Selecting and Performing Service-Learning in a Team-Based Learning Format Fosters Dissonance, Reflective Capacity, Self-Examination, Bias Mitigation, and Compassionate Behavior in Prospective Medical Students



Abstract
:1. Introduction
Part of my application to medical school was a story about my grandfather…He’s the person I probably most respect in this world, and he doesn’t speak English, and I remember going with him as a kid to the doctor…it’s one of my driving factors in medicine, and I’m always willing to interpret [for patients]. I’m always willing to stay behind. I never complain…because I know…people deserve that, and…people probably have grandchildren in medical school or who are doctors, so I pray that [healthcare professionals] really treat…people the best they can.
1.1. The Importance of Dissonance, Implicit Bias, and Their Reconciliation Using Self-Examination and CR
1.2. Team-Based Learning (TBL) Produces a Welcoming Team Environment for Reflection
1.3. Hypotheses
2. Methods
2.1. Participants
2.2. Team Formation and Procedure
2.3. Assessment of Dissonance and Subsequent Development by Students in the First Cohort
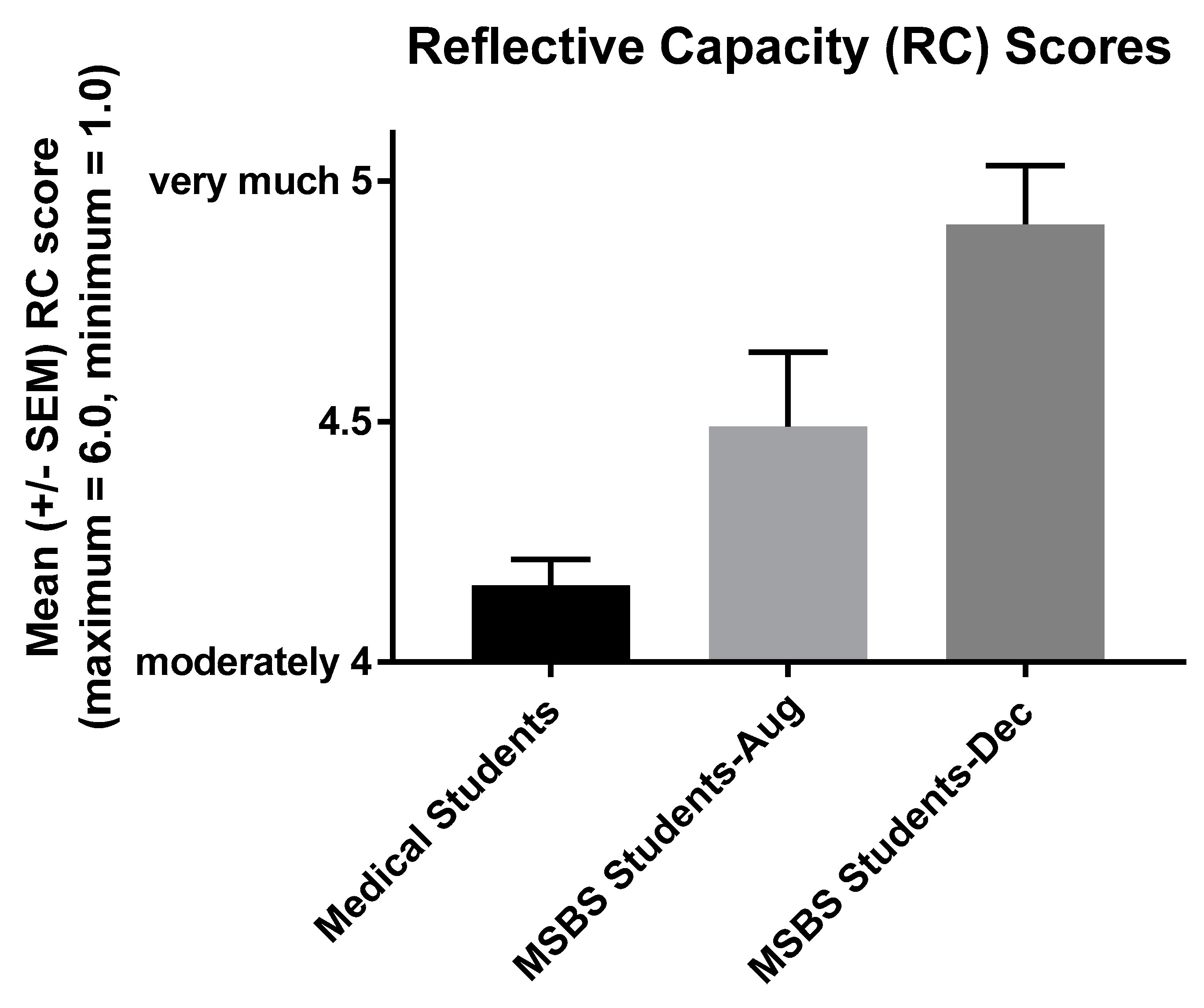
2.4. Measurement of Development by Students in the Second Cohort
2.5. Use of the Third Cohort to Determine Whether Reflective Capacity Correlates with Cognitive Empathy
2.6. Statistical Analysis
3. Results
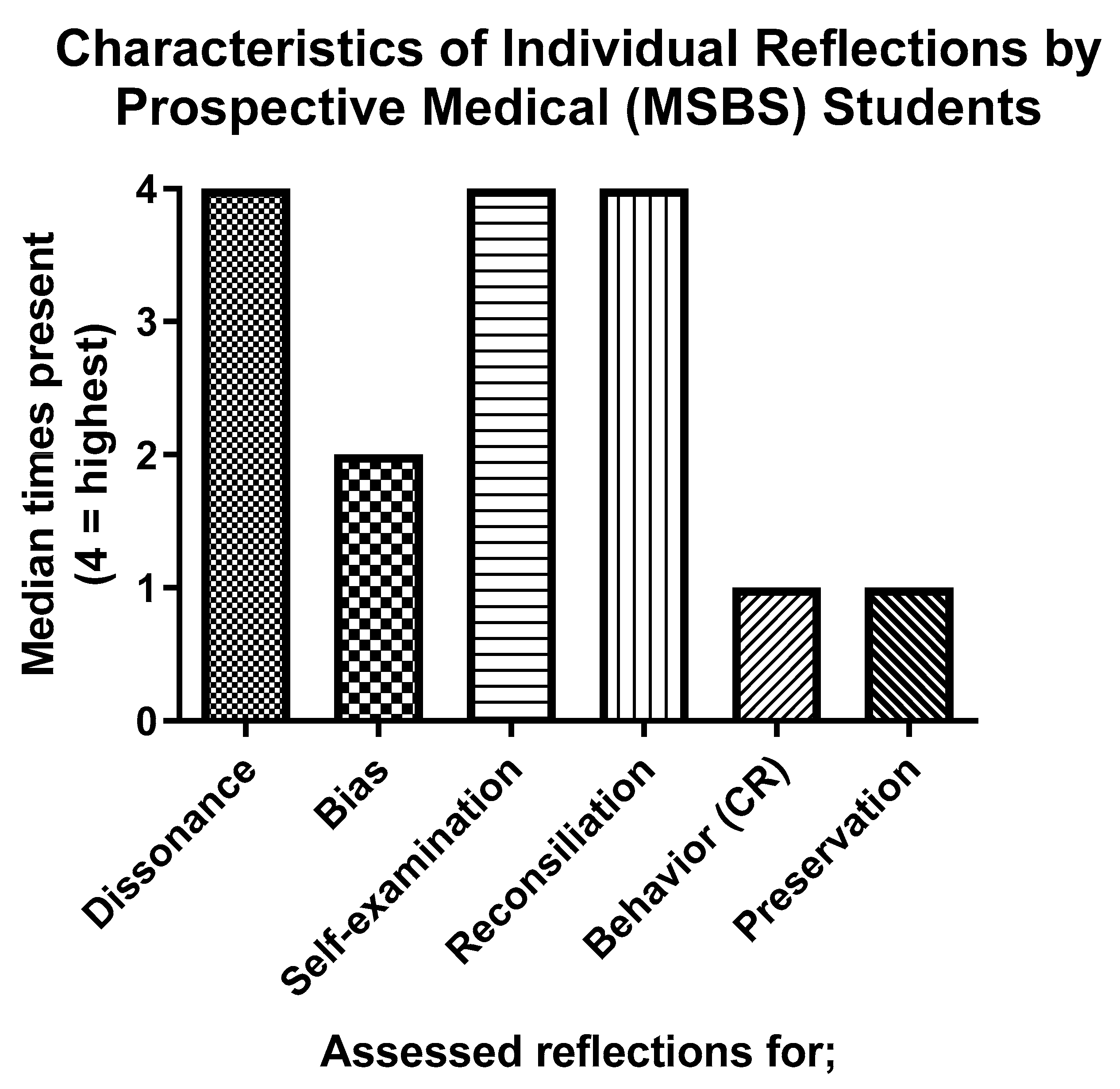
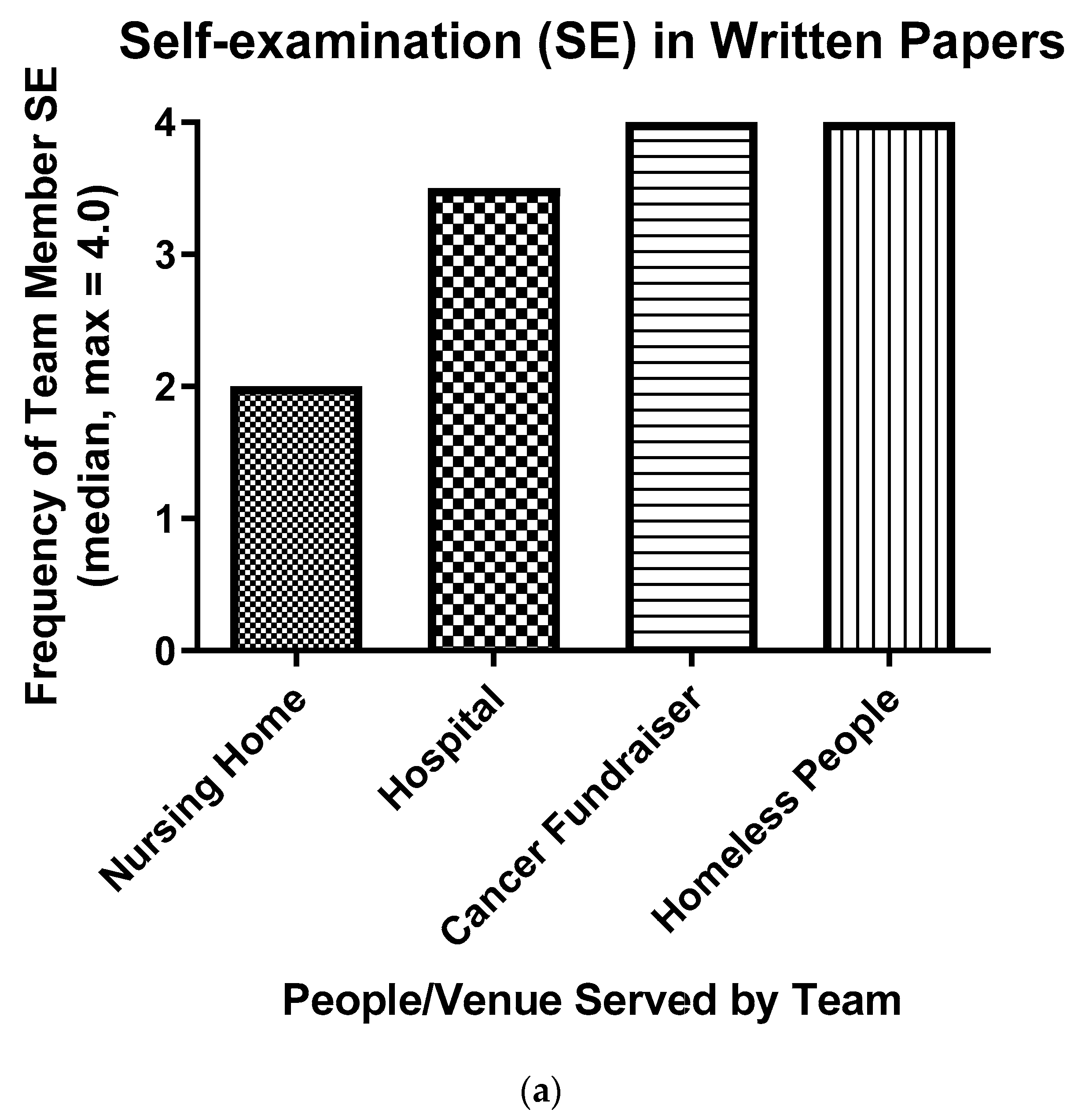
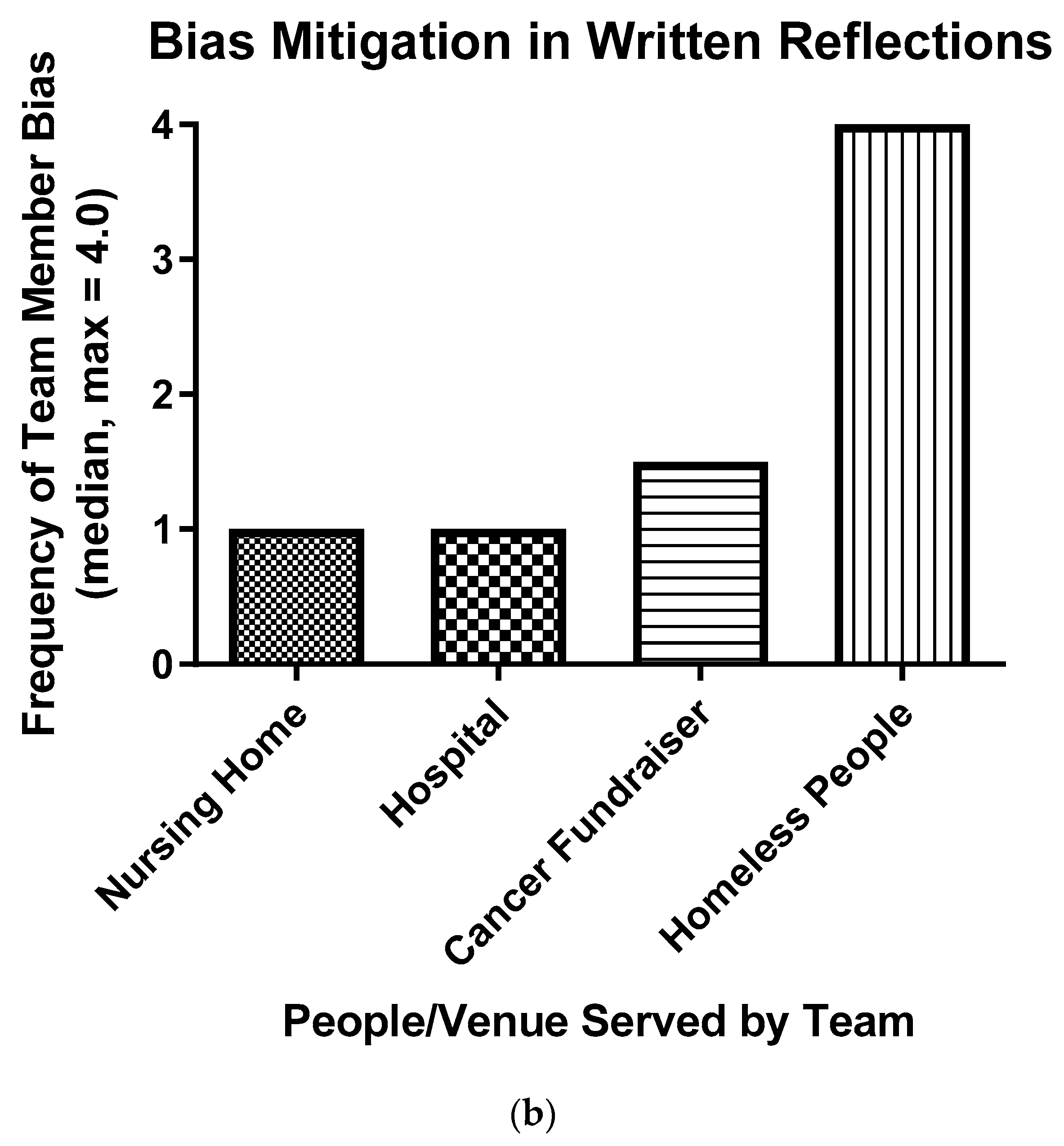
3.1. Dissonance and Bias in the First Cohort
My last reflection, I investigated my anxiety for our volunteer project selection. How, I wanted to work in the hospital compared to the homeless shelter. I wrote about some reasons for these emotions but during this week’s group meeting, I think I pin-pointed where my anxiety stems from…
I have noticed that just walking sixteenth street mall gives me the same feelings that I first experienced that day. I feel scared and intimidated by the thought of even walking by homeless [people]. No matter what color, I have even noticed that I try to cross the street before making any sort of eye contact with them.
I know that my experiences were traumatic, however I cannot let that one experience completely change my view of the entire homeless population…
…Panic, fear, and dread overwhelmed me, and I could not control it. So, instead I embraced it. For the entirety of the drive I simply did not fight the thought but instead tried to feel them out and rationalize how ‘off the wall’ they were and made a pact with myself that after this drive these feelings will be let go. And, that is what I did.
The moment I stepped out of the car, I felt anew. My feelings of dread turned to excitement. An ease came over my mind that is hard to put into words. However, walking in the door, (I know this sounds cliché) but a new man. As part of my job, I stood by the front door and greeted every person that walked through the door that day. It was a true joy, as I no longer felt any fear or anxiety that was gripping me in the car as every person I interacted with during my hours treated me with the utmost respect…
3.2. Value of Students’ Unique Team Experiences
…during this week’s group meeting, I think I pin-pointed where my anxiety stems from… (Appendix A).
4. Discussion
4.1. Impact of Dissonance in the First Cohort
4.2. Team Support Also Likely Fostered Self-Examination and CR
4.3. How Do Results with the Second Cohort Complement and Support Conclusions Regarding the First?
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. (One Student’s Second Reflection)
Appendix B. (the Same Student’s Third Reflection)
References
- Mongrain, M.; Chin, J.M.; Shapira, L.B. Practicing compassion increases happiness and self-esteem. J. Happiness Stud. 2011, 12, 963–981. [Google Scholar] [CrossRef]
- Curry, O.S.; Rowland, L.A.; Van Lissa, C.J.; Zlotowitz, S.; McAlaney, J.; Whitehouse, H. Happy to help? A systematic review and meta-analysis of the effects of performing acts of kindness on the well-being of the actor. J. Exp. Soc. Psychol. 2018, 76, 320–329. [Google Scholar] [CrossRef]
- American Board of Internal Medicine. Project Professionalism; American Board of Internal Medicine Communications: Philadelphia, PA, USA, 1999. [Google Scholar]
- Cohen, J.J. Linking professionalism to humanism: What it means, why it matters. Acad. Med. 2007, 82, 1029–1032. [Google Scholar] [CrossRef] [PubMed]
- Wear, D.; Nixon, L.L. Literary inquiry and professional development in medicine: Against abstractions. Perspect. Biol. Med. 2002, 45, 104–124. [Google Scholar] [CrossRef]
- Dewey, J. How We Think; Prometheus Books: Buffalo, NY, USA, 1933. [Google Scholar]
- Thompson, B.M.; Teal, C.R.; Rogers, J.C.; Paterniti, D.A.; Haidet, P. Ideals, activities, dissonance, and processing: A conceptual model to guide educators’ efforts to stimulate student reflection. Acad. Med. 2010, 85, 902–908. [Google Scholar] [CrossRef]
- Van Winkle, L.J.; Burdick, P.; Bjork, B.C.; Chandar, N.; Green, J.M.; Lynch, S.M.; La Salle, S.; Viselli, S.M.; Robson, C. Critical thinking and reflection on community service for a medical biochemistry course raise students’ empathy, patient-centered orientation, and examination scores. Med. Sci. Educ. 2014, 24, 279–290. [Google Scholar] [CrossRef]
- Hernandez, R.A.; Haidet, P.; Gill, A.C.; Teal, C.R. Fostering students’ reflection about bias in healthcare: Cognitive dissonance and the role of personal and normative standards. Med. Teach. 2013, 35, e1082–e1089. [Google Scholar] [CrossRef]
- Barkan, R.; Ayal, S.; Ariely, D. Ethical dissonance, justifications, and moral behavior. Cur. Opin. Psychol. 2015, 6, 157–161. [Google Scholar] [CrossRef]
- Hall, W.J.; Chapman, M.V.; Lee, K.M.; Merino, Y.M.; Thomas, T.W.; Payne, B.K.; Eng, E.; Day, S.H.; Coyne-Beasley, T. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: A systematic review. Am. J. Public Health 2015, 105, e60–e76. [Google Scholar] [CrossRef]
- Michaelsen, L.K.; Knight, A.B.; Fink, L.D. Team-Based Learning: A Transformative Use of Small Groups in College Teaching; Stylus Publishing: Sterling, VA, USA, 2004. [Google Scholar]
- Schmidt, H.G.; Rotgans, J.I.; Rajalingam, P.; Low-Beer, N. Knowledge reconsolidation: A psychological foundation for team-based learning. Acad. Med. 2019. [Google Scholar] [CrossRef]
- Van Winkle, L.J.; Robson, C.; Chandar, N.; Green, J.M.; Viselli, S.M.; Donovan, K. Use of poems written by physicians to elicit critical reflection by students in a medical biochemistry course. J. Learn. Arts 2011, 7, n1. [Google Scholar] [CrossRef]
- Van Winkle, L.J.; Chandar, N.; Green, J.M.; Lynch, S.M.; Viselli, S.M.; Burdick, P. Does critical reflection by biochemistry learning teams foster patient-centered beliefs among medical students? Med. Sci. Educ. 2011, 21, 158–168. [Google Scholar] [CrossRef]
- Van Winkle, L.J.; Cornell, S.; Fjortoft, N.; Bjork, B.C.; Chandar, N.; Green, J.M.; La Salle, S.; Viselli, S.M.; Burdick, P.; Lynch, S.M. Critical thinking and reflection exercises in a biochemistry course to improve prospective health professions students’ attitudes toward physician-pharmacist collaboration. Am. J. Pharm. Educ. 2013, 77, 169. [Google Scholar] [CrossRef] [PubMed]
- Van Winkle, L.J.; La Salle, S.; Richardson, L.; Bjork, B.C.; Burdick, P.; Chandar, N.; Green, J.M.; Lynch, S.M.; Robson, C.; Viselli, S.M. Challenging medical students to confront their biases: A case study simulation approach. Med. Sci. Educ. 2013, 23, 217–224. [Google Scholar] [CrossRef]
- Hojat, M. Empathy in Health Professions Education and Patient Care; Springer International Publishing: New York, NY, USA, 2016. [Google Scholar]
- Nguyen, Q.D.; Fernandez, N.; Karsenti, T.; Charlin, B. What is reflection? A conceptual analysis of major definitions and a proposal of a five-component model. Med. Educ. 2014, 48, 1176–1189. [Google Scholar] [CrossRef] [PubMed]
- Priddis, L.; Rogers, S.L. Development of the reflective practice questionnaire: Preliminary findings. Reflective Pract. 2018, 19, 89–104. [Google Scholar] [CrossRef]
- Rogers, S.L.; Priddis, L.E.; Michels, N.; Tieman, M.; Van Winkle, L.J. Applications of the reflective practice questionnaire in medical education. BMC Med. Educ. 2019, 19, 47. [Google Scholar] [CrossRef]
- Rosenthal, R.; Rubin, D.B. A simple, general purpose display of magnitude of experimental effect. J. Educ. Psychol. 1982, 74, 166–169. [Google Scholar] [CrossRef]
- Alda, A. If I Understood You, Would I Have This Look on My Face?: My Adventures in the Art and Science of Relating and Communicating; Random House Trade Paperbacks: New York, NY, USA, 2018. [Google Scholar]
- Boud, D.; Walker, D. Promoting reflection in professional courses: The challenge of context. Stud. High. Educ. 1998, 23, 191–206. [Google Scholar] [CrossRef]
- FitzGerald, C.; Hurst, S. Implicit bias in healthcare professionals: A systematic review. BMC Med. Ethics 2017, 18, 19. [Google Scholar] [CrossRef]
- Maxfield, C.M.; Thorpe, M.P.; Desser, T.S.; Heitkamp, D.E.; Hull, N.C.; Johnson, K.S.; Koontz, N.A.; Mlady, G.W.; Welch, T.J.; Grimm, L.J. Bias in radiology resident selection: Do we discriminate against the obese and unattractive? Acad. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Salles, A.; Awad, M.; Goldin, L.; Krus, K.; Lee, J.V.; Schwabe, M.T.; Lai, C.K. Estimating implicit and explicit gender bias among health care professionals and surgeons. JAMA Netw. Open. 2019, 2, e196545. [Google Scholar] [CrossRef] [PubMed]
- De Vries, J.; Timmins, F. Care erosion in hospitals: Problems in reflective nursing practice and the role of cognitive dissonance. Nurse Educ. Today 2016, 38, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Rolfe, G. Rethinking reflective education: What would Dewey have done? Nurse Educ. Today 2014, 34, 1179–1183. [Google Scholar] [CrossRef] [PubMed]
- Bice, A.A. Cognitive dissonance and pediatric procedural pain management: A concept clarification. Pain Manag. Nurs. 2018, 19, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Lacerenza, C.N.; Marlow, S.L.; Tannenbaum, S.I.; Salas, E. Team development interventions: Evidence-based approaches for improving teamwork. Am. Psychol. 2018, 73, 517–531. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 Strongly Disagree | 2 Disagree | 3 Somewhat Disagree | 4 Neither Agree/Disagree | 5 Somewhat Agree | 6 Agree | 7 Strongly Agree | Median * | |
|---|---|---|---|---|---|---|---|---|
| 1. | Having a team service-learning project in Medical Humanities was very engaging. | 6.0 | ||||||
| 1 (3.8%) * | 0 | 0 | 2 (7.7%) | 5 (19.2%) | 9 (34.6%) | 9 (34.6%) | ||
| 2. | I would have been better off on another team in Medical Humanities. | 1.0 | ||||||
| 16 (61.5%) | 7 (26.9%) | 2 (7.7%) | 0 | 1 (3.8%) * | 0 | 0 | ||
| 3. | Next year, Medical Humanities should continue to expect teams of MSBS students to perform service-learning projects and to write reflections on their experiences with the projects. | 6.0 | ||||||
| 1 (3.8%) * | 0 | 0 | 1 (3.8%) | 2 (7.7%) | 10 (38.5%) | 12 (46.2%) | ||
| 4. | All things considered, I could not have been assigned to a stronger team in Medical Humanities. | 6.0 | ||||||
| 0 | 1 (3.8%) | 2 (7.7%) | 1 (3.8%) | 3 (11.5%) | 9 (34.6%) | 10 (38.5%) | ||
| 5. | I gained very little from our service-learning project and written reflections on the project. | 2.0 | ||||||
| 12 (46.2%) | 10 (38.5%) | 2 (7.7%) | 1 (3.8%) | 0 | 0 | 1 (3.8%) * | ||
| 6. | Medical Humanities should continue to use team-based learning in future courses. | 7.0 | ||||||
| 0 | 0 | 0 | 1 (3.8%) * | 2 (7.7%) | 8 (30.8%) | 15 (57.7%) | ||
| 7. | Writing reflections on our service-learning project fostered my professional development. | 6.0 | ||||||
| 1 (3.8%) * | 0 | 0 | 0 | 6 (23.1%) | 10 (38.5%) | 9 (34.6%) | ||
| 8. | Encounters with people in our service-learning project caused me to study for all of my courses with more interest than likely would have occurred without the project. | 4.0 | ||||||
| 3 (11.5%) | 0 | 4 (15.4%) | 9 (34.6%) | 4 (15.4%) | 4 (15.4%) | 2 (7.7%) | ||
| 9. | Encounters with people in our service-learning project will help me to be engaged with people regardless of the setting or disposition of the person. | 6.0 | ||||||
| 1 (3.8%) * | 0 | 0 | 0 | 6 (23.1%) | 8 (30.8%) | 11 (42.3%) | ||
| 10. | Encounters with people/venues in our service-learning project helped me to see my potential biases toward people/venues more clearly. | 6.0 | ||||||
| 1 (3.8%) * | 0 | 0 | 0 | 6 (23.1%) | 10 (38.5%) | 9 (34.6%) | ||
| 11. | Of what biases did you become aware during encounters with people/venues in your service-learning project? | |||||||
| Hypothesis | 1. Service-learning experiences will be associated with dissonance, self-examination, bias mitigation, dissonance reconciliation, and compassionate behavior. | 2. Students will express positive attitudes toward their teams, community service, and recognizing/mitigating their implicit biases in association with team service-learning experiences. | 3. Reflections on team service-learning experiences will be accompanied by increases in students’ reflective capacity. | 4. Students’ reflective capacity scores will correlate positively with their cognitive empathy scores (a component of compassion). |
| Cohort | One | One and two | Two | Three |
| Time of study | Aug–Dec 2017 | Aug–Dec 2017/18 | Aug–Dec 2018 | Aug 2019 |
| Method of data collection | Analysis of written reflections | Survey of attitudes | Reflective practice questionnaire (RPQ) | RPQ and Jefferson Scale of Empathy |
| Independent variable | Reflection on service-learning | Team reflection on service-learning | Reflection on service-learning | Reflective capacity scores |
| Dependent variable(s) | Reported dissonance, self-examination, bias mitigation, dissonance reconciliation, and compassionate behavior | Reported attitudes toward their teams, community service, and recognizing/mitigating their implicit biases | Reflective capacity scores | Cognitive empathy scores |
| Statistical analysis | Kruskal–Wallis | Kruskal–Wallis | ANOVA, t-test | Pearson r values |
| Nature of Negative Bias | Number of Times Expressed |
|---|---|
| Homeless People | 5 |
| Culture/Race | 5 |
| Older People | 3 |
| Attitudes of Other People | 3 |
| Gender | 2 |
| People with Serious Diseases | 2 |
| Other Healthcare Providers | 2 |
| Nonclinical Settings for Service | 1 |
| Hospital Volunteering | 1 |
| Socioeconomic Status | 1 |
| RC | DfI | CG | CC | Unc | SiP | JS | |
|---|---|---|---|---|---|---|---|
| RC | 1 | ||||||
| DfI | 0.13 | 1 | |||||
| CG | 0.28 | −0.14 | 1 | ||||
| CC | 0.62 *** | −0.13 | 0.58 ** | 1 | |||
| Unc | −0.33 | 0.23 | −0.51 ** | −0.62 *** | 1 | ||
| SiP | −0.27 | 0.01 | −0.32 | −0.42 * | 0.68 *** | 1 | |
| JS | 0.57 ** | 0.31 | 0.24 | 0.51 ** | −0.55 ** | −0.48 * | 1 |
| RC | DfI | CG | CC | Unc | SiP | JS | |
|---|---|---|---|---|---|---|---|
| RC | 1 | ||||||
| DfI | 0.17 | 1 | |||||
| CG | 0.42 * | −0.29 | 1 | ||||
| CC | 0.70 *** | −0.08 | 0.43 * | 1 | |||
| Unc | 0.22 | 0.55 ** | −0.04 | 0.00 | 1 | ||
| SiP | 0.29 | 0.39 * | −0.07 | 0.12 | 0.84 *** | 1 | |
| JS | 0.20 | −0.09 | 0.06 | 0.17 | −0.52 ** | −0.50 ** | 1 |
| Hypothesis | 1. Team service-learning experiences will be associated with dissonance, self-examination, bias mitigation, dissonance reconciliation, and compassionate behavior. | 2. Students will express positive attitudes toward their teams, community service, and recognizing/mitigating their implicit biases in association with team service-learning experiences. | 3. Reflections on team service-learning experiences will be accompanied by increases in students’ reflective capacity. | 4. Students’ reflective capacity (RC) scores will correlate positively with their cognitive empathy scores (a component of compassion). |
| Cohort | One | One and two | Two | Three |
| Conclusion 1 | All but one of 26 students reported dissonance, self-examination, bias mitigation, dissonance reconciliation, and compassionate behavior. | Virtually all 52 students overwhelmingly expressed positive attitudes toward their team. | Students’ mean reflective capacity, self-appraisal, and reflection-on-action scores increased significantly. | Students’ RC, self-appraisal, and reflection-on-action scores correlated strongly with their cognitive empathy scores. |
| Conclusion 2 | Teams differed somewhat in their frequency of self-examination and bias mitigation. | Virtually all students mitigated their biases and reported professional development. | Students refocused their uncertainty and stress from negative associations with confidence to positive associations with desire for improvement. | |
| Conclusion 3 | The vast majority of students agreed that their service-learning project was very engaging. | Reflective capacity went from negative to positive associations with uncertainty and stress. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horst, A.; Schwartz, B.D.; Fisher, J.A.; Michels, N.; Van Winkle, L.J. Selecting and Performing Service-Learning in a Team-Based Learning Format Fosters Dissonance, Reflective Capacity, Self-Examination, Bias Mitigation, and Compassionate Behavior in Prospective Medical Students. Int. J. Environ. Res. Public Health 2019, 16, 3926. https://doi.org/10.3390/ijerph16203926
Horst A, Schwartz BD, Fisher JA, Michels N, Van Winkle LJ. Selecting and Performing Service-Learning in a Team-Based Learning Format Fosters Dissonance, Reflective Capacity, Self-Examination, Bias Mitigation, and Compassionate Behavior in Prospective Medical Students. International Journal of Environmental Research and Public Health. 2019; 16(20):3926. https://doi.org/10.3390/ijerph16203926
Chicago/Turabian StyleHorst, Alexis, Brian D. Schwartz, Jenifer A. Fisher, Nicole Michels, and Lon J. Van Winkle. 2019. "Selecting and Performing Service-Learning in a Team-Based Learning Format Fosters Dissonance, Reflective Capacity, Self-Examination, Bias Mitigation, and Compassionate Behavior in Prospective Medical Students" International Journal of Environmental Research and Public Health 16, no. 20: 3926. https://doi.org/10.3390/ijerph16203926