The Angle of Trunk Rotation in School Children: A Study from an Idiopathic Scoliosis Screening. Prevalence and Optimal Age Screening Value

 , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size
2.2. Research Procedure
3. Results
3.1. Demographics
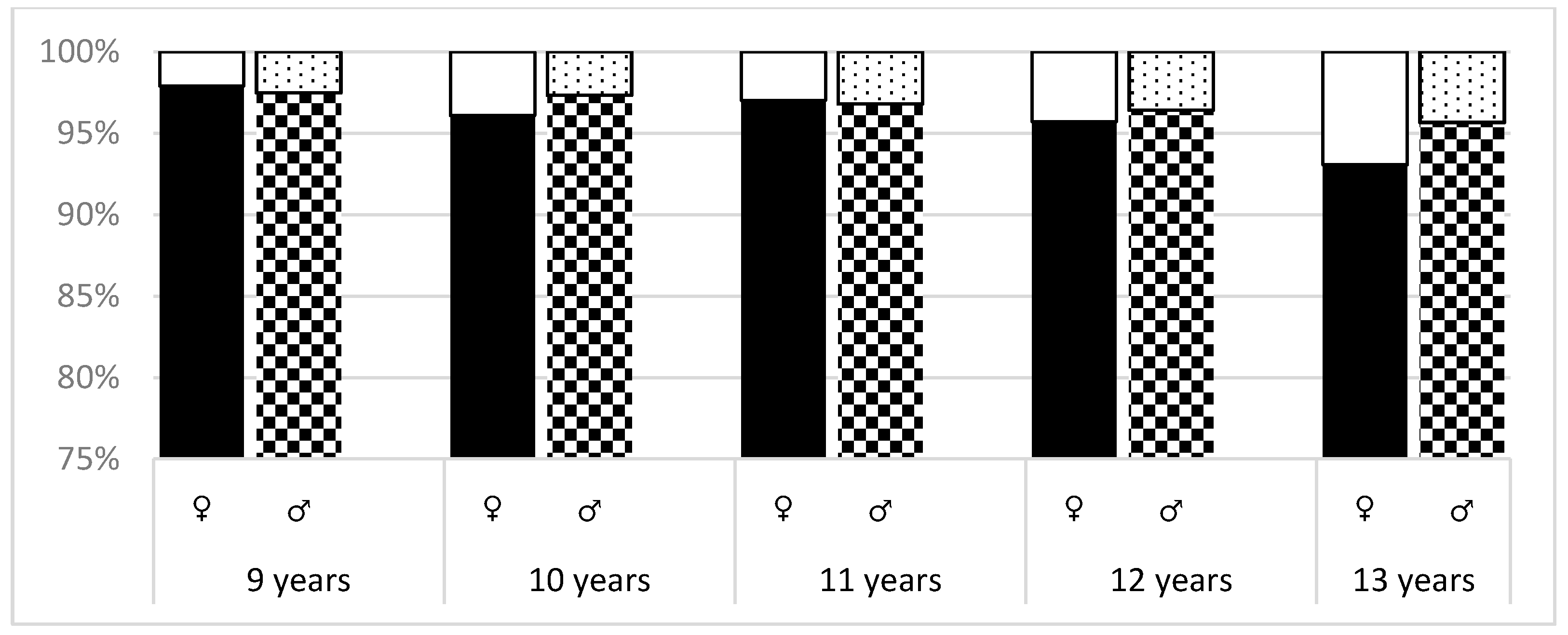
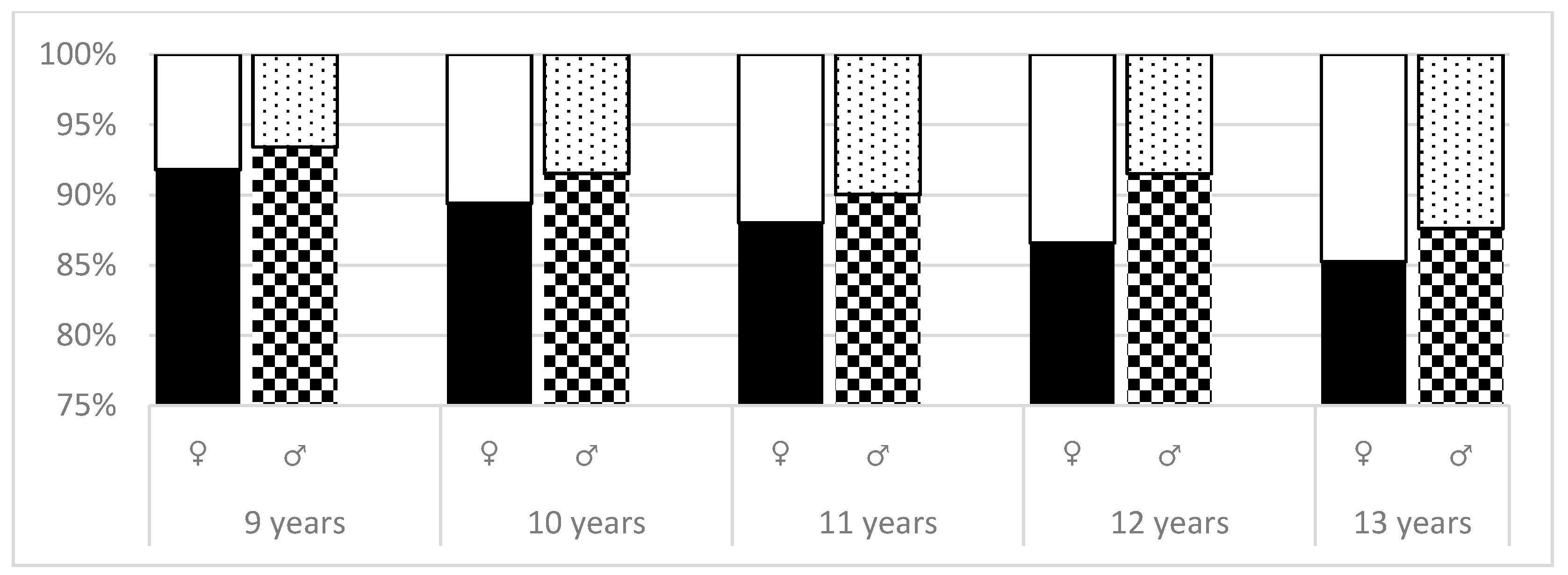
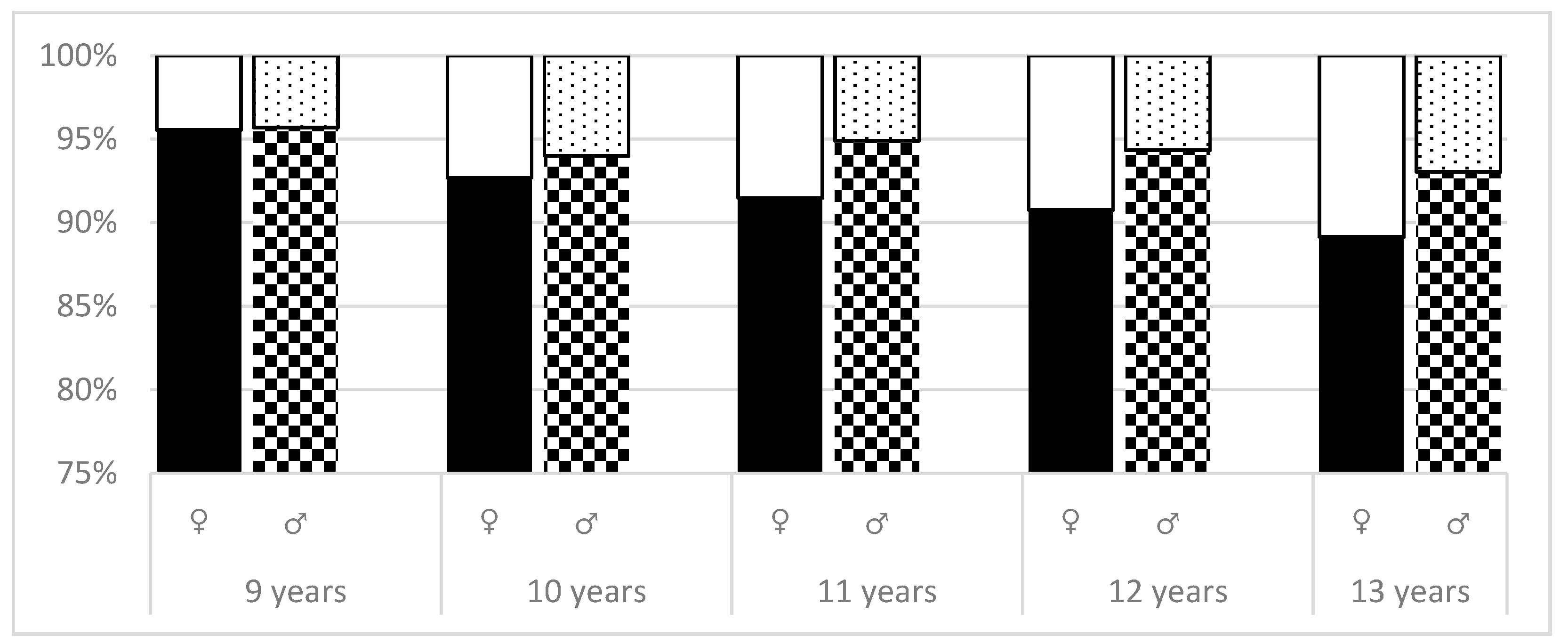
3.2. Prevalence
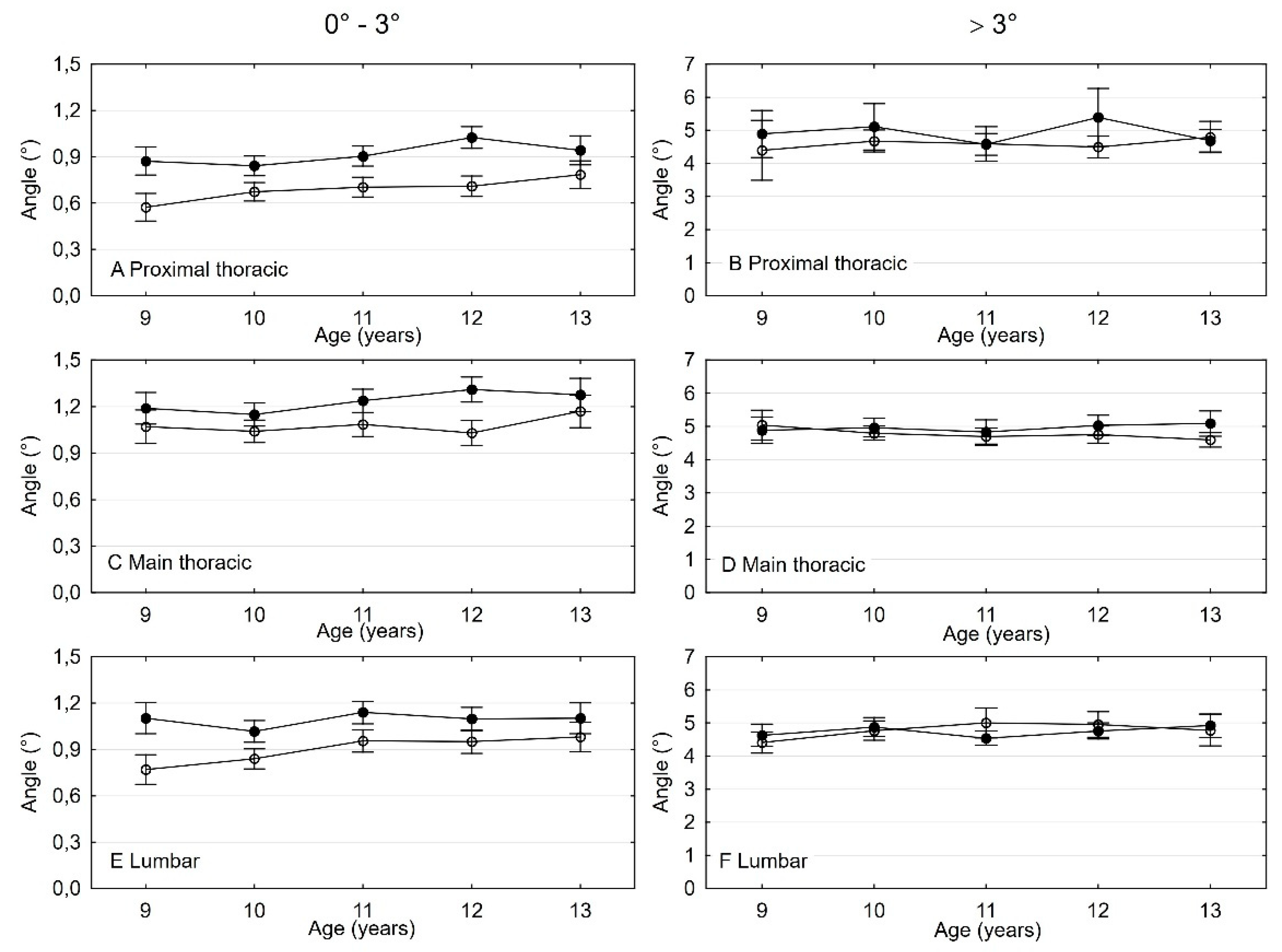
3.3. The Difference and Comparison in ATR Values Between Age and Sex
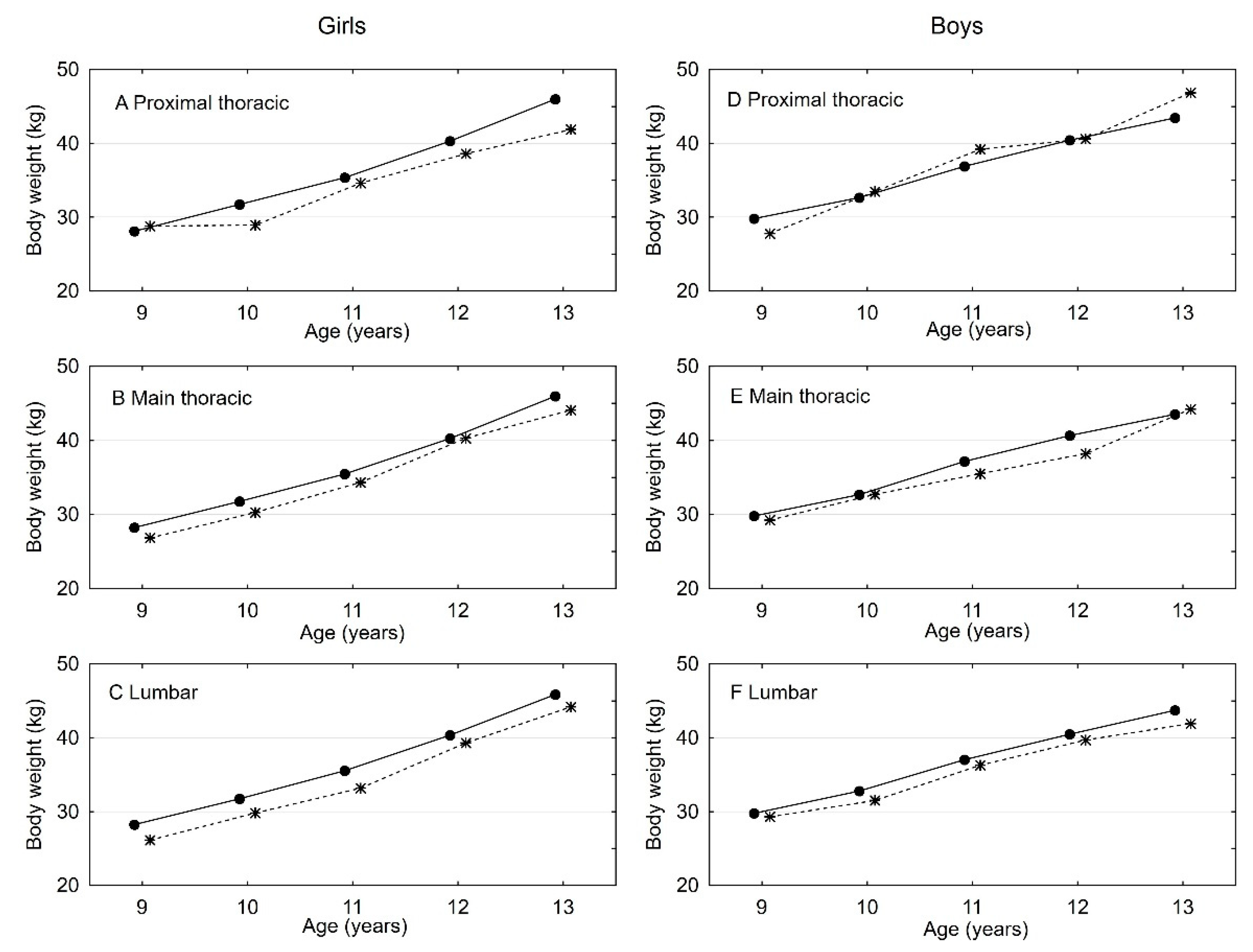
3.4. The Difference and Comparison in Body Weight Values Between Age and Sex
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hideki, S.; Terufumi, K.; Yuichiro, A.; Akira, I.; Katsuhisa, Y.; Yoichi, M.I.; Iwasaki, N.; Kanai, S. Automated noninvasive detection of idiopathic scoliosis in children and adolescents: A principle validation study. Sci. Rep. 2018. [Google Scholar] [CrossRef]
- Fong, D.Y.T.; Lee, C.F.; Cheung, K.M.C.; Cheng, J.C.Y.; Ng, B.K.W.; Lam, T.P.; Luk, K.D.K. A meta-analysis of the clinical effectiveness of school scoliosis screening. Spine 2010, 35, 1061–1071. [Google Scholar] [CrossRef] [PubMed]
- Asher, M.A.; Burton, D.C. Adolescent idiopathic scoliosis: Natural history and long term treatment effects. Scoliosis 2006, 1, 2. [Google Scholar] [CrossRef] [PubMed]
- Scoliosis Research Society (U.S.). Scoliosis: A Handbook for Patients; The Society: Park Ridge, IL, USA, 1986. [Google Scholar]
- Richards, B.S.; Beaty, J.H.; Thompson, G.H.; Willis, R.B. Estimating the effectiveness of screening for scoliosis. Pediatrics 2008, 121, 1296–1297. [Google Scholar] [CrossRef] [PubMed]
- Richards, B.S.; Vitale, M.G. Screening for idiopathic scoliosis in adolescents. An information statement. J. Bone Joint Surg. 2008, 90, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Ueno, M.; Takaso, M.; Nakazawa, T.; Imura, T.; Saito, W.; Shintani, R.; Kotani, T. A 5-year epidemiological study on the prevalence rate of idiopathic scoliosis in Tokyo: School screening of more than 250,000 children. J. Orthop. Sci. 2011, 16, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, S.L.; Dolan, L.A.; Wright, J.G.; Dobbs, M.B. Effects of bracing in adolescents with idiopathic scoliosis. N. Engl. J. Mwd. 2013, 369, 1512–1521. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, R.E. Evaluation of the patient with deformity. In The Pediatric Spine: Principles and Practice; Weinstein, S.L., Ed.; Raven Press: New York, NY, USA, 1994; pp. 185–224. [Google Scholar]
- Grivas, T.B.; Wade, M.H.; Negrini, S.; O’Brien, J.P.; Maruyama, T.; Hawes, M.C.; Rigo, M.; Weiss, H.R.; Kotwicki, T.; Vasilidas, E.S.; et al. SOSORT consensus paper: School screening for scoliosis. Where are we today? Scoliosis 2007. [Google Scholar] [CrossRef]
- Huang, S.C. Cut off point of the scoliometer in school scoliosis screening. Spine 1997, 22, 1985–1989. [Google Scholar] [CrossRef]
- Grivas, T.B.; Vasiliadis, E.S.; Mihas, C.; Triantafyllopoulos, G.; Kaspiris, A. Trunk asymmetry in juveniles. Scoliosis 2008. [Google Scholar] [CrossRef]
- Coelho, D.M.; Bonagamba, G.H.; Oliveira, A.S. Scoliometer measurements of patients with idiopathic scoliosis. Braz. J. Phys. Ther. 2013, 17, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Amendt, L.E.; Ause-Ellias, K.L.; Lundahl Eybers, J.; Wadsworth, C.T.; Nielsen, D.H.; Weinstein, S.L. Validity and Reliability Testing of the Scoliometer. Phys. Ther. 1990, 70, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Balague, F.; Troussier, B.; Salminen, J.J. Non-specific low back pain in children and adolescents: Risk factors. Eur. Spine, J. 1999, 8, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Konieczny, M.R.; Senyurt, H.; Krauspe, R. Epidemiology of adolescent idiopathic scoliosis. J. Child. Orthop. 2013, 7, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Chowanska, J.; Kotwicki, T.; Rosadzinski, K.; Sliwinski, Z. School screening for scoliosis: Can surface topography replace examination with scoliometer. Scoliosis 2012, 7, 9. [Google Scholar] [CrossRef] [PubMed]
- Bunnell, W.P. Outcome of spinal screening. Spine 1993, 18, 1572–1580. [Google Scholar] [CrossRef] [PubMed]
- Cote, P.; Kreitz, B.G.; Caissidy, J. Study of the diagnostic accuracy and realibity of scoliometer and Adam’s forward bend test. Spine 1998, 23, 796–802. [Google Scholar] [CrossRef]
- Bunell, W.P. Selective screening for scoliosis. Clin. Orthop. Relat. Res. 2005, 434, 40–45. [Google Scholar] [CrossRef]
- Bunnel, P.W. An objective criterion for scoliosis screening. J. Bone Surg. 1984, 66, 1381–1386. [Google Scholar] [CrossRef]
- Grivas, T.B.; Vasiliadis, E.S.; Koufopoulos, G.; Triantafyllopoulos, G.; Mouzakis, V. Study of trunk asymmetry in normal children and adolescents. Scoliosis 2006, 1, 19. [Google Scholar] [CrossRef]
- Grossman, D.C.; Curry, S.J.; Owens, D.K.; Barry, M.J.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W.; Kemper, A.R.; Krist, A.H.; Landefeld, C.S.; et al. Screening for adolescent idiopathic scoliosis: US preventive services task force recommendation statement. Jama 2018, 319, 165–172. [Google Scholar] [PubMed]
- Kotwicki, T.; Negrini, S.; Zaina, F.; Grivas, T.B.; Rigo, M.; Maruyama, T.; Durmala, J. Methology of evaluation od morphology of the spineand the trunk in idiopathic scoiliosis and other spinal deformities – 6th sosort consensus paper. Scoliosis 2009. [Google Scholar] [CrossRef] [PubMed]
- Smith, F.M.; Latchford, G.J.; Hall, R.M.; Dickson, R.A. Do chronic medical conditions increase the risk of eating disorder? A cross-sectional investigation of eating pathology in adolescent females with scoliosis and diabetes. J. Adolesc. Health 2008, 42, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.S.K.; Lee, W.T.K.; Tse, Y.K.; Tang, S.P.; Lee, K.M.; Guo, X.; Cheng, J.C.Y. Abnormal peri-pubertal anthropometric measurements and growth pattern in adolescent idiopathic scoliosis: A study of 598 patients. Spine 2003, 28, 2152–2157. [Google Scholar] [CrossRef] [PubMed]
- Kyoungkyu, J.; Dong-il, K. The association between low body weight and scoliosis among Korean Elementary school students. Int. J. Environ. Res. Public Health 2018, 15, 2613. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Female (n = 3440) | Male (n = 3410) | p-Value of Difference * | ||||
|---|---|---|---|---|---|---|---|
| Parameters | Mean | Min–Max | SD | Mean | Min–Max | SD | p |
| Age (years) | 10.98 | 9–13 | 1.23 | 10.99 | 9–13 | 1.23 | 0.5991 |
| Mass (kg) | 35.93 | 16–89 | 10.15 | 36.66 | 16.8–90 | 10.15 | 0.0029 |
| Height (cm) | 140.84 | 114–179 | 9.91 | 141.25 | 114–174.5 | 9.03 | 0.0735 |
| BMI | 17.84 | 7.2–38.5 | 3.32 | 18.13 | 11.1–42.0 | 9.91 | 0.0004 |
| Level 1 (°) | 1.08 | 0–15 | 1.28 | 0.82 | 0–10 | 1.16 | <00001 |
| Level 2 (°) | 1.67 | 0–21 | 1.66 | 1.41 | 0–12 | 1.51 | <0.0001 |
| Level 3 (°) | 1.39 | 0–10 | 1.44 | 1.13 | 0–13 | 1.37 | <0.0001 |
| N (100%) | ATR = 5° | ||
|---|---|---|---|
| N | % | ||
| Level 1 ATR > 3° | N = 246 | 71 | 28.9 |
| Level 2 ATR > 3° | N = 719 | 226 | 31.5 |
| Level 3 ATR > 3° | N = 473 | 157 | 33.2 |
| Level 1 ATR ≥ 0° | N = 6850 | 71 | 1 |
| Level 2 ATR ≥ 0° | N = 6850 | 226 | 3.3 |
| Level 3 ATR ≥ 0° | N = 6850 | 157 | 2.3 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adamczewska, K.; Wiernicka, M.; Malchrowicz-Mośko, E.; Małecka, J.; Lewandowski, J. The Angle of Trunk Rotation in School Children: A Study from an Idiopathic Scoliosis Screening. Prevalence and Optimal Age Screening Value. Int. J. Environ. Res. Public Health 2019, 16, 3426. https://doi.org/10.3390/ijerph16183426
Adamczewska K, Wiernicka M, Malchrowicz-Mośko E, Małecka J, Lewandowski J. The Angle of Trunk Rotation in School Children: A Study from an Idiopathic Scoliosis Screening. Prevalence and Optimal Age Screening Value. International Journal of Environmental Research and Public Health. 2019; 16(18):3426. https://doi.org/10.3390/ijerph16183426
Chicago/Turabian StyleAdamczewska, Katarzyna, Marzena Wiernicka, Ewa Malchrowicz-Mośko, Joanna Małecka, and Jacek Lewandowski. 2019. "The Angle of Trunk Rotation in School Children: A Study from an Idiopathic Scoliosis Screening. Prevalence and Optimal Age Screening Value" International Journal of Environmental Research and Public Health 16, no. 18: 3426. https://doi.org/10.3390/ijerph16183426
APA StyleAdamczewska, K., Wiernicka, M., Malchrowicz-Mośko, E., Małecka, J., & Lewandowski, J. (2019). The Angle of Trunk Rotation in School Children: A Study from an Idiopathic Scoliosis Screening. Prevalence and Optimal Age Screening Value. International Journal of Environmental Research and Public Health, 16(18), 3426. https://doi.org/10.3390/ijerph16183426