Feasibility and Reliability of Physical Fitness Tests among Colombian Preschool Children

 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design Study and Subjects
2.2. Procedures
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ruiz, J.R.; Castro-Piñero, J.; Artero, E.G.; Ortega, F.B.; Sjöström, M.; Suni, J.; Castillo, M.J. Predictive validity of health-related fitness in youth: A systematic review. Br. J. Sports Med. 2009, 43, 909–923. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Peña-Ibagon, J.C.; Martínez-Torres, J.; Tordecilla-Sanders, A.; Correa-Bautista, J.E.; Lobelo, F.; García-Hermoso, A. Handgrip strength cutoff for cardiometabolic risk index among Colombian children and adolescents: The FUPRECOL Study. Sci. Rep. 2017, 14, 42622. [Google Scholar] [CrossRef] [PubMed]
- Agostinis-Sobrinho, C.A.; Ramírez-Vélez, R.; García-Hermoso, A.; Moreira, C.; Lopes, L.; Oliveira-Santos, J.; Abreu, S.; Mota, J.; Santos, R. Low-grade inflammation and muscular fitness on insulin resistance in adolescents: Results from LabMed Physical Activity Study. Pediatr. Diabetes 2018, 19, 429–435. [Google Scholar] [CrossRef] [PubMed]
- García-Hermoso, A.; Ramírez-Campillo, R.; Izquierdo, M. Is Muscular Fitness Associated with Future Health Benefits in Children and Adolescents? A Systematic Review and Meta-Analysis of Longitudinal Studies. Sports Med. 2019, 49, 1079–1094. [Google Scholar] [CrossRef] [PubMed]
- Mintjens, S.; Menting, M.D.; Daams, J.G.; Van Poppel, M.N.; Roseboom, T.J.; Gemke, R.J. Cardiorespiratory fitness in childhood and adolescence affects future cardiovascular risk factors: A systematic review of longitudinal studies. Sports Med. 2018, 48, 2577–2605. [Google Scholar] [CrossRef] [PubMed]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef] [PubMed]
- García-Hermoso, A.; Cavero-Redondo, I.; Ramírez-Vélez, R.; Ruiz, J.; Ortega, F.B.; Lee, D.-C.; Martínez-Vizcaíno, V. Muscular strength as a predictor of all-cause mortality in apparently healthy population: A systematic review and meta-analysis of data from approximately 2 million men and women. Arch. Phys. Med. Rehabil. 2018, 99, 2100–2113. [Google Scholar] [CrossRef] [PubMed]
- Arsenault, J.E.; Mora-Plazas, M.; Forero, Y.; Lopez-Arana, S.; Jáuregui, G.; Baylin, A.; Gordon, P.M.; Villamor, E. Micronutrient and anthropometric status indicators are associated with physical fitness in Colombian schoolchildren. Br. J. Nutr. 2011, 105, 1832–1842. [Google Scholar] [CrossRef]
- Pillsbury, L.; Oria, M.; Pate, R. Fitness Measures and Health Outcomes in Youth; National Academies Press: Washington, DC, USA, 2013. [Google Scholar]
- Cadenas-Sanchez, C.; Martinez-Tellez, B.; Sanchez-Delgado, G.; Mora-Gonzalez, J.; Castro-Piñero, J.; Löf, M.; Ruiz, J.R.; Ortega, F.B. Assessing physical fitness in preschool children: Feasibility, reliability and practical recommendations for the PREFIT battery. J. Sci. Med. Sport 2016, 19, 910–915. [Google Scholar] [CrossRef]
- Henriksson, P.; Leppänen, M.H.; Henriksson, H.; Nyström, C.D.; Cadenas-Sanchez, C.; Ek, A. Physical fitness in relation to later body composition in pre-school children. J. Sci. Med. Sport 2019, 22, 574–579. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Rodrigues-Bezerra, D.; Correa-Bautista, J.E.; Izquierdo, M.; Lobelo, F. Reliability of health-related physical fitness tests among Colombian children and adolescents: The FUPRECOL study. PLoS ONE 2015, 10, e0140875. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Cadenas-Sanchez, C.; Lee, D.-C.; Ruiz, J.R.; Blair, S.N.; Sui, X. Fitness and Fatness as Health Markers through the Lifespan: An Overview of Current Knowledge. Prog. Prev. Med. 2018, 3, e0013. [Google Scholar] [CrossRef]
- Rivera, J.Á.; De Cossío, T.G.; Pedraza, L.S.; Aburto, T.C.; Sánchez, T.G.; Martorell, R. Childhood and adolescent overweight and obesity in Latin America: A systematic review. Lancet Diabetes Endocrinol. 2014, 2, 321–332. [Google Scholar] [CrossRef]
- Hallal, P.C.; Parra, D.C.; Azevedo, M.R.; Pratt, M.; Brownson, R.C. Research on physical activity and health: Where is Latin America. J. Phys. Act. Health 2010, 7 (Suppl. S2), S129–S130. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Cadenas-Sánchez, C.; Sánchez-Delgado, G.; Mora-González, J.; Martínez-Téllez, B.; Artero, E.G. Systematic review and proposal of a field-based physical fitness-test battery in preschool children: The PREFIT battery. Sports Med. 2015, 45, 533–555. [Google Scholar] [CrossRef]
- Cadenas-Sanchez, C.; Alcántara-Moral, F.; Sanchez-Delgado, G.; Mora-Gonzalez, J.; Martinez-Tellez, B.; Herrador-Colmenero, M. Assessment of cardiorespiratory fitness in preschool children: Adaptation of the 20 metres shuttle run test. Nutr. Hosp. 2014, 30, 1333–1343. [Google Scholar]
- Sanchez-Delgado, G.; Cadenas-Sanchez, C.; Mora-Gonzalez, J.; Martinez-Tellez, B.; Chillón, P.; Löf, M. Assessment of handgrip strength in preschool children aged 3 to 5 years. J. Hand Surg. Eur. 2015, 40, 966–972. [Google Scholar] [CrossRef]
- Oja, L.; Jürimäe, T. Assessment of motor ability of 4-and 5-year-old children. Am. J. Hum. Biol. 1997, 9, 659–664. [Google Scholar] [CrossRef]
- Walter, S.; Eliasziw, M.; Donner, A. Sample size and optimal designs for reliability studies. Stat. Med. 1998, 17, 101–110. [Google Scholar] [CrossRef]
- Australian Council for Health, Physical Education and Recreation. Australian Fitness Education Award for Students Aged 9–18: User’s Manual & Curriculum Ideas; Australian Council for Health, Physical Education and Recreation: Hindmarsh, SA, Australia, 1996; p. 15.
- Bland, J.M.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Artero, E.; Espana-Romero, V.; Castro-Pinero, J.; Ortega, F.; Suni, J.; Castillo-Garzon, M. Reliability of field-based fitness tests in youth. Int. J. Sports Med. 2011, 32, 159–169. [Google Scholar] [CrossRef]
- Castro-Piñero, J.; González-Montesinos, J.L.; Mora, J.; Keating, X.D.; Girela-Rejón, M.J.; Sjöström, M.; Ruiz, J.R. Percentile values for muscular strength field tests in children aged 6 to 17 years: Influence of weight status. J. Strength Cond Res. 2009, 23, 2295–2310. [Google Scholar] [CrossRef]
- De Miguel-Etayo, P.; Gracia-Marco, L.; Ortega, F.; Intemann, T.; Foraita, R.; Lissner, L.; Oja, L.; Barba, G.; Michels, N.; Tornaritis, M. Physical fitness reference standards in European children: The IDEFICS study. Int. J. Obes. 2014, 38 (Suppl. S2), S57–S66. [Google Scholar] [CrossRef]
- Cuenca-García, M.; Ortega, F.; Huybrechts, I.; Ruiz, J.; González-Gross, M.; Ottevaere, C.; Sjöström, M.; Dìaz, L.E.; Ciarapica, D.; Molnar, D. Cardiorespiratory fitness and dietary intake in European adolescents: The Healthy Lifestyle in Europe by Nutrition in Adolescence study. Br. J. Nutr. 2012, 107, 1850–1859. [Google Scholar] [CrossRef]
- Ulijaszek, S.J.; Kerr, D.A. Anthropometric measurement error and the assessment of nutritional status. Br. J. Nutr. 1999, 82, 165–177. [Google Scholar] [CrossRef]
- Ulijaszek, S.J.; Lourie, J.A. Anthropometric measurement. Anthropometry 2005, 14, 30. [Google Scholar]
- Nagy, E.; Vicente-Rodriguez, G.; Manios, Y.; Béghin, L.; Iliescu, C.; Censi, L. Harmonization process and reliability assessment of anthropometric measurements in a multicenter study in adolescents. Int. J. Obes. 2008, 32 (Suppl. S5), S58–S65. [Google Scholar] [CrossRef]
- Moreno, L.A.; Joyanes, M.; Mesana, M.I.; González-Gross, M.; Gil, C.M.; Sarría, A. Harmonization of anthropometric measurements for a multicenter nutrition survey in Spanish adolescents. Nutrition 2003, 19, 481–486. [Google Scholar] [CrossRef]
- Stomfai, S.; Ahrens, W.; Bammann, K.; Kovacs, E.; Mårild, S.; Michels, N.; Moreno, L.A.; Pohlabeln, H.; Siani, A.; Tornaritis, M.; et al. Intra-and inter-observer reliability in anthropometric measurements in children. Int. J. Obes. 2008, 32 (Suppl. S5), S58–S65. [Google Scholar] [CrossRef]
- Miguel-Etayo, D.; Mesana, M.; Cardon, G.; De Bourdeaudhuij, I.; Góźdź, M.; Socha, P.; Lateva, M.; Iotova, V.; Koletzko, B.V.; Duvinage, K.; et al. Reliability of anthropometric measurements in European preschool children: The ToyBox-study. Obes. Rev. 2014, 15, 67–73. [Google Scholar] [CrossRef]
- Cadenas-Sanchez, C.; Intemann, T.; Labayen, I.; Peinado, A.B.; Vidal-Conti, J.; Sanchis-Moysi, J. Physical fitness reference standards for preschool children: The PREFIT project. J. Sci. Med. Sport. 2019, 22, 430–437. [Google Scholar] [CrossRef]


{kind=link}
| Component | 1st Trial (T1) | 2nd Trial (T2) | Mean Differences (Standard Deviation T2–T1) * | p Value | Effect Size | pc |
|---|---|---|---|---|---|---|
| Morphologic | ||||||
| Age (years) | 4.00 (0.82) | - | - | - | - | - |
| Weight (kg) | 17.91 (2.82) | 17.92 (2.81) | 0.00 (0.14) | 0.484 | 0.074 | 0.998 |
| Height (m) | 1.05 (0.07) | 1.05 (0.07) | −0.00 (0.01) | 0.004 | 0.314 | 0.997 |
| Body mass index (kg/m2) | 16.01 (1.53) | 16.05 (1.52) | 0.04 (0.21) | 0.073 | 0.191 | 0.990 |
| Waist circumference (cm) | 52.50 (4.78) | 52.27 (4.80) | −0.22 (0.29) | 0.001 | 0.764 | 0.997 |
| Cardiorespiratory | ||||||
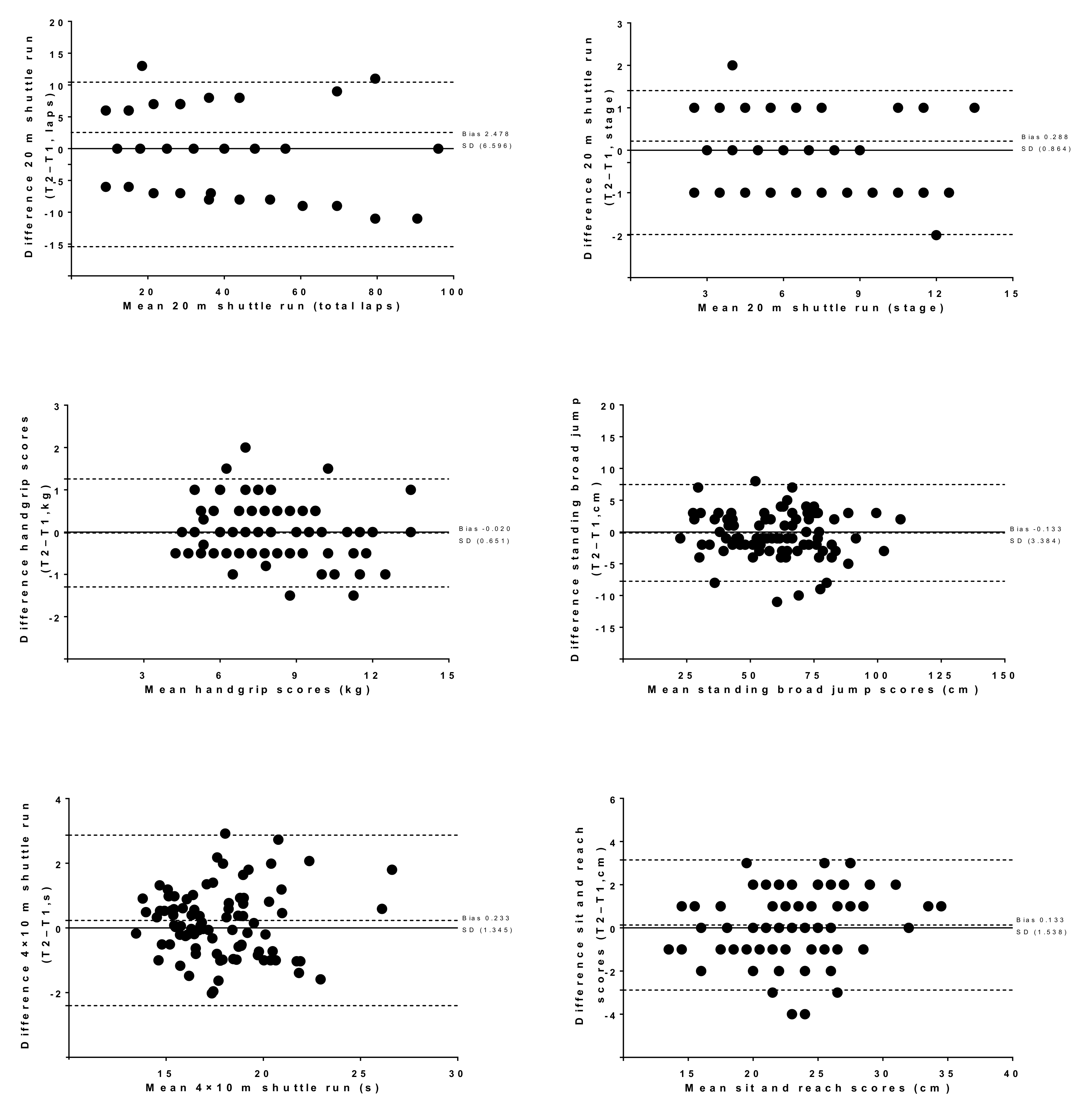
| 20 m shuttle run (laps) | 32.61 (19.98) | 35.08 (21.99) | 2.47 (6.59) | 0.001 | 0.311 | 0.944 |
| 20 m shuttle run (stage) | 5.88 (2.58) | 6.17 (2.73) | 0.28 (0.86) | 0.002 | 0.334 | 0.941 |
| Musculoskeletal | ||||||
| Handgrip (kg) | 7.77 (2.27) | 7.75 (2.21) | −0.02 (0.65) | 0.771 | 0.056 | 0.957 |
| Standing broad jump (cm) | 60.90 (18.71) | 60.76 (18.73) | −0.13 (3.88) | 0.745 | 0.034 | 0.978 |
| Motor and Flexibility | ||||||
| 4 × 10 m shuttle run (s) | 17.82 (2.69) | 18.05 (3.11) | 0.23 (1.34) | 0.102 | 0.174 | 0.890 |
| Sit and reach (cm) | 23.32 (3.93) | 23.45 (4.25) | 0.13 (1.53) | 0.412 | 0.087 | 0.929 |
| Component | 1st Trial (T1) | 2nd Trial (T2) | Mean Differences (Standard Deviation T2–T1) * | |||||
|---|---|---|---|---|---|---|---|---|
| Boys (n = 48) | Girls (n = 42) | Boys (n = 48) | Girls (n = 42) | Boys | p Value, (pc), Effect Size Boys | Girls | p Value, (pc), Effect Size Girls | |
| Morphologic | ||||||||
| Age (years) | 4.04 (0.82) | 3.95 (0.82) | - | - | - | - | - | - |
| Weight (kg) | 18.56 (2.93) | 17.35 (2.73) | 18.54 (2.91) | 17.35 (2.69) | −0.01 (0.15) | 0.422 (0.998) 0.117 | −0.01 (0.13) | 0.909 (0.998) 0.018 |
| Height (m) | 1.07 (0.07) | 1.04 (0.06) | 1.06 (0.07) | 1.04 (0.06) | −0.01 (0.01) | 0.031 (0.997) 0.321 | −0.01 (0.04) | 0.056 (0.997) 0.303 |
| Body mass index (kg/m2) | 16.13 (1.33) | 15.87 (1.75) | 16.16 (1.30) | 15.92 (1.74) | 0.03 (0.23) | 0.307 (0.983) 0.149 | 0.04 (0.18) | 0.105 (0.994) 0.256 |
| Waist circumference (cm) | 52.61 (4.93) | 52.37 (4.67) | 52.35 (4.97) | 52.18 (4.65) | −0.25 (0.23) | 0.001 (0.997) 1.050 | 0.30 (0.98) | 0.001 (0.996) 0.562 |
| Cardiorespiratory fitness | ||||||||
| 20–m shuttle run (stage) | 6.56 (2.87) | 5.11 (1.95) | 6.81 (3.12) | 5.45 (2.00) | 0.25 (0.86) | 0.055 (0.955) 0.289 | 0.33 (0.87) | 0.017 (0.889) 0.379 |
| 20–m shuttle run (laps) | 37.91 (22.71) | 26.54 (14.34) | 40.4 (25.73) | 29.00 (14.85) | 2.50 (7.00) | 0.017 (0.953) 0.291 | 2.45 (6.18) | 0.013 (0.897) 0.381 |
| Musculoskeletal | ||||||||
| Handgrip strength (kg) | 8.19 (2.46) | 7.30 (1.95) | 8.10 (2.39) | 7.35 (1.92) | −0.08 (0.58) | 0.303 (0.970) 0.222 | 0.05 (0.72) | 0.610 (0.930) 0.102 |
| Standing broad jump (cm) | 64.22 (17.63) | 57.09 (19.39) | 63.66 (17.75) | 57.45 (19.47) | −0.56 (3.48) | 0.268 (0.980) 0.162 | 0.35 (4.28) | 0.592 (0.975) 0.083 |
| Motor and Flexibility | ||||||||
| 4 × 10 m shuttle run (s) | 17.27 (2.58) | 18.44 (2.71) | 17.34 (2.44) | 18.87 (3.58) | 0.06 (0.96) | 0.650 (0.926) 0.066 | 0.42 (1.67) | 0.103 (0.854) 0.257 |
| Sit and reach (cm) | 23.45 (3.83) | 23.16 (4.07) | 23.18 (4.26) | 23.76 (4.27) | −0.27 (1.69) | 0.274 (0.910) 0.160 | 0.59 (1.19) | 0.002 (0.949) 0.501 |
| Components | Mean (SD) | Intra-Qbserver (T2 vs. T1) | |
|---|---|---|---|
| Absolute TEM | Relative TEM | ||
| Morphologic | |||
| Weight (kg) | 17.99 (2.87) | 0.112 | 0.625 |
| Height (m) | 1.06 (0.07) | 0.004 | 0.378 |
| Body mass index (kg/m2) | 16.03 (1.53) | 0.166 | 1.035 |
| Waist circumference (cm) | 52.39 (4.80) | 0.287 | 0.547 |
| Absolute TEM | ICC | ||
| Cardiorespiratory fitness | |||
| 20 m shuttle run (stage) | 5.89 (2.58) | − | 0.973 |
| 20 m shuttle run (laps) | 33.85 (20.99) | − | 0.975 |
| Musculoskeletal | |||
| Handgrip strength (kg) | 7.77 (2.23) | 0.502 | 0.984 |
| Standing broad jump (cm) | 58.75 (18.53) | 4.978 | 0.989 |
| Motor and Flexibility | |||
| 4 × 10 m shuttle run (s) | 17.94 (2.90) | 1.052 | 0.951 |
| Sit and reach (cm) | 22.69 (4.14) | 1.687 | 0.964 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amado-Pacheco, J.C.; Prieto-Benavides, D.H.; Correa-Bautista, J.E.; García-Hermoso, A.; Agostinis-Sobrinho, C.; María Alonso-Martínez, A.; Izquierdo, M.; Ramírez-Vélez, R. Feasibility and Reliability of Physical Fitness Tests among Colombian Preschool Children. Int. J. Environ. Res. Public Health 2019, 16, 3069. https://doi.org/10.3390/ijerph16173069
Amado-Pacheco JC, Prieto-Benavides DH, Correa-Bautista JE, García-Hermoso A, Agostinis-Sobrinho C, María Alonso-Martínez A, Izquierdo M, Ramírez-Vélez R. Feasibility and Reliability of Physical Fitness Tests among Colombian Preschool Children. International Journal of Environmental Research and Public Health. 2019; 16(17):3069. https://doi.org/10.3390/ijerph16173069
Chicago/Turabian StyleAmado-Pacheco, Julio Cesar, Daniel Humberto Prieto-Benavides, Jorge Enrique Correa-Bautista, Antonio García-Hermoso, César Agostinis-Sobrinho, Alicia María Alonso-Martínez, Mikel Izquierdo, and Robinson Ramírez-Vélez. 2019. "Feasibility and Reliability of Physical Fitness Tests among Colombian Preschool Children" International Journal of Environmental Research and Public Health 16, no. 17: 3069. https://doi.org/10.3390/ijerph16173069
APA StyleAmado-Pacheco, J. C., Prieto-Benavides, D. H., Correa-Bautista, J. E., García-Hermoso, A., Agostinis-Sobrinho, C., María Alonso-Martínez, A., Izquierdo, M., & Ramírez-Vélez, R. (2019). Feasibility and Reliability of Physical Fitness Tests among Colombian Preschool Children. International Journal of Environmental Research and Public Health, 16(17), 3069. https://doi.org/10.3390/ijerph16173069