School Absenteeism, Health-Related Quality of Life [HRQOL] and Happiness among Young Adults Aged 16–26 Years

 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
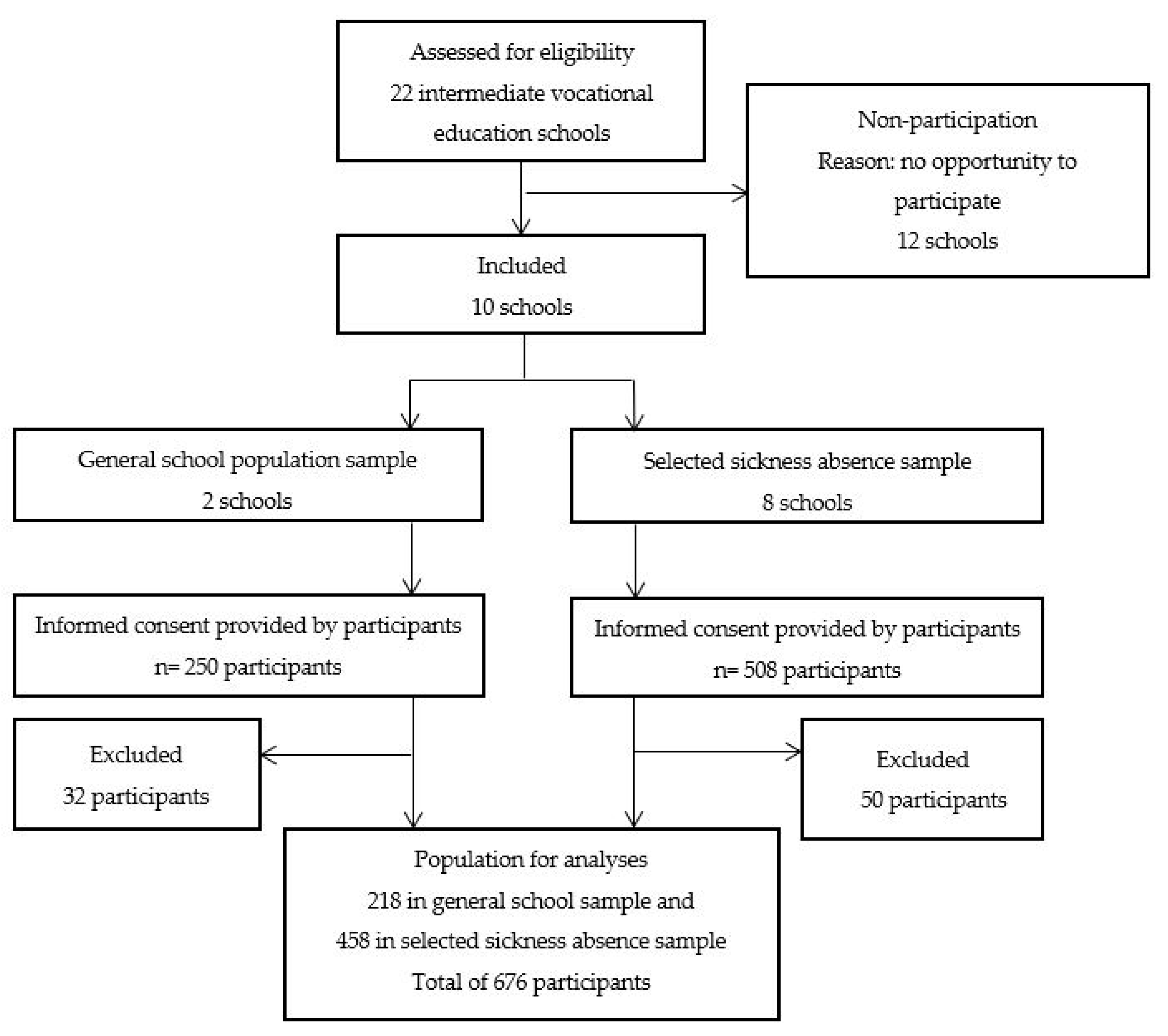
2.2. Setting and Study Population
2.3. Measurements
2.4. Data Analyses
3. Results
3.1. Students’ Characteristics
3.2. Mental HRQOL
3.3. Physical HRQOL
3.4. Happiness
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mojtabai, R.; Olfson, M.; Han, B. National trends in the prevalence and treatment of depression in adolescents and young adults. Pediatrics 2016, 138, e20161878. [Google Scholar] [CrossRef] [PubMed]
- Park, M.J.; Scott, J.T.; Adams, S.H.; Brindis, C.D.; Irwin, C.E. Adolescent and young adult health in the united states in the past decade: Little improvement and young adults remain worse off than adolescents. J. Adolesc. Health 2014, 55, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Maynard, B.R.; Vaughn, M.G.; Nelson, E.J.; Salas-Wrigh, C.P.; Heyne, D.A.; Kremer, K.P. Truancy in the united states: Examining temporal trends and correlates by race, age, and gender. Child Youth Serv. Rev. 2017, 81, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Finning, K.; Ukoumunne, O.C.; Ford, T.; Danielsson-Waters, E.; Shaw, L.; De Jager, I.R.; Stentiford, L.; Moore, D.A. The association between child and adolescent depression and poor attendance at school: A systematic review and meta-analysis. J. Affect. Dis. 2019, 245, 928–938. [Google Scholar] [CrossRef] [PubMed]
- Dembo, R.; Krupa, J.M.; Wareham, J.; Schmeidler, J.; DiClemente, R.J. A multigroup, longitudinal study of truant youths, marijuana use, depression, and std-associated sexual risk behavior. J. Child Adoles. Subst. 2017, 26, 192–204. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kearney, C.A. School absenteeism and school refusal behavior in youth: A contemporary review. Clin. Psychol. Rev. 2008, 28, 451–471. [Google Scholar] [CrossRef] [PubMed]
- Eaton, D.K.; Brener, N.; Kann, L.K. Associations of health risk behaviors with school absenteeism. Does having permission for the absence make a difference? J. Sch. Health 2008, 78, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Bannink, R.; Broeren, S.; Heydelberg, J.; van’t Klooster, E.; Raat, H. Depressive symptoms and clustering of risk behaviours among adolescents and young adults attending vocational education: A cross-sectional study. BMC Public Health 2015, 15, 396. [Google Scholar] [CrossRef]
- Evans, D.R. Enhancing quality-of-life in the population at large. Soc. Indic. Res. 1994, 33, 47–88. [Google Scholar] [CrossRef]
- Osoba, D.A.K.M. Meaningful differences. In Assessing Quality of Life in Clinical Trials; Oxford Press: New York, NY, USA, 2005; Volume 2, pp. 244–257. [Google Scholar]
- Jorngarden, A.; Wettergen, L.; von Essen, L. Measuring health-related quality of life in adolescents and young adults: Swedish normative data for the sf-36 and the hads, and the influence of age, gender, and method of administration. Health Qual. Life Outcomes 2006, 4, 91. [Google Scholar] [CrossRef][Green Version]
- Franquelo-Morales, P.; Sanchez-Lopez, M.; Notario-Pacheco, B.; Miota-Ibarra, J.; Lahoz-Garcia, N.; Gomez-Marcos, M.A.; Martinez-Vizcaino, V. Association between health-related quality of life, obesity, fitness, and sleep quality in young adults: The Cuenca adult study. Behav. Sleep Med. 2018, 16, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A. Happiness and health. Annu. Rev. Public Health 2019, 40, 339–359. [Google Scholar] [CrossRef] [PubMed]
- Gezondheidsmonitor Jeugd. Available online: https://www.monitorgezondheid.nl/vragenlijsten/vragenlijsten-jeugd (accessed on 2 April 2019).
- Keppens, G.; Spruyt, B. Truancy in Europe: Does the type of educational system matter? Eur. J. Educ. 2018, 53, 414–426. [Google Scholar] [CrossRef]
- NJI. Cijfers Schoolverzuim [Numbers on School Absenteeism]. Available online: https://www.nji.nl/Cijfers-schoolverzuim (accessed on 29 July 2019).
- Pflug, V.; Schneider, S. School absenteeism: An online survey via social networks. Child Psychiatry Hum. Dev. 2016, 47, 417–429. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, M.G.; Maynard, B.R.; Salas-Wright, C.P.; Perron, B.E.; Abdon, A. Prevalence and correlates of truancy in the us: Results from a national sample. J. Adolesc. 2013, 36, 767–776. [Google Scholar] [CrossRef] [PubMed]
- Gottfried, M.A. The detrimental effects of missing school: Evidence from urban siblings. Am. J. Educ. 2011, 117, 147–182. [Google Scholar] [CrossRef]
- Rodwell, L.; Romaniuk, H.; Nilsen, W.; Carlin, J.B.; Lee, K.J.; Patton, G.C. Adolescent mental health and behavioural predictors of being neet: A prospective study of young adults not in employment, education, or training. Psychol. Med. 2018, 48, 861–871. [Google Scholar] [CrossRef]
- Suhrcke, M.C.D.P.N. The Impact of Health and Health Behaviours on Educational Outcomes in Highincome Countries: A Review of the Evidence; WHO Regional Office for Europe: Copenhagen, Denmark, 2011. [Google Scholar]
- Crede, M.; Roch, S.G.; Kieszczynka, U.M. Class attendance in college: A meta-analytic review of the relationship of class attendance with grades and student characteristics. Rev. Educ. Res. 2010, 80, 272–295. [Google Scholar] [CrossRef]
- Vanneste, Y.T.M.; Mathijssen, J.J.P.; van de Goor, L.A.M.; Rots-de Vries, M.C.; Feron, F.J.M. Extensive medical absenteeism among secondary school students: An observational study on their health condition from a biopsychosocial perspective. Open J. Prev. Med. 2015, 5, 111–121. [Google Scholar] [CrossRef][Green Version]
- De Ridder, K.A.; Pape, K.; Johnsen, R.; Holmen, T.L.; Westin, S.; Bjorngaard, J.H. Adolescent health and high school dropout: A prospective cohort study of 9000 norwegian adolescents (the young-hunt). PLoS ONE 2013, 8, e74954. [Google Scholar] [CrossRef]
- Schoeneberger, J.A. Longitudinal attendance patterns: Developing high school dropouts. Clear. House 2012, 85, 7–14. [Google Scholar] [CrossRef]
- NJI. Cijfers over Jeugd en Opvoeding—Voortijdig Schoolverlaten [Numbers on Youth and Parenting—Early School Leaving]. Available online: https://www.nji.nl/nl/Databank/Cijfers-over-Jeugd-en-Opvoeding/Cijfers-per-onderwerp/Voortijdig-schoolverlaten (accessed on 14 March 2019).
- De Witte, K.; Nicaise, I.; Lavrijsen, J.; Van Landeghem, G.; Lamote, C.; Van Damme, J. The impact of institutional context, education and labour market policies on early school leaving: A comparative analysis of EU countries. Eur. J. Educ. 2013, 48, 331–345. [Google Scholar] [CrossRef]
- UNESCO. International Standard Classification of Education—ISCED 2011; UNESCO Institute for Statistics: Montreal, QC, Canada, 2012. [Google Scholar]
- Berzin, S.C. Vulnerability in the transition to adulthood: Defining risk based on youth profiles. Child Youth Serv. Rev. 2010, 32, 487–495. [Google Scholar] [CrossRef]
- Van der Vlis, M.K.; Lugtenberg, M.; Vanneste, Y.T.M.; Berends, W.; Mulder, W.; Bannink, R.; Van Grieken, A.; Raat, H.; de Kroon, M.L.A. Medical advice for sick-reported students (mass) in intermediate vocational education schools: Design of a controlled before-and-after study. BMC Public Health 2017, 17, 608. [Google Scholar] [CrossRef] [PubMed]
- National Center for Education Statistics. Status and Trends in the Education of Racial and Ethnic Groups. Available online: https://nces.ed.gov/programs/raceindicators/guide.asp (accessed on 3 September 2019).
- Balfanz, R.; Byrnes, V. The Importance of Being in School: A Report on Absenteeism in the Nation’s Public Schools; Johns Hopkins University Center for Social Organization of Schools: Baltimore, MD, USA, 2012. [Google Scholar]
- Ware, J.E.; Kosinski, M.; Keller, S.D. A 12-item short-form health survey—Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Galenkamp, H.; Stronks, K.; Mokkink, L.B.; Derks, E.M. Measurement invariance of the sf-12 among different demographic groups: The helius study. PLoS ONE 2018, 13, e0203483. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Khalek, A.M. Measuring happiness with a single-item scale. Soc. Behav. Personal. 2006, 34, 139–149. [Google Scholar] [CrossRef]
- Norman, G.R.; Sloan, J.A.; Wyrwich, K.W. Interpretation of changes in health-related quality of life: The remarkable universality of half a standard deviation. Med. Care 2003, 41, 582–592. [Google Scholar] [CrossRef]
- Finning, K.; Ukoumunne, O.C.; Ford, T.; Danielson-Waters, E.; Shaw, L.; Romero De Jager, I.; Stentiford, L.; Moore, D.A. Review: The association between anxiety and poor attendance at school—A systematic review. Child Adolesc. Ment. Health 2019, 24, 205–216. [Google Scholar] [CrossRef]
- Wood, J.J.; Lynne-Landsman, S.D.; Langer, D.A.; Wood, P.A.; Clark, S.L.; Eddy, J.M.; Ialongo, N. School attendance problems and youth psychopathology: Structural cross-lagged regression models in three longitudinal data sets. Child Dev. 2012, 83, 351–366. [Google Scholar] [CrossRef]
- Finning, K.; Ford, T.; Moore, D.A.; Ukoumunne, O.C. Emotional disorder and absence from school: Findings from the 2004 British child and adolescent mental health survey. Eur. Child Adolesc. Psychiatry 2019. [Google Scholar] [CrossRef] [PubMed]
- Gase, L.N.; Kuo, T.; Coller, K.; Guerrero, L.R.; Wong, M.D. Assessing the connection between health and education: Identifying potential leverage points for public health to improve school attendance. Am. J. Public Health 2014, 104, E47–E54. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.; Lycett, K.; Olds, T.; Gold, L.; Wake, M. Use of time and adolescent health-related quality of life/well-being: Ascoping review. Acta Paediatr. 2017, 106, 1239–1245. [Google Scholar] [CrossRef] [PubMed]
- Michaud, P.A.; Delbos-Piot, I.; Narring, F. Silent dropouts in health surveys: Are nonrespondent absent teenagers different from those who participate in school-based health surveys? J. Adolesc. Health 1998, 22, 326–333. [Google Scholar] [CrossRef]


{kind=link}
| Total (N = 676) | 0 Days of Sickness (n = 115) | 1–4 Days of Sickness Absence (n = 275) | ≥5 Days of Sickness Absence (n = 286) | p-Value | |
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | ||
| School absenteeism | 0.000 | ||||
| Number of sick days in past 8 weeks | 5.4 (6.3) | n/a | 2.5 (1.1) | 10.3 (7.1) | |
| Missing n | 0 | ||||
| n (%) | n (%) | n (%) | n (%) | ||
| Truancy in past 4 weeks | 0.005 | ||||
| Never | 412 (60.8) | 85 (73.9) | 161 (58.8) | 165 (57.7) | |
| 1–5 h | 198 (29.2) | 17 (14.8) | 84 (30.7) | 96 (33.6) | |
| ≥6 h | 68 (10.0) | 13 (11.3) | 29 (10.6) | 25 (8.7) | |
| Missing n | 1 | ||||
| Age in years | 0.527 | ||||
| Mean (SD) | 18.5 (2.1) | 18.5 (2.2) | 18.5 (2.0) | 18.6 (2.1) | |
| Missing n | 2 | ||||
| n (%) | n (%) | n (%) | n (%) | ||
| Gender | 0.088 | ||||
| Boys | 176 (26.1) | 26 (22.8) | 63 (22.9) | 87 (30.4) | |
| Girls | 499 (73.9) | 88 (77.2) | 212 (77.1) | 199 (69.6) | |
| Missing n | 1 | ||||
| Country of birth | 0.108 | ||||
| The Netherlands | 617 (92.1) | 100 (87.7) | 250 (91.9) | 267 (94.0) | |
| Other | 53 (7.9) | 14 (12.3) | 22 (8.1) | 17 (6.0) | |
| Missing n | 6 | ||||
| Living situation | 0.064 | ||||
| At home with parents/caretakers | 597 (88.3) | 108 (93.9) | 244 (88.7) | 245 (85.7) | |
| Not at home with parents/caretakers | 79 (11.7) | 7 (6.1) | 31 (11.3) | 41 (14.3) | |
| Missing n | 0 | ||||
| Vocational Education level | 0.003 | ||||
| Starting level and level 1 | 47 (7.2) | 4 (3.6) | 18 (6.7) | 25 (9.1) | |
| Level 2 | 86 (13.1) | 25 (22.7) | 40 (14.9) | 21 (7.6) | |
| Level 3 | 82 (12.5) | 12 (10.9) | 31 (11.6) | 39 (14.1) | |
| Level 4 | 439 (67.1) | 69 (62.7) | 179 (66.8) | 191 (69.2) | |
| Missing n | 25 | ||||
| Debts | 0.101 | ||||
| None | 543 (81.8) | 95 (85.6) | 229 (84.5) | 219 (77.7) | |
| <500 euro | 50 (7.5) | 4 (3.6) | 17 (6.3) | 29 (10.3) | |
| >500 euro | 71 (10.7) | 12 (10.8) | 25 (9.2) | 34 (12.1) | |
| Missing n | 12 | ||||
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | ||
| SF-12/HRQOL | 0.000 | ||||
| Mental health composite | 45.8 (12.9) | 48.1 (11.1) | 47.8 (11.1) | 42.9 (14.1) | |
| Missing n | 0 | ||||
| Physical health composite | 50.8 (9.3) | 54.1 (6.0) | 52.1 (8.1) | 48.3 (10.7) | |
| Missing n | 0 | ||||
| Grade for happiness (range 0–10) | 0.015 | ||||
| Mean (SD) | 7.2 (1.6) | 7.4 (1.9) | 7.3 (1.5) | 7.0 (1.6) | |
| Missing n | 9 |
| SF-12 Mental Component Summary | ||||||
|---|---|---|---|---|---|---|
| Crude Model | Adjusted Model | |||||
| B | (95% CI) | p-Value | B | (95% CI) | p-Value | |
| School absenteeism | ||||||
| Number of sick days in past 8 weeks | ||||||
| Never | ref | ref | ||||
| 1–4 days | −0.06 | (−3.73; 3.62) | 0.976 | −0.34 | (−3.19; 2.52) | 0.818 |
| ≥5 days | −5.13 | (−8.84; −1.42) | 0.007 | −5.14 | (−8.02; −2.25) | 0.001 |
| Truancy in past 4 weeks | ||||||
| Never | ref | ref | ||||
| 1–5 h | −0.05 | (−2.72; 2.61) | 0.968 | 1.31 | (−0.92; 3.55) | 0.249 |
| ≥6 h | −4.70 | (−8.14; −1.26) | 0.007 | −3.84 | (−7.22; −0.47) | 0.026 |
| SF-12 Physical Component Summary | ||||||
|---|---|---|---|---|---|---|
| Crude Model | Adjusted Model | |||||
| B | (95% CI) | p-Value | B | (95% CI) | p-Value | |
| School absenteeism | ||||||
| Number of sick days in past 8 weeks | ||||||
| Never | ref | ref | ||||
| 1–4 days | −0.91 | (−3.51; 1.68) | 0.489 | −2.70 | (−4.74; −0.66) | 0.010 |
| ≥5 days | −5.87 | (−8.49; −3.25) | 0.000 | −6.86 | (−8.93; −4.80) | 0.000 |
| Truancy in past 4 weeks | ||||||
| Never | ref | ref | ||||
| 1–5 h | 1.83 | (−0.05; 3.71) | 0.057 | 2.98 | (1.38; 4.58) | 0.000 |
| ≥6 h | 1.71 | (−0.72; 4.14) | 0.168 | 2.63 | (0.21; 5.04) | 0.033 |
| Happiness | ||||||
|---|---|---|---|---|---|---|
| Crude Model | Adjusted Model | |||||
| B | (95% CI) | p-Value | B | (95% CI) | p-Value | |
| School absenteeism | ||||||
| Number of sick days in past 8 weeks | ||||||
| Never | ref | ref | ||||
| 1–4 days | 0.07 | (−0.41; 0.55) | 0.760 | −0.05 | (−0.42; 0.33) | 0.802 |
| ≥5 days | −0.34 | (−0.83; 0.14) | 0.167 | −0.35 | (−0.73; 0.03) | 0.068 |
| Truancy in past 4 weeks | ||||||
| Never | ref | ref | ||||
| 1–5 h | −0.17 | (−0.52; 0.18) | 0.343 | 0.04 | (−0.25; 0.34) | 0.783 |
| ≥6 h | −0.40 | (−0.85; 0.04) | 0.077 | −0.23 | (−0.67; 0.21) | 0.306 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van den Toren, S.J.; van Grieken, A.; Mulder, W.C.; Vanneste, Y.T.; Lugtenberg, M.; de Kroon, M.L.; Tan, S.S.; Raat, H. School Absenteeism, Health-Related Quality of Life [HRQOL] and Happiness among Young Adults Aged 16–26 Years. Int. J. Environ. Res. Public Health 2019, 16, 3321. https://doi.org/10.3390/ijerph16183321
van den Toren SJ, van Grieken A, Mulder WC, Vanneste YT, Lugtenberg M, de Kroon ML, Tan SS, Raat H. School Absenteeism, Health-Related Quality of Life [HRQOL] and Happiness among Young Adults Aged 16–26 Years. International Journal of Environmental Research and Public Health. 2019; 16(18):3321. https://doi.org/10.3390/ijerph16183321
Chicago/Turabian Stylevan den Toren, Suzanne J., Amy van Grieken, Wico C. Mulder, Yvonne TM Vanneste, Marjolein Lugtenberg, Marlou LA de Kroon, Siok Swan Tan, and Hein Raat. 2019. "School Absenteeism, Health-Related Quality of Life [HRQOL] and Happiness among Young Adults Aged 16–26 Years" International Journal of Environmental Research and Public Health 16, no. 18: 3321. https://doi.org/10.3390/ijerph16183321
APA Stylevan den Toren, S. J., van Grieken, A., Mulder, W. C., Vanneste, Y. T., Lugtenberg, M., de Kroon, M. L., Tan, S. S., & Raat, H. (2019). School Absenteeism, Health-Related Quality of Life [HRQOL] and Happiness among Young Adults Aged 16–26 Years. International Journal of Environmental Research and Public Health, 16(18), 3321. https://doi.org/10.3390/ijerph16183321