products consumption by school youth in urban and country secondary schools from Mazowsze Area. Rocz. PZH 2005, 56, 139–148. [Google Scholar]
- Richardson, A.S.; Boone-Heinonen, J.; Popkin, B.M.; Gordon-Larsen, P. Neighborhood fast food restaurants and fast food consumption: A national study. BMC Public Health 2011, 11, 1–8. [Google Scholar] [CrossRef]
- Łoś-Rycharska, E.; Niecławska, A. Fast-food consumption by 2–3 years old and preschool children. Pediatr. Pol. 2010, 85, 345–352. [Google Scholar] [CrossRef]
- Kral, T.V.E.; Moore, R.H.; Chittams, J.; Jones, E.; O’Malley, L.; Fisher, J.O. Identifying behavioral phenotypes for childhood obesity. Appetite 2018, 127, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Lillycrop, K.A.; Garratt, E.S.; Titcombe, P.; Melton, P.E.; Murray, R.J.S.; Barton, S.J.; Clarke-Harris, R.; Costello, P.M.; Holbrook, J.D.; Hopkins, J.C.; et al. Differential SLC6A4 methylation: a predictive epigenetic marker of adiposity from birth to adulthood. Int. J. Obes. 2019. [Google Scholar] [CrossRef]
- Hinney, A.; Volckmar, A.L.; Antel, J. Genes and the hypothalamic control of metabolism in humans. Best Pract. Res. Clin. Endocrinol. Metab. 2014, 28, 635–647. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Wilkinson, A.; Shen, J.; Wu, X.; Chow, W.H. Genetic polymorphisms in genes related to risk-taking behaviours predicting body mass index trajectory among Mexican American adolescents. Pediatr. Obes. 2017, 12, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Pascual-Gamarra, J.M.; Salazar-Tortosa, D.; Martinez-Tellez, B.; Labayen, I.; Rupérez, A.I.; Censi, L.; Manios, Y.; Nova, E.; Gesteiro, E.; Moreno, L.A.; et al. Association between UCP1, UCP2, and UCP3 gene polymorphisms with markers of adiposity in European adolescents: The HELENA study. Pediatr. Obes. 2019, e12504. [Google Scholar] [CrossRef] [PubMed]
- Samblas, M.; Milagro, F.; Mansego, M.; Marti, A.; Martinez, J. GENOI members PTPRS and PER3 methylation levels are associated with childhood obesity: results from a genome-wide methylation analysis. Pediatr. Obes. 2018, 13, 149–158. [Google Scholar] [CrossRef] [PubMed]






© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zadka, K.; Pałkowska-Goździk, E.; Rosołowska-Huszcz, D. Family Factors Associated with Selected Childhood Nutrition Aspects in Central Poland. Int. J. Environ. Res. Public Health 2019, 16, 541. https://doi.org/10.3390/ijerph16040541
Zadka K, Pałkowska-Goździk E, Rosołowska-Huszcz D. Family Factors Associated with Selected Childhood Nutrition Aspects in Central Poland. International Journal of Environmental Research and Public Health. 2019; 16(4):541. https://doi.org/10.3390/ijerph16040541
Chicago/Turabian StyleZadka, Katarzyna, Ewelina Pałkowska-Goździk, and Danuta Rosołowska-Huszcz. 2019. "Family Factors Associated with Selected Childhood Nutrition Aspects in Central Poland" International Journal of Environmental Research and Public Health 16, no. 4: 541. https://doi.org/10.3390/ijerph16040541