Association between Health Literacy and Subgroups of Health Risk Behaviors among Chinese Adolescents in Six Cities: A Study Using Regression Mixture Modeling



Abstract
1. Introduction
2. Methods
2.1. Study Participants and Procedures
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Prevalence of HRBs
3.2. Class Enumeration
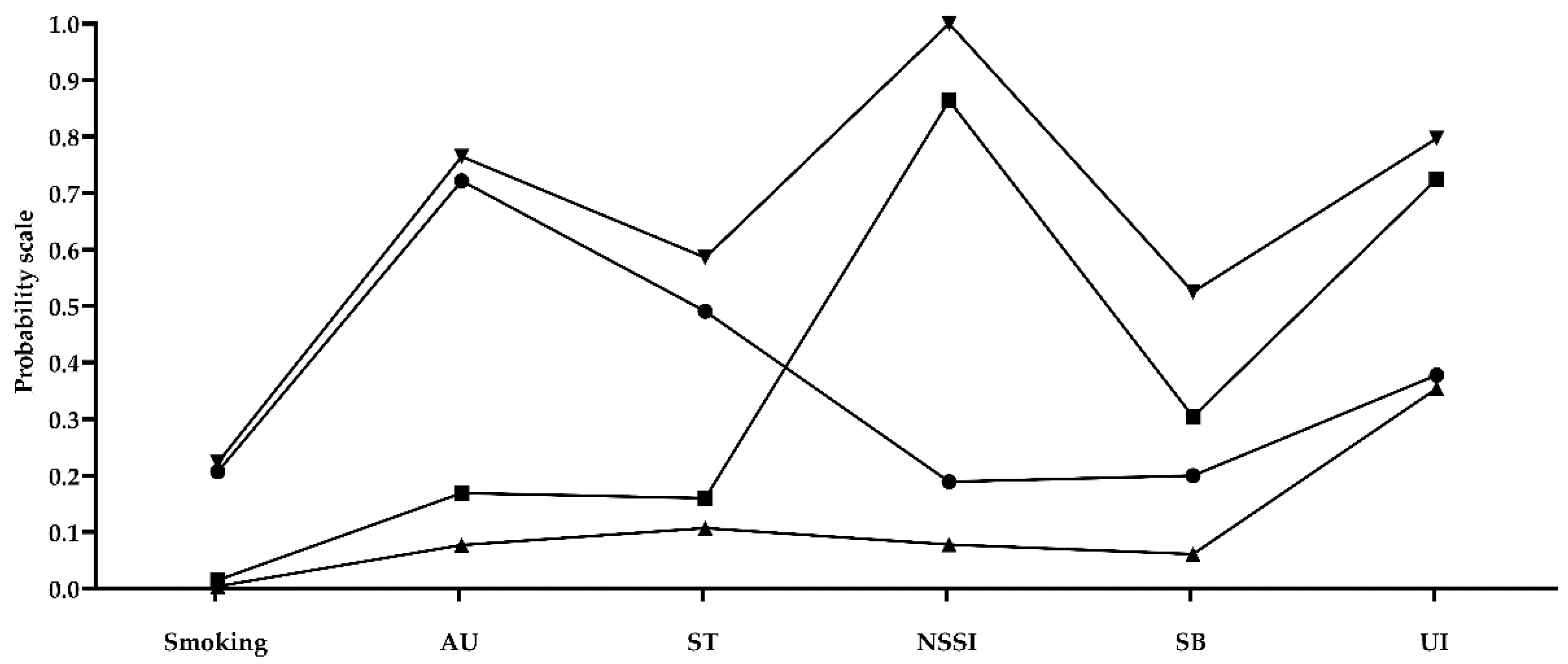
3.3. Characteristics of the Final Four Class Model
3.4. Effect of HL on the Best-Fitting Latent Classes of HRBs
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| HRBs | Health risk behaviors |
| AU | Alcohol use |
| ST | Screen time |
| NSSI | Non-suicidal self-injury |
| SB | Suicidal behavior |
| UI | Unintentional injury |
| HL | Health literacy |
| RMM | Regression mixture modeling |
| LCA | Latent class analysis |
| df | Degrees of freedom |
| AIC | Akaike Information Criteria |
| BIC | Bayesian Information Criteria |
| aBIC | Adjusted Bayesian Information Criteria |
| LMR-LRT | Lo-Mendell-Rubin Likelihood Ratio |
| BLRT | Bootstrapped Likelihood Ratio Tests |
| OR | Odds ratio |
| CI | Confidence interval |
Appendix A

{kind=link}
| Variable | Measures |
|---|---|
| Health literacy | Chinese Adolescent Interactive Health Literacy Questionnaire |
| Current smoking | During the past 30 days, how many days did you smoke cigarettes? |
| Current AU | During the past 30 days, on how many days did you have at least one drink of alcohol? |
| ST | The average hours on weekdays spent on playing games or doing things unrelated to study on the computer every day |
| Non-suicidal self-injury | Adolescent Non-suicidal Self-injury Assessment Questionnaire |
| SB | Have you ever thought about killing yourself in the past 12 months? Have you ever made a plan to kill yourself in the past 12 months? Have you ever tried to kill yourself in the past 12 months? |
| UI | Children and teenager injury monitoring method. UI are divided into road traffic incident, crush, falling and tripping, scratches, puncture or cut, bites and pricks, explosive impact, enclosed anoxic space, drowning, electric shock, chemical or other substances poisoning and other twelve injuries. |
References
- Kickbusch, I.; Nutbeam, D. Health Promotion Glossary; World Health Organization: Geneva, Switzerland, 1998; Available online: https://www.who.int/healthpromotion/about/HPR%20Glossary%201998.pdf (accessed on 22 August 2019).
- Ji, C.Y. Adolescent health risk behavior monitoring: An important frontier of school health work. Chin. J. Sch. Health 2009, 30, 99–105. (In Chinese) [Google Scholar]
- Arrazola, R.A.; Ahluwalia, I.B.; Pun, E.; Garcia de Quevedo, I.; Babb, S.; Armour, B.S. Current tobacco smoking and desire to quit smoking among students aged 13–15 Years-Global Youth Tobacco Survey, 61 ountries, 2012–2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 533–537. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Status Report on Alcohol and Health 2018; World Health Organization: Geneva, Switzerland, 2018; Available online: https://apps.who.int/iris/bitstream/handle/10665/274603/9789241565639-eng.pdf?ua=1 (accessed on 22 August 2019).
- Constance, W.R.; Trickett, S.A.K.; Morgan, S.K. Adolescent light cigarette smoking patterns and adult cigarette smoking. Adv. Epidemiol. 2016, 2016, 1–7. [Google Scholar] [CrossRef]
- Latvala, A.; Rose, R.J.; Pulkkinen, L.; Dick, D.M.; Korhonen, T.; Kaprio, J. Drinking, smoking, and educational achievement: Cross-lagged associations from adolescence to adulthood. Drug Alcohol Depend. 2014, 137, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Hancox, R.J.; Milne, B.J.; Poulton, R. Association between child and adolescent television viewing and adult health: A longitudinal birth cohort study. Lancet 2004, 364, 257–262. [Google Scholar] [CrossRef]
- Swannell, S.V.; Martin, G.E.; Page, A.; Hasking, P.; St John, N.J. Prevalence of non-suicidal self-injury in nonclinical samples: Systematic review, meta-analysis and meta-regression. Suicide Life Threat. Behav. 2014, 44, 273–303. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- World Health Organization. Suicided; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.who.int/en/news-room/fact-sheets/detail/suicide (accessed on 29 September 2019).
- World Health Organization. Health for World’s Adolescents: A Second Chance in the Second Decade: Summary; World Health Organization: Geneva, Switzerland, 2014; Available online: https://apps.who.int/iris/handle/10665/112750 (accessed on 29 September 2019).
- Meader, N.; King, K.; Moe-Byrne, T.; Wright, K.; Graham, H.; Petticrew, M.; Power, C.; White, M.; Sowden, A.J. A systematic review on the clustering and co-occurrence of multiple risk behaviours. BMC Public Health 2016, 16, 657. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D.R.; Wall, M.M.; Haines, J.I.; Story, M.T.; Sherwood, N.E.; van den Berg, P.A. Shared risk and protective factors for overweight and disordered eating in adolescents. Am. J. Prev. Med. 2007, 33, 359–369. [Google Scholar] [CrossRef] [PubMed]
- Pasch, K.E.; Nelson, M.C.; Lytle, L.A.; Moe, S.G.; Perry, C.L. Adoption of risk-related factors through early adolescence: Associations with weight status and implications for causal mechanisms. J. Adolesc. Health 2008, 43, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Beydoun, M.A.; Wang, Y. Is sleep duration associated with childhood obesity? A systematic review and meta-analysis. Obesity 2008, 16, 265–274. [Google Scholar] [CrossRef]
- Krokstad, S.; Ding, D.; Grunseit, A.C.; Sund, E.R.; Holmen, T.L.; Rangul, V.; Bauman, A. Multiple lifestyle behaviours and mortality, findings from a large population-based Norwegian cohort study-The HUNT Study. BMC Public Health 2017, 17, 58. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.J.; Prochaska, J.O. A Review of multiple health behavior change interventions for primary prevention. Am. J. Lifestyle Med. 2011, 5. [Google Scholar] [CrossRef] [PubMed]
- Loef, M.; Walach, H. The combined effects of healthy lifestyle behaviors on all cause mortality: A systematic review and meta-analysis. Prev. Med. 2012, 55, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Laska, M.N.; Pasch, K.E.; Lust, K.; Story, M.; Ehlinger, E. Latent class analysis of lifestyle characteristics and health risk behaviors among college youth. Prev. Sci. 2009, 10, 376–386. [Google Scholar] [CrossRef] [PubMed]
- Hair, E.C.; Park, M.J.; Ling, T.J.; Moore, K.A. Risky behaviors in late adolescence: Co-occurrence, predictors, and consequences. J. Adolesc. Health 2009, 45, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, C.J.; Childs, K.K. Adolescent risk behavior subgroups: An empirical assessment. J. Youth Adolesc. 2010, 39, 541–562. [Google Scholar] [CrossRef] [PubMed]
- Nutbeam, D. The evolving concept of health literacy. Soc. Sci. Med. 2008, 67, 2072–2078. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Library of Medicine. Health Literacy; U.S. National Library of Medicine: Bethesda, MD, USA, 2018. Available online: https://medlineplus.gov/healthliteracy.html (accessed on 22 August 2019).
- Manganello, J.A. Health literacy and adolescents: A framework and agenda for future research. Health Educ. Res. 2008, 23, 840–847. [Google Scholar] [CrossRef]
- Reyna, V.F.; Farley, F. Risk and rationality in adolescent decision making: Implications for theory, practice, and public policy. Psychol. Sci. Public Interest 2006, 7, 1–44. [Google Scholar] [CrossRef]
- Chang, F.C.; Miao, N.F.; Lee, C.M.; Chen, P.H.; Chiu, C.H.; Lee, S.C. The association of media exposure and media literacy with adolescent alcohol and tobacco use. J. Health Psychol. 2016, 21, 513–525. [Google Scholar] [CrossRef]
- Zhang, S.C.; Yang, R.; Wan, Y.H.; Ma, S.S.; Tao, F.B. Association of the health literacy and the incidence of injuries among Chinese middle school students in five provinces. Zhonghua Yu Fang Yi Xue Za Zhi 2018, 52, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.C.; Yang, R.; Li, D.L.; Wang, J.; Wan, Y.H.; Xu, S.J.; Xu, H.L.; Ma, S.S.; Wang, W.; Zeng, H.J.; et al. Interactive effects between health literacy and mobile phone dependence as well as its relation with unintentional injuries in middle school students. Zhonghua Liu Xing Bing Xue Za Zhi 2018, 39, 1549–1554. [Google Scholar] [CrossRef] [PubMed]
- Nurius, P.S.; Macy, R.J. Heterogeneity among violence-exposed women: Applying person-oriented research methods. J. Interpers. Violence 2008, 23, 389–415. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.C.; Wan, Y.H.; Tao, S.M.; Chen, J.; Tao, F.B. Reliability and construct validity of the adolescent interactive health literacy questionnaire. Chin. J. Sch. Health 2014, 35, 332–336, (In Chinese with English abstract). [Google Scholar] [CrossRef]
- Kann, L.; Mcmanus, T.; Harris, W.A.; Shanklin, S.L.; Flint, K.H.; Queen, B.; Lowry, R.; Chyen, D.; Whittle, L.; Thornton, J.; et al. Youth Risk Behavior Surveillance-United States, 2017. MMWR Surveill. Summ. 2018, 67, 28–43. Available online: https://www.cdc.gov/mmwr/volumes/67/ss/ss6708a1.htm (accessed on 29 September 2019).
- Brener, N.D.; Kann, L.; Shanklin, S.; Kinchen, S.; Eaton, D.K.; Hawkins, J.; Flint, K.H. Methodology of the youth risk behavior surveillance system—2013. MMWR Recomm. Rep. 2013, 62, 1–20. [Google Scholar] [PubMed]
- Brener, N.D.; Billy, J.O.G.; Grady, W.R. Assessment of factors affecting the validity of self-reported health-risk behavior among adolescents: Evidence from the scientific literature. J. Adolesc. Health 2003, 33, 436–457. [Google Scholar] [CrossRef]
- American Academy of Pediatries. Committee on Public Education. American Academy of Pediatrics: Children, adolescents, and television. Pediatrics 2001, 107, 423–426. [Google Scholar] [CrossRef]
- Wu, X.; Tao, S.; Zhang, Y.; Zhang, S.; Tao, F. Low physical activity and high screen time can increase the risks of mental health problems and poor sleep quality among Chinese college students. PLoS ONE 2015, 10, e0119607. [Google Scholar] [CrossRef] [PubMed]
- Cao, H.; Qian, Q.; Weng, T.; Yuan, C.; Sun, Y.; Wang, H.; Tao, F. Screen time, physical activity and mental health among urban adolescents in China. Prev. Med. 2011, 53, 316–320. [Google Scholar] [CrossRef]
- Wan, Y.H.; Liu, W.; Hao, J.H.; Tao, F.B. Development and evaluation on reliability and validity of adolescent non-suicidal self-injury assessment questionnaire. Chin. J. Sch. Health 2018, 39, 170–173, (In Chinese with English abstract). [Google Scholar] [CrossRef]
- Wan, Y.H.; Xu, S.J.; Chen, J.; Hu, C.L.; Tao, F.B. Longitudinal effects of psychological symptoms on non-suicidal self-injury: A difference between adolescents and young adults in China. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 237–247. [Google Scholar] [CrossRef] [PubMed]
- National Health Commission of the People’s Republic of China. Methods for Injury Surveillance among Child and Adolescent GB/T 31180 -2014[S]; National Health Commission of the People’s Republic of China: Beijing, China, 2015.
- Collins, L.M.; Lanza, S.T. Latent Class and Latent Transition Analysis: With Applications in the Social, Behavioral, and Health Sciences; Wiley: New York, NY, USA, 2010. [Google Scholar]
- Lamont, A.E.; Vermunt, J.K.; Van Horn, M.L. Regression mixture models: Does modeling the covariance between independent variables and latent classes improve the results? Multivar. Behav. Res. 2016, 51, 35–52. [Google Scholar] [CrossRef] [PubMed]
- Vermunt, J.K. Latent class modeling with covariates: Two improved three-step approaches. Political Anal. 2010, 18, 450–469. [Google Scholar] [CrossRef]
- Clark, S.L.; Muthén, B. Relating Latent Class Analysis Results to Variables not Included in the Analysis. Available online: https://www.researchgate.net/publication/237346694_Relating_Latent_Class_Analysis_Results_to_Variables_not_Included_in_the_Analysis (accessed on 22 August 2019).
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 7th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2012; Available online: https://www.statmodel.com/download/usersguide/Mplus%20user%20guide%20Ver_7_r3_web.pdf (accessed on 22 August 2019).
- Carragher, N.; Adamson, G.; Bunting, B.; McCann, S. Subtypes of depression in a nationally representative sample. J. Affect. Disord. 2009, 113, 88–99. [Google Scholar] [CrossRef] [PubMed]
- Nagin, D. Group-Based Modeling of Development; Harvard University: Cambridge, MA, USA, 2005. [Google Scholar]
- Hamza, C.A.; Stewart, S.L.; Willoughby, T. Examining the link between nonsuicidal self-injury and suicidal behavior: A review of the literature and an integrated model. Clin. Psychol. Rev. 2012, 32, 482–495. [Google Scholar] [CrossRef] [PubMed]
- Nakar, O.; Brunner, R.; Schilling, O.; Chanen, A.; Fischer, G.; Parzer, P.; Carli, V.; Wasserman, D.; Sarchiapone, M.; Wasserman, C.; et al. Developmental trajectories of self-injurious behavior, suicidal behavior and substance misuse and their association with adolescent borderline personality. Pathol. J. Affect. Disord. 2016, 197, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Cicchetti, D.; Rogosch, F. Equifinality and mutifinality in developmental psychopathology. Dev. Psychopathol. 1996, 8, 597–600. [Google Scholar] [CrossRef]
- Levin-Zamir, D.; Lemish, D.; Gofin, R. Media health literacy (MHL): Development and measurement of the concept among adolescents. Health Educ. Res. 2011, 26, 323–335. [Google Scholar] [CrossRef]
- Chang, L.C. Health literacy, self-reported status and health promoting behaviours for adolescents in Taiwan. J. Clin. Nurs. 2011, 20, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.L.; Teufel, J.A.; Birch, D.A. Early adolescents perceptions of health and health literacy. J. Sch. Health 2007, 77, 7–15. [Google Scholar] [CrossRef]
- Weekes, C.V. African Americans and health literacy: A systematic review. ABNF J. 2012, 23, 76–80. [Google Scholar] [PubMed]

| Variable | Total Sample (%) |
|---|---|
| Gender | |
| Male | 10,990 (48.6) |
| Female | 11,638 (51.4) |
| Grade | |
| Middle school | 11,993 (53.0) |
| High school | 10,635 (47.0) |
| Registered residence | |
| Rural | 10,882 (48.1) |
| Urban | 11,746 (51.9) |
| Any siblings | |
| Yes | 12,908 (57.0) |
| No | 9720 (43.0) |
| Accommodation type | |
| Boarding student | 11,320 (50.0) |
| Commuting student | 11,308 (50.0) |
| Father’s educational level a | |
| <High school degree | 13,006 (57.5) |
| ≥High school degree | 9424 (41.6) |
| Mother’s educational level b | |
| <High school degree | 14,335 (63.4) |
| ≥High school degree | 8105 (35.8) |
| Self-reported family economy | |
| Bad | 3240 (14.3) |
| General | 16,345 (72.2) |
| Good | 3043 (13.4) |
| Statistic | 2 Classes | 3 Classes | 4 Classes | 5 Classes |
|---|---|---|---|---|
| df | 50 | 43 | 36 | 29 |
| AIC | 120,896.912 | 119,991.261 | 119,844.588 | 119,822.264 |
| BIC | 121,001.263 | 120,151.800 | 120,061.315 | 120,095.180 |
| aBIC | 120,959.949 | 120,088.241 | 119,975.510 | 119,987.129 |
| LMR-LRT | <0.001 | <0.001 | <0.001 | 0.0592 |
| BLRT | <0.001 | <0.001 | <0.001 | <0.001 |
| Entropy | 0.549 | 0.725 | 0.692 | 0.579 |
| Classification probability | 0.28730 0.71270 | 0.24032 0.04698 0.71270 | 0.28774 0.04472 0.64089 0.02665 | 0.19299 0.28774 0.01003 0.47795 0.03129 |
| Variable | Low-Risk Class | Moderate-Risk Class 1 (Smoking/AU/ST) | Moderate-Risk Class 2 (NSSI/SB/UI) | High-Risk Class (Smoking/AU/ST/NSSI/SB/UI) |
|---|---|---|---|---|
| Adjusted OR (95% CI) | Adjusted OR (95% CI) | Adjusted OR (95% CI) | Adjusted OR (95% CI) | |
| HL | ref. | 0.990 (0.982–0.998) ** | 0.981 (0.979–0.983) *** | 0.965 (0.959–0.970) *** |
| Age | ref. | 1.327 (1.242–1.419) *** | 0.838 (0.814–0.863) *** | 0.978 (0.908–1.054) |
| Gender | ||||
| Male | ref. | ref. | ref. | ref. |
| Female | ref. | 0.183 (0.137–0.245) *** | 0.725 (0.662–0.795) *** | 0.359 (0.265–0.487) *** |
| Registered residence | ||||
| Rural | ref. | ref. | ref. | ref. |
| Urban | ref. | 1.176 (0.920–1.502) | 0.900 (0.816–0.993) ** | 0.843 (0.629–1.129) |
| Household structure | ||||
| Only child | ref. | ref. | ref. | ref. |
| More than one child | ref. | 0.940 (0.753–1.173) | 0.957 (0.871–1.051) | 1.157 (0.885–1.514) |
| Accommodation type | ||||
| Boarding student | ref. | ref. | ref. | ref. |
| Commuting student | ref. | 1.687 (1.323–2.151)*** | 0.736 (0.665–0.815) *** | 1.636 (1.207–2.216) ** |
| Father’s educational level | ||||
| <High school degree | ref. | ref. | ref. | ref. |
| ≥High school degree | ref. | 1.313 (1.035–1.664)** | 0.977 (0.874–1.093) | 1.461 (1.084–1.968) ** |
| Mother’s educational level | ||||
| < High school degree | ref. | ref. | ref. | ref. |
| ≥ High school degree | ref. | 0.945 (0.735–1.214) | 0.994 (0.885–1.116) | 0.951 (0.691–1.309) |
| Self-reported family economy (per level change) | ref. | 1.015 (0.795–1.297) | 0.791 (0.715–0.874) *** | 1.752 (1.234–2.489) ** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, R.; Li, D.; Hu, J.; Tian, R.; Wan, Y.; Tao, F.; Fang, J.; Zhang, S. Association between Health Literacy and Subgroups of Health Risk Behaviors among Chinese Adolescents in Six Cities: A Study Using Regression Mixture Modeling. Int. J. Environ. Res. Public Health 2019, 16, 3680. https://doi.org/10.3390/ijerph16193680
Yang R, Li D, Hu J, Tian R, Wan Y, Tao F, Fang J, Zhang S. Association between Health Literacy and Subgroups of Health Risk Behaviors among Chinese Adolescents in Six Cities: A Study Using Regression Mixture Modeling. International Journal of Environmental Research and Public Health. 2019; 16(19):3680. https://doi.org/10.3390/ijerph16193680
Chicago/Turabian StyleYang, Rong, Danlin Li, Jie Hu, Run Tian, Yuhui Wan, Fangbiao Tao, Jun Fang, and Shichen Zhang. 2019. "Association between Health Literacy and Subgroups of Health Risk Behaviors among Chinese Adolescents in Six Cities: A Study Using Regression Mixture Modeling" International Journal of Environmental Research and Public Health 16, no. 19: 3680. https://doi.org/10.3390/ijerph16193680
APA StyleYang, R., Li, D., Hu, J., Tian, R., Wan, Y., Tao, F., Fang, J., & Zhang, S. (2019). Association between Health Literacy and Subgroups of Health Risk Behaviors among Chinese Adolescents in Six Cities: A Study Using Regression Mixture Modeling. International Journal of Environmental Research and Public Health, 16(19), 3680. https://doi.org/10.3390/ijerph16193680