Centre for the Promotion of Physical Activity and Health (CAPAS-City): A Pyrenean Cross-Cultural Structure to Lead the Way in the Design, Implementation, and Evaluation of Multilevel Physical Activity Interventions


 ,
,  and
and
Abstract
1. Introduction
1.1. Needs and Challenges Related to Multilevel Physical Activity Interventions
1.2. Building Healthy, Liveable, and Sustainable Cities
2. Centre for the Promotion of Physical Activity and Health (CAPAS-City)
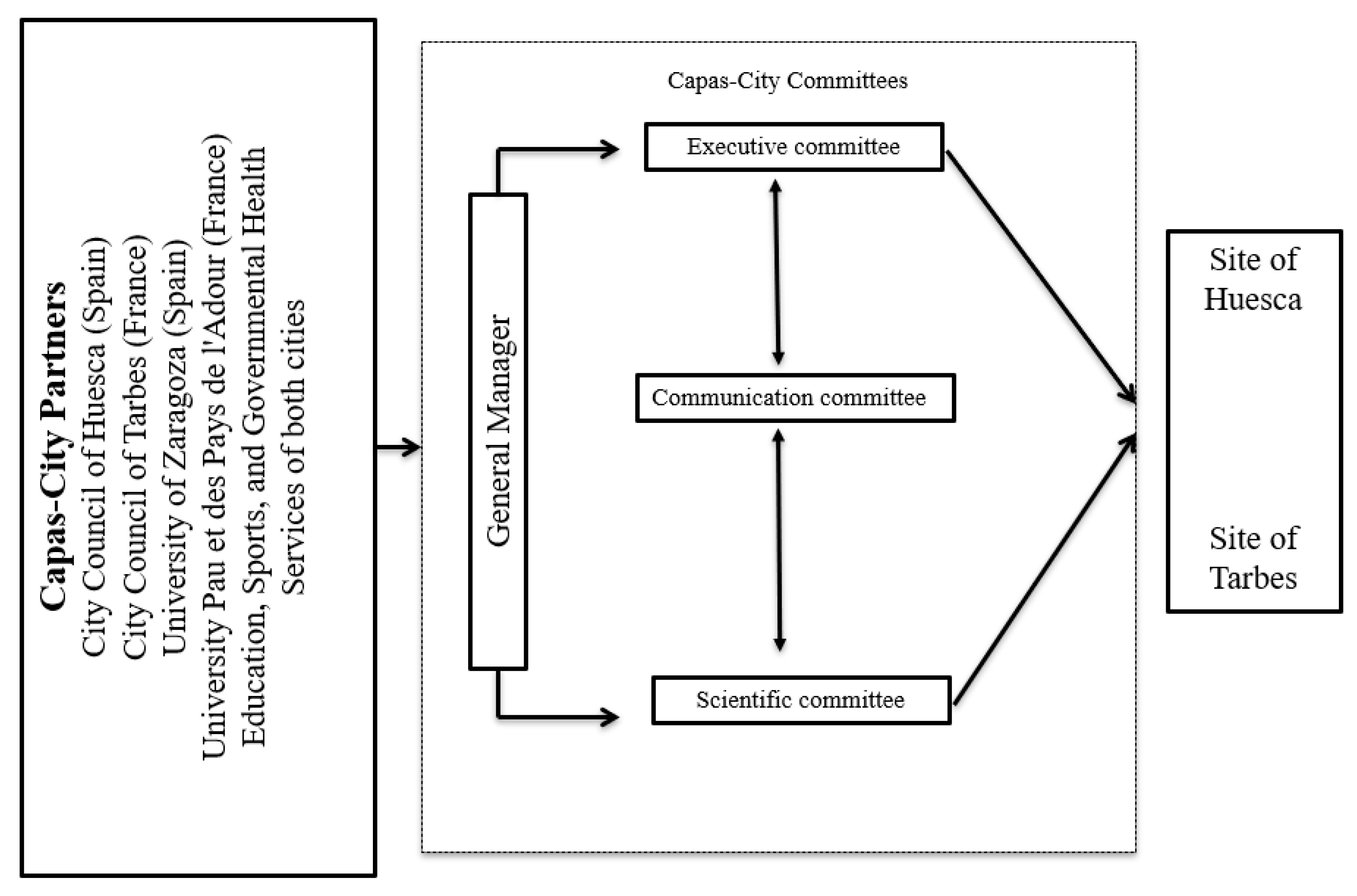
2.1. Partners
2.2. Funding
2.3. Organizational Structure
2.4. Aim, Target Population, and Philosophy of CAPAS-City
2.5. Guiding Principles for Multilevel PA Interventions
2.5.1. Promoting Sustainability
2.5.2. Promoting Integrated and Multisectoral Partnerships
2.5.3. Playing a Leadership Role
2.5.4. Using Evidence-Based Strategies
2.5.5. Promoting Integrated Knowledge Translation
2.5.6. Using a Participatory Research Approach
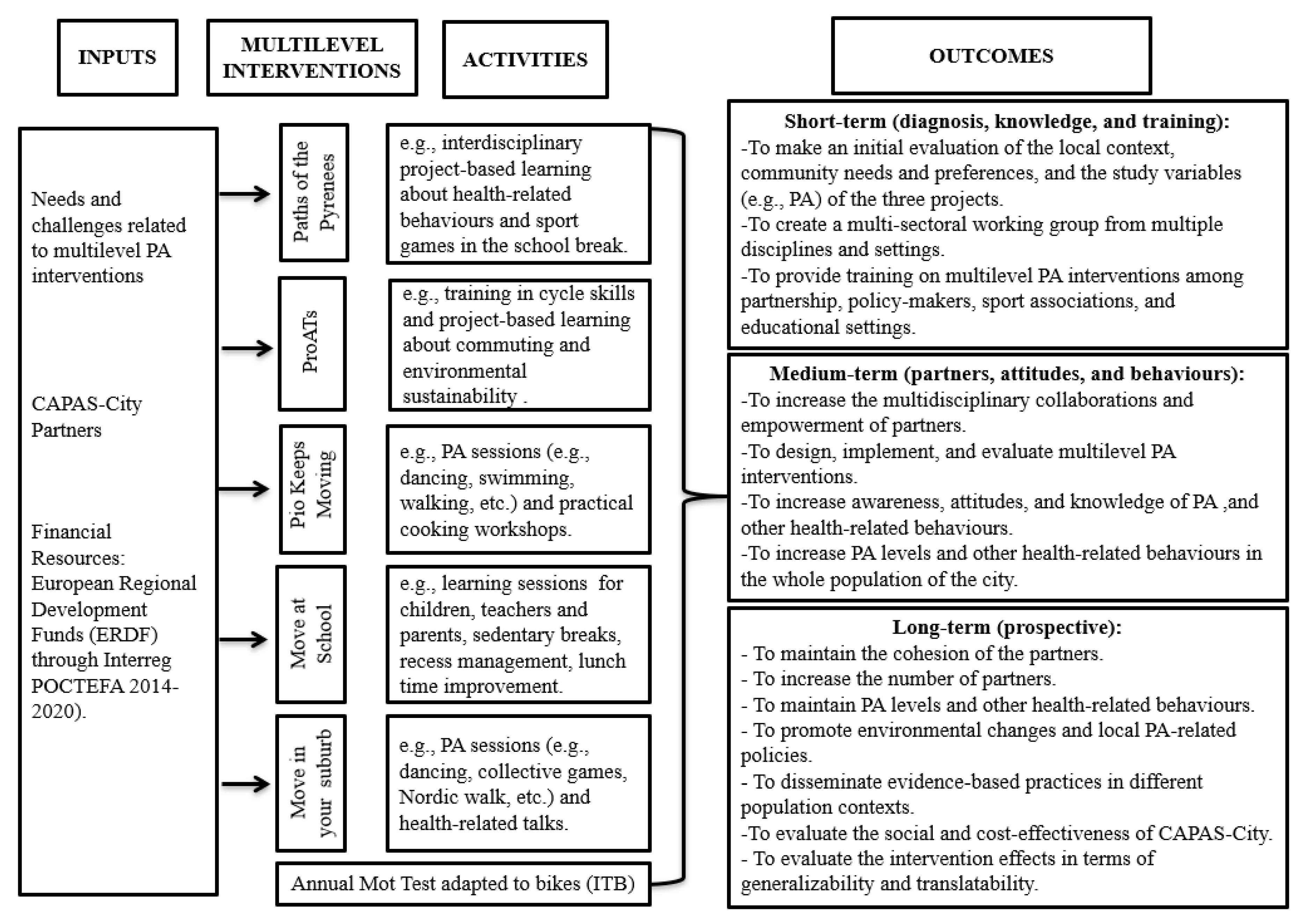
3. CAPAS-City: Organizational Design and Multilevel PA Interventions
3.1. General Organizational Design
3.2. Multilevel PA Interventions
3.2.1. Paths of the Pyrenees Intervention
3.2.2. ProATs Intervention
3.2.3. Pio Keeps Moving Intervention
3.2.4. Move at School Intervention
3.2.5. Move in Your Suburb Intervention
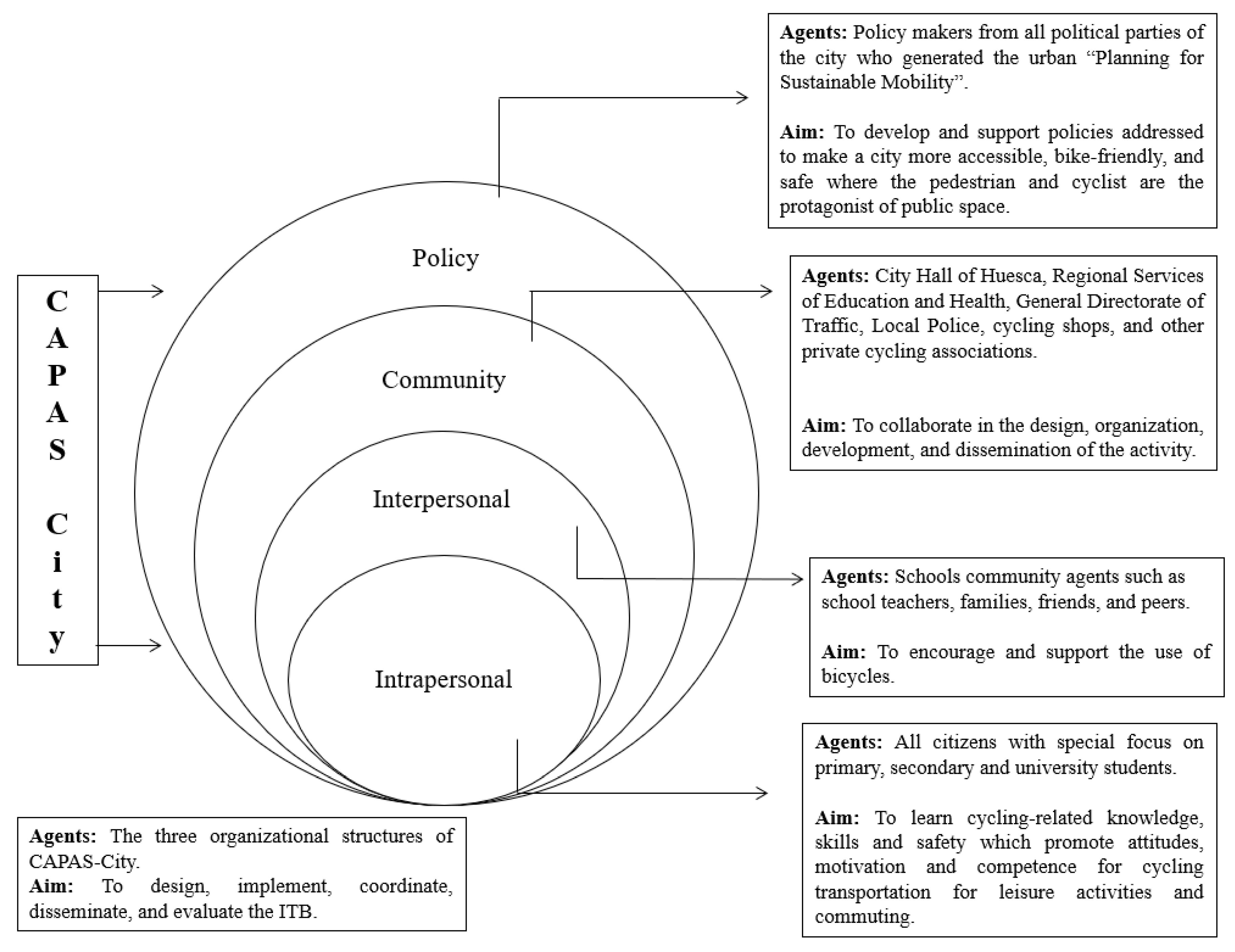
4. “ITB”: An Example of a Strategy Embedded in a Socio-Ecological Framework and Conducted by CAPAS-City to Promote Cycling in the City
5. Preliminary Results
6. Discussion
Limitations and Difficulties
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rhodes, R.E.; Janssen, I.; Bredin, S.S.D.; Warburton, D.E.R.; Bauman, A. Physical activity: Health impact, prevalence, correlates and interventions. Psychol. Health 2017, 32, 942–975. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.; Bredin, S.S. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, 1077–1086. [Google Scholar] [CrossRef]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Lancet Physical Activity Series Working Group. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Roman-Viñas, B.; Zazo, F.; Martínez-Martínez, J.; Aznar-Laín, S.; Serra-Majem, L. Results from Spain’s 2018 report card on physical activity for children and youth. J. Phys. Act. Health 2018, 15, 411–412. [Google Scholar] [CrossRef] [PubMed]
- Aubert, S.; Aucouturier, J.; Ganière, C.; Fillon, A.; Genin, P.; Schipman, J.; Larras, B.; Praznoczy, C.; Duclos, M.; Thivel, D. Results from France’s 2018 report card on physical activity for children and youth. J. Phys. Act. Health 2018, 15, 360–362. [Google Scholar] [CrossRef] [PubMed]
- Borde, R.; Smith, J.J.; Sutherland, R.; Nathan, N.; Lubans, D.R. Methodological considerations and impact of school-based interventions on objectively measured physical activity in adolescents: A systematic review and meta-analysis. Obes. Rev. 2017, 18, 476–490. [Google Scholar] [CrossRef] [PubMed]
- Love, R.; Adams, J.; van Sluijs, E.M. Are school-based physical activity interventions effective and equitable? A meta-analysis of cluster randomized controlled trials with accelerometer-assessed activity. Obes. Rev. 2019, 20, 859–870. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, S.; Häcker, A.L.; Henderson, M.; Barnett, T.; Mathieu, M.E.; Pagani, L.; Bigras, J.L. Physical activity programs with post-intervention follow-up in children: A comprehensive review according to categories of intervention. Int. J. Environ. Res. Public Health 2016, 13, 664. [Google Scholar] [CrossRef] [PubMed]
- Sims, J.; Scarborough, P.; Foster, C. The effectiveness of interventions on sustained childhood physical activity: A systematic review and meta-analysis of controlled studies. PLoS ONE 2015, 10, e0132935. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.M.; Brennan, S.F.; French, D.P.; Patterson, C.C.; Kee, F.; Hunter, R.F. Effectiveness of physical activity interventions in achieving behaviour change maintenance in young and middle aged adults: A systematic review and meta-analysis. Soc. Sci. Med. 2017, 192, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.F.; Martin, B.W.; Martin, B.W. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Sallis, J.F.; Owen, N. Ecological Models of Health Behavior. In Health Behavior and Health Education: Theory, Research, and Practice; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2015; pp. 43–64. [Google Scholar]
- Sallis, J.F. Needs and challenges related to multilevel interventions: Physical activity examples. Health Educt. Behav. 2018, 45, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Schölmerich, V.L.; Kawachi, I. Translating the socio-ecological perspective into multilevel interventions: Gaps between theory and practice. Health Educt. Behav. 2016, 43, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Scheirer, M.A. Linking sustainability research to intervention types. Am. J. Public Health. 2013, 103, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Proctor, E.; Luke, D.; Calhoun, A.; McMillen, C.; Brownson, R.; McCrary, S.; Padek, M. Sustainability of evidence-based healthcare: Research agenda, methodological advances, and infrastructure support. Implement. Sci. 2015, 10, 88. [Google Scholar] [CrossRef] [PubMed]
- Stokols, D. Translating social ecological theory into guidelines for community health promotion. Am. J. Health Promot. 1996, 10, 282–298. [Google Scholar] [CrossRef] [PubMed]
- Hagger, M.S.; Weed, M. Do interventions based on behavioral theory work in the real world? Int. J. Behav. Nutr. Phys. Act. 2019, 16, 36. [Google Scholar] [CrossRef]
- Holmes, B.J.; Best, A.; Davies, H.; Hunter, D.; Kelly, M.P.; Marshall, M.; Rycroft-Malone, J. Mobilising knowledge in complex health systems: A call to action. Evid. Policy 2017, 13, 539–560. [Google Scholar] [CrossRef]
- Richard, L.; Gauvin, L. Building and Implementing Ecological Health Promotion Interventions. In Health Promotion in Canada, Fourth Edition: New Perspectives on Theory, Practice, Policy, and Research Paperback; Rootman, I., Pederson, A., Frohlich, K., Dupéré, S., Eds.; John Wiley & Sons: New York, NY, USA, 2017. [Google Scholar]
- Milat, A.J.; King, L.; Newson, R.; Wolfenden, L.; Rissel, C.; Bauman, A.; Redman, S. Increasing the scale and adoption of population health interventions: Experiences and perspectives of policy makers, practitioners, and researches. Health Res. Policy Syst. 2014, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Hynynen, S.T.; van Stralen, M.M.; Sniehotta, F.F.; Araújo-Soares, V.; Hardeman, W.; Chinapaw, M.J.M.; Vasankari, T.; Hankonen, N. A systematic review of school-based interventions targeting physical activity and sedentary behaviour among older adolescents. Int. Rev. Sport Exerc. Psychol. 2016, 9, 22–44. [Google Scholar] [CrossRef] [PubMed]
- Millstein, R.A.; Oreskovic, N.M.; Quintiliani, L.M.; James, P.; Intille, S. The need for local, multidisciplinary collaborations to promote advances in physical activity research and policy change: The creation of the Boston physical activity resource collaborative (BPARC). J. Phys. Act. Res. 2018, 3, 74. [Google Scholar] [CrossRef] [PubMed]
- Lucidarme, S.; Marlier, M.; Cardon, G.; De Bourdeaudhuij, I.; Willem, A. Critical success factors for physical activity promotion through community partnerships. Int. J. Public Health 2014, 59, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Nastasi, B.K.; Hitchcock, J. Challenges of evaluating multilevel interventions. Am. J. Community Psychol. 2009, 43, 360–376. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Bull, F. Translating science to inform global policy on physical activity. J. Sport Health Sci. 2018, 7, 3–4. [Google Scholar] [CrossRef] [PubMed]
- O’Cathain, A.; Croot, L.; Duncan, E.; Rousseau, N.; Sworn, K.; Turner, K.M.; Yardley, L.; Hoddinott, P. Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open 2019, 9, e029954. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Owen, N.; Fisher, E.B. Ecological Models of Health Behavior. In Health Behavior and Health Education: Theory, Research, and Practice; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 465–485. [Google Scholar]
- Telama, R.; Yang, X.; Leskinen, E.; Kankaanpaa, A.; Hirvensalo, M.; Tammelin, T.; Viikari, J.S.; Raitakari, O.T. Tracking of physical activity from early childhood through youth into adulthood. Med. Sci. Sports Exerc. 2014, 46, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Craike, M.; Wiesner, G.; Hilland, T.A.; Bengoechea, E.G. Interventions to improve physical activity among socioeconomically disadvantaged groups: An umbrella review. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 43. [Google Scholar] [CrossRef] [PubMed]
- Alberga, A.S.; Fortier, M.; Bean, C.; Freedhoff, Y. Youth get a D+ grade in physical activity: How can we change public health messages to help reverse this trend? Appl. Physiol. Nutr. 2019, 44, 567–570. [Google Scholar] [CrossRef]
- Gakidou, E.; Afshin, A.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulle, A.M.; Avera, S.F.; Aboyans, V.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef]
- Mikkelsen, B.; Novotny, R.; Gittelsohn, J. Multi-level, multi-component approaches to community based interventions for healthy living—A three case comparison. Int. J. Environ. Res. Public Health. 2016, 13, 1023. [Google Scholar] [CrossRef] [PubMed]
- Trickett, E.J.; Beehler, S.; Deutsch, C.; Green, L.W.; Hawe, P.; McLeroy, K.; Miller, R.L.; Rapkin, B.D.; Schensul, J.J.; Schulz, A.J.; et al. Advancing the science of community-level interventions. Am. J. Public Health 2011, 101, 1410–1419. [Google Scholar] [CrossRef]
- Zhang, T.; Solmon, M. Integrating self-determination theory with the social ecological model to understand students’ physical activity behaviors. Int. Rev. Sport Exerc. Psychol. 2013, 6, 54–76. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness; Guilford Publications: New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Plotnikoff, R.C.; Costigan, S.A.; Karunamuni, N.; Lubans, D.R. Social cognitive theories used to explain physical activity behavior in adolescents: A systematic review and meta-analysis. Prev. Med. 2013, 56, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Toft, U.; Bloch, P.; Reinbach, H.; Winkler, L.; Buch-Andersen, T.; Aagaard-Hansen, J.; Mikkelsen, B.E.; Jensen, B.B.; Glümer, C. Project SoL-A community-based, multi-component health promotion intervention to improve eating habits and physical activity among Danish families with young children. Part 1: Intervention development and implementation. Int. J. Environ. Res. Public Health 2018, 15, 1097. [Google Scholar] [CrossRef] [PubMed]
- Brand, T.; Pischke, C.; Steenbock, B.; Schoenbach, J.; Poettgen, S.; Samkange-Zeeb, F.; Zeeb, H. What works in community-based interventions promoting physical activity and healthy eating? A review of reviews. Int. J. Environ. Res. Public Health 2014, 11, 5866–5888. [Google Scholar] [CrossRef] [PubMed]
- Messing, S.; Rütten, A.; Abu-Omar, K.; Ungerer-Röhrich, U.; Goodwin, L.; Burlacu, I.; Gediga, G. Physical activity promotion for children and adolescents: A systematic review of reviews. Front. Public Health 2019, 7, 55. [Google Scholar] [CrossRef]
- Murillo, B.; García-Bengoechea, E.; Generelo, E.; Bush, P.L.; Zaragoza, J.; Julián-Clemente, J.A.; García-González, L. Promising school-based strategies and intervention guidelines to increase physical activity of adolescents. Health Educ. Res. 2013, 28, 523–538. [Google Scholar] [CrossRef]
- Chen, P.G.; Diaz, N.; Lucas, G.; Rosenthal, M.S. Dissemination of results in community-based participatory research. Am. J. Prev. Med. 2010, 39, 372–378. [Google Scholar] [CrossRef]
- Giles-Corti, B.; Sallis, J.F.; Sugiyama, T.; Frank, L.D.; Lowe, M.; Owen, N. Translating active living research into policy and practice: One important pathway to chronic disease prevention. J. Public Health Policy 2015, 36, 231–243. [Google Scholar] [CrossRef]
- Tripathy, J.P.; Bhatnagar, A.; Shewade, H.D.; Kumar, A.M.V.; Zachariah, R.; Harries, A.D. Ten tips to improve the visibility and dissemination of research for policy makers and practitioners. Public Health Action 2017, 7, 10–14. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Disseminating the Research Findings; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Hardy, L.J.; Hughes, A.; Hulen, E.; Figueroa, A.; Evans, C.; Begay, R.C. Hiring the experts: Best practices for community-engaged research. Qual. Res. 2016, 16, 592–600. [Google Scholar] [CrossRef] [PubMed]
- Westhues, A.; Ochocka, J.; Jacobson, N.; Simich, L.; Maiter, S.; Janzen, R.; Fleras, A. Developing theory from complexity: Reflections on a collaborative mixed method participatory action research study. Qual. Health Res. 2008, 18, 701–717. [Google Scholar] [CrossRef] [PubMed]
- Sevil, J.; García-González, L.; Abós, A.; Generelo, E.; Aibar, A. Can high schools be an effective setting to promote healthy lifestyles? Effects of a multiple behaviour change intervention in adolescents. J. Adolesc. Health 2019, 64, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Larouche, R.; Ghekiere, A. An ecological model of active transportation. In Children’s Active Transportation; Larouche, R., Ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 93–103. [Google Scholar] [CrossRef]
- Foster, C.; Kelly, P.; Reid, H.A.; Roberts, N.; Murtagh, E.M.; Humphreys, D.K.; Panter, K.; Milton, K. What works to promote walking at the population level? A systematic review. Br. J. Sports Med. 2018, 52, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.A.; Blackburn, N.E.; Woods, C.; Byrne, M.; van Nassau, F.; Tully, M.A. Interventions promoting active transport to school in children: A systematic review and meta-analysis. Prev. Med. 2019, 123, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Winters, M.; Buehler, R.; Götschi, T. Policies to promote active travel: Evidence from reviews of the literature. Curr. Environ. Health Rep. 2017, 4, 278–285. [Google Scholar] [CrossRef]
- Julián, J.A.; Ibor, E.; Aguareles, I.; Beltrán, J.; Navarro, Á. La bicicleta en el ámbito educativo. Tándem Didáctica Educ. Física 2018, 61, 45–51. [Google Scholar]
- Kwasnicka, D.; Dombrowski, S.U.; White, M.; Sniehotta, F. Theoretical explanations for maintenance of behaviour change: A systematic review of behaviour theories. Health Psychol. Rev. 2016, 10, 277–296. [Google Scholar] [CrossRef]
- Special Eurobarometer 472 Sport and Physical Activity; Wave EB88.4. TNS Opinión & Social; European Commission: Brussels, Belgium, 2008. [CrossRef]
- Dawson, J.; Huikuri, S.; Armada, F. Liverpool Active City 2005–2010: Increasing population physical activity levels through intersectoral action. J. Phys. Act. Health 2015, 12, 749–755. [Google Scholar] [CrossRef]
- Diez, E.; Aviñó, D.; Paredes-Carbonell, J.J.; Segura, J.; Suárez, O.; Gerez, M.D.; Pérez, A.; Daban, F.; Camprubí, L. Una buena inversión: La promoción de la salud en las ciudades y los barrios. Gac. Sanit. 2016, 30, 74–80. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Project | Aim | Design/Method | Sample Ages | Measures and Instruments |
|---|---|---|---|---|
| Paths of the Pyrenees | To examine the effects of a school-based intervention on multiple health behaviours and other motivational outcomes | Quasi-experimental design (experimental and control group) One academic year/600 h | Adolescents aged 12–14 years | PA and sedentary time were measured by accelerometers. The other health-related behaviours were measured by using self-reported scales. Motivational outcomes from SDT framework were measured by using self-reported scales. Discussion groups were also conducted. |
| ProATs | To examine the effects of a school-based intervention on active transport to school and other motivational outcomes | Quasi-experimental design (experimental and control group) Two academic years/100 h (24 weeks) | Children aged 10–12 years | PA and sedentary time were measured by accelerometers Active transport was measured by accelerometers. Perceived barriers and motivational outcomes from SDT framework were measured by using self-reported scales. Focus groups among children, parents, and teachers were also conducted. |
| Pio Keeps Moving | To examine the effects of a community-based healthy lifestyle programme on PA, healthy eating, and other motivational outcomes | Community-based participatory action research 2 years/154 h 127 PA and nutrition sessions | Disadvantaged adult women (particularly adult Roma women), from 27 to 58 years old. | PA and sedentary time were measured by accelerometers. One-to-one semi-structured interviews and discussion groups were conducted to measure PA, healthy eating, other health-related behaviours and motivational outcomes. |
| Move at School | To examine the effects of a school-based intervention on PA, sedentary time, physical fitness, motivational outcomes and academic achievement | Quasi-experimental design (experimental and control group) One academic year | Children aged 6–11 years | PA and sedentary time were measured by accelerometers. Physical fitness was estimated based on the Eurofit battery test. Motivational outcomes from SDT framework were measured by using self-reported scales Academic achievement was assessed using standardized tests. |
| Move in your Suburb | To examine the effects of a community-based intervention on PA, sedentary time, physical fitness, well-being, loneliness, and motivational outcomes | One arm interventional study (experimental group only) 9 months (3 3–month phases) | Disadvantaged adult men and women (48.5 ± 13.5 years old) | PA and sedentary time were measured by accelerometers. Physical fitness was assessed with field tests. Physical self-perceptions, well-being, perceptions of loneliness, and motivational outcomes from SDT framework were assessed with self-reported scales. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaragoza Casterad, J.; Sevil-Serrano, J.; Bois, J.E.; Generelo, E.; Lhuisset, L.; Aibar-Solana, A. Centre for the Promotion of Physical Activity and Health (CAPAS-City): A Pyrenean Cross-Cultural Structure to Lead the Way in the Design, Implementation, and Evaluation of Multilevel Physical Activity Interventions. Int. J. Environ. Res. Public Health 2019, 16, 3631. https://doi.org/10.3390/ijerph16193631
Zaragoza Casterad J, Sevil-Serrano J, Bois JE, Generelo E, Lhuisset L, Aibar-Solana A. Centre for the Promotion of Physical Activity and Health (CAPAS-City): A Pyrenean Cross-Cultural Structure to Lead the Way in the Design, Implementation, and Evaluation of Multilevel Physical Activity Interventions. International Journal of Environmental Research and Public Health. 2019; 16(19):3631. https://doi.org/10.3390/ijerph16193631
Chicago/Turabian StyleZaragoza Casterad, Javier, Javier Sevil-Serrano, Julien E. Bois, Eduardo Generelo, Léna Lhuisset, and Alberto Aibar-Solana. 2019. "Centre for the Promotion of Physical Activity and Health (CAPAS-City): A Pyrenean Cross-Cultural Structure to Lead the Way in the Design, Implementation, and Evaluation of Multilevel Physical Activity Interventions" International Journal of Environmental Research and Public Health 16, no. 19: 3631. https://doi.org/10.3390/ijerph16193631
APA StyleZaragoza Casterad, J., Sevil-Serrano, J., Bois, J. E., Generelo, E., Lhuisset, L., & Aibar-Solana, A. (2019). Centre for the Promotion of Physical Activity and Health (CAPAS-City): A Pyrenean Cross-Cultural Structure to Lead the Way in the Design, Implementation, and Evaluation of Multilevel Physical Activity Interventions. International Journal of Environmental Research and Public Health, 16(19), 3631. https://doi.org/10.3390/ijerph16193631