Healthy for Life Pilot Study: A Multicomponent School and Home Based Physical Activity Intervention for Disadvantaged Children



Abstract
1. Introduction
2. Materials and Methods
2.1. Intervention Design
- 10 × one-hour school-based training sessions consisting of 15–20 min of classroom training, linked to the National Health and Wellbeing curriculum [36] and 40–45 min of physical activities to support the training were delivered by a teacher and physiotherapist. The physical activities were, wherever possible, fruit and vegetable themed to complement the SAKG program [35]. The school-based sessions are outlined in more detail in Table 1.
- a ‘passport to fun’ home-based activity booklet to encourage children’s daily participation in PA through ‘fun’ with their parents, guardians, siblings and friends over the 10-week intervention. The activities were designed to meet the needs of both small and large families and for parents and guardians who may have varying levels of physical ability and fitness. Activities consisted of a range of indoor and outdoor activities, and activities with and without equipment.
- 4 × one-hour parent workshops, to support the SAKG program and promote awareness of a healthy diet and the importance of exercise, were delivered by a trained nutritionist and educator. All sessions were based on the Australian Guide to Healthy Eating (AGHE) and the Australian PA guidelines for all Australians (12). Instructions were given on: how to read a food label to identify hidden fats, sugar and salt; food groups and serving sizes; and nutrition and PA for disease prevention. Parents from the intervention school were invited through the school newsletter, Parents and Friends Association and individual flyers to attend 4 × 1 h workshops on the benefits of a healthy diet and PA. Attending parents were provided with a demonstration of how to cook a healthy main course and dessert for their household. They were provided with enough food to prepare the meal for all those eating within the family home, with instruction and food free of charge. They were invited to provide feedback on the workshops and complete the Australian Nutrition Knowledge Questionnaire (GNKQ) before and after training (13) and a short questionnaire on PA.
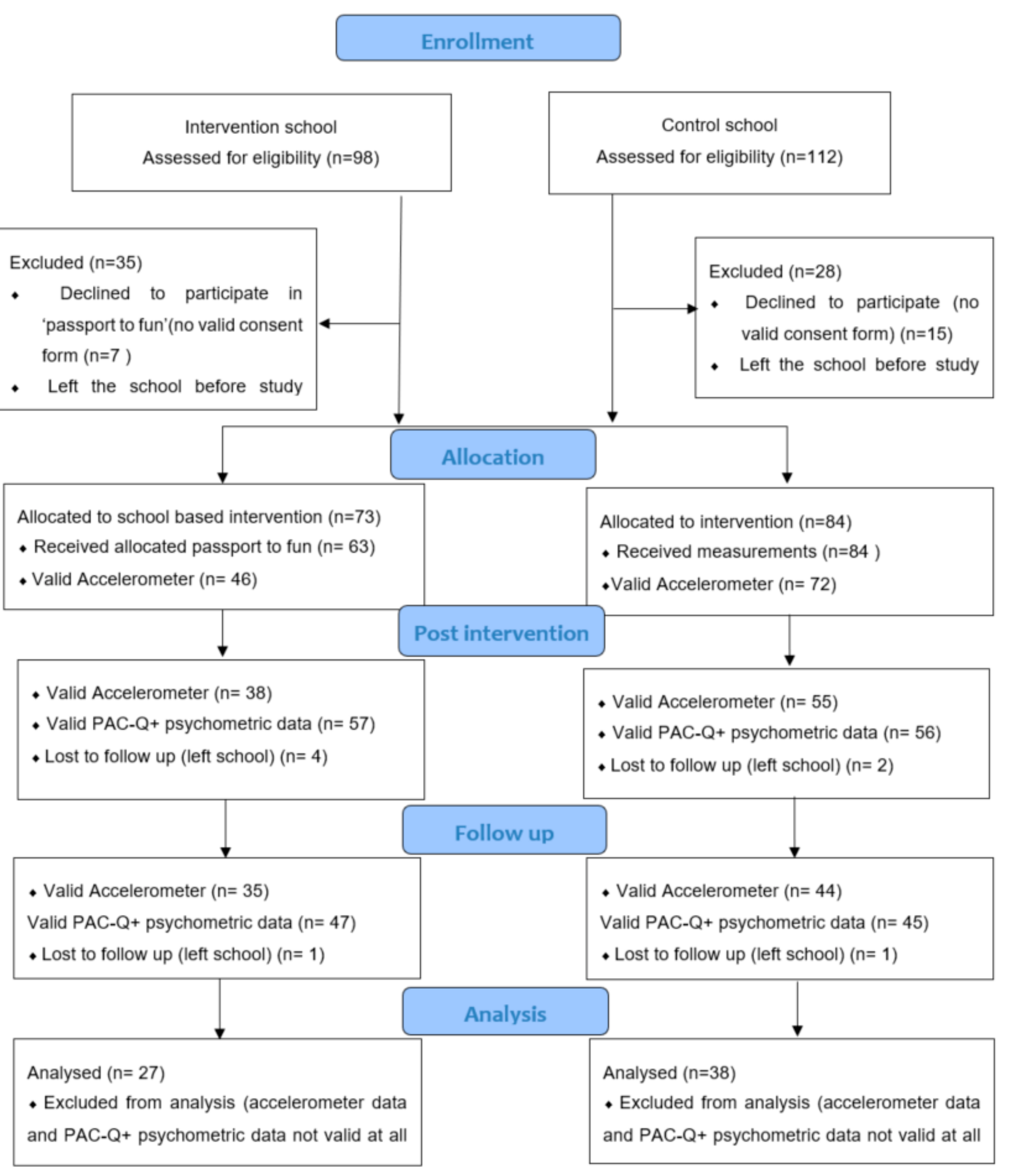
2.2. Participants
2.3. Study Design
2.4. Measures
2.4.1. Psychosocial Variables
2.4.2. Physical Activity
Self-Reported Physical Activity
2.4.3. Device-Measured Physical Activity
2.4.4. Assessment of Parent Information Sessions.
Nutrition Knowledge
Assessment of PA Knowledge
2.4.5. Program Feedback
Focus Groups with the Children
Focus Groups with the Parent
Interviews with the Teachers
2.5. Statistical Analysis
3. Results
3.1. Participants
3.2. Physical Activity Levels Achieved through Active Play
3.3. Relationships with Device Measured PA and Self-Reported PA
3.4. Psychological Variables which Influence PA
3.4.1. Psychological Variables which Influence Device Measured PA
3.4.2. Psychological Variables which Influence Self-Report PA
3.5. Feedback from all Stakeholders; The Children, Parents and Teachers
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

References
- World Health Organisation. Global Recommendations on Physical Activity for Health. 2018. Available online: https://www.who.int/dietphysicalactivity/publications/9789241599979/en/ (accessed on 4 April 2019).
- The Global Matrix on Physical Activity for Children and Youth. The Active Healthy Kids Global Alliance Is a Network. 2018. Available online: https://www.activehealthykids.org/global-matrix/ (accessed on 15 June 2019).
- Muscular Fitness: It’s Time for a Jump Start. The 2018 Active Healthy Kids Australia Report Card on Physical Activity for Children and Young People. Adelaide, South Australia. 2018. Available online: http://dx.doi.org/10.25954/5b862301479a1 (accessed on 1 June 2019).
- Smith, M.; Ikeda, E.; Hinckson, E.; Duncan, S.; Maddison, R.; Meredith-Jones, K.; Walker, C.; Mandic, S. Results from New Zealand’s 2018 Report Card on Physical Activity for Children and Youth. J. Phys. Act. Health 2018, 15, S390–S392. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [PubMed]
- Telama, R.; Yang, X.; Leskinen, E.; Kankaanpää, A.; Hirvensalo, M.; Tammelin, T.; Viikari, J.S.A.; Raitakari, O.T. Tracking of Physical Activity from Early Childhood through Youth into Adulthood. Med. Sci. Sports Exerc. 2014, 46, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Chung, A.; Backholer, K.; Wong, E.; Palermo, C.; Keating, C.; Peeters, A. Trends in child and adolescent obesity prevalence in economically advanced countries according to socioeconomic position: A systematic review. Obes. Rev. 2016, 17, 276–295. [Google Scholar] [CrossRef] [PubMed]
- Law, C.; Power, C.; Graham, H.; Merrick, D. Obesity and health inequalities. Obes. Rev. 2007, 8, 19–22. [Google Scholar]
- 2011–Australian Bureau of Statistics (ABS). Australian Health Survey: Physical Activity, Catalogue No. 4364.0. Australian Bureau of Statistics: Canberra. 2013. Available online: https://www.abs.gov.au/australianhealthsurvey (accessed on 15 June 2019).
- Humbert, M.L.; Chad, K.E.; Spink, K.S.; Muhajarine, N.; Anderson, K.D.; Bruner, M.W.; Girolami, T.M.; Odnokon, P.; Gryba, C.R. Factors That Influence Physical Activity Participation Among High- and Low-SES Youth. Qual. Health Res. 2006, 16, 467–483. [Google Scholar] [CrossRef] [PubMed]
- Craike, M.; Wiesner, G.; Hilland, T.A.; Bengoechea, E.G. Interventions to improve physical activity among socioeconomically disadvantaged groups: An umbrella review. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 43. [Google Scholar] [CrossRef]
- Hills, A.P.; Dengel, D.R.; Lubans, D.R. Supporting Public Health Priorities: Recommendations for Physical Education and Physical Activity Promotion in Schools. Prog. Cardiovasc. Dis. 2015, 57, 368–374. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. Healthy People 2010: Understanding and Improving Health. 2000. Available online: http://www.eric.ed.gov/PDFS/ED443794.pdf (assessed on 15 June 2019).
- Salmon, J.; Timperio, A.; Cleland, V.; Venn, A. Trends in children’s physical activity and weight status in high and low socio-economic status areas of Melbourne, Victoria, 1985–2001. Aust. N. Z. J. Public Health 2005, 29, 337–342. [Google Scholar] [CrossRef]
- Kriemler, S.; Meyer, U.; Martin, E.; Van Sluijs, E.M.F.; Andersen, L.B.; Martin, B.W. Effect of school-based interventions on physical activity and fitness in children and adolescents: A review of reviews and systematic update. Br. J. Sports Med. 2011, 45, 923–930. [Google Scholar] [CrossRef]
- Lonsdale, C.; Rosenkranz, R.R.; Peralta, L.R.; Bennie, A.; Fahey, P.; Lubans, D.R. A systematic review and meta-analysis of interventions designed to increase moderate-to-vigorous physical activity in school physical education lessons. Prev. Med. 2013, 56, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Verstraete, S.J.; Cardon, G.M.; De Clercq, D.L.R.; De Bourdeaudhuij, I.M.M. Increasing children’s physical activity levels during recess periods in elementary schools: The effects of providing game equipment. Eur. J. Public Health 2006, 16, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Van Sluijs, E.M.F.; McMinn, A.M.; Griffin, S.J. Effectiveness of interventions to promote physical activity in children and adolescents: Systematic review of controlled trials. BMJ 2007, 335, 703. [Google Scholar] [CrossRef] [PubMed]
- Stanley, R.M.; Ridley, K.; Olds, T.S.; Dollman, J. Development and psychometric properties of the Y-PASS questionnaire to assess correlates of lunchtime and after-school physical activity in children. BMC Public Health 2014, 14, 412. [Google Scholar] [CrossRef] [PubMed]
- Atkin, A.J.; Gorely, T.; Biddle, S.J.H.; Cavill, N.; Foster, C. Interventions to promote physical activity in young people conducted in the hours immediately after school: A systematic review. Int. J. Behav. Med. 2011, 18, 176–187. [Google Scholar] [CrossRef]
- Demetriou, Y.; Gillison, F.; McKenzie, T.L. After-School Physical Activity Interventions on Child and Adolescent Physical Activity and Health: A Review of Reviews. Adv. Phys. Educ. 2017, 7, 191–215. [Google Scholar] [CrossRef]
- Singletary, C.R.; Weaver, G.; Carson, R.L.; Beets, M.W.; Pate, R.R.; Saunders, R.P.; Peluso, A.G.; Moore, J.B. Evaluation of a comprehensive school physical activity program: Be a Champion! Eval. Program Plan. 2019, 75, 54–60. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Comprehensive School Physical Activity Programs: A Guide for Schools. 2013. Available online: https://www.cdc.gov/healthyschools/professional_development/e-learning/cspap.html (accessed on 12 June 2019).
- Veugelers, P.J.; Schwartz, M.E. Comprehensive school health in Canada. Can. J. Public Health 2010, 101, S5–S8. [Google Scholar]
- Tannehill, D.; Van der Mars, H.; McPhail, A. Comprehensive school physical activity programs. In Building Effective Physical Education Programs; Tannehill, D., Van der Mars, H., McPhail, A., Eds.; Jones and Bartlett Learning: Burlington, MA, USA, 2014; pp. 27–54. [Google Scholar]
- Dai, C. School Health Program: Impacting Physical Activity Behaviors among Disadvantaged Students. J. Sch. Health 2019, 89, 468–475. [Google Scholar] [CrossRef]
- Martin, J.J.; McCaughtry, N.; Flory, S.; Murphy, A.; Wisdom, K. Using Social Cognitive Theory to Predict Physical Activity and Fitness in Underserved Middle School Children. Res. Q. Exerc. Sport 2011, 82, 247–255. [Google Scholar] [CrossRef]
- Martin, J.J.; McCaughtry, N. Using social cognitive theory to predict physical activity in inner-city African American school children. J. Sport Exerc. Psychol. 2008, 30, 378–391. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.J.; McCaughtry, N. Predicting Physical Activity in Inner-City Hispanic American Children. Hisp. Health Care Int. 2008, 6, 150–158. [Google Scholar] [CrossRef]
- Beets, M.W.; Pitetti, K.H.; Forlaw, L. The Role of Self-efficacy and Referent Specific Social Support in Promoting Rural Adolescent Girls’ Physical Activity. Am. J. Health Behav. 2007, 31, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.Y.; Pender, N. Determinants of physical activity among Taiwanese adolescents: An application of the health promotion model. Res. Nurs. Health 2002, 25, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Duncan, S.C.; Duncan, T.E.; Strycker, L.A. Sources and Types of Social Support in Youth Physical Activity. Health Psychol. 2005, 24, 3–10. [Google Scholar] [CrossRef]
- Ashford, S.; Edmunds, J.; French, D.P.; Williams, S. What is the best way to change self-efficacy to promote lifestyle and recreational physical activity? A systematic review with meta-analysis. Br. J. Health Psychol. 2010, 15, 265–288. [Google Scholar] [CrossRef] [PubMed]
- Plotnikoff, R.C.; Costigan, S.A.; Karunamuni, N.; Lubans, D.R. Social cognitive theories used to explain physical activity behavior in adolescents: A systematic review and meta-analysis. Prev. Med. 2013, 56, 245–253. [Google Scholar] [CrossRef]
- Stephanie Alexander Kitchen Garden Program 2017. Available online: https://www.kitchengardenfoundation.org.au/ (accessed on 30 April 2019).
- Australian Health and Physical Activty National Curriculum. 2014. Available online: https://www.australiancurriculum.edu.au/resources/curriculum-connections/dimensions/?Id=46754&YearLevels=42683#dimension-content (accessed on 8 December 2017).
- Motl, R.W.; Dishman, R.K.; Saunders, R.; Dowda, M.; Felton, G.; Pate, R.R. Measuring enjoyment of physical activity in adolescent girls. Am. J. Prev. Med. 2001, 21, 110–117. [Google Scholar] [CrossRef]
- Dishman, R.; Motl, R.; Saunders, R.; Dowda, M.; Felton, G.; Ward, D.S.; Pate, R. Factorial Invariance and Latent Mean Structure of Questionnaires Measuring Social-Cognitive Determinants of Physical Activity among Black and White Adolescent Girls. Prev. Med. 2002, 34, 100–108. [Google Scholar] [CrossRef]
- Dishman, R.K.; Motl, R.W.; Saunders, R.; Felton, G.; Ward, D.S.; Dowda, M.; Pate, R.R. Enjoyment Mediates Effects of a School-Based Physical-Activity Intervention. Med. Sci. Sports Exerc. 2005, 37, 478–487. [Google Scholar] [CrossRef]
- Saelens, B.E.; Gehrman, C.A.; Sallis, J.F.; Calfas, K.J.; Sarkin, J.A.; Caparosa, S. Use of self-management strategies in a 2-year cognitive-behavioral intervention to promote physical activity. Behav. Ther. 2000, 31, 365–379. [Google Scholar] [CrossRef]
- Sallis, J.F.; Taylor, W.C.; Dowda, M.; Freedson, P.S.; Pate, R.R. Correlates of Vigorous Physical Activity for Children in Grades 1 through 12: Comparing Parent-Reported and Objectively Measured Physical Activity. Pediatr. Exerc. Sci. 2002, 14, 30–44. [Google Scholar] [CrossRef]
- Crocker, P.R.E.; Bailey, D.A.; Faulkner, R.A.; Kowalski, K.C.; McGrath, R. Measuring general levels of physical activity: Preliminary evidence for the Physical Activity Questionnaire for Older Children. Med. Sci. Sports Exerc. 1997, 29, 1344–1349. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Loprinzi, P.D.; Moore, R.; Pfeiffer, K.A. Comparison of Accelerometer Cut Points for Predicting Activity Intensity in Youth. Med. Sci. Sports Exerc. 2011, 43, 1360–1368. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.D.; Timperio, A.; Crawford, D.; Salmon, J. What Factors Are Associated with Adolescents’ School Break Time Physical Activity and Sedentary Time? PLoS ONE 2013, 8, e56838. [Google Scholar] [CrossRef] [PubMed]
- Hendrie, G.A.; Cox, D.N.; Coveney, J. Validation of the General Nutrition Knowledge Questionnaire in an Australian community sample. Nutr. Diet. 2008, 65, 72–77. [Google Scholar] [CrossRef]
- Parmenter, K.; Wardle, J. Development of a general nutrition knowledge questionnaire for adults. Eur. J. Clin. Nutr. 1999, 53, 298–308. [Google Scholar] [CrossRef]
- Dishman, R.K.; Hales, D.P.; Sallis, J.F.; Saunders, R.P.; Dunn, A.L.; Bedimo-Rung, A.L.; Ring, K.B. Validity of Social-Cognitive Measures for Physical Activity in Middle-School Girls. J. Pediatr. Psychol. 2010, 35, 72–88. [Google Scholar] [CrossRef]
- Rich, C.; Geraci, M.; Griffiths, L.; Sera, F.; Dezateux, C.; Cortina-Borja, M. Quality Control Methods in Accelerometer Data Processing: Defining Minimum Wear Time. PLoS ONE 2013, 8, e67206. [Google Scholar] [CrossRef]
- Barreira, T.V.; Schuna, J.M.; Tudor-Locke, C.; Chaput, J.-P.; Church, T.S.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; et al. Reliability of accelerometer-determined physical activity and sedentary behavior in school-aged children: A 12-country study. Int. J. Obes. Suppl. 2015, 5, S29–S35. [Google Scholar] [CrossRef]
- Cohen, K.E.; Morgan, P.J.; Plotnikoff, R.C.; Callister, R.; Lubans, D.R. Fundamental movement skills and physical activity among children living in low-income communities: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 49. [Google Scholar] [CrossRef] [PubMed]
- Hume, C.; Salmon, J.; Veitch, J.; Crawford, D.; Ball, K. Children Who Meet Recommendations for Physical Activity and Screen-Time Despite Socioeconomic Disadvantage. 2010. Available online: https://www.deakin.edu.au/__data/assets/pdf_file/0004/306976/summary-3.pdf (accessed on 15 June 2019).
- Stanley, R.M.; Maher, C.; Dollman, J. Modelling the contribution of walking between home and school to daily physical activity in primary age children. BMC Public Health 2015, 15, 445. [Google Scholar] [CrossRef] [PubMed]
- Dishman, R.K.; Motl, R.W.; Sallis, J.F.; Dunn, A.L.; Birnbaum, A.S.; Welk, G.J.; Bedimo-Rung, A.L.; Voorhees, C.C.; Jobe, J.B. Self-Management Strategies Mediate Self-Efficacy and Physical Activity. Am. J. Prev. Med. 2005, 29, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Prochaska, J.J.; Taylor, W.C. A review of correlates of physical activity of children and adolescents. Med. Sci. Sports Exerc. 2000, 32, 963–975. [Google Scholar] [CrossRef] [PubMed]
- Dishman, R.K.; Dunn, A.L.; Sallis, J.F.; Vandenberg, R.J.; Pratt, C.A. Social-Cognitive Correlates of Physical Activity in a Multi-Ethnic Cohort of Middle-School Girls: Two-year Prospective Study. J. Pediatr. Psychol. 2009, 35, 188–198. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Week | Classroom Instruction | Outdoor Instruction | |
|---|---|---|---|
| Session Outcomes/Curriculum Link | Elaborations | ||
| 1 | Identify and practice strategies to promote health, safety and wellbeing (ACPPS036) | What is physical activity? How much physical activity do you need in a day? | Team based games: rob the fruit bowl, run the gauntlet, rotten apples |
| 2 | Identify how to set a goal. Strategies for goal setting | Define goal setting and use SMART (s-specific, m-measurable, a-achievable, r-realistic, t-timely) goal format. Set goals for ‘passport to fun’. | Vegetable Olympics: carrot relay, vegetable tunnel ball, egg and spoon relay |
| 3 | Barriers and enablers to physical activity at home | Identify barriers and brainstorm enablers | Team building; build a scarecrow. |
| 4 | Barriers and enablers to physical activity at home | Identify barriers and brainstorm enablers | Gym stations: rope, mat, ball and cone activities |
| 5 | Examine the benefits of physical activity and physical fitness to health and wellbeing, (ACPMP046) | Benefits of physical activity and physical fitness to health and wellbeing to include the influence on sleep, concentration and fitness | Dance routines |
| 6 | Identify and practice strategies to promote health, safety and wellbeing (ACPPSO36) | Introduction to pedometers | Pedometer—‘treasure’ map around the edible kitchen garden located around the perimeter of the school. |
| 7 | Cultural considerations to physical activity, (ACPPS042) | Discussion on cultural diversity within the class and link to diversity in traditional sports around the world and in Australia. | Active vegetable and fruit memory games |
| 8 | The importance of Friendships and engaging friends in physical activity, (ACPMP048) | Discussion on the importance of friendships and enablers to building friendships | Capture the carrot tag game |
| 9 | Liquids while exercising | Discussion on water vs. sports drinks, energy drinks, cordial, fruit juice | Fruit salad soccer game |
| 10 | Reassess goals | Refer to ‘passport to fun’ and level of participation | Healthy ‘food plate’ relay |
| Participants | Intervention School n = 63 | Control School n = 84 | All n = 147 | p Values | ||
|---|---|---|---|---|---|---|
| % Cohort | % Responders | % Cohort | % Responders | % Responders | ||
| Female (%) | 64 | 64 | 55 | 55 | 59 | 0.294 |
| Class year (%) | 0.265 | |||||
| combined 3/4 | 27 | 27 | 23 | 23 | 25 | |
| combined 4/5 | 27 | 27 | 23 | 23 | 25 | |
| straight 6 + combined 5/6 | 26 | 26 | 26 | 26 | 27 | |
| straight 7 | 19 | 19 | 29 | 29 | 23 | |
| Ethnicity (%) | 0.755 | |||||
| Aboriginal | 13 | 19 | 3 | 11 | 7 | |
| European | 14 | 21 | 6 | 26 | 10 | |
| African | 10 | 14 | 1 | 0 | 4 | |
| Asian | 0 | 0 | 4 | 16 | 2 | |
| Other | 31 | 47 | 11 | 47 | 20 | |
| Highest parental education (%) | 0.755 | |||||
| High school (partial or completed) | 54 | 63 | 23 | 71 | 38 | |
| Some post-secondary | 29 | 33 | 8 | 23 | 17 | |
| Bachelor degree | 2 | 2 | 1 | 3 | 1 | |
| Postgraduate | 2 | 2 | 1 | 3 | 1 | |
| Parent marital status (%) | 0.082 | |||||
| married/partner | 41 | 48 | 25 | 68 | 53 | |
| single parent/guardian | 44 | 52 | 12 | 32 | 45 | |
| Parents working outside the home (%) | 0.032 | |||||
| none | 59 | 68 | 18 | 48 | 35 | |
| <15 h/wk | 13 | 15 | 2 | 7 | 7 | |
| part time (15–35 h/wk | 5 | 6 | 11 | 29 | 8 | |
| full time (36+ h/wk) | 9 | 11 | 6 | 16 | 8 | |
| Household size (no. of people living in the house) mean (SD) | 5.3 (2.6) | 4.9 (1.5) | 5.2 (2.9) | 0.469 | ||
| Timeframe MVPA (min/day) | Data at Each Time Point | Complete Data for 3 Time Points | ||||
|---|---|---|---|---|---|---|
| Baseline | Post Intervention | Follow-Up | Baseline | Post Intervention | Follow-Up | |
| Intervention School (n) | 46 | 38 | 35 | 27 | 27 | 27 |
| Total day | 147 ± 44 | 138 ± 44 | 145 ± 42 | 146 ± 41 | 142 ± 8 | 143 ± 40 |
| School break time | 43 ± 6 | 41 ± 6 | 44 ± 5 | 43 ± 2 | 43 ± 2 | 42 ± 3 |
| After-school | 60 ± 6 | 58 ± 7 | 59 ± 6 | 59 ± 6 | 56 ± 7 | 59 ± 6 |
| Control school (n) | 72 | 55 | 44 | 38 | 38 | 38 |
| Total day | 131 ± 26 | 132 ± 33 | 131 ± 29 | 138 ± 36 | 132 ± 42 | 144 ± 40 |
| School break time | 42 ± 2 | 41 ± 4 | 43 ± 3 | 44 ± 3 | 43 ± 2 | 41 ± 3 |
| After-school | 56 ± 5 | 50 ± 6 | 51 ± 4 | 53 ± 5 | 49 ± 7 | 48 ± 6 |
| Intervention School | Data at Each Time Point | Complete Data for 3 Time Points | ||||
|---|---|---|---|---|---|---|
| Baseline | Post Intervention | Follow-Up | Baseline | Post Intervention | Follow-Up | |
| n | 63 | 57 | 47 | 27 | 27 | 27 |
| PAC-Q | 3.4 ± 0.8 | 3.4 ± 0.9 | 3.7 + 0.6 | 3.4 ± 0.8 | 3.6 + 0.6 | 3.7 ± 0.6 |
| self-management | 2.9 ± 0.7 | 2.8 ± 0.9 | 3.5 ± 0.6 | 3.2 + 0.8 | 3.0 + 0.9 | 3.5 + 0.6 |
| barriers | 2.0 ± 0.7 | 2.0 ± 0.7 | 2.8 ± 0.8 | 2.2 + 0.8 | 1.9 ± 0.5 | 2.8 ± 0.7 |
| outcome expectancy | 3.7 + 1.1 | 3.6 ± 1.1 | 2.5 ± 1.1 | 3.5 ± 1.2 | 3.9 ± 1.0 | 2.6 ± 1.3 |
| enjoyment | 3.2 ± 0.8 | 3.0 ± 0.7 | 3.5 ± 0.9 | 3.4 ± 0.9 | 3.1 ± 0.6 | 3.5 ± 1.0 |
| self-efficacy | 3.5 ± 0.9 | 3.5 ± 1.0 | 3.3 + 0.9 | 3.6 ± 0.9 | 3.7 ± 0.8 | 3.3 ± 0.9 |
| social support home | 3.0 ± 1.2 | 3.3 ± 1.0 | 3.6 + 1.0 | 3.1 ± 1.1 | 3.3 ± 1.1 | 3.5 ± 1.0 |
| school support | 3.0 ± 1.2 | 3.2 ± 1.1 | 3.3 ± 1.1 | 3.2 ± 1.1 | 3.3 + 1.1 | 3.3 + 1.1 |
| Control school | ||||||
| n | 72 | 56 | 45 | 38 | 38 | 38 |
| PAC-Q | a 3.2 ± 0.8 | 3.6 ± 0.6 | b 3.5 ± 0.6 | a 3.1 ± 0.7 | a 3.3 ± 0.6 | c 3.3 ± 0.9 |
| self-management | a 3.2 ± 0.8 | 3.0 ± 0.9 | b 3.5 ± 0.6 | c 2.4 ± 0.8 | a 2.4 ± 0.8 | c 3.1 ± 0.7 |
| barriers | 2.2 ± 0.8 | 1.9 ± 0.5 | a 2.8 ± 0.7 | 1.8 ± 0.6 | 1.8 ± 0.7 | 1.7 ± 0.7 |
| outcome expectancy | 3.5 ± 1.2 | 3.9 ± 1.0 | 2.6 ± 1.3 | 3.3 ± 1.0 | 3.3 ± 0.9 | a2.8 ± 1.6 |
| enjoyment | 3.4 ± 0.9 | 3.1 ± 0.6 | 3.5 + 1.0 | 2.9 ± 0.7 | 2.8 ± 0.6 | 3.5 + 0.9 |
| self-efficacy | 3.6 ± 0.9 | a 3.7 ± 0.8 | a 3.4 ± 0.9 | 3.3 ± 0.9 | c 3.0 ± 0.8 | a 2.8 ± 0.8 |
| social support home | a 3.1 ± 1.1 | a 3.3 ± 1.1 | b 3.5 + 1.0 | 2.6 + 0.7 | a 2.8 ± 0.9 | b 3.1 + 0.8 |
| school support | a 3.2 ± 1.1 | a 3.1 ± 1.0 | a 2.8 ± 1.1 | 2.6 ± 0.7 | 2.8 ± 0.9 | a 2.8 ± 0.9 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pearce, K.; Dollman, J. Healthy for Life Pilot Study: A Multicomponent School and Home Based Physical Activity Intervention for Disadvantaged Children. Int. J. Environ. Res. Public Health 2019, 16, 2935. https://doi.org/10.3390/ijerph16162935
Pearce K, Dollman J. Healthy for Life Pilot Study: A Multicomponent School and Home Based Physical Activity Intervention for Disadvantaged Children. International Journal of Environmental Research and Public Health. 2019; 16(16):2935. https://doi.org/10.3390/ijerph16162935
Chicago/Turabian StylePearce, Karma, and James Dollman. 2019. "Healthy for Life Pilot Study: A Multicomponent School and Home Based Physical Activity Intervention for Disadvantaged Children" International Journal of Environmental Research and Public Health 16, no. 16: 2935. https://doi.org/10.3390/ijerph16162935
APA StylePearce, K., & Dollman, J. (2019). Healthy for Life Pilot Study: A Multicomponent School and Home Based Physical Activity Intervention for Disadvantaged Children. International Journal of Environmental Research and Public Health, 16(16), 2935. https://doi.org/10.3390/ijerph16162935