Emotional Effects of the Duration, Efficiency, and Subjective Quality of Sleep in Healthcare Personnel

 ,
,  ,
, 


Abstract
1. Introduction
1.1. Sleep Quality and Emotion Management
1.2. Research Objectives
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analyses
3. Results
3.1. Sleep and Emotional Intelligence Components: Descriptive and Correlational Analyses
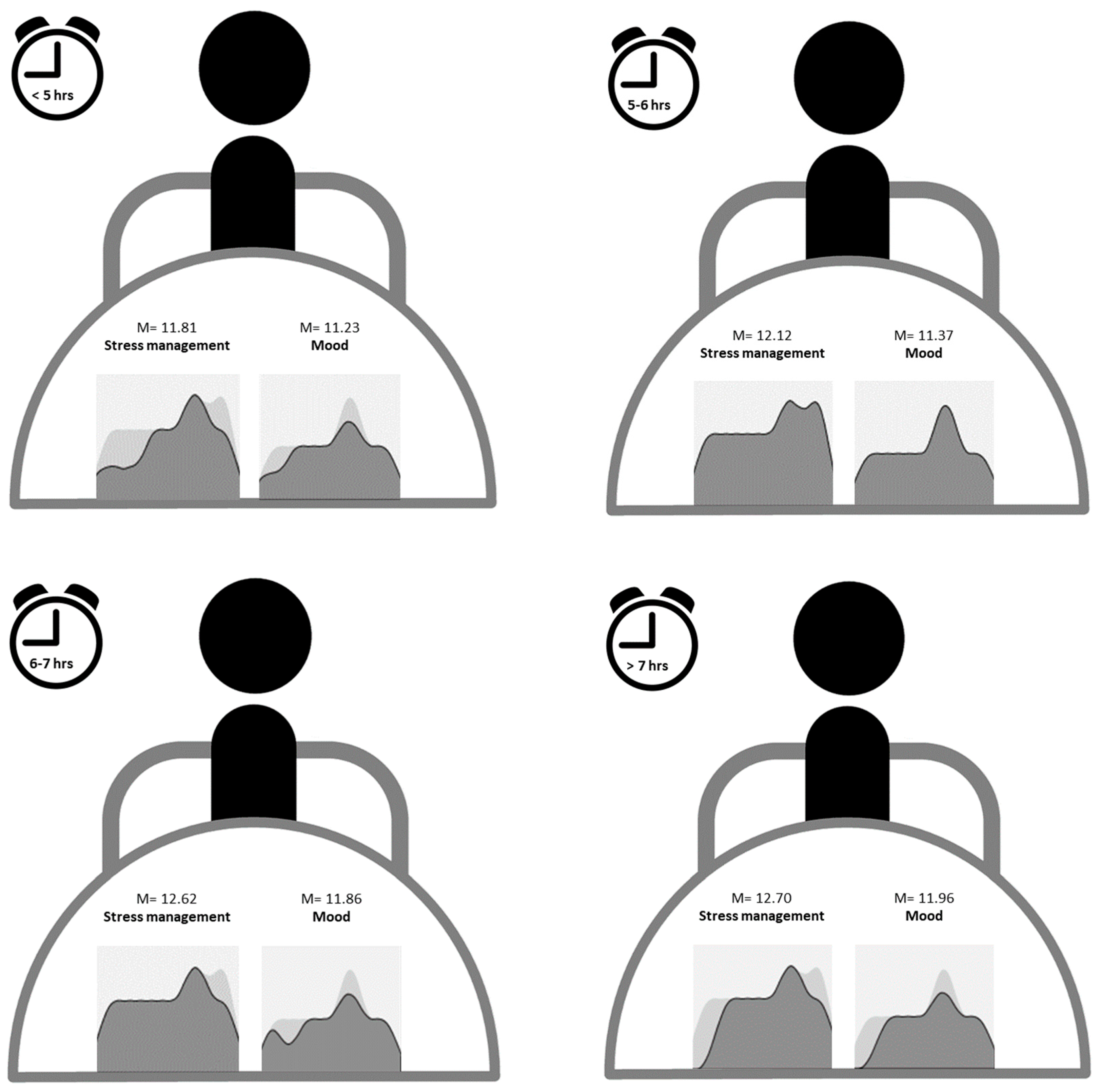
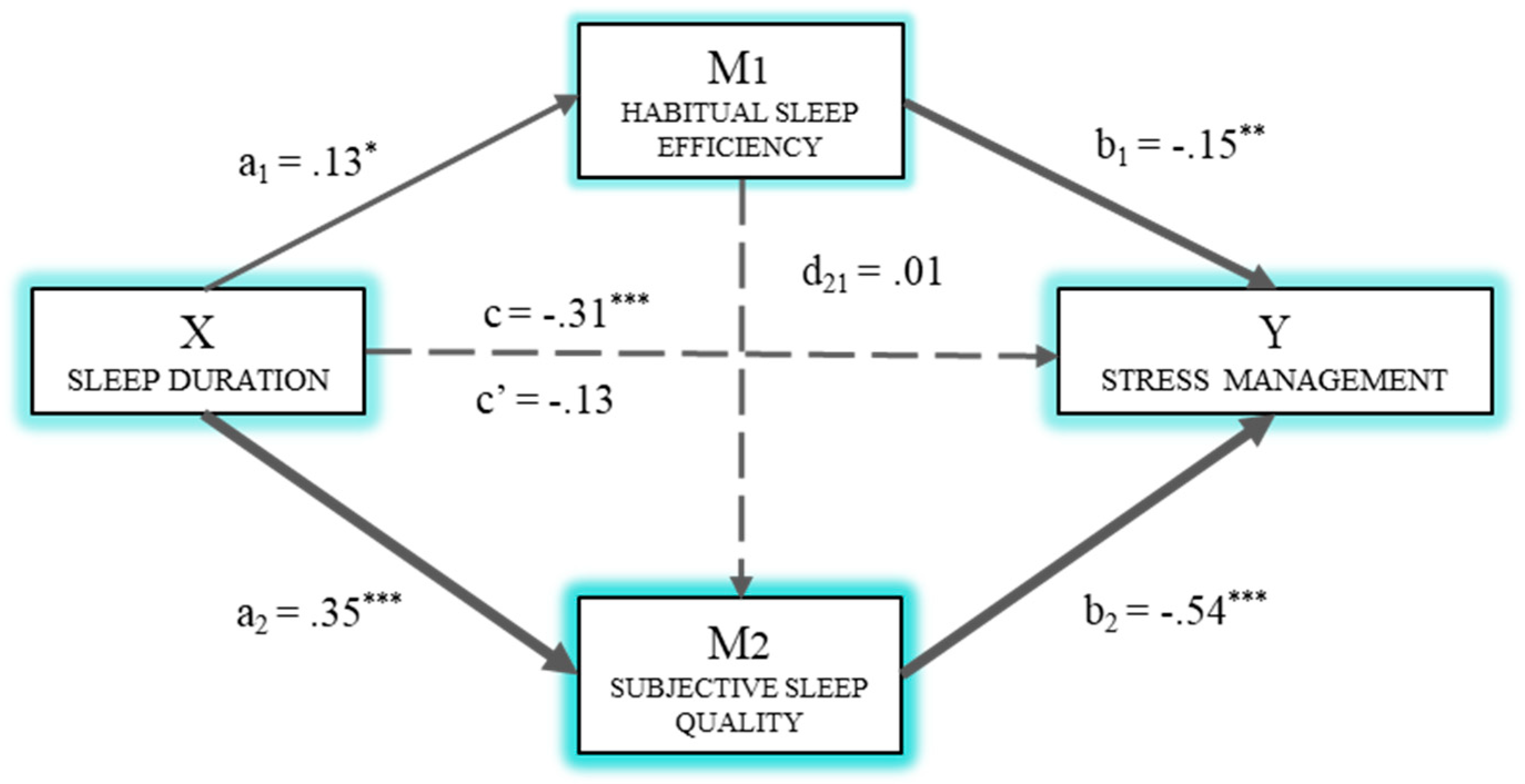
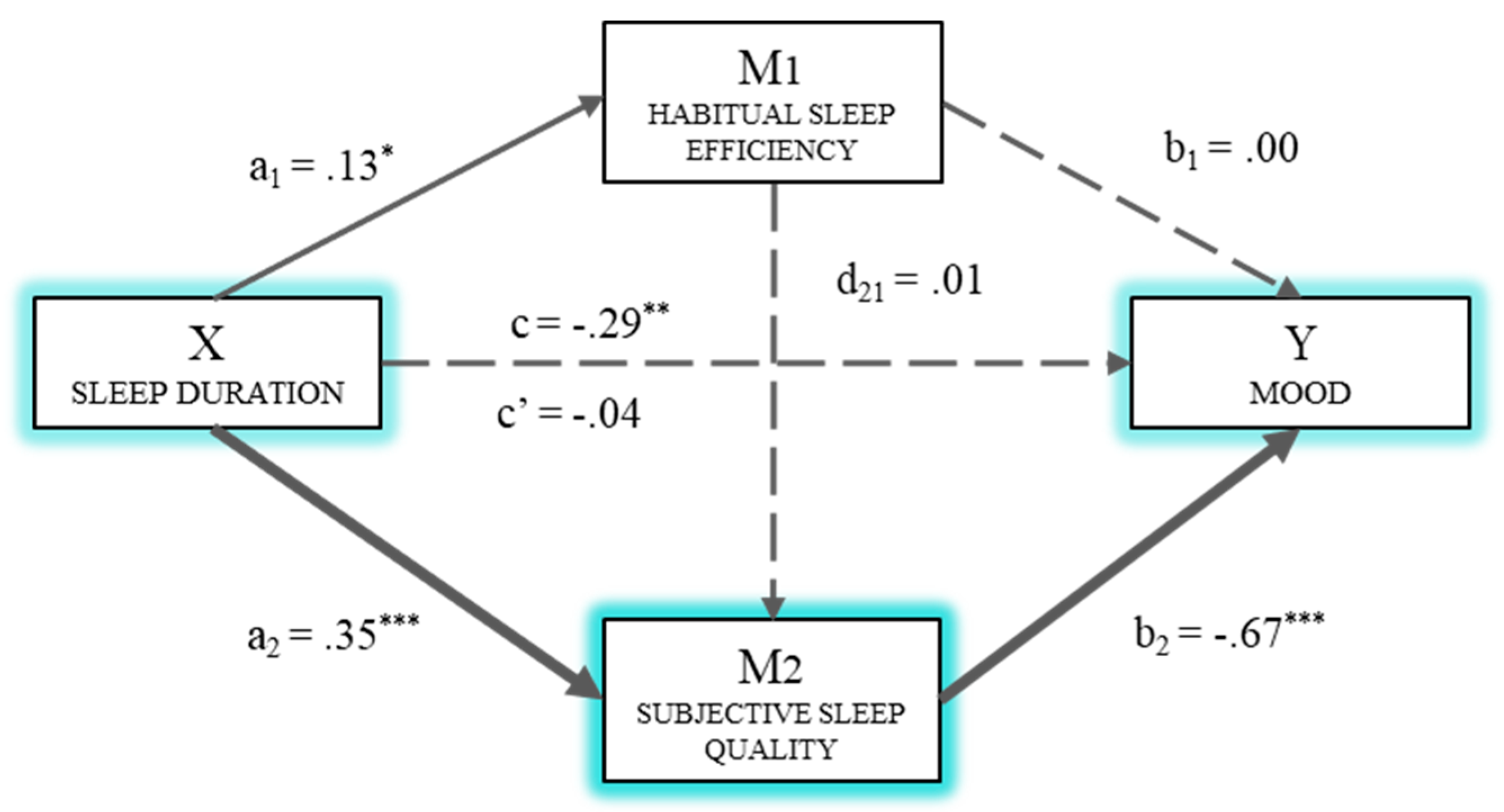
3.2. Multiple Mediation Analysis for the Effects of Sleep Duration on Stress Management and Mood
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- De Castillo, V.; Corrente, J.E.; Bojikian, B. Association between sleep quality and quality of life in nursing professionals working rotating shifts. Rev. Saude Publica 2014, 48, 594–601. [Google Scholar] [CrossRef]
- Foley, J.E.; Weinraub, M. Sleep, Affect, and Social Competence from Preschool to Preadolescence: Distinct Pathways to Emotional and Social Adjustment for Boys and for Girls. Front. Psychol. 2017, 8, 711. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Brandolim, N.; De Jesús, S.N.; Viseu, J.N.; Dieter, C.; Guerreiro, M.; Dominguez, R.B. Depression and quality of life in older adults: Mediation effect of sleep quality. Int. J. Clin. Health Psychol. 2018, 18, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Zamanian, Z.; Nikeghbal, K.; Khajehnasiri, F. Influence of Sleep on Quality of Life Among Hospital Nurses. Electron. Physician 2016, 8, 1811–1816. [Google Scholar] [CrossRef]
- Chen, X.; Gelaye, B.; Williams, M.A. Sleep characteristics and health-related quality of life among a national sample of American young adults: Assessment of possible health disparities. Qual. Life Res. 2014, 23, 613–625. [Google Scholar] [CrossRef] [PubMed]
- Thurston, R.C.; Chang, Y.; von Känel, R.; Barinas-Mitchell, E.; Jennings, J.R.; Hall, M.H.; Santoro, N.; Buysse, D.J.; Matthews, K.A. Sleep Characteristics and Carotid Atherosclerosis Among Midlife Women. Sleep 2017, 40, zsw052. [Google Scholar] [CrossRef] [PubMed]
- Orzech, K.M.; Grandner, M.A.; Roane, B.M.; Carskadon, M.A. Digital media use in the 2 h before bedtime is associated with sleep variables in university students. Comput. Hum. Behav. 2016, 55, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Saling, L.L.; Haire, M. Are you awake? Mobile phone use after lights out. Comput. Hum. Behav. 2016, 64, 932–937. [Google Scholar] [CrossRef]
- Tian, X.; Yu, G.; He, F. An analysis of sleep complaints on Sina Weibo. Comput. Hum. Behav. 2016, 62, 230–235. [Google Scholar] [CrossRef]
- Xanidis, N.; Brignell, C.M. The association between the use of social network sites, sleep quality and cognitive function during the day. Comput. Hum. Behav. 2016, 55, 121–126. [Google Scholar] [CrossRef]
- Grandner, M.A. Sleep, Health, and Society. Sleep Med. Clin. 2017, 12, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Simonelli, G.; Marshall, N.S.; Grillakis, A.; Miller, C.B.; Hoyos, C.M.; Glozier, N. Sleep health epidemiology in low and middle-income countries: A systematic review and meta-analysis of the prevalence of poor sleep quality and sleep duration. Sleep Health 2018, 4, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Chien, P.L.; Su, H.F.; Hsieh, P.C.; Siao, R.Y.; Ling, P.Y.; Jou, H.J. Sleep Quality among Female Hospital Staff Nurses. Sleep Disord. 2013, 283490. [Google Scholar] [CrossRef] [PubMed]
- Heckman, C.J.; Kloss, J.D.; Feskanich, D.; Culnan, E.; Schernhammer, E.S. Associations Among Rotating Night Shift Work, Sleep, and Skin Cancer in Nurses’ Health Study II Participants. Occup. Environ. Med. 2017, 74, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Gadie, A.; Shafto, M.; Leng, Y.; Kievit, R.A. How are age-related differences in sleep quality associated with health outcomes? An epidemiological investigation in a UK cohort of 2406 adults. BMJ Open 2017, 7, e014920. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.L.C.; Wu, M.P.; Ho, C.H.; Wang, J.J. Risks of treated anxiety, depression, and insomnia among nurses: A nationwide longitudinal cohort study. PLoS ONE 2018, 13, e0204224. [Google Scholar] [CrossRef] [PubMed]
- An, F.R.; Qi, Y.K.; Zeng, J.Y.; Ding, Y.M.; Chiu, H.F.; Ungvari, G.S.; Newhouse, R.; Yu, D.S.; Lai, K.Y.; Xiang, Y.T. The Prevalence of Insomnia, Its Demographic Correlates, and Treatment in Nurses Working in Chinese Psychiatric and General Hospitals. Perspect. Psychiatr. Care 2016, 52, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Surani, S.; Murphy, J.; Shah, A. Sleepy nurses: Are we willing to accept the challenge today? Nurs. Adm. Q. 2007, 31, 146–151. [Google Scholar] [CrossRef]
- Sveinsdóttir, H. Self-assessed quality of sleep, occupational health, working environment, illness experience and job satisfaction of female nurses working different combination of shifts. Scand. J. Caring Sci. 2006, 20, 229–237. [Google Scholar] [CrossRef]
- Flo, E.; Pallesen, S.; Mageroy, N.; Moen, B.E.; Gronli, J.; Nordhus, I.H.; Bjorvatn, B. Shift Work Disorder in Nurses—Assessment, Prevalence and Related Health Problems. PLoS ONE 2012, 7, e33981. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Sun, D.M.; Li, C.B.; Tao, M.F. Influencing Factors for Sleep Quality Among Shift-working Nurses: A Cross-Sectional Study in China Using 3-factor Pittsburgh Sleep Quality Index. Asian Nurs. Res. 2016, 10, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Roskoden, F.C.; Krüger, J.; Vogt, L.J.; Gärtner, S.; Hannich, H.J.; Steveling, A.; Lerch, M.M.; Aghdassi, A.A. Physical Activity, Energy Expenditure, Nutritional Habits, Quality of Sleep and Stress Levels in Shift-Working Health Care Personnel. PLoS ONE 2017, 12, e0169983. [Google Scholar] [CrossRef] [PubMed]
- Gifkins, J.; Johnston, A.; Loudoun, R. The impact of shift work on eating patterns and self-care strategies utilised by experienced and inexperienced nurses. Chronobiol. Int. 2018, 35, 811–820. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Fuentes, M.C.; Molero, M.M.; Barragán, A.B.; Martos, Á.; Gázquez, J.J. Association with the Quality of Sleep and the Mediating Role of Eating on Self-Esteem in Healthcare Personnel. Nutrients 2019, 11, 321. [Google Scholar] [CrossRef] [PubMed]
- An, M.; Kim, J.; Pig, S.; Kim, S.H.; Hwang, Y.Y. Factors Affecting Sleep Quality of Clinical Nurses Working in a Hospital. Korean J. Adult Nurs. 2018, 30, 126–135. [Google Scholar] [CrossRef]
- Lallukka, T.; Sivertsen, B.; Kronholm, E.; Papelera, Y.S.; Overland, S.; Glow, N. Association of sleep duration and sleep quality with the physical, social, and emotional functioning among Australian adults. Sleep Health 2018, 4, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Sin, N.L.; Almeida, D.M.; Crain, T.L.; Kossek, E.E.; Berkman, L.F.; Buxton, O.M. Bidirectional, Temporal Associations of Sleep with Positive Events, Affect, and Stressors in Daily Life Across a Week. Ann. Behav. Med. 2017, 51, 402–415. [Google Scholar] [CrossRef] [PubMed]
- Holgado-Tello, F.P.; Amor, P.J.; Lasa-Aristu, A.; Domínguez-Sánchez, A.; Delgado, B. Two new brief versions of the Cognitive Emotion Regulation Questionnaireand its relationships with depression and anxiety. Ann. Psychol. 2018, 34, 458–464. [Google Scholar] [CrossRef]
- López-García, C.; Ruiz-Hernández, J.A.; Llor-Zaragoza, L.; Llor-Zaragoza, P.; Jiménez-Barbero, J.A. Violencia de usuarios y bienestar psicológico en profesionales de atención primaria de salud. Eur. J. Psychol. Appl. Leg. Context 2018, 10, 57–63. [Google Scholar] [CrossRef]
- Castellano, E.; Muñoz-Navarro, R.; Sol, M.; Spontón, C.; Medrano, L.A. Cognitive processes of emotional regulation, burnout and work engagement. Psicothema 2019, 31, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Klumpp, H.; Roberts, J.; Kapella, M.C.; Kennedy, A.E.; Kumar, A.; Phan, K.L. Subjective and Objective Sleep Quality Modulate Emotion Regulatory Brain Function in Anxiety and Depression. Depress. Anxiety 2017, 34, 651–660. [Google Scholar] [CrossRef] [PubMed]
- Motomura, Y.; Kitamura, S.; Oba, K.; Terasawa, Y.; Enomoto, M.; Katayose, Y.; Hida, A.; Moriguchi, Y.; Higuchi, S.; Mishima, K. Sleep debt elicits negative emotional reaction through diminished amygdala-anterior cingulate functional connectivity. PLoS ONE 2013, 8, e56578. [Google Scholar] [CrossRef]
- Gruber, R.; Cassoff, J. The interplay between sleep and emotion regulation: Conceptual framework empirical evidence and future directions. Curr. Psychiatry Rep. 2014, 16, 500. [Google Scholar] [CrossRef] [PubMed]
- Denis, D.; Akhtar, R.; Holding, B.C.; Murray, C.; Panatti, J.; Claridge, G.; Sadeh, A.; Barclay, N.L.; O’Leary, R.; Maughan, B.; et al. Externalizing behaviors and callous-unemotional traits: Different associations with sleep quality. J. Sleep Res. 2017, 40, zsx070. [Google Scholar] [CrossRef] [PubMed]
- Serrat, O. Understanding and Developing Emotional Intelligence. In Knowledge Solutions: Tools, Methods, and Approaches to Drive Organizational Performance; Springer: Singapore, 2017. [Google Scholar]
- Lee, J.H.; Ok, C.H. Reducing burnout and enhancing job satisfaction: Critical role of hotel employees’ emotional intelligence and emotional labor. Int. J. Hosp. Manag. 2012, 31, 1101–1112. [Google Scholar] [CrossRef]
- Bar-On, R. The Bar-On model of emotional-social intelligence (ESI). Psicothema 2006, 18, 13–25. [Google Scholar]
- Pérez-Fuentes, M.C.; Molero, M.M.; Gázquez, J.J.; Simón, M.M. Analysis of Burnout Predictors in Nursing: Risk and Protective Psychological Factors. Eur. J. Psychol. Appl. Leg. Context 2019, 11, 33–40. [Google Scholar] [CrossRef]
- Wersebe, H.; Lieb, R.; Meyer, A.H.; Hofer, P.; Gloster, A.T. The link between stress, well-being, and psychological flexibility during an Acceptance and Commitment Therapy self-help intervention. Int. J. Clin. Health Psychol. 2018, 18, 60–68. [Google Scholar] [CrossRef]
- Pérez-Fuentes, M.C.; Molero, M.M.; Gázquez, J.J.; Oropesa, N.F. The Role of Emotional Intelligence in Engagement in Nurses. Int. J. Environ. Res. Public Health 2018, 15, 1915. [Google Scholar] [CrossRef]
- Cabanach, R.G.; Souto-Gestal, A.; Fernández, R. Perfiles de regulación emocional y estrés académico en estudiantes de fisioterapia. Eur. J. Educ. Psychol. 2017, 10, 57–67. [Google Scholar] [CrossRef]
- Martos, A.; Pérez-Fuentes, M.C.; Molero, M.M.; Gázquez, J.J.; Simón, M.M.; Barragán, A.B. Burnout y engagement en estudiantes de Ciencias de la Salud. Eur. J. Investig. 2018, 8, 23–36. [Google Scholar] [CrossRef]
- Killgore, W.D. Self-reported sleep correlates with prefrontal-amygdala functional connectivity and emotional functioning. Sleep 2013, 36, 1597–1608. [Google Scholar] [CrossRef] [PubMed]
- Nowack, K. Sleep, emotional intelligence, and interpersonal effectiveness: Natural bedfellows. Consult. Psychol. J. Pract. 2017, 69, 66–79. [Google Scholar] [CrossRef]
- Lemola, S.; Ledermann, T.; Friedman, E.M. Variability of Sleep Duration Is Related to Subjective Sleep Quality and Subjective Well-Being: An Actigraphy Study. PLoS ONE 2013, 8, e71292. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Cheng, Y.; Germain, A.; Moul, D.E.; Franzen, P.L.; Fletcher, M.; Monk, T.H. Night-to-night sleep variability in older adults with and without chronic insomnia. Sleep Med. Rev. 2010, 11, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.W. The mediating role of sleep quality in the relationship between personality and subjective well-being. SAGE Open 2018, 1–10. [Google Scholar] [CrossRef]
- Amidu, N.; Issah, H.; Alhassan, M.; Nyagre, V.; Yahaya, W.; Mwinsanga, P.P.; Adams, Y. Stress, Anxiety and Sleep Disorder among Nurses: A Cross-Sectional Study of Rotation vs. Fixed Shift Workers. Int. Neuropsychiatr. Dis. J. 2018, 11, 1–12. [Google Scholar] [CrossRef]
- Kaplan, K.A.; Hirshman, J.; Hernandez, B.; Stefanick, M.L.; Hoffman, A.R.; Redline, S.; Ancoli-Israel, S.; Stone, K.; Friedman, L.; Zeitzer, J.M.; et al. When a gold standard isn’t so golden: Lack of prediction of subjective sleep quality from sleep polysomnography. Biol. Psychol. 2017, 123, 37–46. [Google Scholar] [CrossRef]
- Reed, D.L.; Sacco, W.P. Measuring Sleep Efficiency: What Should the Denominator Be? J. Clin. Sleep Med. 2016, 12, 263–266. [Google Scholar] [CrossRef]
- Macías, J.A.; Royuela, A. La versión española del índice de calidad de sueño de Pittsburgh. Inf. Psiquiátricas 1996, 146, 465–472. [Google Scholar]
- Royuela, A.; Macías, J.A. Propiedades clinimétricas de la version castellana del Cuestionario de Pittsburgh. Vigilia-Sueño 1997, 9, 81–94. [Google Scholar]
- Pérez-Fuentes, M.C.; Gázquez, J.J.; Mercader, I.; Molero, M.M. Brief Emotional Intelligence Inventory for Senior Citizens (EQ-i-20M). Psicothema 2014, 26, 524–530. [Google Scholar] [CrossRef]
- Bar-On, R.; Parker, J.D.A. The Bar-on Emotional Quotient Inventory: Youth Version (EQ-i:YV) Technical Manual; Multi-Health Systems, Inc.: Toronto, ON, Canada, 2000. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process. Analysis: A Regression-Based Approach; The Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Bar-On, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Construct | Dimensions | SSQ | SL | SD | HSE | SDi | USM | DD | INTRA | INTER | SM | ADAP |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PSQI Sleep quality | SSQ | ̶ | ||||||||||
| SL | 0.41 *** | ̶ | ||||||||||
| SD | 0.49 *** | 0.25 *** | ̶ | |||||||||
| HSE | 0.07 * | 0.07 * | 0.07 * | ̶ | ||||||||
| SDi | 0.31 *** | 0.27 *** | 0.23 *** | 0.00 | ̶ | |||||||
| USM | 0.23 *** | 0.27 *** | 0.16 *** | 0.01 | 0.23 *** | ̶ | ||||||
| DD | 0.29 *** | 0.21 *** | 0.23 *** | −0.02 | 0.31 *** | 0.19 *** | ̶ | |||||
| EQi-M-20 <Emotional intelligence | INTRA | −0.09 ** | −0.04 | −0.04 | 0.01 | −0.03 | 0.03 | −0.05 | ̶ | |||
| INTER | −0.00 | 0.00 | −0.00 | −0.02 | 0.01 | 0.00 | 0.01 | 0.37 *** | ̶ | |||
| SM | −0.15 *** | −0.10 *** | −0.11 *** | 0.08 ** | −0.16 *** | −0.12 *** | −0.19 *** | −0.00 | 0.06 * | ̶ | ||
| ADAP | −0.04 | −0.02 | −0.00 | −0.01 | −0.06 * | −0.03 | −0.10 ** | 0.40 *** | 0.57 *** | 0.04 | ̶ | |
| MO | −0.17 *** | −0.11 *** | −0.09 ** | −0.01 | −0.17 *** | −0.13 *** | −0.23 *** | 0.36 *** | 0.35 *** | 0.19 *** | 0.54 *** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Fuentes, M.d.C.; Molero Jurado, M.d.M.; Simón Márquez, M.d.M.; Barragán Martín, A.B.; Gázquez Linares, J.J. Emotional Effects of the Duration, Efficiency, and Subjective Quality of Sleep in Healthcare Personnel. Int. J. Environ. Res. Public Health 2019, 16, 3512. https://doi.org/10.3390/ijerph16193512
Pérez-Fuentes MdC, Molero Jurado MdM, Simón Márquez MdM, Barragán Martín AB, Gázquez Linares JJ. Emotional Effects of the Duration, Efficiency, and Subjective Quality of Sleep in Healthcare Personnel. International Journal of Environmental Research and Public Health. 2019; 16(19):3512. https://doi.org/10.3390/ijerph16193512
Chicago/Turabian StylePérez-Fuentes, María del Carmen, María del Mar Molero Jurado, María del Mar Simón Márquez, Ana Belén Barragán Martín, and José Jesús Gázquez Linares. 2019. "Emotional Effects of the Duration, Efficiency, and Subjective Quality of Sleep in Healthcare Personnel" International Journal of Environmental Research and Public Health 16, no. 19: 3512. https://doi.org/10.3390/ijerph16193512
APA StylePérez-Fuentes, M. d. C., Molero Jurado, M. d. M., Simón Márquez, M. d. M., Barragán Martín, A. B., & Gázquez Linares, J. J. (2019). Emotional Effects of the Duration, Efficiency, and Subjective Quality of Sleep in Healthcare Personnel. International Journal of Environmental Research and Public Health, 16(19), 3512. https://doi.org/10.3390/ijerph16193512