Non-Surgical Treatment of Periodontal Disease in a Pregnant Caucasian Women Population: Adverse Pregnancy Outcomes of a Randomized Clinical Trial

Abstract
1. Introduction
2. Material and Methods
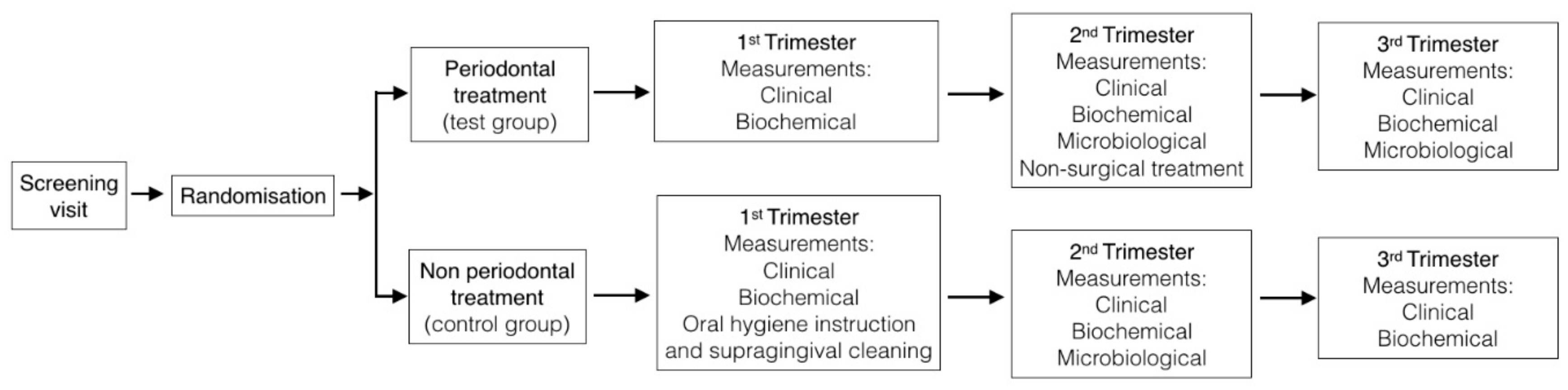
2.1. Study Design
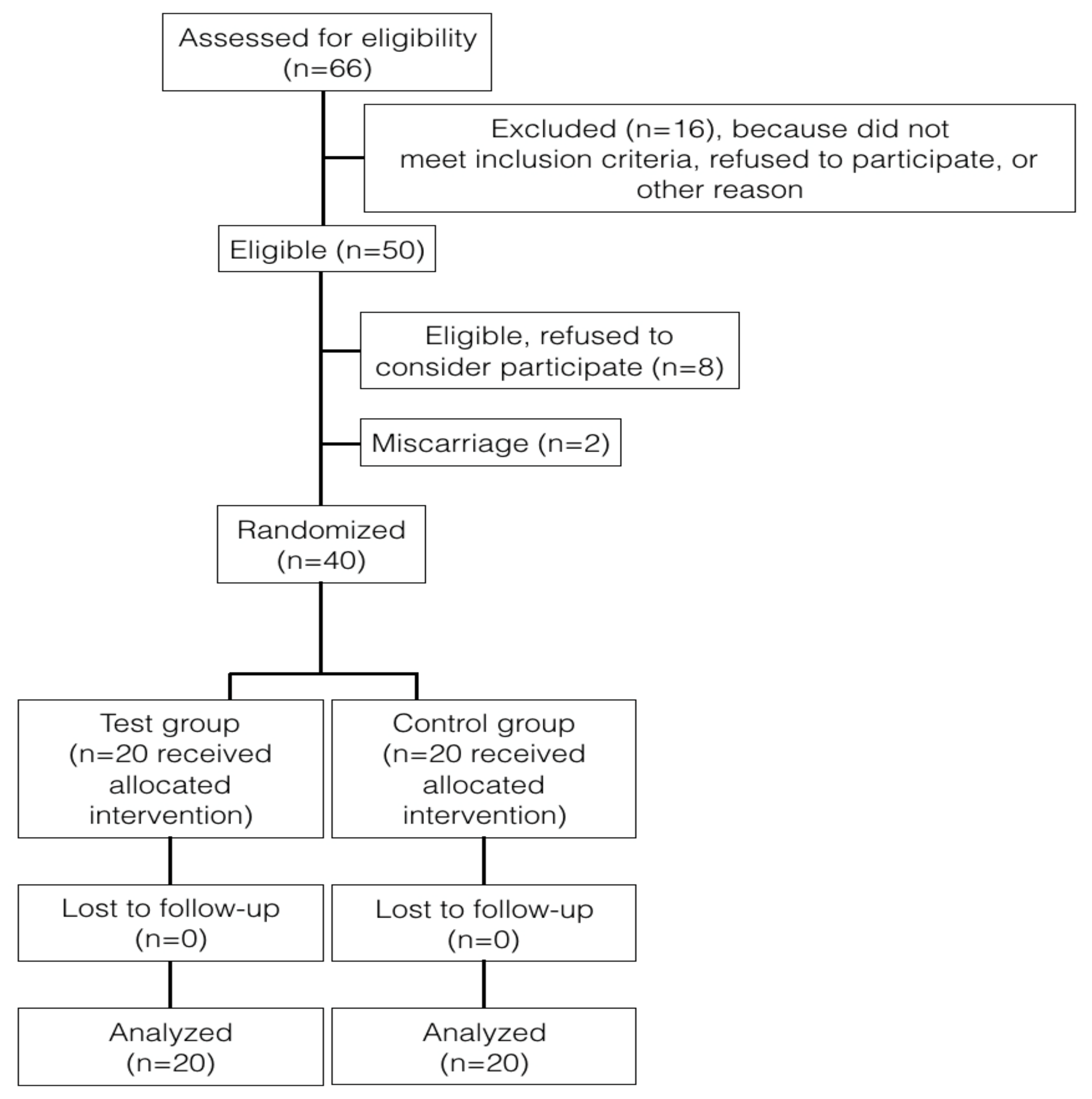
2.2. Study Population
2.3. Inclusion/Exclusion Criteria
2.4. Maternal Characteristics
2.5. Periodontal Measurements
- Interdental CAL was detectable at ≥2 non-adjacent teeth, or
- Buccal or oral CAL ≥3 mm with pocketing ≥3 mm was detectable at ≥2 teeth but the observed CAL could not be ascribed to non-periodontitis-related causes such as: (1) gingival recession of traumatic origin; (2) dental caries extending in the cervical area of the tooth; (3) presence of CAL on the distal aspect of a second molar and associated with malposition or extraction of a third molar; (4) an endodontic lesion draining through the marginal periodontium; and (5) the occurrence of a vertical root fracture.
2.6. Biochemical Variables
2.7. Microbiological Variables
2.8. Periodontal Treatment
2.9. Outcomes
2.10. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mathews, T.J.; Menacker, F.; MacDorman, M.F. Infant mortality statistics from the 2001 period linked birth/infant death data set. Natl. Vital Stat. Rep. 2003, 52, 1–28. [Google Scholar] [PubMed]
- Chang, H.H.; Larson, J.; Blencowe, H.; Spong, C.Y.; Howson, C.P.; Cairns-Smith, S.; Lackritz, E.M.; Lee, S.K.; Mason, E.; Serazin, A.C.; et al. Preventing preterm births: Analysis of trends and potential reductions with interventions in 39 countries with very high human development index. Lancet 2013, 381, 223–234. [Google Scholar] [CrossRef]
- Blencowe, H.; Cousens, S.; Jassir, F.B.; Say, L.; Chou, D.; Mathers, C.; Hogan, D.; Shiekh, S.; Qureshi, Z.U.; You, D.; et al. National, regional, and worldwide estimates of stillbirth rates in 2015, with trends from 2000: A systematic analysis. Lancet Glob. Health 2016, 4, e98–e108. [Google Scholar] [CrossRef]
- Purisch, S.E.; Gyamfi-Bannerman, C. Epidemiology of preterm birth. Semin. Perinatol. 2017, 41, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Vogel, J.P.; Chawanpaiboon, S.; Moller, A.-B.; Watananirun, K.; Bonet, M.; Lumbiganon, P. The global epidemiology of preterm birth. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 52, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Kornman, K.S.; Page, R.C.; Tonetti, M.S. The host response to the microbial challenge in periodontitis: Assembling the players. Periodontology 2000, 14, 33–53. [Google Scholar] [CrossRef]
- Carta, G.; Persia, G.; Falciglia, K.; Iovenitti, P. Periodontal disease and poor obstetrical outcome. Clin. Exp. Obstet. Gynecol. 2004, 31, 47–49. [Google Scholar]
- Lopez, N.J.; Da Silva, I.; Ipinza, J.; Gutiérrez, J. Periodontal Therapy Reduces the Rate of Preterm Low Birth Weight in Women with Pregnancy-Associated Gingivitis. J. Periodontol. 2005, 76, 2144–2153. [Google Scholar] [CrossRef]
- Santa Cruz, I.; Herrera, D.; Martin, C.; Herrero, A.; Sanz, M. Association between periodontal status and pre-term and/or low-birth weight in Spain: Clinical and microbiological parameters. J. Periodontal Res. 2013, 48, 443–451. [Google Scholar] [CrossRef]
- Sanz, M.; Kornman, K. Working group 3 of joint EFP/AAP workshop. Periodontitis and adverse pregnancy outcomes: Consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Clin. Periodontol. 2013, 84, S164–S169. [Google Scholar] [CrossRef]
- Gürsoy, M.; Könönen, E.; Gursoy, U.K.; Tervahartiala, T.; Pajukanta, R.; Sorsa, T. Periodontal Status and Neutrophilic Enzyme Levels in Gingival Crevicular Fluid during Pregnancy and Postpartum. J. Periodontol. 2010, 81, 1790–1796. [Google Scholar] [CrossRef] [PubMed]
- Madianos, P.N.; Bobetsis, Y.A.; Offenbacher, S. Adverse pregnancy outcomes (APOs) and periodontal disease: Pathogenic mechanisms. J. Clin. Periodontol. 2013, 40, 170–180. [Google Scholar] [CrossRef] [PubMed]
- Minckwitz, G.; Grischke, E.-M.; Schwab, S.; Hettinger, S.; Loibl, S.; Aulmann, M.; Kaufmann, M. Predictive value of serum interleukin-6 and -8 levels in preterm labor or rupture of the membranes. Acta Obstet. Gynecol. Scand. 2000, 79, 667–672. [Google Scholar]
- Gücer, F.; Balkanli-Kaplan, P.; Yüksel, M.; A Yüce, M.; Türe, M.; Yardim, T. Maternal serum tumor necrosis factor-alpha in patients with preterm labor. J. Reprod. Med. 2001, 46, 232–236. [Google Scholar] [PubMed]
- Pitiphat, W.; Gillman, M.W.; Joshipura, K.J.; Williams, P.L.; Douglass, C.W.; Rich-Edwards, J.W. Plasma C-reactive protein in early pregnancy and preterm delivery. Am. J. Epidemiol. 2005, 162, 1108–1113. [Google Scholar] [CrossRef] [PubMed]
- Agueda, A.; Ramón, J.; Manau, C.; Guerrero, A.; Echeverria, J. Periodontal disease as a risk factor for adverse pregnancy outcomes: A prospective cohort study. J. Clin. Periodontol. 2008, 35, 16–22. [Google Scholar] [CrossRef]
- Offenbacher, S.; Boggess, K.A.; Murtha, A.P.; Jared, H.L.; Lieff, S.; McKaig, R.G.; Mauriello, S.M.; Moss, K.L.; Beck, J.D. Progressive Periodontal Disease and Risk of Very Preterm Delivery. Obstet. Gynecol. 2006, 107, 29–36. [Google Scholar] [CrossRef]
- Rakoto-Alson, S.; Tenenbaum, H.; Davideau, J.-L. Periodontal Diseases, Preterm Births, and Low Birth Weight: Findings from a Homogeneous Cohort of Women in Madagascar. J. Periodontol. 2010, 81, 205–213. [Google Scholar] [CrossRef]
- Matevosyan, N.R. Periodontal disease and perinatal outcomes. Arch. Gynecol. Obstet. 2011, 283, 675–686. [Google Scholar] [CrossRef]
- Vergnes, J.N.; Sixou, M. Preterm low birth weight and maternal periodontal status: A meta-analysis. Am. J. Obstet. Gynecol. 2007, 196, 135.e1–135.e7. [Google Scholar] [CrossRef]
- Puertas, A.; Magan-Fernandez, A.; Blanc, V.; Revelles, L.; O´Valle, F.; Pozo, E.; León, R.; Mesa, F. Association of periodontitis with preterm birth and low birth weight: A comprehensive review. J. Materm. Fetal Neonatal Med. 2018, 31, 597–602. [Google Scholar] [CrossRef] [PubMed]
- Teshome, A.; Yitayeh, A. Relationship between periodontal disease and preterm low birth weight: Systematic review. Pan Afr. Med. J. 2016, 24, 215. [Google Scholar] [CrossRef] [PubMed]
- Jeffcoat, M.; Parry, S.; Sammel, M.; Clothier, B.; Catlin, A.; Macones, G. Periodontal infection and preterm birth: Successful periodontal therapy reduces the risk of preterm birth. BJOG Int. J. Obstet. Gynaecol. 2011, 118, 635–636. [Google Scholar] [CrossRef]
- Offenbacher, S.; Lin, D.; Strauss, R.; McKaig, R.; Irving, J.; Barros, S.P.; Moss, K.; Barrow, D.A.; Hefti, A.; Beck, J.D. Effects of Periodontal Therapy During Pregnancy on Periodontal Status, Biologic Parameters, and Pregnancy Outcomes: A Pilot Study. J. Periodontol. 2006, 77, 2011–2024. [Google Scholar] [CrossRef] [PubMed]
- Radnai, M.; Pal, A.; Novák, T.; Urban, E.; Eller, J.; Gorzo, I. Benefits of Periodontal Therapy When Preterm Birth Threatens. J. Dent. Res. 2009, 88, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Tarannum, F.; Faizuddin, M. Effect of Periodontal Therapy on Pregnancy Outcome in Women Affected by Periodontitis. J. Periodontol. 2007, 78, 2095–2103. [Google Scholar] [CrossRef] [PubMed]
- Macones, G.A.; Parry, S.; Nelson, D.B.; Strauss, J.F.; Ludmir, J.; Cohen, A.W.; Stamilio, D.M.; Appleby, D.; Clothier, B.; Sammel, M.D.; et al. Treatment of localized periodontal disease in pregnancy does not reduce the occurrence of preterm birth: Results from the Periodontal Infections and Prematurity Study (PIPS). Am. J. Obstet. Gynecol. 2010, 202, 147.e1–147.e8. [Google Scholar] [CrossRef]
- Michalowicz, B.S.; Hodges, J.S.; DiAngelis, A.J.; Lupo, V.R.; Novak, M.J.; Ferguson, J.E.; Buchanan, W.; Bofill, J.; Papapanou, P.N.; Mitchell, D.A.; et al. Treatment of Periodontal Disease and the Risk of Preterm Birth. N. Engl. J. Med. 2006, 355, 1885–1894. [Google Scholar] [CrossRef]
- Merchant, A.T.; Sutherland, M.W.; Liu, J.; Pitiphat, W.; Dasanayake, A. Periodontal treatment among mothers with mild to moderate periodontal disease and preterm birth: Reanalysis of OPT trial data accounting for selective survival. Int. J. Epidemiol. 2018, 47, 1670–1678. [Google Scholar] [CrossRef]
- Offenbacher, S.; Beck, J.D.; Jared, H.L.; Mauriello, S.M.; Mendoza, L.C.; Couper, D.J.; Stewart, D.D.; Murtha, A.P.; Cochran, D.L.; Dudley, D.J.; et al. Effects of periodontal therapy on rate of preterm delivery: A randomized controlled trial. Obstet. Gynecol. 2009, 114, 551–559. [Google Scholar] [CrossRef]
- Oliveira, A.M.; de Oliveira, P.A.; Cota, L.O.; Magalhaes, C.S.; Moreira, A.N.; Costa, F.O. Periodontal therapy and risk for adverse pregnancy outcomes. Clin. Oral. Investig. 2011, 15, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Kinane, D.; Bouchard, P. On behalf of group E of the European Workshop on Periodontology Periodontal diseases and health: Consensus Report of the Sixth European Workshop on Periodontology. J. Clin. Periodontol. 2008, 35, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Pannuti, C.M.; Guglielmetti, M.R.; Chambrone, L.A. Evidence grade associating periodontitis with preterm birth and/or low birth weight: II. A systematic review of randomized trials evaluating the effects of periodontal treatment. J. Clin. Periodontol. 2011, 38, 902–914. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S162–S170. [Google Scholar] [CrossRef] [PubMed]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar] [PubMed]
- Syed, S.A.; Loesche, W.J. Survival of Human Dental Plaque Flora in Various Transport Media. Appl. Microbiol. 1972, 24, 638–644. [Google Scholar] [PubMed]
- Alsina, M.; Olle, E.; Frías, J. Improved, Low-Cost Selective Culture Medium for Actinobacillus actinomycetemcomitans. J. Clin. Microbiol. 2001, 39, 509–513. [Google Scholar] [CrossRef]
- Michalowicz, B.S.; Novak, M.J.; Hodges, J.S.; DiAngelis, A.; Buchanan, W.; Papapanou, P.N.; Mitchell, D.A.; Ferguson, J.E.; Lupo, V.; Bofill, J.; et al. Serum inflammatory mediators in pregnancy: Changes after periodontal treatment and association with pregnancy outcomes. J. Periodontol. 2009, 80, 1731–1741. [Google Scholar] [CrossRef]
- Baccaglini, L. A meta-analysis of randomized controlled trials shows no evidence that periodontal treatment during pregnancy prevents adverse pregnancy outcomes. J. Am. Dent. Assoc. 2011, 142, 1192–1193. [Google Scholar] [CrossRef]
- Kaur, M.; Geisinger, M.L.; Geurs, N.C.; Griffin, R.; Vassilopoulos, P.J.; Vermeulen, L.; Haigh, S.; Reddy, M.S. Effect of intensive oral hygiene regimen during pregnancy on periodontal health, cytokine levels, and pregnancy outcomes: A pilot study. J. Periodontol. 2014, 85, 1684–1692. [Google Scholar] [CrossRef]
- Ide, M.; McPartlin, D.; Coward, P.; Crook, M.; Lumb, P.; Wilson, R. Effect of treatment of chronic periodontitis on levels of serum markers of acute-phase inflammatory and vascular responses. J. Clin. Periodontol. 2003, 30, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Fiorini, T.; Susin, C.; da Rocha, J.M.; Weidlich, P.; Vianna, P.; Moreira, C.H.; Bogo Chies, J.A.; Rösing, C.K.; Oppermann, R.V. Effect of nonsurgical periodontal therapy on serum and gingival crevicular fluid cytokine levels during pregnancy and postpartum. J. Periodontal Res. 2013, 48, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Novak, M.J.; Novak, K.F.; Hodges, J.S.; Kirakodu, S.; Govindaswami, M.; DiAngelis, A.; Buchanan, W.; Papapanou, P.N.; Michalowicz, B.S. Periodontal Bacterial Profiles in Pregnant Women: Response to Treatment and Associations with Birth Outcomes in the Obstetrics and Periodontal Therapy (OPT) Study. J. Periodontol. 2008, 79, 1870–1879. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Martínez, R.E.; Moreno-Castillo, D.F.; Loyola-Rodríguez, J.P.; Sánchez-Medrano, A.G.; Miguel-Hernández, J.H.; Olvera-Delgado, J.H.; Domínguez-Pérez, R.A. Association between periodontitis, periodontopathogens and preterm birth: Is it real? Arch. Gynecol. Obstet. 2016, 294, 47–54. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| - | Test Group (n = 20) | Control Group (n = 20) |
|---|---|---|
| Age (years, mean ± SD) | 32.14 ± 4.27 | 32.25 ± 4.21 |
| Body Mass Index (Kg/m2, mean ± SD) | 24.89 ± 5.68 | 24.73 ± 3.71 |
| Education level (n, %) | ||
| Primary | 30% | 35% |
| Secondary | 40% | 35% |
| University | 30% | 30% |
| Residence (n, %) | ||
| Rural | 75% | 90% |
| Urban | 25% | 10% |
| Marital status (n, %) | ||
| Single | 0% | 5% |
| Common-law partner | 40% | 40% |
| Married | 60% | 55% |
| Previous spontaneous abortion (n, %) | ||
| No spontaneous abortion | 95% | 95% |
| One spontaneous abortion | 5% | 5% |
| Previous pregnancy (n, %) | ||
| No previous pregnancy | 80% | 85% |
| One previous pregnancy | 20% | 15% |
| Clinical Parameters | 1st Trimester | 2nd Trimester | 3rd Trimester | |
|---|---|---|---|---|
| Number of teeth (mean ± SD) | Test group (n = 20) | 26.95 ± 1.21 | 26.95 ± 1.21 | 26.95 ± 1.21 |
| Control group (n = 20) | 26.32 ± 2.77 | 26.32 ± 2.77 | 26.32 ± 2.77 | |
| p = 0.32; CI (−1.91–0.64) | p = 0.32; CI (−1.91–0.64) | p = 0.32; CI (−1.91–0.64) | ||
| Plaque index (mean ± SD) | Test group (n = 20) | 41.39 ± 18.27 | 40.21 ± 18.54 | 21.17 ± 15.59 |
| Control group (n = 20) | 32.96 ± 20.08 | 34.36 ± 18.68 | 35.68 ± 17.64 | |
| p = 0.54; CI (−15.69–8.34) | p = 0.32; CI (−17.61–5.91) | p = 0.01; CI (3.99–25.01) | ||
| Bleeding on probing (mean ± SD) | Test group (n = 20) | 48.30 ± 14.80 | 54.57 ± 18.61 | 27.88 ± 15.29 |
| Control group (n = 20) | 32.78 ± 14.92 | 42.59 ± 18.00 | 43.21 ± 20.77 | |
| p = 0.01; CI (−23.81–−7.89) | p = 0.04; CI (−23.55–−0.40) | p = 0.01; CI (3.83–26.81) | ||
| Probing depth ≤3 mm (%, mean ± SD) | Test group (n = 20) | 57.38 ± 21.28 | 52.42 ± 21.43 | 70.34 ± 17.46 |
| Control group (n = 20) | 74.15 ± 12.20 | 70.00 ± 14.54 | 65.22 ± 16.81 | |
| p = 0.01; CI (3.03–22.92) | p = 0.01; CI (5.95–29.21) | p = 0.35; CI (−15.95–5.72) | ||
| Probing depth 4–5 mm (%, mean ± SD) | Test group (n = 20) | 35.64 ± 17.34 | 39.88 ± 19.12 | 24.39 ± 12.30 |
| Control group (n = 20) | 24.69 ± 10.36 | 26.11 ± 10.67 | 29.87 ± 12.96 | |
| p = 0.09; CI (−15.77–1.10) | p = 0.01; CI (−23.62–−3.92) | p = 0.17; CI (−2.50–13.46) | ||
| Probing depth ≥6 (%, mean ± SD) | Test group (n = 20) | 6.90 ± 9.59 | 7.69 ± 10.55 | 5.31 ± 8.87 |
| Control group (n = 20) | 3.68 ± 1.17 | 4.27 ± 6.95 | 4.77 ± 6.08 | |
| p = 0.01; CI (−9.35–−1.72) | p = 0.23; CI (−9.10–2.25) | p = 0.82; CI (−5.37–4.29) | ||
| Clinical attachment loss ≥3 mm (mm, mean ± SD) | Test group (n = 20) | 0.74 ± 0.38 | 0.77 ± 0.46 | 0.69 ± 0.57 |
| Control group (n = 20) | 0.42 ± 0.27 | 0.50 ± 0.32 | 0.60 ± 0.35 | |
| p = 0.01; CI (−0.46–−0.11) | p = 0.03; CI (−0.53–−0.18) | p = 0.56; CI (−0.39–0.21) | ||
| Biochemical Parameters | 1st Trimester | 2nd Trimester | 3rd Trimester | |
|---|---|---|---|---|
| Fibrinogen (mg/dL, mean ± SD) | Test group (n = 20) | 365.06 ± 55.12 | 387.06 ± 49.25 | 447.65 ± 52.27 |
| Control group (n = 20) | 352.39 ± 58.17 | 401.50 ± 75.88 | 463.61 ± 89.47 | |
| p = 0.54; CI (−42.28–22.47) | p = 0.28; CI (−18.43–61.76) | p = 0.42; CI (−29.59–68.79) | ||
| TNF-α (pg/mL, mean ± SD) | Test group (n = 20) | 7.80 ± 3.87 | 7.17 ± 3.20 | 6.97 ± 2.65 |
| Control group (n = 20) | 7.00 ± 3.47 | 7.80 ± 3.61 | 7.50 ± 2.72 | |
| p = 0.99; CI (−2.07–2.06) | p = 0.61; CI (−1.52–2.55) | p = 0.50; CI (−1.08–2.15) | ||
| Interleukin-6 (pg/mL, mean ± SD) | Test group (n = 20) | 3.04 ± 2.56 | 2.54 ± 1.33 | 2.84 ± 1.42 |
| Control group (n = 20) | 3.01 ± 2.26 | 3.05 ± 2.49 | 2.36 ± 0.97 | |
| p = 0.63; CI (−1.55–0.95) | p = 0.43; CI (−0.70–1.61) | p = 0.33; CI (−1.06–0.37) | ||
| Interleukin-8 (pg/mL, mean ± SD) | Test group (n = 20) | 14.94 ± 19.09 | 10.24 ± 6.27 | 11.41 ± 10.26 |
| Control group (n = 20) | 8.61 ± 4.55 | 19.94 ± 20.84 | 10.89 ± 8.21 | |
| p = 0.54; CI (−9.55–5.13) | p = 0.27; CI (−4.64–16.25) | p = 0.80; CI (−6.15–4.76) | ||
| Microbiological Variables | - | 2nd Trimester | 3rd Trimester | p |
|---|---|---|---|---|
| Aggregatibacter actinomycetemcomitans (%, mean ± SD) | Test (n = 20) | 0.98 ± 3.00 | 0 ± 0 | 0.15; CI (−2.33_0.38) |
| Control (n = 20) | 0.30 ± 2.83 | 0.28 ± 3.12 | 0.20; CI (−2.51_0.57) | |
| Porphyromonas gingivalis (%, mean ± SD) | Test (n = 20) | 22.97 ± 25.62 | 3.63 ± 5.14 | 0.01; CI (−31.17–−7.51) |
| Control (n = 20) | 23.38 ± 18.23 | 24.59 ± 19.22 | 0.21; CI (−20.94–5.01) | |
| Prevotella intermedia (%, mean ± SD) | Test (n = 20) | 2.60 ± 1.20 | 0 ± 0 | <0.01; CI (−3.14–−2.06) |
| Control (n = 20) | 2.79 ± 1.42 | 2.54 ± 1.55 | 0.59; CI (−2.44–1.45) | |
| Tannerella forsythia (%, mean ± SD) | Test (n = 20) | 3.30 ± 4.67 | 0 ± 0 | <0.01; CI (−5.41–−1.19) |
| Control (n = 20) | 4.69 ± 1.28 | 4.80 ± 2.34 | 0.64; CI (−4.56–2.89) | |
| Parvimona micra (%, mean ± SD) | Test (n = 20) | 0.73 ± 1.65 | 0 ± 0 | 0.06; CI (−1.48–0.02) |
| Control (n = 20) | 1.68 ± 3.72 | 1.86 ± 3.02 | 0.85; CI (−1.11–1.33) | |
| Campylobacter rectus (%, mean ± SD) | Test (n = 20) | 1.72 ± 7.33 | 0 ± 0 | 0.30; CI (−5.04–1.60) |
| Control (n = 20) | 1.32 ± 3.72 | 1.33 ± 3.83 | 0.32; CI (−5.56–1.93) | |
| Fusobacterium nucleatum (%, mean ± SD) | Test (n = 20) | 1.96 ± 2.68 | 0 ± 0 | <0.01; CI (−3.17–−0.75) |
| Control (n = 20) | 2.18 ± 1.82 | 2.20 ± 2.30 | 0.64; CI (−4.56–2.89) | |
| Capnocytophaga (%, mean ± SD) | Test (n = 20) | 0.06 ± 0.26 | 0 ± 0 | 0.32; CI (−0.18–0.06) |
| Control (n = 20) | 0.10 ± 0.25 | 0.12 ± 0.34 | 0.19; CI (−0.16–0.03) | |
| Eikenella corrondens (%, mean ± SD) | Test (n = 20) | 0.40 ± 1.13 | 0 ± 0 | 0.12; CI (−0.91–0.11) |
| Control (n = 20) | 1.31 ± 1.91 | 1.22 ± 1.23 | 0.59; CI (−1.39–2.35) | |
| Eubacterium spp. (%, mean ± SD) | Test (n = 20) | 0 ± 0 | 0 ± 0 | - |
| Control (n = 20) | 0 ± 0 | 0 ± 0 | - |
| Primary Outcomes | Test Group (n = 20) | Control Group (n = 20) | Total | |
|---|---|---|---|---|
| Preterm Birth † | No | 19 | 17 | 36 |
| Yes | 1 | 3 | 4 | |
| Total | 20 | 20 | 40 | |
| Low Birth Weight ‡ | No | 19 | 17 | 36 |
| Yes | 1 | 3 | 4 | |
| Total | 20 | 20 | 40 | |
| Variable | Type III Sum of Squares | p |
|---|---|---|
| Age | 0.206 | NS |
| Body Mass Index | 0.181 | NS |
| Treatment | 1.194 | NS |
| Variable | Type III Sum of Squares | p |
|---|---|---|
| Age | 91,359.53 | NS |
| Body Mass Index | 1555.01 | NS |
| Treatment | 685,694.99 | NS |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caneiro-Queija, L.; López-Carral, J.; Martin-Lancharro, P.; Limeres-Posse, J.; Diz-Dios, P.; Blanco-Carrion, J. Non-Surgical Treatment of Periodontal Disease in a Pregnant Caucasian Women Population: Adverse Pregnancy Outcomes of a Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2019, 16, 3638. https://doi.org/10.3390/ijerph16193638
Caneiro-Queija L, López-Carral J, Martin-Lancharro P, Limeres-Posse J, Diz-Dios P, Blanco-Carrion J. Non-Surgical Treatment of Periodontal Disease in a Pregnant Caucasian Women Population: Adverse Pregnancy Outcomes of a Randomized Clinical Trial. International Journal of Environmental Research and Public Health. 2019; 16(19):3638. https://doi.org/10.3390/ijerph16193638
Chicago/Turabian StyleCaneiro-Queija, Leticia, Jose López-Carral, Pablo Martin-Lancharro, Jacobo Limeres-Posse, Pedro Diz-Dios, and Juan Blanco-Carrion. 2019. "Non-Surgical Treatment of Periodontal Disease in a Pregnant Caucasian Women Population: Adverse Pregnancy Outcomes of a Randomized Clinical Trial" International Journal of Environmental Research and Public Health 16, no. 19: 3638. https://doi.org/10.3390/ijerph16193638
APA StyleCaneiro-Queija, L., López-Carral, J., Martin-Lancharro, P., Limeres-Posse, J., Diz-Dios, P., & Blanco-Carrion, J. (2019). Non-Surgical Treatment of Periodontal Disease in a Pregnant Caucasian Women Population: Adverse Pregnancy Outcomes of a Randomized Clinical Trial. International Journal of Environmental Research and Public Health, 16(19), 3638. https://doi.org/10.3390/ijerph16193638