Health Vulnerability Index for Disaster Risk Reduction: Application in Belt and Road Initiative (BRI) Region

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Phase I
Data Scoping and Variable Selection
2.2. Phase II
Statistical Model for the Health Vulnerability Index
2.3. Phase III
Disaster Risk Index Model
Exposure and Hazard
Disaster Risk Index
3. Results
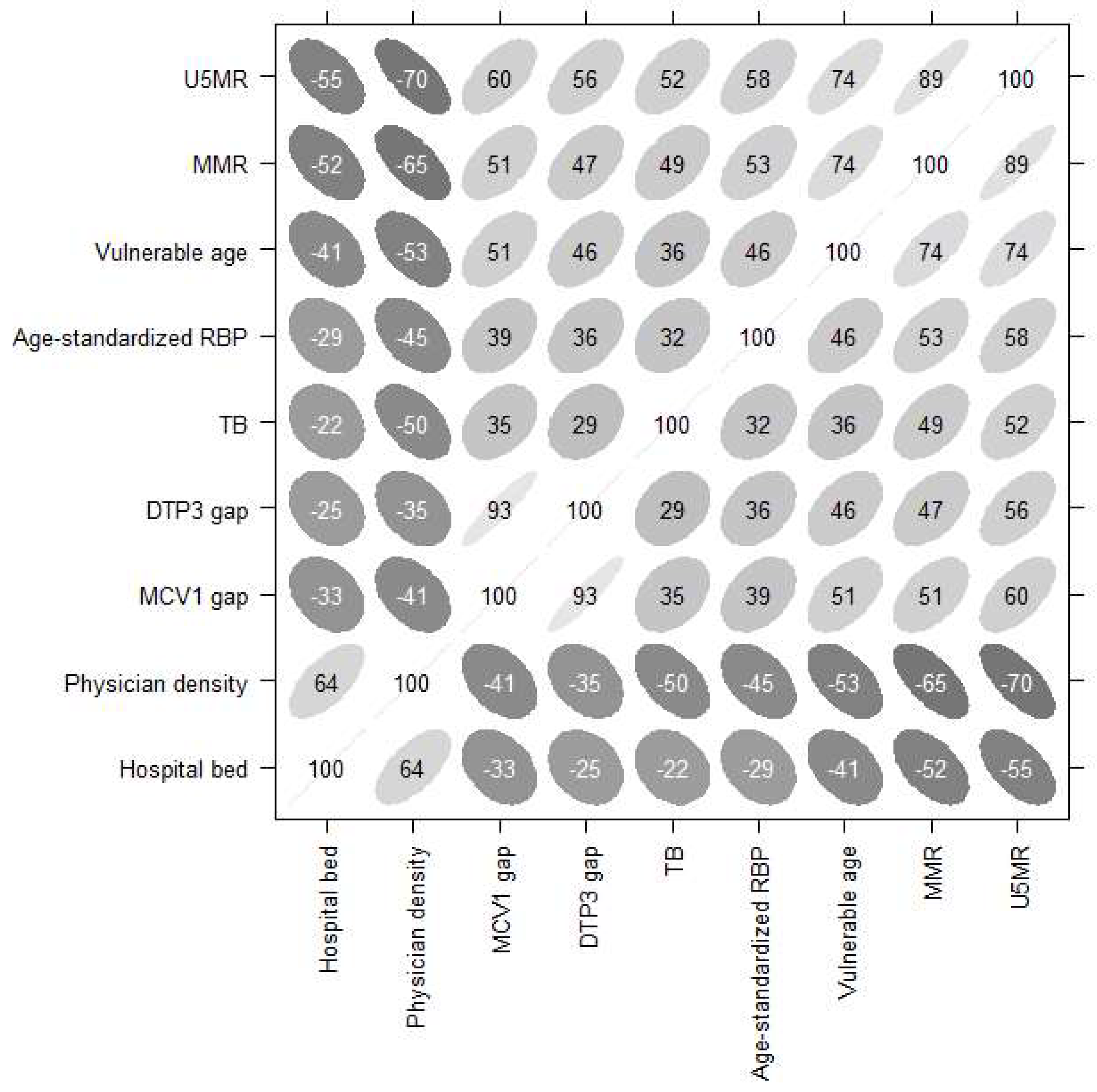
3.1. Key Indicators of Vulnerability
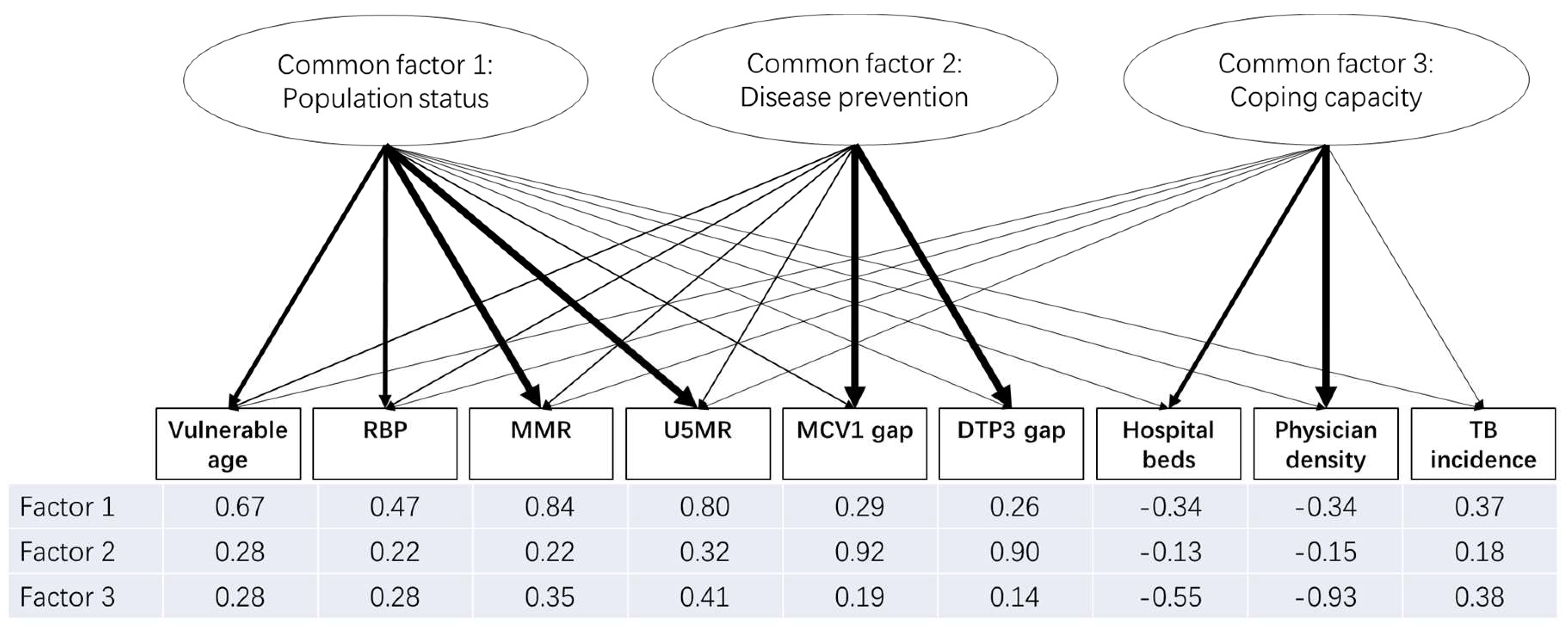
3.2. Underlying Dimensions of Health Vulnerability
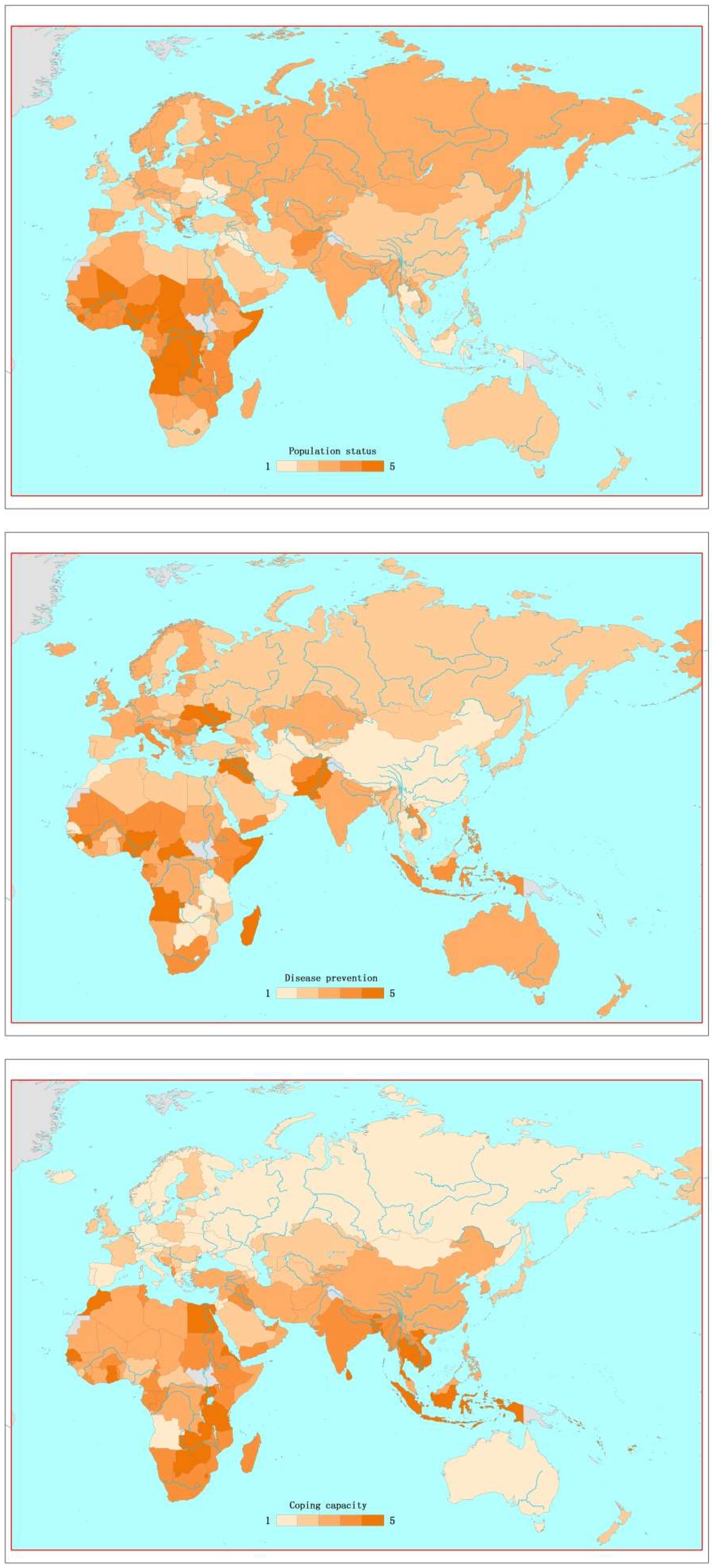
3.3. Factor Scores of Countries
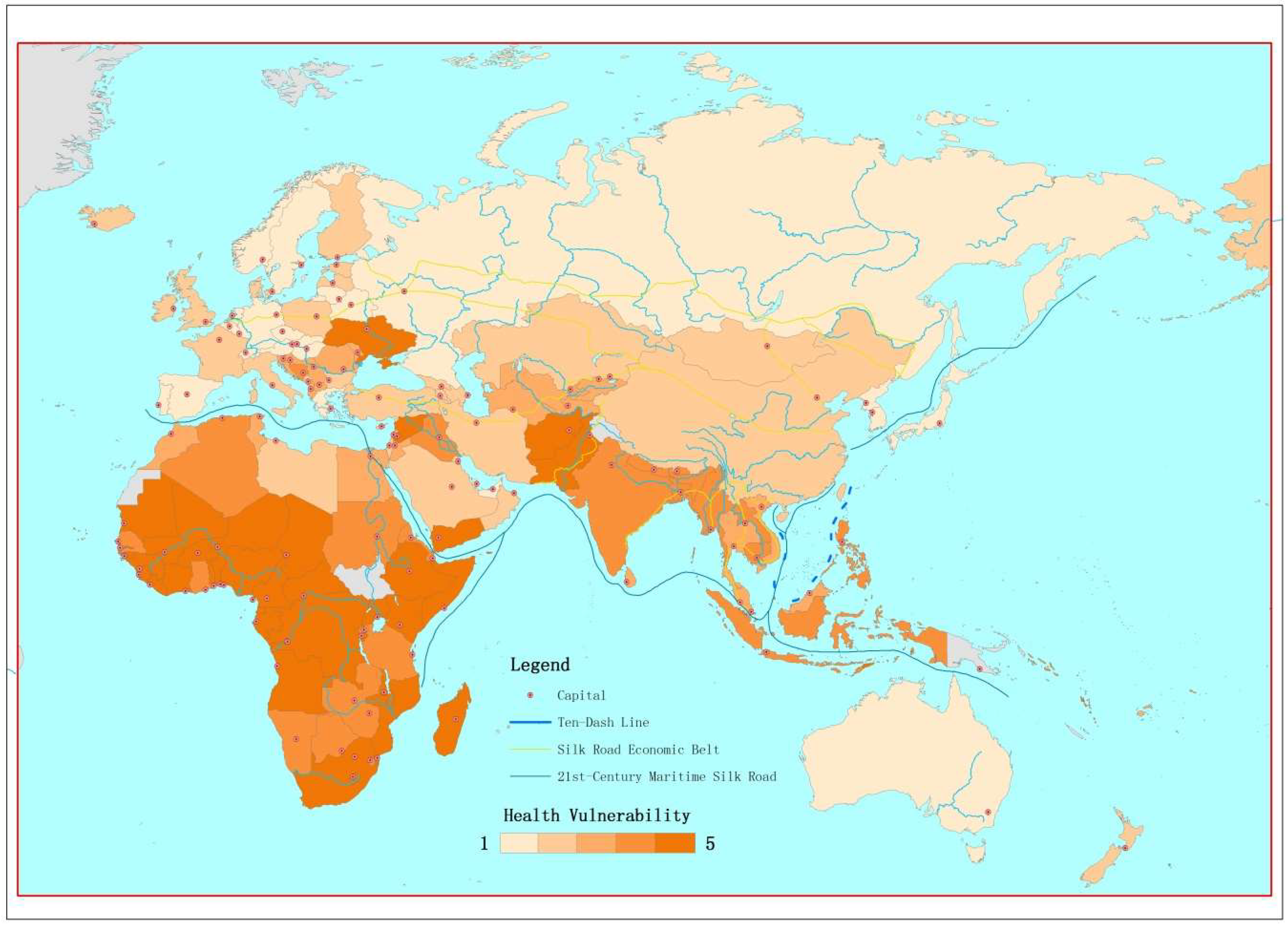
3.4. Health Vulnerability Index of Countries
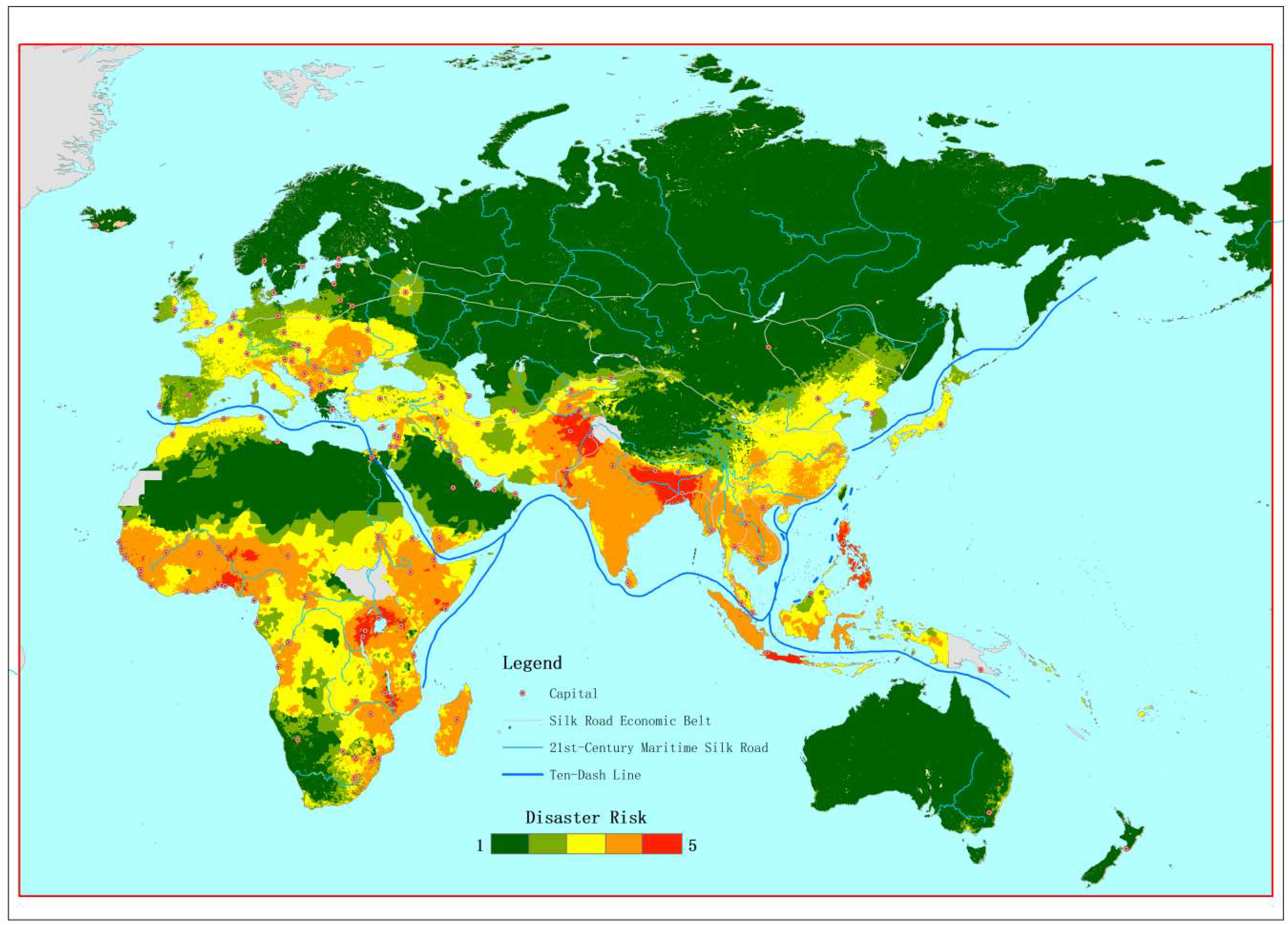
3.5. Disaster Risk Mapping in Silk Road
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- CRED & UNISDR. Economic Losses, Poverty & Disasters, 1998–2017. 2018. Available online: https://www.unisdr.org/files/61119_credeconomiclosses.pdf (accessed on 10 December 2018).
- CRED. Natural disasters in 2017: Lower mortality, Higher Cost. 2018. Available online: https://cred.be/sites/default/files/CredCrunch50.pdf (accessed on 17 December 2018).
- Guha-Sapir, D.; Hoyois, P.H.; Wallemacq, P.; Below, R. Annual Disaster Statistical Review 2016: The Numbers and Trends; Centre for Research on the Epidemiology of Disasters (CRED): Brussels, Belgium, 2017. [Google Scholar]
- IPCC (Intergovernmental Panel on Climate Change). Climate Change 2014: Impacts, Adaptation, and Vulnerability. 2014. Available online: http://www.ipcc.ch/report/ar5/wg2/ (accessed on 11 December 2018).
- UN (United Nations). Sendai Framework for Disaster Risk Reduction 2015–2030. 2015. Available online: https://www.unisdr.org/files/43291_sendaiframeworkfordrren.pdf (accessed on 14 December 2018).
- Kron, W. Flood Risk = hazard• values• vulnerability. Water Int. 2005, 30, 58–68. [Google Scholar] [CrossRef]
- UNISDR. Terminology on Disaster Risk Reduction; UNISDR: Geneva, Switzerland, 2009. [Google Scholar]
- Chan, E.Y.Y.; Murray, V. What are the health research needs for the Sendai Framework? Lancet. 2017, 390, e35–e36. [Google Scholar] [CrossRef]
- Brooks, N.; Adger, W.N.; Kelly, P.M. The determinants of vulnerability and adaptive capacity at the national level and the implications for adaptation. Glob. Environ. Chang. 2005, 15, 151–163. [Google Scholar] [CrossRef]
- Cutter, S.L.; Carolina, S.; Boruff, B.J.; Carolina, S.; Shirley, W.L.; Carolina, S. Social Vulnerability to Environmental Hazards n. Soc. Sci. Q. 2003, 84, 242–261. [Google Scholar] [CrossRef]
- UNDP (United Nations Development Programme). Reducing Disaster Risk: A Challenge for Development; United Nations Development Programme: New York, NY, USA, 2004. [Google Scholar]
- Reid, C.E.; O’neill, M.S.; Gronlund, C.J.; Brines, S.J.; Brown, D.G.; Diez-Roux, A.V.; Schwartz, J. Mapping community determinants of heat vulnerability. Environ. Health Perspect. 2009, 117, 1730. [Google Scholar] [CrossRef] [PubMed]
- Wolf, T.; McGregor, G. The development of a heat wave vulnerability index for London, United Kingdom. Weather Clim. Extrem. 2013, 1, 59–68. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Q.; Liu, T.; Lin, H.; Xiao, J.; Luo, Y.; Zeng, W.; Zeng, S.; Wei, Y.; Chu, C.; Baum, S.; et al. The spatial distribution of health vulnerability to heat waves in Guangdong Province, China. Glob. Health Action 2014, 7, 25051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phung, D.; Rutherford, S.; Dwirahmadi, F.; Chu, C.; Do, C.M.; Nguyen, T.; Duong, N.C. The spatial distribution of vulnerability to the health impacts of flooding in the Mekong Delta, Vietnam. Int. J. Biometeorol. 2016, 60, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Pastrana, M.E.; Brito, R.L.; Nicolino, R.R.; de Oliveira, C.S.; Haddad, J.P. Spatial and statistical methodologies to determine the distribution of dengue in Brazilian municipalities and relate incidence with the health vulnerability index. Spat. Spatio-Temporal Epidemiol. 2014, 11, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.M.; Awan, H.; Khan, N. Mapping vulnerability to climate change and its repercussions on human health in Pakistan. Glob. Health 2012, 8, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inter-Agency Standing Committee (IASC) and the European Commission. Interpreting and Applying the INFORM Global Model. 2015. Available online: http://www.inform-index.org/LinkClick.aspx?fileticket=M-RXb0tKsjs%3d&tabid=101&portalid=0&mid=447 (accessed on 17 December 2018).
- Welle, T.; Birkmann, J. The world risk index–an approach to assess risk and vulnerability on a global scale. J. Extrem. Events 2015, 2, 1550003. [Google Scholar] [CrossRef]
- Chan, E.Y.Y. Public Health Humanitarian Responses to Natural Disasters; Routledge: London, UK, 2017. [Google Scholar]
- NDRC (National Development and Reform Commission). Vision and Actions on Jointly Building Silk Road Economic Belt and 21st-Century Maritime Silk Road. 2015. Available online: http://http://en.ndrc.gov.cn/newsrelease/201503/t20150330_669367.html (accessed on 16 December 2018).
- Hu, R.; Liu, R.; Hu, N. China’s Belt and Road Initiative from a global health perspective. Lancet Glob. Health. 2017, 5, e752–e753. [Google Scholar] [CrossRef]
- Lo, S.T.T.; Chan, E.Y.Y.; Chan, G.K.W.; Murray, V.; Ardalan, A.; Abrahams, J. Health Emergency and Disaster Management (H-EDRM): Developing the research field within the Sendai Framework paradigm. Int. J. Disaster Risk Sci. 2017. [Google Scholar] [CrossRef]
- Nardo, M.; Saisana, M.; Saltelli, A.; Tarantola, S.; Hoffman, A.; Giovannini, E. Handbook on Constructing Composite Indicators; OECD: Paris, France, 2008. [Google Scholar]
- Everitt, B.; Hothorn, T. An Introduction to Applied Multivariate Analysis with R; Springer Science & Business Media: New York, NY, USA, 2011. [Google Scholar]
- Kaiser, H.F. The varimax criterion for analytic rotation in factor analysis. Psychometrika 1958, 23, 187–200. [Google Scholar] [CrossRef]
- Li, V.O.; Han, Y.; Lam, J.C.; Zhu, Y.; Bacon-Shone, J. Air pollution and environmental injustice: Are the socially deprived exposed to more PM 2.5 pollution in Hong Kong? Environ. Sci. Policy. 2018, 80, 53–61. [Google Scholar] [CrossRef]
- UNEP/UNISDR. Global Risk Data Platform. 2013. Available online: https://preview.grid.unep.ch (accessed on 1 November 2018).
- Shi, P.; Kasperson, R. World Atlas of Natural Disaster Risk; Springer: Heidelberg, Germany, 2015. [Google Scholar]
- SEDAC (Socioeconomic Data and Applications Center). UN-Adjusted Population Density, v4. Available online: http://beta.sedac.ciesin.columbia.edu/data/set/gpw-v4-population-density-adjusted-to-2015-unwpp-country-totals/maps (accessed on 15 December 2018).
- WHO (World Health Organization). Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks. 2009. Available online: https://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdf (accessed on 17 December 2018).
- Trninić, V.; Jelaska, I.; Štalec, J. Appropriateness and limitations of factor analysis methods utilized in psychology and kinesiology: Part, I.I. Fizička Kultura, 2013; 67, 1–7. [Google Scholar]
- WHO (World Health Organization). Emergency Risk Management for Health—Overview. 2011. Available online: http://www.who.int/hac/techguidance/preparedness/risk_management_overview_17may2013.pdf?ua=1 (accessed on 10 December 2018).
- Ciurean, R.L.; Schröter, D.; Glade, T. Conceptual frameworks of vulnerability assessments for natural disasters reduction. In Approaches to Disaster Management; IntechOpen: London, UK, 2013. [Google Scholar]
- Matyas, D.; Pelling, M. Disaster Vulnerability and Resilience: Theory, Modelling and Prospective; Foresight: London, UK, 2012. [Google Scholar]
- Rappold, A.G.; Reyes, J.; Pouliot, G.; Cascio, W.E.; Diaz-Sanchez, D. Community vulnerability to health impacts of wildland fire smoke exposure. Environ. Sci. Technol. 2017, 51, 6674–6682. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dimension of Health Vulnerability | Indicator | Conceptual Relevance to Health Vulnerability |
|---|---|---|
| Vulnerable age a | 1. Population ages 0–14 and population ages 65 and above (% of total) | Extreme age groups (children and elderly) are known to be more vulnerable to health risks and less likely to be resilient when a disaster strikes. This is an important component in the “dependency ratio”. They are more likely to accumulate post-disaster health and service needs. |
| Premature mortality b | 2. Under-five mortality rate (probability of dying by age five per 1000 live births) | Leading indicator of health in the United Nation (UN)’s Sustainable Development Goals (SDGs). It is closely linked to maternal health. |
| Preventable mortality b | 3. Maternal mortality ratio (per 100,000 live births) | Leading indicator of health in the UN’s Sustainable Development Goals (SDGs). In addition to preventable deaths, this indicator reflects the capacity of health systems to effectively prevent and address the complications occurring during pregnancy and childbirth. |
| Vaccination gap for measles b | 4. Measles-containing-vaccine first-dose (MCV1) immunization coverage gap among one-year-olds (%) | Standard Expanded Program on Immunization (EPI) for common preventable Childhood Communicable Diseases for children <one year old. Coverage may be used to monitor immunization services as well as guide disease eradication and elimination efforts, and are a good indicator of health system performance. MCV1: Measles is one of the most contagious and mortality-causing diseases in displaced camps. DTP3: Tetanus is common preventable infection associated with injury/wound. |
| Vaccination gap for diphtheria, tetanus, and pertussis b | 5. Diphtheria tetanus toxoid and pertussis (DTP3) immunization coverage gap among 1-year-olds (%) | |
| Chronic diseases status b | 6. Raised blood pressure (SBP ≥140 OR DBP ≥90), age-standardized (%) | A proxy indicator for chronic non-communicable disease. Hypertension and heart disease are some of the leading causes of mortality and morbidity globally. Disease status and potential activity limitations among adults can impair one’s ability to prepare, respond, or recover from a disaster. |
| Infectious disease b | 7. Incidence of tuberculosis (per 100,000 population per year) | Tuberculosis (TB) is the second leading infectious cause of death, and one of the most burden-inflicting diseases in the world. SDGs include ending the TB epidemic by 2030. The incidence of tuberculosis gives an indication of the burden of TB in a population. |
| Coping capacity b | 8. Hospital beds (per 10,000 population) | Health systems resources indicate the level of access to care and the provision of quality medical care, which are highly correlated with live-saving and health status. |
| 9. Physicians’ density (per 1000 population) |
| Components | INFORM | World Risk Index | The Proposed Index |
|---|---|---|---|
| Infectious diseases | Tuberculosis prevalence | Tuberculosis prevalence | |
| Estimate % of adults (>15) living with HIV | |||
| Malaria death rate | |||
| Chronic diseases | Age-standardized raised blood pressure | ||
| Maternal outcome | Maternal mortality | Maternal mortality | |
| Children under five | Under-five mortality | Under five mortality | |
| Malnutrition in children under five | |||
| Medical services and access | Physician ratio | Physicians ratio | Physicians ratio |
| Hospital beds ratio | Hospital beds ratio | ||
| Per capita expenditure on private and public health care | Public medical expenditure; private medical expenditure | ||
| Immunization | Measles immunization coverage | Coverage of two the MCV1 and DTP3 vaccine | |
| Dependency ratio | Proportion of population <15 years old and >65 years old | Proportion of population <15 years old and >65 years old |
| Top 10 Countries/Regions with Highest Vulnerability/Capacity | INFORM | World Risk Index | The Proposed Index | |
|---|---|---|---|---|
| Coping Capacity | Vulnerability | Vulnerability Including Susceptibility, Coping Capacities, and Adaptive Capacities | Vulnerability | |
| 1 | South Sudan | South Sudan | Chad | Somalia |
| 2 | Somalia | Somalia | Eritrea | Central African Republic |
| 3 | Chad | Central African Republic | Afghanistan | Chad |
| 4 | Central African Republic | Democratic Republic of the Congo | Haiti | Equatorial Guinea |
| 5 | Democratic Republic of the Congo | Chad | Niger | Nigeria |
| 6 | Yemen | Yemen | Central African Republic | Guinea |
| 7 | Guinea-Bissau | Syria | Liberia | Sierra Leone |
| 8 | Eritrea | Afghanistan | Sierra Leone | Mali |
| 9 | Liberia | Haiti | Mozambique | Niger |
| 10 | Togo | Sudan | Guinea | Democratic Republic of the Congo |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, E.Y.Y.; Huang, Z.; Lam, H.C.Y.; Wong, C.K.P.; Zou, Q. Health Vulnerability Index for Disaster Risk Reduction: Application in Belt and Road Initiative (BRI) Region. Int. J. Environ. Res. Public Health 2019, 16, 380. https://doi.org/10.3390/ijerph16030380
Chan EYY, Huang Z, Lam HCY, Wong CKP, Zou Q. Health Vulnerability Index for Disaster Risk Reduction: Application in Belt and Road Initiative (BRI) Region. International Journal of Environmental Research and Public Health. 2019; 16(3):380. https://doi.org/10.3390/ijerph16030380
Chicago/Turabian StyleChan, Emily Yang Ying, Zhe Huang, Holly Ching Yu Lam, Carol Ka Po Wong, and Qiang Zou. 2019. "Health Vulnerability Index for Disaster Risk Reduction: Application in Belt and Road Initiative (BRI) Region" International Journal of Environmental Research and Public Health 16, no. 3: 380. https://doi.org/10.3390/ijerph16030380