Impact of Critical Illness Insurance on the Burden of High-Cost Rural Residents in Central China: An Interrupted Time Series Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and the CII Policy
2.2. Data Collection
2.3. Study Variables
2.4. Statistical Analysis
3. Results
3.1. Changes of Indicators before and after the Implementation of the CII Policy
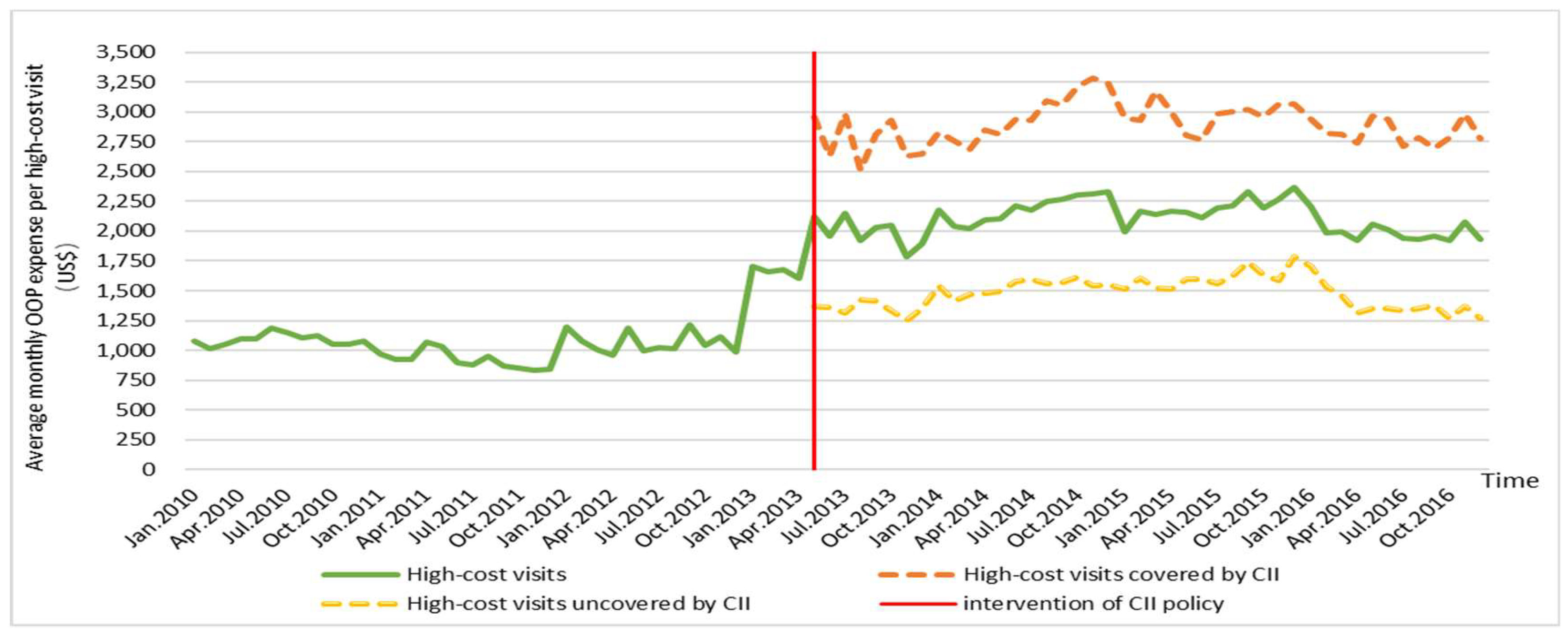
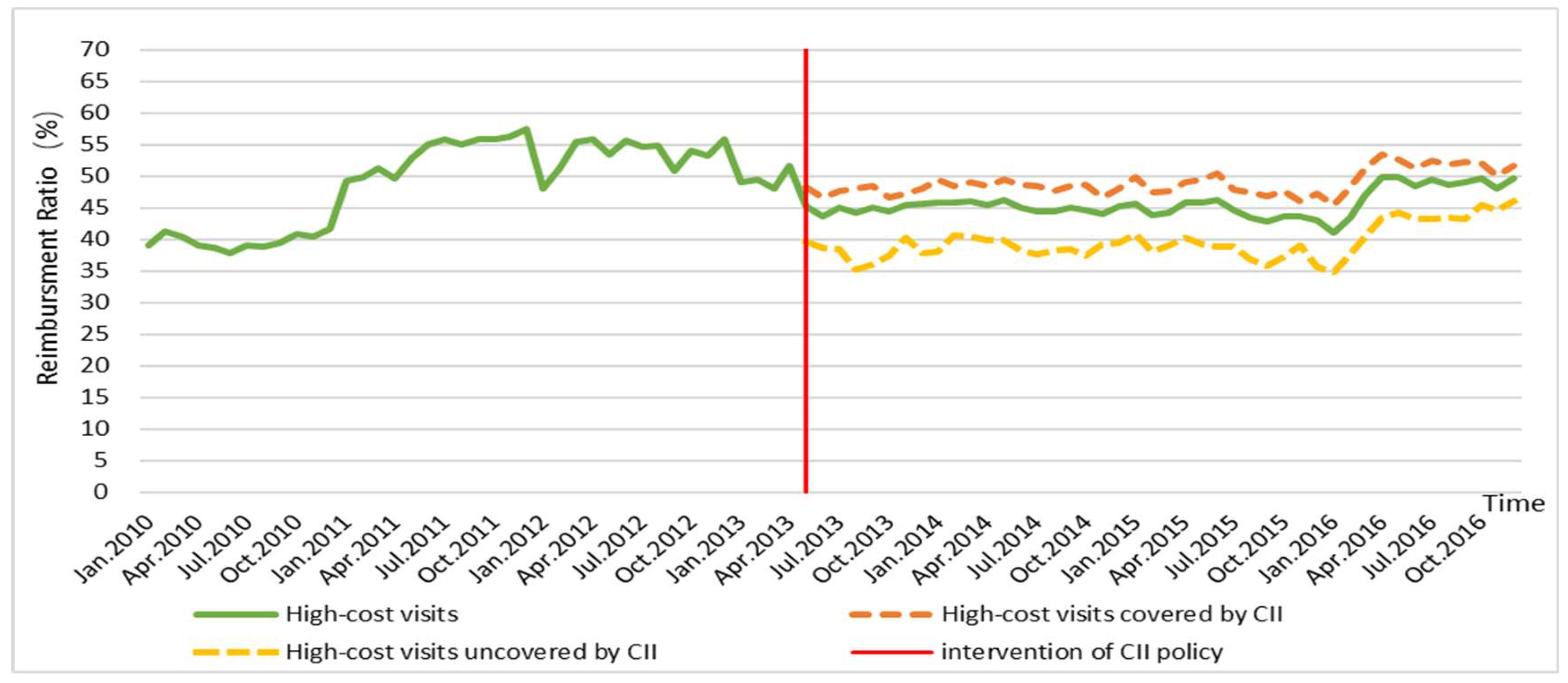
3.2. Trends of Out-of-Pocket Expenses and Reimbursement Ratio (RR) in 2010–2016
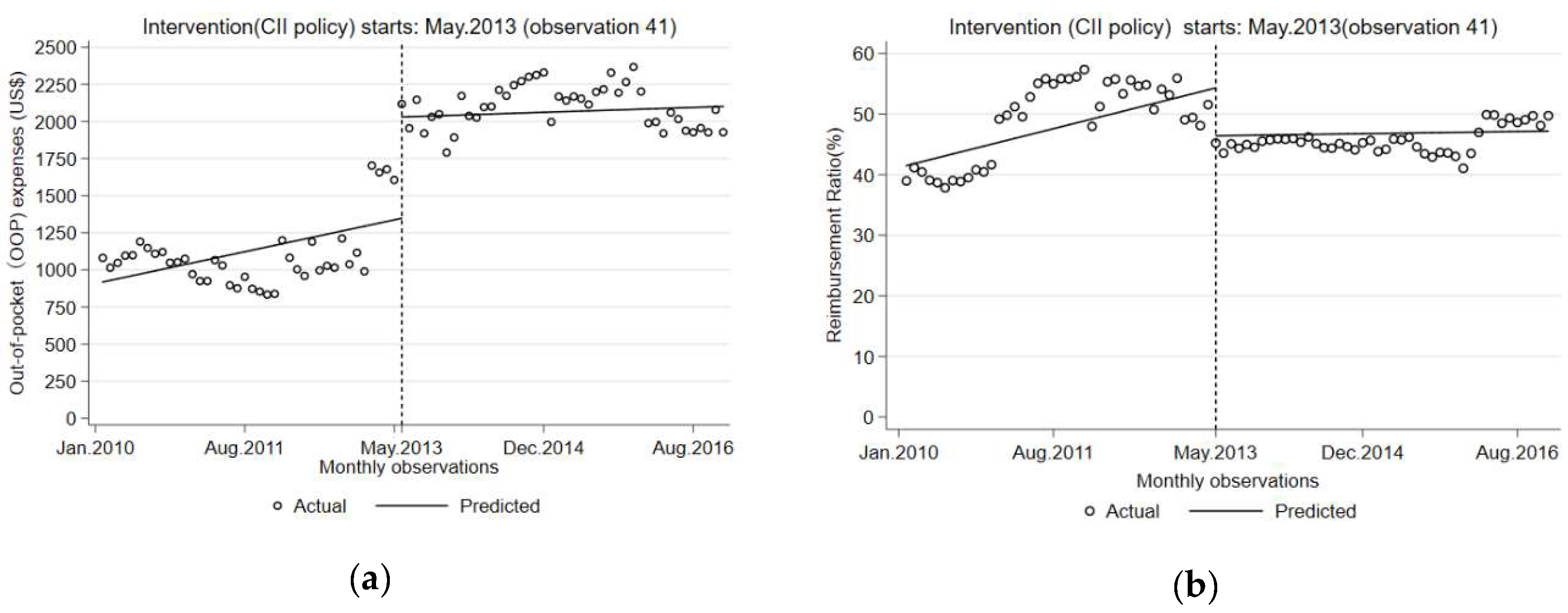
3.3. Impact of the Critical Illness Insurance Policy
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Observation | Time | Intervention | Time after Intervention | THE 1 (US$) | OOP 2 (US$) | RR 3 (%) | Inpatient Visits |
|---|---|---|---|---|---|---|---|---|
| Jan. 2010 | 1 | 1 | 0 | 0 | 1770.3 | 1080.5 | 39.0 | 359 |
| Feb. 2010 | 2 | 2 | 0 | 0 | 1724.1 | 1014.6 | 41.2 | 261 |
| Mar. 2010 | 3 | 3 | 0 | 0 | 1757.8 | 1047.1 | 40.4 | 475 |
| Apr. 2010 | 4 | 4 | 0 | 0 | 1798.5 | 1095.9 | 39.1 | 480 |
| May 2010 | 5 | 5 | 0 | 0 | 1791.5 | 1098.6 | 38.7 | 444 |
| June 2010 | 6 | 6 | 0 | 0 | 1913.7 | 1190.0 | 37.8 | 455 |
| July 2010 | 7 | 7 | 0 | 0 | 1881.4 | 1147.2 | 39.0 | 429 |
| Aug. 2010 | 8 | 8 | 0 | 0 | 1812.8 | 1108.4 | 38.9 | 436 |
| Sep. 2010 | 9 | 9 | 0 | 0 | 1852.1 | 1120.5 | 39.5 | 433 |
| Oct. 2010 | 10 | 10 | 0 | 0 | 1771.0 | 1048.5 | 40.8 | 345 |
| Nov. 2010 | 11 | 11 | 0 | 0 | 1766.0 | 1051.7 | 40.4 | 537 |
| Dec. 2010 | 12 | 12 | 0 | 0 | 1840.6 | 1074.2 | 41.6 | 769 |
| Jan. 2011 | 13 | 13 | 0 | 0 | 1909.8 | 971.2 | 49.1 | 398 |
| Feb. 2011 | 14 | 14 | 0 | 0 | 1841.5 | 924.3 | 49.8 | 329 |
| Mar. 2011 | 15 | 15 | 0 | 0 | 1895.4 | 924.7 | 51.2 | 599 |
| Apr. 2011 | 16 | 16 | 0 | 0 | 2111.4 | 1065.3 | 49.5 | 562 |
| May 2011 | 17 | 17 | 0 | 0 | 2182.2 | 1029.5 | 52.8 | 627 |
| June 2011 | 18 | 18 | 0 | 0 | 1994.8 | 896.5 | 55.1 | 750 |
| July 2011 | 19 | 19 | 0 | 0 | 1982.1 | 875.9 | 55.8 | 789 |
| Aug. 2011 | 20 | 20 | 0 | 0 | 2116.7 | 953.2 | 55.0 | 785 |
| Sep. 2011 | 21 | 21 | 0 | 0 | 1975.2 | 872.2 | 55.8 | 719 |
| Oct. 2011 | 22 | 22 | 0 | 0 | 1930.3 | 853.3 | 55.8 | 655 |
| Nov. 2011 | 23 | 23 | 0 | 0 | 1899.0 | 833.1 | 56.1 | 759 |
| Dec. 2011 | 24 | 24 | 0 | 0 | 1964.4 | 838.3 | 57.3 | 926 |
| Jan. 2012 | 25 | 25 | 0 | 0 | 2304.4 | 1199.2 | 48.0 | 608 |
| Feb. 2012 | 26 | 26 | 0 | 0 | 2217.3 | 1081.6 | 51.2 | 828 |
| Mar. 2012 | 27 | 27 | 0 | 0 | 2246.2 | 1003.4 | 55.3 | 960 |
| Apr. 2012 | 28 | 28 | 0 | 0 | 2167.4 | 959.1 | 55.7 | 911 |
| May 2012 | 29 | 29 | 0 | 0 | 2550.1 | 1189.8 | 53.3 | 1035 |
| June 2012 | 30 | 30 | 0 | 0 | 2243.0 | 996.3 | 55.6 | 1019 |
| July 2012 | 31 | 31 | 0 | 0 | 2263.6 | 1027.4 | 54.6 | 1140 |
| Aug. 2012 | 32 | 32 | 0 | 0 | 2245.7 | 1015.0 | 54.8 | 1057 |
| Sep. 2012 | 33 | 33 | 0 | 0 | 2459.3 | 1211.7 | 50.7 | 1064 |
| Oct. 2012 | 34 | 34 | 0 | 0 | 2260.9 | 1037.9 | 54.1 | 1041 |
| Nov. 2012 | 35 | 35 | 0 | 0 | 2380.8 | 1115.4 | 53.1 | 1077 |
| Dec. 2012 | 36 | 36 | 0 | 0 | 2244.2 | 989.7 | 55.9 | 1041 |
| Jan. 2013 | 37 | 37 | 0 | 0 | 3340.6 | 1702.5 | 49.0 | 963 |
| Feb. 2013 | 38 | 38 | 0 | 0 | 3274.3 | 1656.1 | 49.4 | 564 |
| Mar. 2013 | 39 | 39 | 0 | 0 | 3231.4 | 1677.5 | 48.1 | 888 |
| Apr. 2013 | 40 | 40 | 0 | 0 | 3314.3 | 1605.7 | 51.6 | 931 |
| May 2013 | 41 | 41 | 1 | 1 | 3863.9 | 2117.3 | 45.2 | 725 |
| June 2013 | 42 | 42 | 1 | 2 | 3461.8 | 1954.2 | 43.5 | 729 |
| July 2013 | 43 | 43 | 1 | 3 | 3907.3 | 2146.2 | 45.1 | 925 |
| Aug. 2013 | 44 | 44 | 1 | 4 | 3448.6 | 1919.8 | 44.3 | 905 |
| Sep. 2013 | 45 | 45 | 1 | 5 | 3689.0 | 2030.8 | 44.9 | 773 |
| Oct. 2013 | 46 | 46 | 1 | 6 | 3691.9 | 2048.7 | 44.5 | 1010 |
| Nov. 2013 | 47 | 47 | 1 | 7 | 3285.1 | 1790.1 | 45.5 | 1051 |
| Dec. 2013 | 48 | 48 | 1 | 8 | 3486.2 | 1892.4 | 45.7 | 1135 |
| Jan. 2014 | 49 | 49 | 1 | 9 | 4016.0 | 2172.4 | 45.9 | 1067 |
| Feb. 2014 | 50 | 50 | 1 | 10 | 3760.6 | 2037.1 | 45.8 | 677 |
| Mar. 2014 | 51 | 51 | 1 | 11 | 3749.1 | 2025.6 | 46.0 | 1095 |
| Apr. 2014 | 52 | 52 | 1 | 12 | 3836.3 | 2096.7 | 45.3 | 984 |
| May 2014 | 53 | 53 | 1 | 13 | 3904.6 | 2100.3 | 46.2 | 1004 |
| June 2014 | 54 | 54 | 1 | 14 | 4028.7 | 2212.2 | 45.1 | 1056 |
| July 2014 | 55 | 55 | 1 | 15 | 3911.0 | 2173.0 | 44.4 | 1170 |
| Aug. 2014 | 56 | 56 | 1 | 16 | 4034.8 | 2244.4 | 44.4 | 1032 |
| Sep. 2014 | 57 | 57 | 1 | 17 | 4136.9 | 2270.9 | 45.1 | 1071 |
| Oct. 2014 | 58 | 58 | 1 | 18 | 4153.6 | 2300.6 | 44.6 | 1025 |
| Nov. 2014 | 59 | 59 | 1 | 19 | 4136.7 | 2313.0 | 44.1 | 1016 |
| Dec. 2014 | 60 | 60 | 1 | 20 | 4254.8 | 2330.0 | 45.2 | 1397 |
| Jan. 2015 | 61 | 61 | 1 | 21 | 3673.4 | 1996.6 | 45.6 | 898 |
| Feb. 2015 | 62 | 62 | 1 | 22 | 3857.2 | 2167.3 | 43.8 | 997 |
| Mar. 2015 | 63 | 63 | 1 | 23 | 3834.0 | 2140.5 | 44.2 | 1388 |
| Apr. 2015 | 64 | 64 | 1 | 24 | 4005.1 | 2168.1 | 45.9 | 1207 |
| May 2015 | 65 | 65 | 1 | 25 | 3969.7 | 2154.0 | 45.7 | 1190 |
| June 2015 | 66 | 66 | 1 | 26 | 3928.5 | 2114.2 | 46.2 | 1260 |
| July 2015 | 67 | 67 | 1 | 27 | 3966.8 | 2198.5 | 44.6 | 1407 |
| Aug. 2015 | 68 | 68 | 1 | 28 | 3918.8 | 2216.5 | 43.4 | 1328 |
| Sep. 2015 | 69 | 69 | 1 | 29 | 4077.6 | 2328.7 | 42.9 | 1200 |
| Oct. 2015 | 70 | 70 | 1 | 30 | 3892.7 | 2193.2 | 43.7 | 1160 |
| Nov. 2015 | 71 | 71 | 1 | 31 | 4015.3 | 2265.3 | 43.6 | 1188 |
| Dec. 2015 | 72 | 72 | 1 | 32 | 4153.8 | 2367.1 | 43.0 | 1368 |
| Jan. 2016 | 73 | 73 | 1 | 33 | 3734.3 | 2201.7 | 41.0 | 1359 |
| Feb. 2016 | 74 | 74 | 1 | 34 | 3519.7 | 1988.5 | 43.5 | 1201 |
| Mar. 2016 | 75 | 75 | 1 | 35 | 3764.9 | 1996.9 | 47.0 | 1523 |
| Apr. 2016 | 76 | 76 | 1 | 36 | 3830.5 | 1919.4 | 49.9 | 1152 |
| May 2016 | 77 | 77 | 1 | 37 | 4106.5 | 2059.6 | 49.8 | 1165 |
| June 2016 | 78 | 78 | 1 | 38 | 3911.4 | 2015.6 | 48.5 | 1178 |
| July 2016 | 79 | 79 | 1 | 39 | 3824.6 | 1937.5 | 49.3 | 1292 |
| Aug. 2016 | 80 | 80 | 1 | 40 | 3748.3 | 1926.7 | 48.6 | 1288 |
| Sep. 2016 | 81 | 81 | 1 | 41 | 3837.0 | 1955.5 | 49.0 | 1095 |
| Oct. 2016 | 82 | 82 | 1 | 42 | 3829.5 | 1926.1 | 49.7 | 1007 |
| Nov. 2016 | 83 | 83 | 1 | 43 | 4005.1 | 2078.4 | 48.1 | 1145 |
| Dec. 2016 | 84 | 84 | 1 | 44 | 3832.3 | 1926.9 | 49.7 | 1466 |
Appendix B

References
- Zook, C.J.; Moore, F.D. High-cost users of medical care. N. Engl. J. Med. 1980, 302, 996–1002. [Google Scholar] [CrossRef]
- Hayes, S.L.; Salzberg, C.A.; Mccarthy, D.; Radley, D.C.; Abrams, M.K.; Shah, T.; Anderson, G.F. High-Need, High-Cost Patients: Who Are They and How Do They Use Health Care? A Population-Based Comparison of Demographics, Health Care Use, and Expenditures. Issue Brief 2016, 26, 1. [Google Scholar]
- Wammes, J.J.G.; van der Wees, P.J.; Tanke, M.A.C.; Westert, G.P.; Jeurissen, P.P.T. Systematic review of high-cost patients’ characteristics and healthcare utilisation. BMJ Open 2018, 8, e023113. [Google Scholar] [CrossRef]
- Wodchis, W.P.; Austin, P.C.; Henry, D.A. A 3-year study of high-cost users of health care. Can. Med Assoc. J. 2016, 188, 182–188. [Google Scholar] [CrossRef]
- Ku, L.J.E.; Chiou, M.J.; Liu, L.F. Variations in the persistence of health expenditures and the implications for the design of capitation payments in Taiwan. J. Health Serv. Res. Policy 2015, 20, 146–153. [Google Scholar] [CrossRef]
- Zulman, D.M.; Chee, C.P.; Wagner, T.H.; Yoon, J.; Cohen, D.M.; Holmes, T.H.; Ritchie, C.; Asch, S.M. Multimorbidity and healthcare utilisation among high-cost patients in the US Veterans Affairs Health Care System. BMJ Open 2015, 5, e007771. [Google Scholar] [CrossRef]
- Feder, J.L. Predictive Modeling and Team Care for High-Need Patients at HealthCare Partners. Health Aff. 2011, 30, 416–418. [Google Scholar] [CrossRef][Green Version]
- Xin, H. How Do High Cost-Sharing Policies for Physician Care Affect Inpatient Care Use and Costs Among People with Chronic Disease? J. Ambul. Care Manag. 2015, 38, 100–108. [Google Scholar] [CrossRef]
- Blumenthal, D.; Chernof, B.; Fulmer, T.; Lumpkin, J.; Selberg, J. Caring for High-Need, High-Cost Patients—An Urgent Priority. N. Engl. J. Med. 2016, 375, 909–911. [Google Scholar] [CrossRef]
- Anderson, G.F.; Ballreich, J.; Bleich, S.; Boyd, C.; Dugoff, E.; Leff, B.; Salzburg, C.; Wolff, J. Attributes Common to Programs That Successfully Treat High-Need, High-Cost Individuals. Am. J. Manag. Care 2015, 21, e597–e600. [Google Scholar]
- Brown, R.S.; Peikes, D.; Peterson, G.; Schore, J.; Razafindrakoto, C.M. Six Features Of Medicare Coordinated Care Demonstration Programs That Cut Hospital Admissions Of High-Risk Patients. Health Aff. 2012, 31, 1156–1166. [Google Scholar] [CrossRef]
- Progress of Critical Illness Insurance Program Based on New Rural Cooperative Medical System. Available online: http://www.nhc.gov.cn/xcs/s3574/201408/3b8402adec4843f0bf36e114227e09de.shtml (accessed on 3 April 2019).
- General Office of the State Council Guiding Opinions on Carrying out Critical Disease Insurance Work for Urban and Rural Residents. Available online: http://www.gov.cn/zhengce/content/2015-08/02/content_10041.htm (accessed on 27 Feburary 2019).
- Li, H.; Jiang, L. Catastrophic medical insurance in China. Lancet 2017, 390, 1724–1725. [Google Scholar] [CrossRef]
- Zhang, Y.; Vanneste, J.; Xu, J.; Liu, X. Critical Illness Insurance to alleviate catastrophic health expenditures: New evidence from China. Int. J. Health Econ. Manag. 2019, 19, 193–212. [Google Scholar] [CrossRef]
- Liu, P.; Jiang, L.; Li, C.; Sun, M.; Rieger, A.; Hao, M. How to deal with burden of critical illness: A comparison of strategies in different areas of China. Pak. J. Med. Sci. 2014, 30, 659–663. [Google Scholar] [CrossRef]
- Zhao, S.W.; Zhang, X.Y.; Dai, W.; Ding, Y.X.; Chen, J.Y.; Fang, P.Q. Effect of the catastrophic medical insurance on household catastrophic health expenditure: Evidence from China. Gac. Sanit. 2019, in press. [Google Scholar] [CrossRef]
- Fang, P.; Pan, Z.; Zhang, X.; Bai, X.; Gong, Y.; Yin, X. The effect of critical illness insurance in China. Medicine 2018, 97, e11362. [Google Scholar] [CrossRef]
- Jiang, J.; Chen, S.; Xin, Y.; Wang, X.; Zeng, L.; Zhong, Z.; Xiang, L. Does the critical illness insurance reduce patients’ financial burden and benefit the poor more: A comprehensive evaluation in rural area of China. J. Med. Econ. 2019, 22, 455–463. [Google Scholar] [CrossRef]
- Figueroa, J.F.; Zhou, X.; Jha, A.K. Characteristics and Spending Patterns of Persistently High-Cost Medicare Patients. Health Aff. 2019, 38, 107–114. [Google Scholar] [CrossRef]
- Nguyen, N.H.; Khera, R.; Ohno-Machado, L.; Sandborn, W.J.; Singh, S. Annual Burden and Costs of Hospitalization for High-Need, High-Cost Patients with Chronic Gastrointestinal and Liver Diseases. Clin. Gastroenterol. Hepatol. 2018, 16, 1284. [Google Scholar] [CrossRef]
- Zeng, Y.; Li, J.; Yuan, Z.; Fang, Y. The effect of China’s new cooperative medical scheme on health expenditures among the rural elderly. Int. J. Equity Health 2019, 18, 27. [Google Scholar] [CrossRef]
- Ma, J.; Xu, J.; Zhang, Z.; Wang, J. New cooperative medical scheme decreased financial burden but expanded the gap of income-related inequity: Evidence from three provinces in rural China. Int. J. Equity Health 2016, 15, 72. [Google Scholar] [CrossRef]
- Li, X.; Zhou, Q.; Wang, X.; Su, S.; Zhang, M.; Jiang, H.; Wang, J.; Liu, M. The effect of low insurance reimbursement on quality of care for non-small cell lung cancer in China: A comprehensive study covering diagnosis, treatment, and outcomes. BMC Cancer 2018, 18, 683. [Google Scholar] [CrossRef]
- Xiang, L.; Pan, Y.; Hou, S.; Zhang, H.; Sato, K.D.; Li, Q.; Wang, J.; Tang, S. The impact of the new cooperative medical scheme on financial burden of tuberculosis patients: Evidence from six counties in China. Infect. Dis. Poverty 2016, 5, 8. [Google Scholar] [CrossRef]
- Linden, A. Conducting interrupted time-series analysis for single- and multiple-group comparisons. Stata J. 2015, 15, 480–500. [Google Scholar] [CrossRef]
- Wagner, A.K.; Soumerai, S.B.; Zhang, F.; Ross-Degnan, D. Segmented regression analysis of interrupted time series studies in medication use research. J. Clin. Pharm. Ther. 2002, 27, 299–309. [Google Scholar] [CrossRef]
- Sloboda, B. Introduction to Time Series Analysis and Forecasting. Int. J. Forecast. 2009, 25, 209–211. [Google Scholar] [CrossRef]
- Pavon-Leon, P.; Reyes-Morales, H.; Martinez, A.J.; Maria Mendez-Main, S.; del Carmen Gogeascoechea-Trejo, M.; Blazquez-Morales, M.S.L. Out-of-pocket expenditure by elderly adults enrolled in a public health insurance programme in Mexico. Gac. Sanit. 2017, 31, 286–291. [Google Scholar]



| Before the CII Policy Was Implemented | |||||||
| BMI (Year 2010) | BMI (Year from 2011) | ||||||
| Deductible | PRR 1 | Cap | Deductible | PRR 1 | Cap | ||
| (US$) | (%) | (US$) | (US$) | (%) | (US$) | ||
| A1 2 | 16 | 80 | 8070 | A1 2 | 0 | 90 | 16,140 |
| A2 3 | 32 | 60 | A2 3 | 32 | 80 | ||
| B 4 | 81 | 40 | B 5 | 81 | 60 | ||
| After the CII Policy was Implemented | |||||||
| BMI | CII | ||||||
| Deductible | PRR 1 | Cap | Deductible 5 | Expenses | PRR 1 | Cap | |
| (US$) | (%) | (US$) | (US$) | (US$) | (%) | (US$) | |
| A1 2 | 16 | 90 | 16,140 | 1291 | 1291–4842 | 50 | No cap |
| A2 3 | 81 | 60 | 4842–8070 | 60 | |||
| B 4 | 129 | 50 | >8070 | 70 | |||
| Variables | Implementation of the CII Policy | |
|---|---|---|
| Before (Mean ± SD 1) | After (Mean ± SD) | |
| Total number of high-cost inpatient visits | 28,448 | 49,309 |
| Proportion of high-cost inpatients visits covered by CII (%) | 0 | 44.0 ± 3.2 |
| Proportion of high-cost inpatients visits in-county (%) | 60.9 ± 34.1 | 86.9 ± 21.6 |
| Hospitalization expenses of high-cost inpatient visits (US$) | 2155.6 ± 438.6 | 3863.5 ± 207.5 |
| OOP expenses of high-cost inpatient visits (US$) | 1089.6 ± 216.8 | 2100.4 ± 140.1 |
| CII Reimbursement ratio per high-cost inpatient visit (%) | 0 | 8.0 ± 2.8 |
| BMI Reimbursement ratio per high-cost inpatient visit (%) | 42.6 ± 16.2 | 38.8 ± 2.1 |
| Non-reimbursable expenses ratio per high-cost inpatient visit (%) | 34.1 ± 28.1 | 25.4 ± 1.5 |
| Variables | Value (SE 1) | t-Value | p-Value | 95% CI | DW 2 |
|---|---|---|---|---|---|
| OOP (US$) | 2.2 | ||||
| β0: Baseline level | 918.1 (111.1) | 8.3 | <0.01 3 | (697.0, 1139.2) | |
| β1: Baseline slope | 10.7 (4.6) | 2.3 | 0.02 | (1.6, 19.9) | |
| β2: Level change after CII policy | 682.6 (118.9) | 5.7 | <0.01 3 | (446.0, 919.2) | |
| β3: Slope change after CII policy | −9.1 (6.8) | −1.3 | 0.19 | (−22.6, 4.4) | |
| Reimbursement Ratio (%) | 2.2 | ||||
| β0: Baseline level | 41.5 (3.0) | 13.8 | <0.01 3 | (35.5, 47.5) | |
| β1: Baseline slope | 0.3 (0.1) | 2.7 | 0.01 | (0.1, 0.6) | |
| β2: Level change after CII policy | −7.9 (2.1) | −3.7 | <0.01 3 | (−12.1, −3.7) | |
| β3: Slope change after CII policy | −0.3 (0.2) | −1.6 | 0.11 | (−0.7, 0.1) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, L.; Jiang, J.; Xiang, L.; Wang, X.; Zeng, L.; Zhong, Z. Impact of Critical Illness Insurance on the Burden of High-Cost Rural Residents in Central China: An Interrupted Time Series Study. Int. J. Environ. Res. Public Health 2019, 16, 3528. https://doi.org/10.3390/ijerph16193528
Li L, Jiang J, Xiang L, Wang X, Zeng L, Zhong Z. Impact of Critical Illness Insurance on the Burden of High-Cost Rural Residents in Central China: An Interrupted Time Series Study. International Journal of Environmental Research and Public Health. 2019; 16(19):3528. https://doi.org/10.3390/ijerph16193528
Chicago/Turabian StyleLi, Lu, Junnan Jiang, Li Xiang, Xuefeng Wang, Li Zeng, and Zhengdong Zhong. 2019. "Impact of Critical Illness Insurance on the Burden of High-Cost Rural Residents in Central China: An Interrupted Time Series Study" International Journal of Environmental Research and Public Health 16, no. 19: 3528. https://doi.org/10.3390/ijerph16193528
APA StyleLi, L., Jiang, J., Xiang, L., Wang, X., Zeng, L., & Zhong, Z. (2019). Impact of Critical Illness Insurance on the Burden of High-Cost Rural Residents in Central China: An Interrupted Time Series Study. International Journal of Environmental Research and Public Health, 16(19), 3528. https://doi.org/10.3390/ijerph16193528