Long-Term Trends of Liver Cancer Incidence and Mortality in China 1990–2017: A Joinpoint and Age–Period–Cohort Analysis


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Incidence and Mortality Data of Liver Cancer
2.3. Statistical Analysis
2.3.1. Age–Period–Cohort Analysis
2.3.2. Joinpoint Regression Analysis
3. Results
3.1. Descriptive Analysis of Incidence and Mortality Trends
3.2. Age–Period–Cohort Analysis
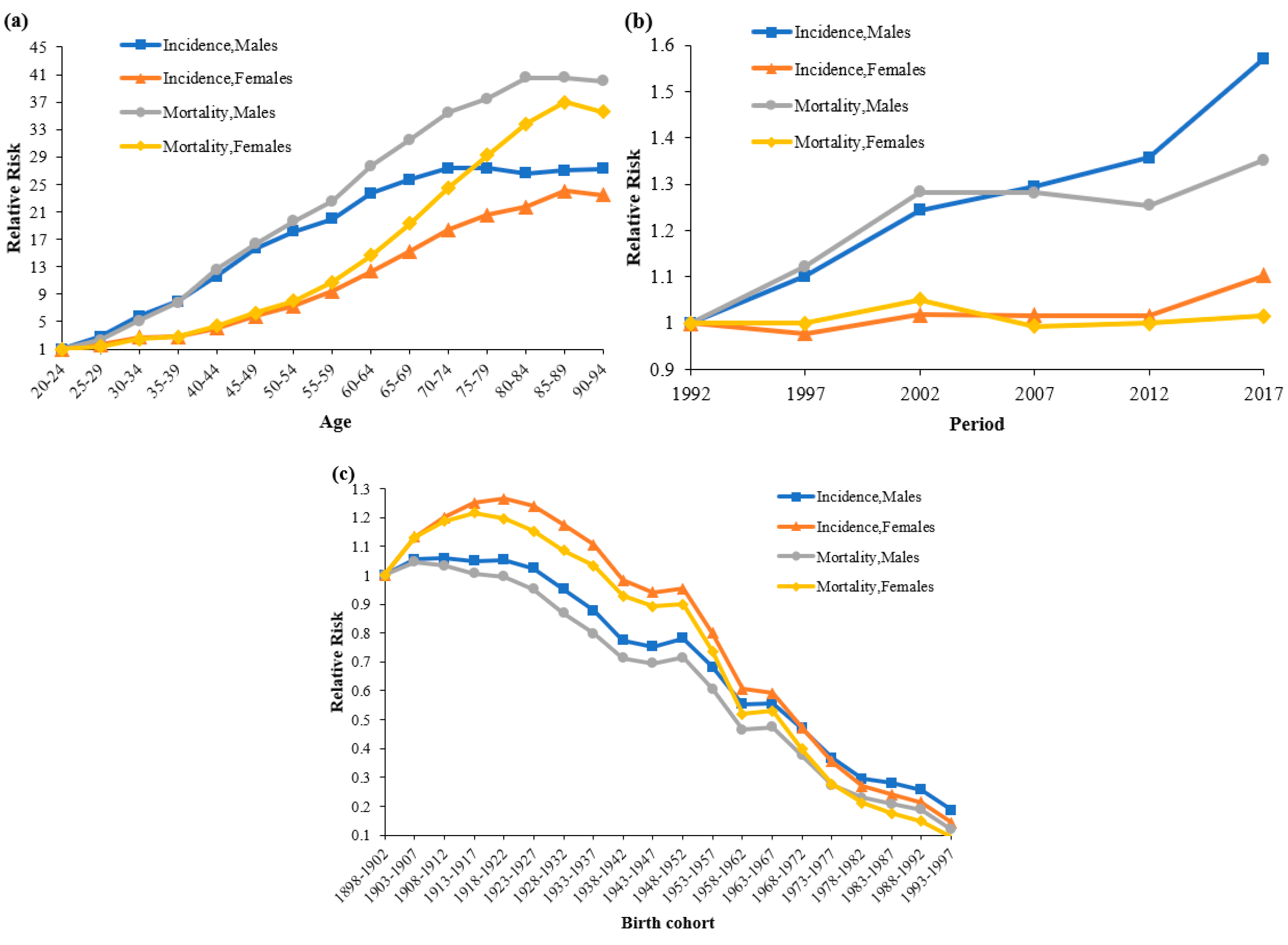
3.2.1. Age Effect
3.2.2. Period Effect
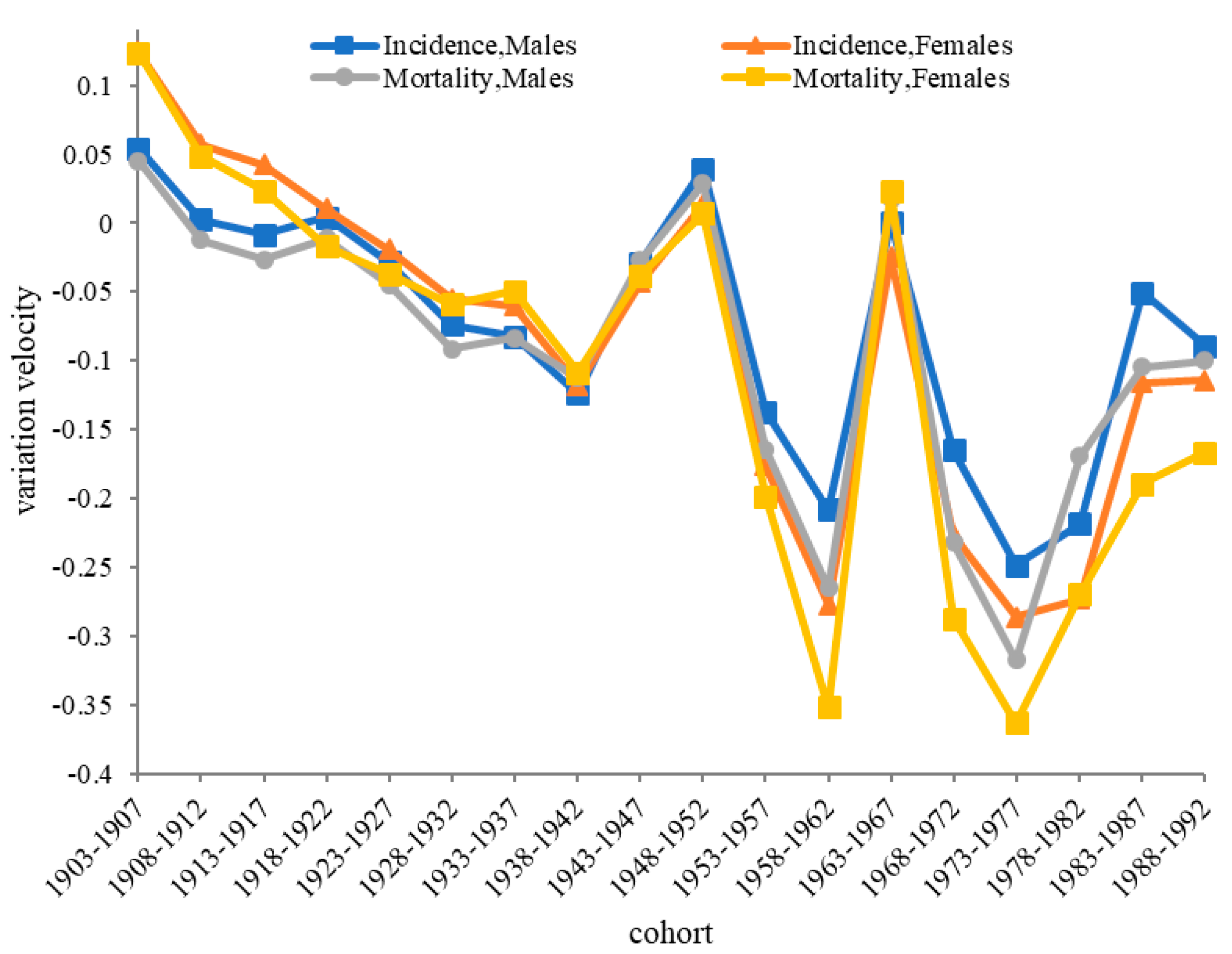
3.2.3. Cohort Effect
4. Discussion
4.1. Age Effects
4.2. Period Effects
4.3. Cohort Effects
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Age Group | Mortality (AAPC) | Incidence (AAPC) | ||||
|---|---|---|---|---|---|---|
| Both Gender | Males | Females | Both Gender | Males | Females | |
| Age-standardized Rate | −0.8 (−0.9, −0.6) | −0.5 (−0.6, −0.3) | −1.3 (−1.6, −1.0) | −0.2 (−0.2, −0.1) | 0.2 (0.1, 0.3.0) | −1.1 (−1.2, −1.0) |
| 5–9 | −3.6 (−4.3, −2.9) | −3.8 (−4.5, −3.0) | −3.6 (−4.9, −2.4) | −2.8 (−3.2, −2.5) | −2.8 (−3.2, −2.5) | −3.1 (−3.4, −2.8) |
| 10–14 | −2.6 (−3.2, −2.0) | −2.9 (−3.5, −2.3) | −2.7 (−4.1, −1.3) | −1.7 (−1.9, −1.4) | −1.9 (−2.2, −1.5) | −1.6 (−1.9, −1.3) |
| 15–19 | −2.7 (−3, −2.4) | −2.3 (−2.7, −1.9) | −3.8 (−4.4, −3.3) | −1.6 (−1.8, −1.4) | −1.1 (−1.4, −0.9) | −2.9 (−3.2, −2.6) |
| 20–24 | −3.4 (−4.6, −2.2) | −2.9 (−3.5, −2.4) | −4.5 (−6.3, −2.7) | −2.3 (−2.6, −2.0) | −1.8 (−2.1, −1.4) | −3.3 (−3.5, −3.1) |
| 25–29 | −2.2 (−4, −0.3) | −1.8 (−3, −0.5) | −3.3 (−4.2, −2.5) | −1.4 (−1.8, −1.0) | −0.9 (−1.3, −0.5) | −2.8 (−3.2, −2.4) |
| 30–34 | −2.5 (−3.6, −1.5) | −2.1 (−3.1, −1.1) | −3.7 (−4.5, −3.0) | −1.4 (−1.7, −1.1) | −1.0 (−1.3, −0.7) | −3.0 (−3.2, −2.7) |
| 35–39 | −2.7 (−3.1, −2.3) | −2.4 (−2.8, −1.9) | −3.9 (−4.2, −3.6) | −1.7 (−1.9, −1.4) | −1.3 (−1.6, −1.1) | −3.1 (−3.2, −2.9) |
| 40–44 | −2.9 (−3.7, −2.2) | −2.6 (−3.5, −1.8) | −3.9 (−4.4, −3.4) | −1.5 (−1.8, −1.3) | −1.1 (−1.3, −0.9) | −2.9 (−3, −2.8) |
| 45–49 | −1.6 (−1.9, −1.3) | −1.3 (−1.6, −1.0) | −2.8 (−3.2, −2.3) | −0.8 (−1, −0.5) | −0.3 (−0.5, −0.2) | −2.4 (−2.6, −2.2) |
| 50–54 | −0.9 (−1.3, −0.5) | −0.5 (−0.9, −0.1) | −1.9 (−2.8, −1.1) | −0.3 (−0.6, 0.0) | 0.3 (0, 0.7) | −1.6 (−1.9, −1.3) |
| 55–59 | −1.5 (−2.3, −0.6) | −1.2 (−1.9, −0.4) | −2.7 (−3.3, −2.1) | −0.6 (−0.8, −0.5) | −0.2 (−0.3, 0.0) | −2.0 (−2.1, −1.8) |
| 60–64 | −0.4 (−0.6, −0.2) | 0 (−0.3, 0.3) | −1.4 (−1.6, −1.2) | 0.1 (0, 0.2) | 0.6 (0.5, 0.7) | −1.0 (−1.2, −0.9) |
| 65–69 | 0.0 (−0.4, 0.5) | 0.5 (0.2, 0.9) | −0.7 (−1, −0.3) | 0.7 (0.4, 0.9) | 1.1 (0.9, 1.4) | −0.5 (−0.7, −0.2) |
| 70–74 | −0.5 (−0.7, −0.2) | −0.3 (−0.5, −0.1) | −1.0 (−1.3, −0.6) | 0 (−0.1, 0.1) | 0.3 (0.2, 0.4) | −0.9 (−1.1, −0.7) |
| 75–79 | −0.2 (−0.6, 0.1) | 0.1 (−0.4, 0.5) | −0.9 (−1.2, −0.6) | 0.2 (0.2, 0.3) | 0.7 (0.6, 0.8) | −0.8 (−0.8, −0.7) |
| 80–84 | 0.2 (−0.2, 0.6) | 0.4 (0, 0.8) | −0.3 (−0.9, 0.4) | 0.9 (0.8, 1.0) | 1.2 (1.1, 1.3) | 0.3 (0.2, 0.3) |
| 85–89 | 0.3 (0, 0.7) | 0.5 (0.2, 0.8) | −0.1 (−0.5, 0.4) | 1.0 (0.9, 1.0) | 1.3 (1.3, 1.4) | 0.4 (0.4, 0.5) |
| 90–94 | 0.7 (0.3, 1.1) | 1.0 (0.6, 1.4) | 0.5 (0.3, 0.7) | 1.5 (1.4, 1.6) | 1.8 (1.7, 1.9) | 1.2 (1.1, 1.3) |

References
- GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990−2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Burden of Disease Liver Cancer Collaboration. The Burden of Primary Liver Cancer and Underlying Etiologies From 1990 to 2015 at the Global, Regional, and National Level: Results from the Global Burden of Disease Study 2015. JAMA Oncol. 2017, 3, 1683–1691. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Wang, H.; Zeng, X.; Yin, P.; Zhu, J.; Chen, W.; Li, X.; Wang, L.; Wang, L.; Liu, Y.; et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, in press. [Google Scholar] [CrossRef]
- Cocker, F.; Yee, K.C.; Palmer, A.J.; De Graaff, B. Increasing incidence and mortality related to liver cancer in Australia: Time to turn the tide. Aust. N. Z. J. Public Health 2019, 43, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Jiang, Y.; Yuan, H.; Fang, Q.; Cai, N.; Suo, C.; Jin, L.; Zhang, T.; Chen, X. The trends in incidence of primary liver cancer caused by specific etiologies: Results from the Global Burden of Disease Study 2016 and implications for liver cancer prevention. J. Hepatol. 2019, 70, 674–683. [Google Scholar] [CrossRef]
- Tapper, E.B.; Parikh, N.D. Mortality due to cirrhosis and liver cancer in the United States, 1999–2016: Observational study. BMJ 2018, 362, k2817. [Google Scholar] [CrossRef]
- Maucort-Boulch, D.; De Martel, C.; Franceschi, S.; Plummer, M. Fraction and incidence of liver cancer attributable to hepatitis B and C viruses worldwide. Int. J. Cancer 2018, 142, 2471–2477. [Google Scholar] [CrossRef]
- Wu, J.; Yang, S.; Xu, K.; Ding, C.; Zhou, Y.; Fu, X.; Li, Y.; Deng, M.; Wang, C.; Liu, X.; et al. Patterns and Trends of Liver Cancer Incidence Rates in Eastern and Southeastern Asian Countries (1983–2007) and Predictions to 2030. Gastroenterology 2018, 154, 1719–1728.e5. [Google Scholar] [CrossRef]
- Petrick, J.L.; Braunlin, M.; Laversanne, M.; Valery, P.; Bray, F.; McGlynn, K.A. International trends in liver cancer incidence, overall and by histologic subtype, 1978–2007. Int. J. Cancer 2016, 139, 1534–1545. [Google Scholar] [CrossRef]
- Zeng, H.; Chen, W.; Zheng, R.; Zhang, S.; Ji, J.S.; Zou, X.; Xia, C.; Sun, K.; Yang, Z.; Li, H.; et al. Changing cancer survival in China during 2003–15: A pooled analysis of 17 population-based cancer registries. Lancet Glob. Health 2018, 6, e555–e567. [Google Scholar] [CrossRef]
- Srivatanakul, P.; Sriplung, H.; Deerasamee, S. Epidemiology of liver cancer: An overview. Asian Pac. J. Cancer Prev. 2004, 5, 118–125. [Google Scholar]
- Tsai, W.-C.; Kung, P.-T.; Wang, Y.-H.; Kuo, W.-Y.; Li, Y.-H. Influence of the time interval from diagnosis to treatment on survival for early-stage liver cancer. PLoS ONE 2018, 13, e0199532. [Google Scholar] [CrossRef]
- Endeshaw, M.; Hallowell, B.D.; Razzaghi, H.; Senkomago, V.; McKenna, M.T.; Saraiya, M. Trends in liver cancer mortality in the United States: Dual burden among foreign- and US-born persons. Cancer 2019, 125, 726–734. [Google Scholar] [CrossRef]
- Kihn-Alarcón, A.J.; Toledo-Ponce, M.F.; Velarde, A.; Xu, X. Liver Cancer in Guatemala: An Analysis of Mortality and Incidence Trends from 2012 to 2016. J. Glob. Oncol. 2019, 5, 1–8. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, Y.; Li, M.; Cheng, K.; Zhao, X.; Zheng, Y.; Liu, Y.; Lei, S.; Wang, L. Long-term trends of liver cancer mortality by gender in urban and rural areas in China: An age-period-cohort analysis. BMJ Open 2018, 8, e020490. [Google Scholar] [CrossRef]
- Ho, Y.R.; Ma, S.-P.; Chang, K.Y. Trends in regional cancer mortality in Taiwan 1992–2014. Cancer Epidemiol. 2019, 59, 185–192. [Google Scholar] [CrossRef]
- Melkonian, S.C.; Jim, M.A.; Reilley, B.; Erdrich, J.; Berkowitz, Z.; Wiggins, C.L.; Haverkamp, D.; White, M.C. Incidence of primary liver cancer in American Indians and Alaska Natives, US, 1999–2009. Cancer Causes Control. 2018, 29, 833–844. [Google Scholar] [CrossRef]
- Zheng, R.; Qu, C.; Zhang, S.; Zeng, H.; Sun, K.; Gu, X.; Xia, C.; Yang, Z.; Li, H.; Wei, W.; et al. Liver cancer incidence and mortality in China: Temporal trends and projections to 2030. Chin. J. Cancer Res. 2018, 30, 571–579. [Google Scholar] [CrossRef]
- Mak, D.; Sengayi, M.; Chen, W.C.; De Villiers, C.B.; Singh, E.; Kramvis, A. Liver cancer mortality trends in South Africa: 1999–2015. BMC Cancer 2018, 18, 798. [Google Scholar] [CrossRef]
- Yang, Y.; Fu, W.; Land, K. A Methodological Comparison of Age-Period-Cohort Models: The Intrinsic Estimator and Conventional Generalized Linear Models. Sociol. Methodol. 2004, 34, 75–110. [Google Scholar] [CrossRef]
- Su, S.Y.; Chiang, C.J.; Yang, Y.W.; Lee, W.C. Secular trends in liver cancer incidence from 1997 to 2014 in Taiwan and projection to 2035: An age-period-cohort analysis. J. Formos. Med. Assoc. 2019, 118, 444–449. [Google Scholar] [CrossRef]
- Dal Maso, L.; Lise, M.; Zambon, P.; Crocetti, E.; Serraino, D.; Ricceri, F.; Vercelli, M.; de Lisi, V.; Tagliabue, G.; Federico, M.; et al. Incidence of primary liver cancer in Italy between 1988 and 2002: An age-period-cohort analysis. Eur. J. Cancer 2008, 44, 285–292. [Google Scholar] [CrossRef]
- Jiang, X.; Pan, S.Y.; De Groh, M.; Liu, S.; Morrison, H. Increasing incidence in liver cancer in Canada, 1972–2006: Age-period-cohort analysis. J. Gastrointest. Oncol. 2011, 2, 223–231. [Google Scholar]
- Fang, E.F.; Scheibye-Knudsen, M.; Jahn, H.J.; Li, J.; Ling, L.; Guo, H.; Zhu, X.; Preedy, V.; Lu, H.; Bohr, V.A.; et al. A research agenda for aging in China in the 21st century. Ageing Res. Rev. 2015, 24, 197–205. [Google Scholar] [CrossRef] [Green Version]
- Manthey, J.; Shield, K.D.; Rylett, M.; Hasan, O.S.M.; Probst, C.; Rehm, J. Global alcohol exposure between 1990 and 2017 and forecasts until 2030: A modelling study. Lancet 2019, 393, 2493–2502. [Google Scholar] [CrossRef]
- Arem, H.; Loftfield, E.; Saint-Maurice, P.F.; Freedman, N.D.; Matthews, C.E. Physical activity across the lifespan and liver cancer incidence in the NIH-AARP Diet and Health Study cohort. Cancer Med. 2018, 7, 1450–1457. [Google Scholar] [CrossRef] [Green Version]
- Fu, J.; Wang, H. Precision diagnosis and treatment of liver cancer in China. Cancer Lett. 2018, 412, 283–288. [Google Scholar] [CrossRef]
- Benhamiche, A.-M.; Faivre, C.; Minello, A.; Clinard, F.; Mitry, E.; Hillon, P.; Faivre, J.; Faivre-Finn, C. Time trends and age-period-cohort effects on the incidence of primary liver cancer in a well-defined French population: 1976–1995. J. Hepatol. 1998, 29, 802–806. [Google Scholar] [CrossRef]
- Li, C.; Lumey, L. Exposure to the Chinese famine of 1959–61 in early life and long-term health conditions: A systematic review and meta-analysis. Int. J. Epidemiol. 2017, 46, 1157–1170. [Google Scholar] [CrossRef]
- Liu, X.Z.; Wang, J.L. An introduction to China’s health care system. J. Public Health Policy 1991, 12, 104–116. [Google Scholar] [CrossRef]
- Huang, W.; Long, H.; Li, J.; Tao, S.; Zheng, P.; Tang, S.; Abdullah, A.S. Delivery of public health services by community health workers (CHWs) in primary health care settings in China: A systematic review (1996–2016). Glob. Health Res. Policy 2018, 3, 18. [Google Scholar] [CrossRef]
- Wang, F.; Liang, Y. China’s Rural Cooperative Medical Scheme: A type of health insurance or a type of health cooperative? Prim. Health Care Res. Dev. 2017, 18, 194–199. [Google Scholar] [CrossRef]
- Shi, L. Health care in China: A rural-urban comparison after the socioeconomic reforms. Bull. World Health Organ. 1993, 71, 723–736. [Google Scholar]
- Zhang, J.; Mauzerall, D.L.; Zhu, T.; Liang, S.; Ezzati, M.; Remais, J.V. Environmental health in China: Progress towards clean air and safe water. Lancet 2010, 375, 1110–1119. [Google Scholar] [CrossRef]
- Dorak, M.T.; Karpuzoglu, E. Gender Differences in Cancer Susceptibility: An Inadequately Addressed Issue. Front. Genet. 2012, 3, 268. [Google Scholar] [CrossRef] [Green Version]
- Duan, T. An exploratory discussion on the lateralization of rural females in distribution of household resources in the underdeveloped areas in western China. J. Shaanxi Norm. Univ. 2008, 37, 122–128. [Google Scholar]
- Chen, L.; Liu, R.; Pozhidaeva, M.; Xie, J.; Cao, W.; Zhang, F.; Reis, C.; Sharma, M.; Zhao, Y. Changes in the Sociodemographic Factors of Tobacco and Alcohol Consumption in Chinese Adolescents from 2004 to 2011. Int. J. Environ. Res. Public Health 2018, 15, 1211. [Google Scholar] [CrossRef]
- Im, P.K.; Millwood, I.Y.; Guo, Y.; Du, H.; Chen, Y.; Bian, Z.; Tan, Y.; Guo, Z.; Wu, S.; Hua, Y.; et al. Patterns and trends of alcohol consumption in rural and urban areas of China: Findings from the China Kadoorie Biobank. BMC Public Health 2019, 19, 217. [Google Scholar] [CrossRef]
- Millwood, I.Y.; Walters, R.G.; Mei, X.W.; Guo, Y.; Yang, L.; Bian, Z.; Bennett, D.A.; Chen, Y.; Dong, C.; Hu, R.; et al. Conventional and genetic evidence on alcohol and vascular disease aetiology: A prospective study of 500 000 men and women in China. Lancet 2019, 393, 1831–1842. [Google Scholar] [CrossRef]
- Liu, R.; Chen, L.; Zeng, H.; Reis, C.; Reis, H.; Yang, X.; Lin, X.; Li, H.; Meng, X.; Sharma, M.; et al. Tobacco and Alcohol Consumption Rates among Chinese Women of Reproductive Age in 2004–2011: Rate and Sociodemographic Influencing Factors. Int. J. Environ. Res. Public Health 2018, 16, 56. [Google Scholar] [CrossRef]
- Liu, X.; Baecker, A.; Wu, M.; Zhou, J.Y.; Yang, J.; Han, R.Q.; Wang, P.; Jin, Z.; Liu, A.; Gu, X.; et al. Interaction between tobacco smoking and hepatitis B virus infection on the risk of liver cancer in a Chinese population. Int. J. Cancer 2018, 142, 1560–1567. [Google Scholar] [CrossRef]
- Ding, C.; Fu, X.; Zhou, Y.; Liu, X.; Wu, J.; Huang, C.; Deng, M.; Li, Y.; Li, L.; Yang, S. Disease burden of liver cancer in China from 1997 to 2016: An observational study based on the Global Burden of Diseases. BMJ Open 2019, 9, e025613. [Google Scholar] [CrossRef]
- Chen, J.G.; Zhang, S.W. Liver cancer epidemic in China: Past, present and future. Semin. Cancer Biol. 2011, 21, 59–69. [Google Scholar] [CrossRef]
- Yang, F.; Ma, L.; Yang, Y.; Liu, W.; Zhao, J.; Chen, X.; Wang, M.; Zhang, H.; Cheng, S.; Shen, F.; et al. Contribution of Hepatitis B Virus Infection to the Aggressiveness of Primary Liver Cancer: A Clinical Epidemiological Study in Eastern China. Front. Oncol. 2019, 9, 370. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Wang, Y.; Feng, X.; Wang, R.; Wang, Y.; Zeng, H.; Qi, J.; Zhao, H.; Li, N.; Cai, J.; et al. Contribution of hepatitis B virus and hepatitis C virus to liver cancer in China north areas: Experience of the Chinese National Cancer Center. Int. J. Infect. Dis. 2017, 65, 15–21. [Google Scholar] [CrossRef] [Green Version]
- Luo, Z.; Li, L.; Ruan, B. Impact of the implementation of a vaccination strategy on hepatitis B virus infections in China over a 20-year period. Int. J. Infect. Dis. 2012, 16, e82–e88. [Google Scholar] [CrossRef] [Green Version]
- Qu, C.; Chen, T.; Fan, C.; Zhan, Q.; Wang, Y.; Lü, J.; Lu, L.-L.; Ni, Z.; Huang, F.; Yao, H.; et al. Efficacy of Neonatal HBV Vaccination on Liver Cancer and Other Liver Diseases over 30-Year Follow-up of the Qidong Hepatitis B Intervention Study: A Cluster Randomized Controlled Trial. PLoS Med. 2014, 11, e1001774. [Google Scholar] [CrossRef]
- Cui, F.; Shen, L.; Li, L.; Wang, H.; Wang, F.; Bi, S.; Liu, J.; Zhang, G.; Wang, F.; Zheng, H.; et al. Prevention of Chronic Hepatitis B after 3 Decades of Escalating Vaccination Policy, China. Emerg. Infect. Dis. 2017, 23, 765–772. [Google Scholar] [CrossRef] [Green Version]


| Segments | Both | Males | Females | |||
|---|---|---|---|---|---|---|
| Year | APC * (95% CI) | Year | APC (95% CI) | Year | APC (95% CI) | |
| ASMR | ||||||
| trend1 | 1990–2000 | 0.0 (−0.1, 0.2) | 1990–2000 | 0.5 * (0.4, 0.6) | 1990–2000 | −0.9 * (−1.2, −0.6) |
| trend2 | 2000–2004 | −1.5 * (−2.1, −0.8) | 2000–2004 | −1.4 * (−2.1, −0.7) | 2000–2004 | −1.6 * (−2.7, −0.4) |
| trend3 | 2004–2007 | −3.7 * (−4.6, −2.7) | 2004–2007 | −3.2 * (−4.1, −2.3) | 2004–2007 | −4.5 * (−6.2, −2.9) |
| trend4 | 2007–2013 | −1.4 * (−1.7, −1.2) | 2007–2013 | −1.5 * (−1.7, −1.3) | 2007–2012 | −1.6 * (−2.2, −1.1) |
| trend5 | 2013–2017 | 1.3 * (0.8, 1.8) | 2013–2017 | 1.6 * (1.1, 2.0) | 2012–2017 | 0.2(−0.3, 0.8) |
| AAPC * | 1990–2017 | −0.8 * (−0.9, −0.6) | 1990–2017 | −0.5 * (−0.6, −0.3) | 1990–2017 | −1.3 * (−1.6, −1.0) |
| ASIR | ||||||
| trend1 | 1990–2000 | 0.2 * (0.1, 0.3) | 1990–2000 | 0.7 * (0.6, 0.7) | 1990–2000 | −0.9 * (−1, −0.8) |
| trend2 | 2000–2010 | −1.9 *(−1.9, −1.9) | 2000–2009 | −1.7 * (−1.7, −1.6) | 2000–2006 | −2.2(−2.4, −2.1) |
| trend3 | 2010–2013 | 0.9 * (0.5, 1.4) | 2009–2012 | 0.3(−0.2, 0.8) | 2006–2009 | −3.1 * (−3.4, −2.7) |
| trend4 | 2013–2017 | 2.5 * (2.2, 2.7) | 2012–2015 | 2.4 * (1.9, 2.9) | 2009–2012 | −0.8 * (−1.4, −0.3) |
| trend5 | - | - | 2015–2017 | 3.5 * (2.6, 4.5) | 2012–2017 | 0.9 * (0.7, 1.1) |
| AAPC | 1990–2017 | −0.2 * (−0.2, −0.1) | 1990–2017 | 0.2 * (0.1, 0.3) | 1990–2017 | −1.1 * (−1.2, −1.0) |
| Variables | Incidence (Coef, 95% CI) | Mortality (Coef, 95% CI) | ||
|---|---|---|---|---|
| Males | Females | Males | Females | |
| Age | ||||
| 20–24 | −2.59 * (−4.98, −0.21) | −2.03 * (−3.58, −0.48) | −2.73 (−6.43, 0.97) | −2.19 (−4.75, 0.36) |
| 25–29 | −1.57 *** (−2.33, −0.8) | −1.53 *** (−2.31, −0.76) | −1.9 ** (−3.29, −0.52) | −1.86 * (−3.31, −0.41) |
| 30–34 | −0.83 ** (−1.3, −0.36) | −1.04 *** (−1.54, −0.54) | −1.1 ** (−1.90, −0.30) | −1.29 ** (−2.18, −0.40) |
| 35–39 | −0.52 ** (−0.91, −0.13) | −1.00 *** (−1.43, −0.57) | −0.68 * (−1.32, −0.04) | −1.17 ** (−1.9, −0.45) |
| 40–44 | −0.14 (−0.47, 0.19) | −0.63 *** (−0.95, −0.32) | −0.2 (−0.74, 0.33) | −0.73 ** (−1.26, −0.19) |
| 45–49 | 0.16 (−0.12, 0.45) | −0.27 * (−0.52, −0.02) | 0.06 (−0.4, 0.51) | −0.36 (−0.79, 0.06) |
| 50–54 | 0.31 * (0.06, 0.55) | −0.05 (−0.26, 0.15) | 0.24 (−0.15, 0.63) | −0.11(−0.45, 0.22) |
| 55–59 | 0.4 *** (0.19, 0.61) | 0.21 * (0.05, 0.37) | 0.38 * (0.06, 0.71) | 0.18 (−0.08, 0.44) |
| 60–64 | 0.57 *** (0.4, 0.75) | 0.48 *** (0.35, 0.61) | 0.59 *** (0.32, 0.86) | 0.49 *** (0.27, 0.70) |
| 65–69 | 0.66 *** (0.51, 0.81) | 0.69 *** (0.57, 0.81) | 0.72 *** (0.48, 0.95) | 0.76 *** (0.55, 0.98) |
| 70–74 | 0.72 *** (0.59, 0.85) | 0.88 *** (0.75, 1.00) | 0.84 *** (0.61, 1.06) | 1 *** (0.74, 1.26) |
| 75–79 | 0.72 *** (0.59, 0.84) | 0.99 *** (0.84, 1.14) | 0.89 *** (0.65, 1.13) | 1.18 *** (0.85, 1.50) |
| 80–84 | 0.69 *** (0.55, 0.83) | 1.05 *** (0.86, 1.23) | 0.97 *** (0.69, 1.25) | 1.32 *** (0.91, 1.73) |
| 85–89 | 0.71 *** (0.55, 0.86) | 1.15 *** (0.92, 1.38) | 0.97 *** (0.63, 1.30) | 1.41 *** (0.92, 1.91) |
| 90–94 | 0.72 *** (0.53, 0.90) | 1.12 *** (0.85, 1.39) | 0.96 *** (0.56, 1.36) | 1.37 *** (0.78, 1.96) |
| Period | ||||
| 1992 | −0.22 *** (−0.33, −0.11) | −0.02 (−0.15, 0.1) | −0.19 (−0.39, 0.01) | −0.01 (−0.26, 0.24) |
| 1997 | −0.12 *** (−0.19, −0.05) | −0.04 (−0.12, 0.03) | −0.07 (−0.2, 0.05) | −0.01 (−0.16, 0.14) |
| 2002 | 0.00 (−0.04, 0.03) | 0.00 (−0.03, 0.03) | 0.06 * (0.01, 0.10) | 0.04 (−0.01, 0.09) |
| 2007 | 0.04 * (0, 0.07) | 0.00 (−0.03, 0.03) | 0.06 * (0.01, 0.11) | −0.02 (−0.07, 0.04) |
| 2012 | 0.08 * (0.01, 0.15) | −0.01 (−0.08, 0.07) | 0.04 (−0.09, 0.16) | −0.01 (−0.16, 0.14) |
| 2017 | 0.23 *** (0.12, 0.34) | 0.08 (−0.05, 0.20) | 0.11 (−0.09, 0.31) | 0.01 (−0.25, 0.26) |
| Cohort | ||||
| 1898–1902 | 0.48 * (0.06, 0.90) | 0.41 (−0.03, 0.85) | 0.63 (−0.25, 1.50) | 0.54 (−0.39, 1.46) |
| 1903–1907 | 0.53 ** (0.13, 0.94) | 0.53 * (0.12, 0.95) | 0.67 (−0.18, 1.52) | 0.66 (−0.23, 1.55) |
| 1908–1912 | 0.54 ** (0.14, 0.93) | 0.59 ** (0.19, 0.99) | 0.66 (−0.18, 1.49) | 0.71 (−0.15, 1.57) |
| 1913–1917 | 0.53 ** (0.14, 0.91) | 0.63 ** (0.24, 1.02) | 0.63 (−0.19, 1.46) | 0.73 (−0.11, 1.57) |
| 1918–1922 | 0.53 ** (0.15, 0.91) | 0.64 ** (0.26, 1.03) | 0.62 (−0.21, 1.45) | 0.72 (−0.12, 1.55) |
| 1923–1927 | 0.5 * (0.12, 0.89) | 0.62 ** (0.23, 1.01) | 0.57 (−0.26, 1.41) | 0.68 (−0.16, 1.52) |
| 1928–1932 | 0.43 * (0.03, 0.83) | 0.57 ** (0.17, 0.96) | 0.48 (−0.37, 1.33) | 0.62 (−0.24, 1.48) |
| 1933–1937 | 0.35 (−0.06, 0.76) | 0.51* (0.09, 0.92) | 0.4 (−0.47, 1.27) | 0.57 (−0.32, 1.46) |
| 1938–1942 | 0.22 (−0.20, 0.65) | 0.39 (−0.04, 0.82) | 0.29 (−0.62, 1.19) | 0.46 (−0.47, 1.39) |
| 1943–1947 | 0.19 (−0.25, 0.64) | 0.35 (−0.11, 0.81) | 0.26 (−0.68, 1.20) | 0.42 (−0.56, 1.40) |
| 1948–1952 | 0.23 (−0.24, 0.70) | 0.36 (−0.13, 0.85) | 0.29 (−0.69, 1.27) | 0.43 (−0.60, 1.47) |
| 1953–1957 | 0.1 (−0.40, 0.59) | 0.18 (−0.34, 0.71) | 0.12 (−0.90, 1.15) | 0.23 (−0.87, 1.33) |
| 1958–1962 | −0.11 (−0.64, 0.42) | −0.09 (−0.66, 0.47) | −0.14 (−1.22, 0.94) | −0.12 (−1.29, 1.06) |
| 1963–1967 | −0.11 (−0.67, 0.45) | −0.12 (−0.72, 0.49) | −0.12 (−1.25, 1.01) | −0.1 (−1.35, 1.15) |
| 1968–1972 | −0.28 (−0.87, 0.32) | −0.34 (−1.01, 0.32) | −0.35 (−1.55, 0.84) | −0.38 (−1.74, 0.97) |
| 1973–1977 | −0.52 (−1.18, 0.13) | −0.63 (−1.45, 0.19) | −0.67 (−1.98, 0.63) | −0.75 (−2.37, 0.88) |
| 1978–1982 | −0.74 (−1.52, 0.04) | −0.9 (−2.03, 0.22) | −0.84 (−2.36, 0.68) | −1.02 (−3.22, 1.18) |
| 1983–1987 | −0.79 (−1.77, 0.19) | −1.02 (−2.48, 0.44) | −0.95 (−2.97, 1.08) | −1.21 (−4.30, 1.89) |
| 1988–1992 | −0.88 (−2.76, 1.00) | −1.13 (−3.69, 1.42) | −1.05 (−5.16, 3.06) | −1.37 (−7.16, 4.41) |
| 1993–1997 | −1.2 (−9.21, 6.82) | −1.54 (−9.38, 6.30) | −1.5 (−18.46, 15.46) | −1.83 (−18.78, 15.12) |
| AIC | 6.94 | 4.93 | 7.04 | 5.16 |
| BIC | 2099.21 | 77.97 | 2364.42 | 160.07 |
| Deviance | 2333.19 | 311.96 | 2598.40 | 394.06 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, F.; Mubarik, S.; Zhang, Y.; Wang, L.; Wang, Y.; Yu, C.; Li, H. Long-Term Trends of Liver Cancer Incidence and Mortality in China 1990–2017: A Joinpoint and Age–Period–Cohort Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2878. https://doi.org/10.3390/ijerph16162878
Wang F, Mubarik S, Zhang Y, Wang L, Wang Y, Yu C, Li H. Long-Term Trends of Liver Cancer Incidence and Mortality in China 1990–2017: A Joinpoint and Age–Period–Cohort Analysis. International Journal of Environmental Research and Public Health. 2019; 16(16):2878. https://doi.org/10.3390/ijerph16162878
Chicago/Turabian StyleWang, Fang, Sumaira Mubarik, Yu Zhang, Lu Wang, Yafeng Wang, Chuanhua Yu, and Hao Li. 2019. "Long-Term Trends of Liver Cancer Incidence and Mortality in China 1990–2017: A Joinpoint and Age–Period–Cohort Analysis" International Journal of Environmental Research and Public Health 16, no. 16: 2878. https://doi.org/10.3390/ijerph16162878