Rethinking Suicide in Rural Australia: A study Protocol for Examining and Applying Knowledge of the Social Determinants to Improve Prevention in Non-Indigenous Populations

 ,
, {kind=link}
Abstract
:1. Introduction
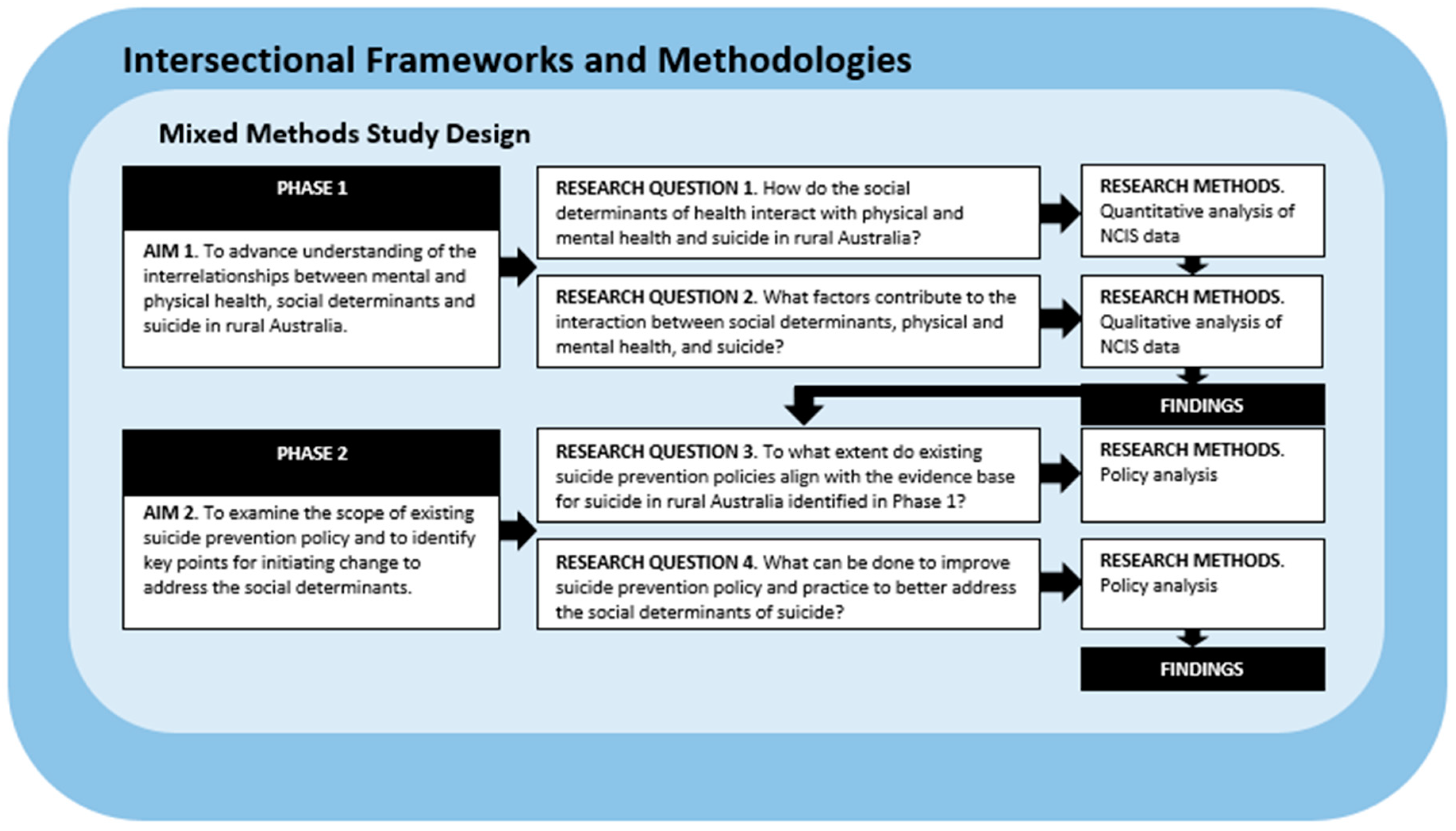
2. Research Design, Methodology, and Methods
2.1. Research Questions
- How do the social determinants of health interact with physical and mental health and suicide in rural Australia?
- What social processes or circumstances contribute to the interaction between social determinants, physical and mental health, and suicide in rural Australia?
- To what extent do suicide prevention policies align with the evidence about suicide in rural Australia?
- What can be done to improve suicide prevention policy and practice to better address the social determinants of suicide in rural Australia?
2.2. Theoretical Framework
2.3. Phase One—Study of Coronial Suicide Data from Regional and Remote Australia
2.3.1. Data Collection
2.3.2. Data Analysis
2.4. Phase Two—Policy Analysis
2.5. Ethical Considerations
3. Discussion
3.1. How do Mental and Physical Health, Social Determinants, and Suicide in Rural Australia Interrelate?
3.2. How can Policy and Services Better Address These Complex Experiences?
4. Strengths and Limitations of the Study
5. Significance
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hazell, T.; Dalton, H.; Caton, T.; Perkins, D. Rural Suicide and Its Prevention; Centre for Rural and Remote Mental Health: Orange, NSW, Australia, 2017; Available online: www.crrmh.com.au/content/uploads/RuralSuicidePreventionPaper_2017_WEB_FINAL.pdf (accessed on 9 July 2019).
- Knox, K.L.; Conwell, Y.; Caine, E.D. If suicide is a public health problem, what are we doing to prevent it? Am. J. Public Health 2004, 94, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.; Balfour, R.; Bell, R.; Marmot, M. Social determinants of mental health. Int. Rev. Psychiatr. 2014, 26, 392–407. [Google Scholar] [CrossRef] [PubMed]
- Page, A.; Morrell, S.; Taylor, R.; Carter, G.; Dudley, M. Divergent trends in suicide by socio-economic status in Australia. Soc. Psych. Psych. Epid. 2006, 41, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Too, L.S.; Law, P.C.; Spittal, M.J.; Page, A.; Milner, A. Widening socioeconomic inequalities in Australian suicide, despite recent declines in suicide rates. Soc. Psych. Psych. Epid. 2018, 53, 969–976. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, S.J.; Hooker, C. A ‘systems’ approach to suicide prevention: Radical change or doing the same things better? Public Health Res. Pract. 2017, 27, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Marušič, A. Seven steps to integrating suicidology. Crisis 2008, 29, 115–117. [Google Scholar] [CrossRef]
- Commission on Social Determinants of Health. Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health. Final Report of the Commission on Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2008; Available online: www.who.int/social_determinants/thecommission/finalreport/en/ (accessed on 9 July 2019).
- World Health Organization. Preventing Suicide: A Global Imperative; World Health Organization: Geneva, Switzerland, 2014; Available online: www.who.int/mental_health/suicide-prevention/world_report_2014/en/ (accessed on 9 July 2019).
- Australian Government Department of Health. National Suicide Prevention Trial: Background and Overview; Australian Government Department of Health: Canberra, ACT, Australia, 2017.
- Bourke, L. Toward understanding youth suicide in an Australian rural community. Soc. Sci. Med. 2003, 57, 2355–2365. [Google Scholar] [CrossRef]
- Hossain, D.; Eley, R.; Coutts, J.; Gorman, D. Mental health of farmers in Southern Queensland: Issues and support. Aust. J. Rural Health 2008, 16, 343–348. [Google Scholar] [CrossRef] [Green Version]
- Wexler, L. Looking across three generations of Alaska Natives to explore how culture fosters indigenous resilience. Transcult. Psychiatry 2014, 51, 73–92. [Google Scholar] [CrossRef]
- Inder, K.J.; Handley, T.E.; Johnston, A.; Weaver, N.; Coleman, C.; Lewin, T.J.; Slade, T.; Kelly, B.J. Determinants of suicidal ideation and suicide attempts: Parallel cross-sectional analyses examining geographical location. BMC Psychiatry 2014, 14, 208. [Google Scholar] [CrossRef]
- Brew, B.; Inder, K.; Allen, J.; Thomas, M.; Kelly, B. The health and wellbeing of Australian farmers: A longitudinal cohort study. BMC Public Health 2016, 16. [Google Scholar] [CrossRef] [PubMed]
- Alston, M.; Kent, J. The Big Dry: The link between rural masculinities and poor health outcomes for farming men. J. Sociol. 2008, 44, 133–147. [Google Scholar] [CrossRef]
- Berry, H.L.; Hogan, A.; Owen, J.; Rickwood, D.; Fragar, L. Climate change and farmers’ mental health: Risks and responses. Asia Pac. J. Public Health 2011, 23, 119S–132S. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N. Proximal, distal, and the politics of causation: What’s level got to do with it? Am. J. Public Health 2008, 98, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, S.J.; River, J. Beyond the medical model: Future directions for suicide intervention services. Int. J. Health Serv. 2018, 48, 189–203. [Google Scholar] [CrossRef] [PubMed]
- Bowleg, L. The problem with the phrase women and minorities: Intersectionality: An important theoretical framework for public health. Am. J. Public Health 2012, 102, 1267–1273. [Google Scholar] [CrossRef]
- Hankivsky, O. Health Inequities in Canada: Intersectional Frameworks and Practices; UBC Press: Vancouver, Canada, 2011. [Google Scholar]
- Mental Health Commission of New South Wales. Strategic Framework for Suicide Prevention in NSW 2018–2023; NSW Government: Sydney, Australia, 2018.
- National Mental Health Commission. Final Report: Expert Reference Group to COAG Working Group on Mental Health Reform on National Targets and Indicators for Mental Health Reform; National Mental Health Commission: Sydney, Australia, 2013. [Google Scholar]
- Suicide Prevention Australia. Transforming Suicide Prevention Research: A National Action Plan; Suicide Prevention Australia: Sydney, Australia, 2015; Available online: www.lifeline.org.au/static/uploads/files/transforming-suicide-prevention-research-a-national-action-plan-wfnudsxrjkqu.pdf (accessed on 9 July 2019).
- Grace, D. Intersectionality—Informed Mixed Methods Research: A Primer; The Institute for Intersectionality Research and Policy: Columbia, Canada, 2014; Available online: https://s3.amazonaws.com/academia.edu.documents/33687424/MixedMethodsPrimer_Final_Grace.pdf?response-content-disposition=inline%3B%20filename%3DIntersectionality-informed_Mixed_Method.pdf&X-Amz-Algorithm=AWS4-HMAC-SHA256&X-Amz-Credential=AKIAIWOWYYGZ2Y53UL3A%2F20190715%2Fus-east-1%2Fs3%2Faws4_request&X-Amz-Date=20190715T011330Z&X-Amz-Expires=3600&X-Amz-SignedHeaders=host&X-Amz-Signature=1943674ecc1551b24bb2963a38bdebc63b26d9a3075c8e0e0b310a9fd312d966 (accessed on 15 July 2019).
- Hankivsky, O.; Cormier, R. Intersectionality and public policy: Some lessons from existing models. Polit. Res. Quart. 2011, 64, 217–229. [Google Scholar] [CrossRef]
- van Mens-Verhulst, J.; Radtke, L. Intersectionality and Mental Health: A Case Study. Available online: www.vanmens.info/verhulst/en/wp-content/INTERSECTIONALITY%20AND%20MENTAL%20HEALTH2.pdf (accessed on 9 July 2019).
- Coburn, D.; Denny, K.; Mykhalovskiy, E.; McDonough, P.; Robertson, A.; Love, R. Population health in Canada: A brief critique. Am. J. Public Health 2003, 93, 392–396. [Google Scholar] [CrossRef]
- Hankivsky, O.; Christoffersen, A. Intersectionality and the determinants of health: A Canadian perspective. Crit. Public Health 2008, 18, 271–283. [Google Scholar] [CrossRef]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revision; World Health Organization: Geneva, Switzerland, 2016. Available online: www.who.int/classifications/icd/ICD10Volume2_en_2010.pdf (accessed on 9 July 2019).
- Australian Bureau of Statistics. Australian Statistical Geography Standard (ASGS): Volume 5—Remoteness Structure, July 2016; cat. no. 1270.0.55.005; Australian Bureau of Statistics: Canberra, Australia, 2018.
- Pitman, A.L.; Osborn, D.P.J.; Rantell, K.; King, M.B. Bereavement by suicide as a risk factor for suicide attempt: A cross-sectional national UK-wide study of 3432 young bereaved adults. BMJ Open 2015, 6, e009948. [Google Scholar] [CrossRef]
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; John Wiley & Sons: New York, NY, USA, 1987. [Google Scholar]
- Knol, M.J.; VanderWeele, T.J. Recommendations for presenting analyses of effect modification and interaction. Int. J. Epidemiol. 2012, 41, 514–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burns, R.A. Sex and age trends in Australia’s suicide rate over the last decade: Something is still seriously wrong with men in middle and late life. Psychiat. Res. 2016, 245, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Logan, J.; Hall, J.; Karch, D. Suicide categories by patterns of known risk factors: A latent class analysis. Arch. Gen. Psychiat. 2011, 68, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Sinyor, M.; Tan, L.P.L.; Schaffer, A.; Gallagher, D.; Shulman, K. Suicide in the oldest old: An observational study and cluster analysis. Int. J. Geriatr. Psych. 2016, 31, 33–40. [Google Scholar] [CrossRef] [PubMed]
- McCall, L. The complexity of intersectionality. Signs 2005, 30, 1771–1800. [Google Scholar] [CrossRef]
- Hunting, G. Intersectionality-Informed Qualitative Research: A Primer; The Institute for Intersectionality Research & Policy, The Institute for Intersectionality Research & Policy, Simon Fraser University: Vancouver, Canada, 2014; Available online: https://www.ifsee.ulaval.ca/sites/ifsee.ulaval.ca/files/b95277db179219c5ee8080a99b0b91276941.pdf (accessed on 9 July 2019).
- Rodriguez, J.K. Intersectionality and Qualitative Research. In The SAGE Handbook of Qualitative Business and Management Research Methods: History and Traditions; Cassell, C., Cunliffe, A.L., Grandy, G., Eds.; Sage: London, UK, 2018; pp. 429–461. [Google Scholar]
- National Mental Health Commission. The Fifth National Mental Health and Suicide Prevention Plan; Australian Government: Canberra, Australia, 2017. Available online: http://www.coaghealthcouncil.gov.au/Portals/0/Fifth%20National%20Mental%20Health%20and%20Suicide%20Prevention%20Plan.pdf (accessed on 9 July 2019).
- National Mental Health Commission. The 2017 National Report on Mental Health and Suicide Prevention; Australian Government: Canberra, Australia, 2017. Available online: www.mentalhealthcommission.gov.au/media/202298/NMHC17-3367_National_Report_ACC2.pdf (accessed on 9 July 2019).
- Senate Community Affairs Committee Secretariat. Accessibility and Quality of Mental Health Services in Australia; Commonwealth Government of Australia: Canberra, Australia, 2018. Available online: www.aph.gov.au/Parliamentary_Business/Committees/Senate/Community_Affairs/MentalHealthServices/Report (accessed on 9 July 2019).
- Queensland Mental Health Commission. Queensland Suicide Prevention Action Plan 2015–2017; Queensland Mental Health Commission: Brisbane, Australia, 2015. Available online: www.qmhc.qld.gov.au/sites/default/files/wp-content/uploads/2015/09/Queensland-Suicide-Prevention-Action-Plan-2015-17_WEB.pdf (accessed on 9 July 2019).
- South Australian Health. South Australian Suicide Prevention Plan 2017–2021; Government of South Australia: Adelaide, Australia, 2017. Available online: www.sahealth.sa.gov.au/wps/wcm/connect/89cf2e8040a76656898cfb2559774525/South+Australian+Suicide+Prevention+Plan_June+2018_Final.pdf?MOD=AJPERES&CACHEID=ROOTWORKSPACE-89cf2e8040a76656898cfb2559774525-mHWj1VX (accessed on 9 July 2019).
- Department of Health and Human Services. Tasmanian Suicide Prevention Strategy (2016–2020); Tasmanian Government: Hobart, Australia, 2016. Available online: www.dhhs.tas.gov.au/__data/assets/pdf_file/0014/214412/151152_DHHS_Suicide_Prevention_Strategy_Final_WCAG.pdf (accessed on 9 July 2019).
- Fitzpatrick, S.J.; Hooker, C.; Kerridge, I. Suicidology as a social practice. Soc. Epistemol. 2015, 29, 303–322. [Google Scholar] [CrossRef]
- Gruskin, S.; Daniels, N. Justice and human rights: Priority setting and fair deliberative process. Am. J. Public Health 2008, 98, 1573–1577. [Google Scholar] [CrossRef] [PubMed]
- Elliott-Farrelly, T. Australian Aboriginal suicide: The need for an Aboriginal suicidology. Adv. Ment. Health 2004, 3, 138–145. [Google Scholar] [CrossRef]
- Tatz, C. Aboriginal Suicide is Different, 2nd ed.; Aboriginal Studies Press: Canberra, Australia, 2005. [Google Scholar]
- Yuval-Davis, N. Intersectionality and feminist politics. Eur. J. Womens Stud. 2006, 13, 193–209. [Google Scholar] [CrossRef]
- Malatzky, C.; Bourke, L. Re-producing rural health: Challenging dominant discourses and the manifestation of power. J. Rural Stud. 2016, 45, 157–164. [Google Scholar] [CrossRef]
- Judd, F.; Cooper, A.-M.; Fraser, C.; Davis, J. Rural suicide—people or place effects? Aust. N. Z. J. Psychiat. 2006, 40, 208–216. [Google Scholar] [CrossRef]
- Qi, X.; Hu, W.; Page, A.; Tong, S. Spatial clusters of suicide in Australia. BMC Psychiatry 2012, 12. [Google Scholar] [CrossRef] [PubMed]
- Torok, M.; Konings, P.; Batterham, P.J.; Christensen, H. Spatial clustering of fatal, and non-fatal, suicide in new South Wales, Australia: Implications for evidence-based prevention. BMC Psychiatry 2017, 17, 339. [Google Scholar] [CrossRef] [PubMed]
- Mills, C. Decolonizing Global Mental Health; Routledge: New York, NY, USA, 2014. [Google Scholar]
- Stuckler, D.; Basu, S. The Body Economic: Why Austerity Kills; Basic Books: New York, NY, USA, 2013. [Google Scholar]
- Gavin, M.; Rogers, A. Narratives of suicide in psychological autopsy: Bringing lay knowledge back in. J. Ment. Health 2006, 15, 135–144. [Google Scholar] [CrossRef]
- Horwitz, A.V. Creating Mental Illness; The University of Chicago Press: Chicago, IL, USA, 2002. [Google Scholar]
- Bauer, G.R. Incorporating intersectionality theory into population health research methodology: Challenges and the potential to advance health equity. Soc. Sci. Med. 2014, 110, 10–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baum, F.E.; Laris, P.; Fisher, M.; Newman, L.; MacDougall, C. “Never mind the logic, give me the numbers”: Former Australian health ministers’ perspectives on the social determinants of health. Soc. Sci. Med. 2013, 87, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Baker, P.; Friel, S.; Kay, A.; Baum, F.; Strazdins, L.; Mackean, T. What enables and constrains the inclusion of the social determinants of health inequities in government policy agendas? A narrative review. Int J Health Policy Manag. 2018, 7, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Embrett, M.G.; Randall, G.E. Social determinants of health and health equity policy research: Exploring the use, misuse, and nonuse of policy analysis theory. Soc. Sci. Med. 2014, 108, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.P. Political determinants of health. Eur. J. Public Health 2014, 24, 2. [Google Scholar] [CrossRef]
- Raphael, D.; Curry-Stevens, A.; Bryant, T. Barriers to addressing the social determinants of health: Insights from the Canadian experience. Health Policy 2008, 88, 222–235. [Google Scholar] [CrossRef]
- Exworthy, M. Policy to tackle the social determinants of health: Using conceptual models to understand the policy process. Health Policy Plann. 2008, 23, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Carey, G.; Crammond, B. Taking Action on the Social Determinants of Health: Insights from Politicians, Policymakers and Lobbyists; Social Determinants of Health Alliance, The Australian National University and Monash University: Canberra, Australia, 2014; Available online: www.sdoha.org.au/140714Taking%20Action.pdf (accessed on 9 July 2019).
- Carey, G.; Crammond, B. Action on the social determinants of health: Views from inside the policy process. Soc. Sci. Med. 2015, 128, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Carey, G. Re-conceptualising public health interventions in government: A response to recent commentaries. Int. J. Health Policy Manag. 2016, 5, 569–570. [Google Scholar] [CrossRef] [PubMed]
- Goldney, R.D. Qualitative and quantitative approaches in suicidology: Commentary. Arch. Suicide Res. 2002, 6, 69–73. [Google Scholar] [CrossRef]
- Kral, M.J.; Links, P.S.; Bergmans, Y. Suicide studies and the need for mixed methods research. J. Mix. Methods Res. 2012, 6, 236–249. [Google Scholar] [CrossRef]
- Tait, G.; Carpenter, B.J.; De Leo, D.; Tatz, C. Problems with the coronial determination of ‘suicide’. Mortality 2015, 20, 233–247. [Google Scholar] [CrossRef]
- Graham, J.W. Missing data analysis: Making it work in the real world. Annu. Rev. Psychol. 2009, 60, 549–576. [Google Scholar] [CrossRef]
- Spratt, M.; Carpenter, J.; Sterne, J.A.C.; Carlin, J.B.; Heron, J.; Henderson, J.; Tilling, K. Strategies for multiple imputation in longitudinal studies. Am. J. Epidemiol. 2010, 172, 478–487. [Google Scholar] [CrossRef]
- Mallon, S.; Galway, K.; Hughes, L.; Rondón-Sulbaran, J.; Leavey, G. An exploration of integrated data on the dynamics of suicide among women. Sociol Health Illn. 2016, 38, 662–675. [Google Scholar] [CrossRef]
- Fincham, B.; Langer, S.; Scourfield, J.; Shiner, M. Understanding Suicide: A Social Autopsy; Palgrave Macmillan: London, UK, 2011. [Google Scholar]
- Rogers, J.R.; Lester, D. Understanding Suicide: Why We Don’t and How We Might; Hogrefe: Cambridge, MA, USA, 2010. [Google Scholar]

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fitzpatrick, S.J.; Brew, B.K.; Read, D.M.Y.; Inder, K.J.; Hayes, A.; Perkins, D. Rethinking Suicide in Rural Australia: A study Protocol for Examining and Applying Knowledge of the Social Determinants to Improve Prevention in Non-Indigenous Populations. Int. J. Environ. Res. Public Health 2019, 16, 2944. https://doi.org/10.3390/ijerph16162944
Fitzpatrick SJ, Brew BK, Read DMY, Inder KJ, Hayes A, Perkins D. Rethinking Suicide in Rural Australia: A study Protocol for Examining and Applying Knowledge of the Social Determinants to Improve Prevention in Non-Indigenous Populations. International Journal of Environmental Research and Public Health. 2019; 16(16):2944. https://doi.org/10.3390/ijerph16162944
Chicago/Turabian StyleFitzpatrick, Scott J., Bronwyn K. Brew, Donna M. Y. Read, Kerry J. Inder, Alan Hayes, and David Perkins. 2019. "Rethinking Suicide in Rural Australia: A study Protocol for Examining and Applying Knowledge of the Social Determinants to Improve Prevention in Non-Indigenous Populations" International Journal of Environmental Research and Public Health 16, no. 16: 2944. https://doi.org/10.3390/ijerph16162944