Association between Resting Heart Rate and Colorectal Cancer: Results from a Case-Controlled Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Ethical Approval
2.3. Definition of CRC
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Non-PS-Matched and PS-Matched CRC Patient Cohorts
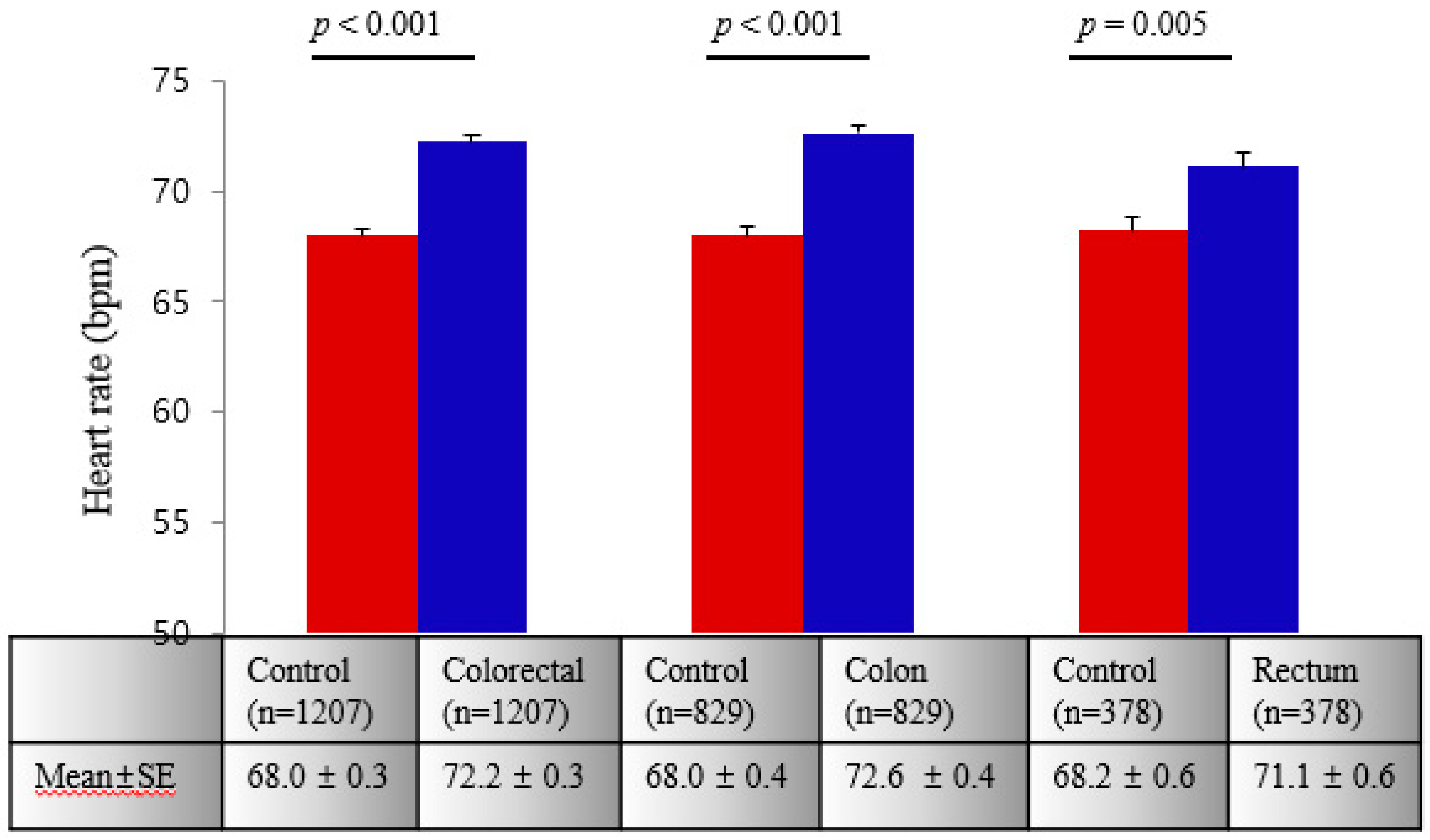
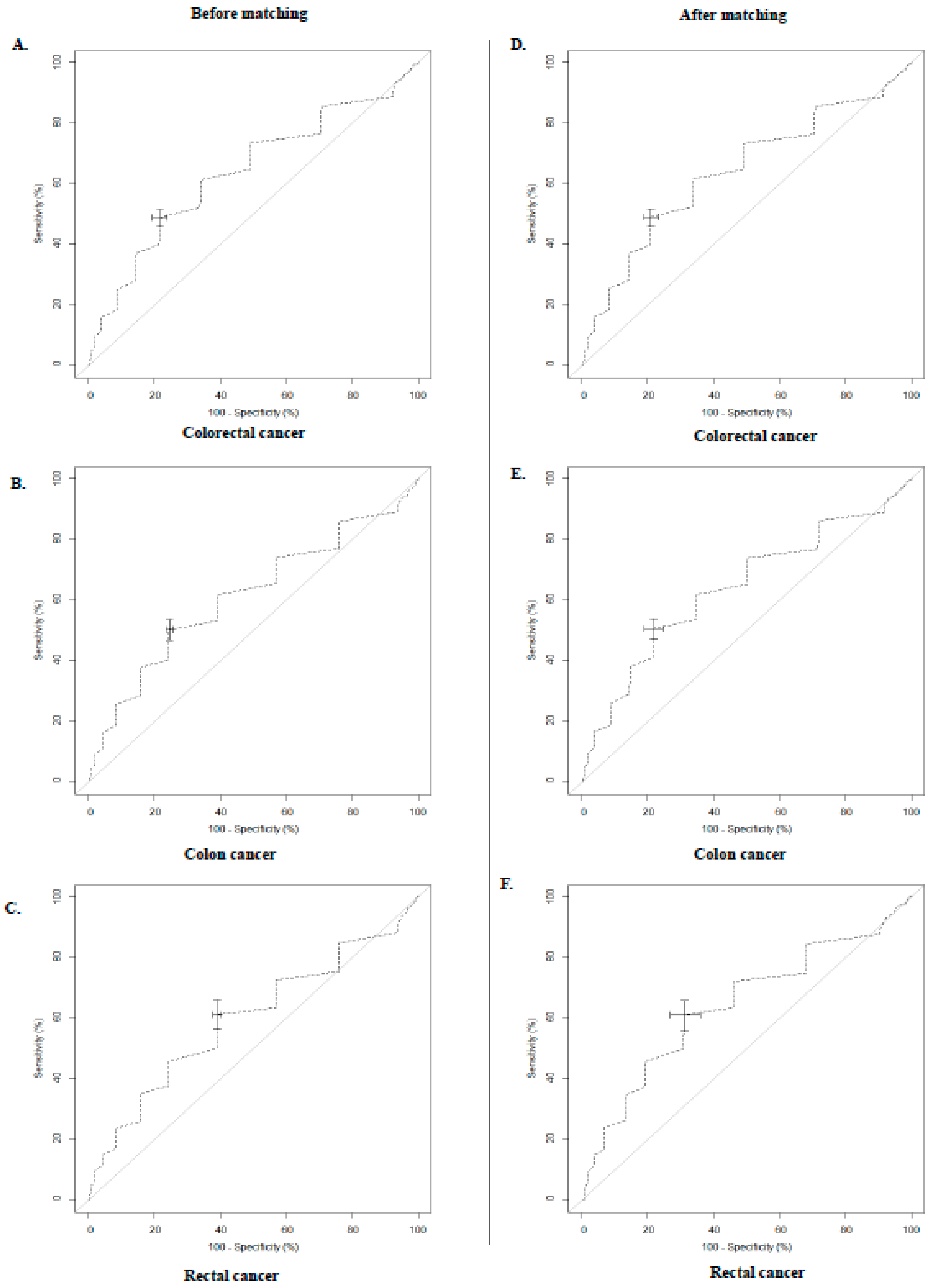
3.2. Associations between RHR and CRC
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Larsen, V.; Morton, V.; Norat, T.; Moreira, A.; Potts, J.F.; Reeves, T.; Bakolis, I. Dietary patterns derived from principal component analysis (PCA) and risk of colorectal cancer: A systematic review and meta-analysis. Eur. J. Clin. Nutr. 2019, 73, 366–386. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Lee, D.H.; Han, K.D.; Shin, C.M.; Kim, N. Abdominal obesity, glucose intolerance and decreased high-density lipoprotein cholesterol as components of the metabolic syndrome are associated with the development of colorectal cancer. Eur. J. Epidemiol. 2018, 33, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- Grassi, G.; Vailati, S.; Bertinieri, G.; Seravalle, G.; Stella, M.L.; Dell’Oro, R.; Mancia, G. Heart rate as marker of sympathetic activity. J. Hypertens. 1998, 16, 1635–1639. [Google Scholar] [CrossRef] [PubMed]
- Kovar, D.; Cannon, C.P.; Bentley, J.H.; Charlesworth, A.; Rogers, W.J. Does initial and delayed heart rate predict mortality in patients with acute coronary syndromes? Clin. Cardiol. 2004, 27, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Woodward, M.; Webster, R.; Murakami, Y.; Barzi, F.; Lam, T.H.; Fang, X.; Suh, I.; Batty, G.D.; Huxley, R.; Rodgers, A. The association between resting heart rate, cardiovascular disease and mortality: Evidence from 112,680 men and women in 12 cohorts. Eur. J. Prev. Cardiol. 2014, 21, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Bohm, M.; Swedberg, K.; Komajda, M.; Borer, J.S.; Ford, I.; Dubost-Brama, A.; Lerebours, G.; Tavazzi, L. Heart rate as a risk factor in chronic heart failure (shift): The association between heart rate and outcomes in a randomised placebo-controlled trial. Lancet 2010, 376, 886–894. [Google Scholar] [CrossRef]
- Ho, J.E.; Bittner, V.; Demicco, D.A.; Breazna, A.; Deedwania, P.C.; Waters, D.D. Usefulness of heart rate at rest as a predictor of mortality, hospitalization for heart failure, myocardial infarction, and stroke in patients with stable coronary heart disease (data from the treating to new targets [TNT] trial). Am. J. Cardiol. 2010, 105, 905–911. [Google Scholar] [CrossRef]
- Tverdal, A.; Hjellvik, V.; Selmer, R. Heart rate and mortality from cardiovascular causes: A 12 year follow-up study of 379,843 men and women aged 40-45 years. Eur. Heart J. 2008, 29, 2772–2781. [Google Scholar] [CrossRef]
- Palatini, P.; Julius, S. Association of tachycardia with morbidity and mortality: Pathophysiological considerations. J. Hum. Hypertens. 1997, 11 Suppl 1, S19–S27. [Google Scholar]
- Fox, K.; Borer, J.S.; Camm, A.J.; Danchin, N.; Ferrari, R.; Lopez Sendon, J.L.; Steg, P.G.; Tardif, J.C.; Tavazzi, L.; Tendera, M. Resting heart rate in cardiovascular disease. J. Am. Coll. Cardiol. 2007, 50, 823–830. [Google Scholar] [CrossRef] [PubMed]
- Palatini, P.; Julius, S. Elevated heart rate: A major risk factor for cardiovascular disease. Clin. Exp. Hypertens. 2004, 26, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Alhalabi, L.; Singleton, M.J.; Oseni, A.O.; Shah, A.J.; Zhang, Z.M.; Soliman, E.Z. Relation of higher resting heart rate to risk of cardiovascular versus noncardiovascular death. Am. J. Cardiol. 2017, 119, 1003–1007. [Google Scholar] [CrossRef]
- Greenland, P.; Daviglus, M.L.; Dyer, A.R.; Liu, K.; Huang, C.F.; Goldberger, J.J.; Stamler, J. Resting heart rate is a risk factor for cardiovascular and noncardiovascular mortality: The chicago heart association detection project in industry. Am. J. Epidemiol. 1999, 149, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Seviiri, M.; Lynch, B.M.; Hodge, A.M.; Yang, Y.; Liew, D.; English, D.R.; Giles, G.G.; Milne, R.L.; Dugue, P.A. Resting heart rate, temporal changes in resting heart rate, and overall and cause-specific mortality. Heart 2018, 104, 1076–1085. [Google Scholar] [CrossRef]
- Jouven, X.; Escolano, S.; Celermajer, D.; Empana, J.P.; Bingham, A.; Hermine, O.; Desnos, M.; Perier, M.C.; Marijon, E.; Ducimetiere, P. Heart rate and risk of cancer death in healthy men. PLoS ONE 2011, 6, e21310. [Google Scholar] [CrossRef]
- Cole, S.W.; Sood, A.K. Molecular pathways: Beta-adrenergic signaling in cancer. Clin. Cancer Res. 2012, 18, 1201–1206. [Google Scholar] [CrossRef]
- Masur, K.; Niggemann, B.; Zanker, K.S.; Entschladen, F. Norepinephrine-induced migration of SW 480 colon carcinoma cells is inhibited by β-blockers. Cancer Res. 2001, 61, 2866–2869. [Google Scholar]
- Guo, K.; Ma, Q.; Wang, L.; Hu, H.; Li, J.; Zhang, D.; Zhang, M. Norepinephrine-induced invasion by pancreatic cancer cells is inhibited by propranolol. Oncol. Rep. 2009, 22, 825–830. [Google Scholar]
- van Kruijsdijk, R.C.; van der Graaf, Y.; Bemelmans, R.H.; Nathoe, H.M.; Peeters, P.H.; Visseren, F.L. The relation between resting heart rate and cancer incidence, cancer mortality and all-cause mortality in patients with manifest vascular disease. Cancer Epidemiol. 2014, 38, 715–721. [Google Scholar] [CrossRef]
- Anker, M.S.; Ebner, N.; Hildebrandt, B.; Springer, J.; Sinn, M.; Riess, H.; Anker, S.D.; Landmesser, U.; Haverkamp, W.; von Haehling, S. Resting heart rate is an independent predictor of death in patients with colorectal, pancreatic, and non-small cell lung cancer: Results of a prospective cardiovascular long-term study. Eur. J. Heart Fail. 2016, 18, 1524–1534. [Google Scholar] [CrossRef] [PubMed]
- Jansen, L.; Weberpals, J.; Kuiper, J.G.; Vissers, P.A.J.; Wolkewitz, M.; Hoffmeister, M.; Brenner, H. Pre- and post-diagnostic beta-blocker use and prognosis after colorectal cancer: Results from a population-based study. Int. J. Cancer Res. 2017, 141, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Hicks, B.M.; Murray, L.J.; Powe, D.G.; Hughes, C.M.; Cardwell, C.R. Beta-blocker usage and colorectal cancer mortality: A nested case-control study in the UK clinical practice research datalink cohort. Ann. Oncol. 2013, 24, 3100–3106. [Google Scholar] [CrossRef] [PubMed]
- Jansen, L.; Hoffmeister, M.; Arndt, V.; Chang-Claude, J.; Brenner, H. Stage-specific associations between beta blocker use and prognosis after colorectal cancer. Cancer 2014, 120, 1178–1186. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, J.H.; Park, Y.; Park, S.J.; Cheon, J.H.; Kim, W.H.; Park, J.S.; Jeon, J.Y.; Kim, T.I. Resting heart rate is an independent predictor of advanced colorectal adenoma recurrence. PLoS ONE 2018, 13, e0193753. [Google Scholar] [CrossRef] [PubMed]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The korea national health and nutrition examination survey (knhanes). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef]
- Korea Centers for Disease Control and Prevention. The Korea National Health and Nutrition Examination Survey. Available online: https://knhanes.cdc.go.kr/knhanes/main.do (accessed on 5 April 2019).
- Hari, D.M.; Leung, A.M.; Lee, J.H.; Sim, M.S.; Vuong, B.; Chiu, C.G.; Bilchik, A.J. AJCC cancer staging manual 7th edition criteria for colon cancer: Do the complex modifications improve prognostic assessment? J. Am. Coll. Surg. 2013, 217, 181–190. [Google Scholar] [CrossRef]
- World Health Organization. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000. [Google Scholar]
- Fitzgerald, P.J. Is norepinephrine an etiological factor in some types of cancer? Int. J. Cancer 2009, 124, 257–263. [Google Scholar] [CrossRef]
- Zhong, S.; Yu, D.; Zhang, X.; Chen, X.; Yang, S.; Tang, J.; Zhao, J.; Wang, S. Beta-blocker use and mortality in cancer patients: Systematic review and meta-analysis of observational studies. Eur. J. Cancer Prev. 2016, 25, 440–448. [Google Scholar] [CrossRef]
- Komninou, D.; Ayonote, A.; Richie, J.P., Jr.; Rigas, B. Insulin resistance and its contribution to colon carcinogenesis. Exp Biol Med 2003, 228, 396–405. [Google Scholar] [CrossRef]
- Zeman, R.J.; Ludemann, R.; Easton, T.G.; Etlinger, J.D. Slow to fast alterations in skeletal muscle fibers caused by clenbuterol, a beta 2-receptor agonist. Am. J. Physiol. 1988, 254, E726–E732. [Google Scholar] [CrossRef] [PubMed]
- Jamerson, K.A.; Smith, S.D.; Amerena, J.V.; Grant, E.; Julius, S. Vasoconstriction with norepinephrine causes less forearm insulin resistance than a reflex sympathetic vasoconstriction. Hypertension 1994, 23, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Abbruzzese, C.; Diodoro, M.G.; Sperduti, I.; Mileo, A.M.; Pattaro, G.; De Salvo, L.; Cosimelli, M.; Perrotti, N.; Paggi, M.G. Detection of phosphorylated insulin receptor in colorectal adenoma and adenocarcinoma: Implications for prognosis and clinical outcome. J. Cell. Physiol. 2015, 230, 562–567. [Google Scholar] [CrossRef] [PubMed]
- van der Sijp, M.P.; Bastiaannet, E.; Mesker, W.E.; van der Geest, L.G.; Breugom, A.J.; Steup, W.H.; Marinelli, A.W.; Tseng, L.N.; Tollenaar, R.A.; van de Velde, C.J.; et al. Differences between colon and rectal cancer in complications, short-term survival and recurrences. Int. J. Colorectal Dis. 2016, 31, 1683–1691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, E.K.; Giovannucci, E.; Wu, K.; Rosner, B.; Fuchs, C.S.; Willett, W.C.; Colditz, G.A. Comparison of risk factors for colon and rectal cancer. Int. J. Cancer 2004, 108, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Paschke, S.; Jafarov, S.; Staib, L.; Kreuser, E.D.; Maulbecker-Armstrong, C.; Roitman, M.; Holm, T.; Harris, C.C.; Link, K.H.; Kornmann, M. Are colon and rectal cancer two different tumor entities? A proposal to abandon the term colorectal cancer. Int. J. Mol. 2018, 19, 2577. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, H. Effect of measurement duration on accuracy of pulse-counting. Ergonomics 2013, 56, 1940–1944. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Variable | Control | Cases | p | ||||
|---|---|---|---|---|---|---|---|
| Colorectal | Colon | Rectum | †P | ‡P | §P | ||
| N | 5909 | 1241 | 854 | 387 | |||
| Age (years) | 47.3 ± 15.5 | 62.6 ± 11.8 | 63.4 ± 11.5 | 61.0 ± 12.4 | * | * | * |
| Gender | * | * | * | ||||
| Male | 2836 (48.0) | 712 (57.4) | 464 (54.3) | 248 (64.1) | |||
| Female | 3073 (52.0) | 529 (42.6) | 390 (45.7) | 139 (35.9) | |||
| SBP (mmHg) | 116.5 ± 15.6 | 126.0 ± 15.1 | 126.2 ± 15.1 | 125.4 ± 15.0 | * | * | * |
| DBP (mmHg) | 75.2 ± 10.2 | 77.2 ± 10.3 | 77.1 ± 10.3 | 77.5 ± 10.2 | * | * | * |
| RHR (bpm) | 68.7 ± 9.0 | 72.7 ± 11.3 | 72.8 ± 11.3 | 72.3 ± 11.3 | * | * | * |
| Weight status | * | * | NS | ||||
| Underweight | 2386 (40.4) | 555 (44.7) | 380 (44.5) | 175 (45.2) | |||
| Normal | 1442 (24.4) | 308 (24.8) | 217 (25.4) | 91 (23.5) | |||
| Overweight | 1844 (31.2) | 310 (25.0) | 210 (24.6) | 100 (25.8) | |||
| Obese | 237 (4.0) | 68 (5.5) | 47 (5.5) | 21 (5.4) | |||
| WBC (103 cells) | 6.2 ± 1.3 | 6.4 ± 1.5 | 6.6 ± 1.5 | 6.1 ± 1.4 | * | * | NS |
| Glucose (mg/dL) | 98.9 ± 21.1 | 109.4 ± 31.2 | 110.3 ± 32.5 | 107.5 ± 28.2 | * | * | * |
| TC (mg/dL) | 188.1 ± 33.7 | 176.1 ± 36.7 | 173.3 ± 35.7 | 182.1 ± 38.2 | * | * | * |
| HTN, n (%) | 913 (15.4) | 518 (41.7) | 374 (43.8) | 144 (37.2) | * | * | * |
| DM, n (%) | 371 (6.3) | 225 (18.1) | 161 (18.8) | 64 (16.5) | * | * | * |
| Dyslipidemia, n (%) | 405 (6.8) | 200 (16.1) | 147 (17.2) | 53 (13.7) | * | * | * |
| Alcohol | * | * | * | ||||
| Never | 602 (10.2) | 688 (55.4) | 492 (57.6) | 196 (50.7) | |||
| Ex | 804 (13.6) | 330 (26.6) | 187 (21.9) | 143 (37.0) | |||
| Current | 4503 (76.2) | 223 (18.0) | 175 (20.5) | 48 (12.4) | |||
| Smoking | * | * | * | ||||
| Never | 3383 (57.3) | 764 (61.5) | 552 (64.6) | 212 (54.8) | |||
| Ex | 1183 (20.0) | 362 (29.2) | 222 (26.0) | 140 (36.2) | |||
| Current | 1343 (22.7) | 115 (9.3) | 80 (9.4) | 35 (9.0) | |||
| TNM stage | |||||||
| 0 | - | 326 (26.3) | 187 (21.9) | 139 (35.9) | |||
| I | - | 365 (29.4) | 270 (31.6) | 95 (24.6) | |||
| II | - | 359 (28.9) | 257 (30.1) | 102 (26.4) | |||
| III | - | 191 (15.4) | 140 (16.4) | 51 (13.2) | |||
| Variable | Control | Colorectal | p | Control | Colon | p | Control | Rectum | p |
|---|---|---|---|---|---|---|---|---|---|
| N | 1207 | 1207 | 829 | 829 | 378 | 378 | |||
| Age (years) | 62.0 ± 11.4 | 62.0 ± 11.4 | NS | 62.7 ± 11.1 | 62.7 ± 11.1 | NS | 60.4 ± 12.0 | 60.4 ± 12.0 | NS |
| Gender | NS | NS | NS | ||||||
| Male | 695 (57.6) | 695 (57.6) | 452 (54.5) | 452 (54.5) | 243 (64.3) | 243 (64.3) | |||
| Female | 512 (42.4) | 512 (42.4) | 377 (45.5) | 377 (45.5) | 135 (35.7) | 135 (35.7) | |||
| SBP (mmHg) | 123.6 ± 16.1 | 125.6 ± 15.0 | * | 123.4 ± 16.3 | 126.1 ± 15.0 | * | 124.2 ± 15.9 | 125.4 ± 15.0 | NS |
| DBP (mmHg) | 75.6 ± 10.3 | 77.3 ± 10.3 | * | 75.4 ± 10.2 | 77.2 ± 10.3 | * | 76.3 ± 10.4 | 77.5 ± 10.2 | NS |
| RHR (bpm) | 67.6 ± 9.2 | 72.7 ± 11.3 | * | 67.8 ± 9.2 | 72.9 ± 11.4 | * | 67.1 ± 9.1 | 72.2 ± 11.3 | * |
| Weight status | * | * | * | ||||||
| Underweight | 28 (2.3) | 64 (5.3) | 18 (2.2) | 45 (5.4) | 10 (2.6) | 19 (5.0) | |||
| Normal | 423 (35.1) | 543 (45.0) | 302 (36.4) | 372 (44.9) | 121 (32.0) | 171 (45.2) | |||
| Overweight | 338 (28.0) | 302 (25.0) | 226 (27.3) | 211 (25.5) | 112 (29.6) | 91 (24.1) | |||
| Obese | 418 (34.3) | 298 (24.7) | 283 (34.1) | 201 (24.3) | 135 (35.7) | 97 (25.7) | |||
| WBC (103 cells) | 6.2 ± 1.3 | 6.4 ± 1.5 | * | 6.1 ± 1.3 | 6.6 ± 1.5 | * | 6.2 ± 1.3 | 6.1 ± 1.4 | NS |
| Glucose (mg/dL) | 103.6 ± 22.0 | 109.3 ± 31.1 | * | 102.9 ± 20.7 | 110.2 ± 32.3 | * | 105.2 ± 24.6 | 107.5 ± 28.1 | NS |
| TC (mg/dL) | 191.2 ± 34.7 | 177.0 ± 36.4 | * | 192.0 ± 34.7 | 174.4 ± 35.3 | * | 189.5 ± 34.6 | 182.6 ± 38.2 | * |
| HTN, n (%) | 381 (31.6) | 497 (41.18) | * | 278 (33.5) | 357 (43.1) | * | 103 (27.2) | 140 (37.0) | * |
| DM, n (%) | 148 (12.3) | 216 (17.90) | * | 102 (12.3) | 157 (18.9) | * | 46 (12.2) | 59 (15.6) | NS |
| Dyslipidemia,n (%) | 130 (10.77) | 193 (16.0) | * | 100 (12.1) | 141 (17.0) | * | 30 (7.9) | 52 (13.8) | * |
| Alcohol | * | * | * | ||||||
| Never | 189 (15.7) | 659 (54.6) | 149 (18.0) | 470 (56.7) | 40 (10.6) | 189 (50.0) | |||
| Ex | 220 (18.2) | 325 (26.9) | 151 (18.2) | 184 (22.2) | 69 (18.2) | 141 (37.3) | |||
| Current | 798 (66.1) | 223 (18.5) | 529 (63.8) | 175 (21.1) | 269 (71.2) | 48 (12.7) | |||
| Smoking | * | * | * | ||||||
| Never | 591 (49.0) | 740 (61.3) | 430 (51.9) | 533 (64.3) | 161 (42.6) | 207 (54.8) | |||
| Ex | 351 (29.1) | 352 (29.2) | 237 (28.6) | 216 (26.1) | 114 (30.2) | 136 (36.0) | |||
| Current | 265 (21.9) | 115 (9.5) | 162 (19.5) | 80 (9.6) | 103 (27.3) | 35 (9.2) | |||
| TNM stage | |||||||||
| 0 | - | 320 (26.5) | - | 184 (22.2) | - | 136 (36.0) | |||
| I | - | 353 (29.3) | - | 260 (31.4) | - | 93 (24.6) | |||
| II | - | 345 (28.6) | - | 246 (29.7) | - | 99 (26.2) | |||
| III | - | 189 (15.7) | - | 139 (16.8) | - | 50 (13.2) |
| Model | Colorectal Cancer | Colon Cancer | Rectal Cancer | |||
|---|---|---|---|---|---|---|
| OR (95% CIs) | p | OR (95% CIs) | p | OR (95% CIs) | p | |
| Before PS matching | ||||||
| Univariable * | 1.043 (1.036–1.049) | <0.001 | 1.045 (1.037–1.053) | <0.001 | 1.040 (1.030–1.051) | <0.001 |
| Multivariable † | 1.043 (1.034–1.051) | <0.001 | 1.046 (1.037–1.055) | <0.001 | 1.040 (1.027–1.052) | <0.001 |
| After PS matching | ||||||
| Univariable ** | 1.051 (1.042–1.060) | <0.001 | 1.050 (1.039–1.061) | <0.001 | 1.053 (1.036–1.070) | <0.001 |
| Multivariable ‡ | 1.044 (1.032–1.057) | <0.001 | 1.046 (1.032–1.061) | <0.001 | 1.035 (1.008–1.063) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, Y.-J.; Lee, H.S.; Cho, M.R.; Kim, S.N.; Jeon, J.Y.; Kim, N.K.; Lee, J.-W. Association between Resting Heart Rate and Colorectal Cancer: Results from a Case-Controlled Study. Int. J. Environ. Res. Public Health 2019, 16, 2883. https://doi.org/10.3390/ijerph16162883
Kwon Y-J, Lee HS, Cho MR, Kim SN, Jeon JY, Kim NK, Lee J-W. Association between Resting Heart Rate and Colorectal Cancer: Results from a Case-Controlled Study. International Journal of Environmental Research and Public Health. 2019; 16(16):2883. https://doi.org/10.3390/ijerph16162883
Chicago/Turabian StyleKwon, Yu-Jin, Hye Sun Lee, Mi Ra Cho, Si Nae Kim, Justin Y. Jeon, Nam Kyu Kim, and Ji-Won Lee. 2019. "Association between Resting Heart Rate and Colorectal Cancer: Results from a Case-Controlled Study" International Journal of Environmental Research and Public Health 16, no. 16: 2883. https://doi.org/10.3390/ijerph16162883