Children Exposure-Related Behavior Patterns and Risk Perception Associated with Recreational Beach Use



 ,
, 

Abstract
:1. Introduction and Background
2. Methods
2.1. Survey Instruments
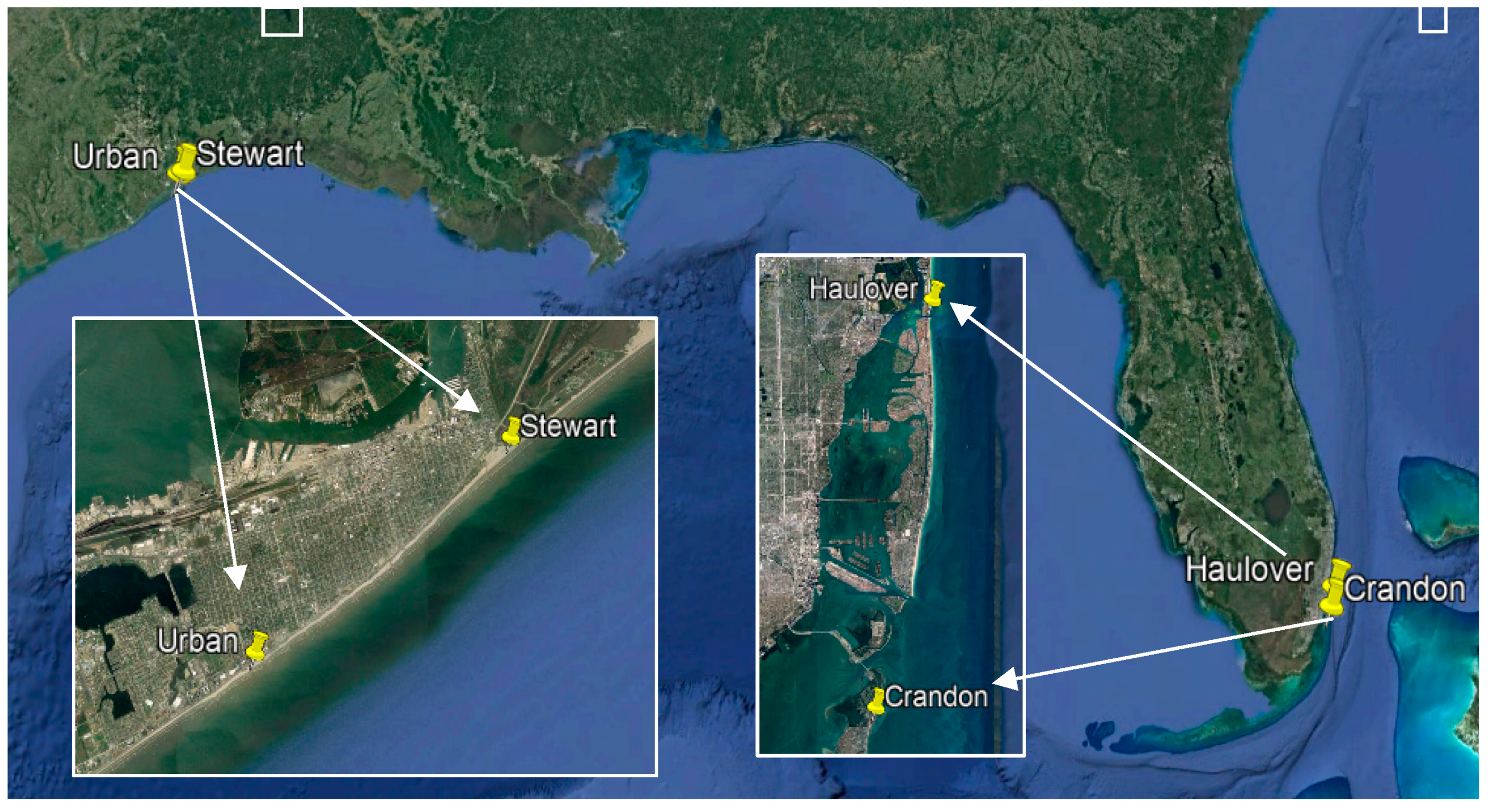
2.2. Recruitment and Data Collection
2.3. Data Refinement and Statistical Analysis
3. Results and Discussion
3.1. Demographic Results
3.2. Exposure Assessment Results
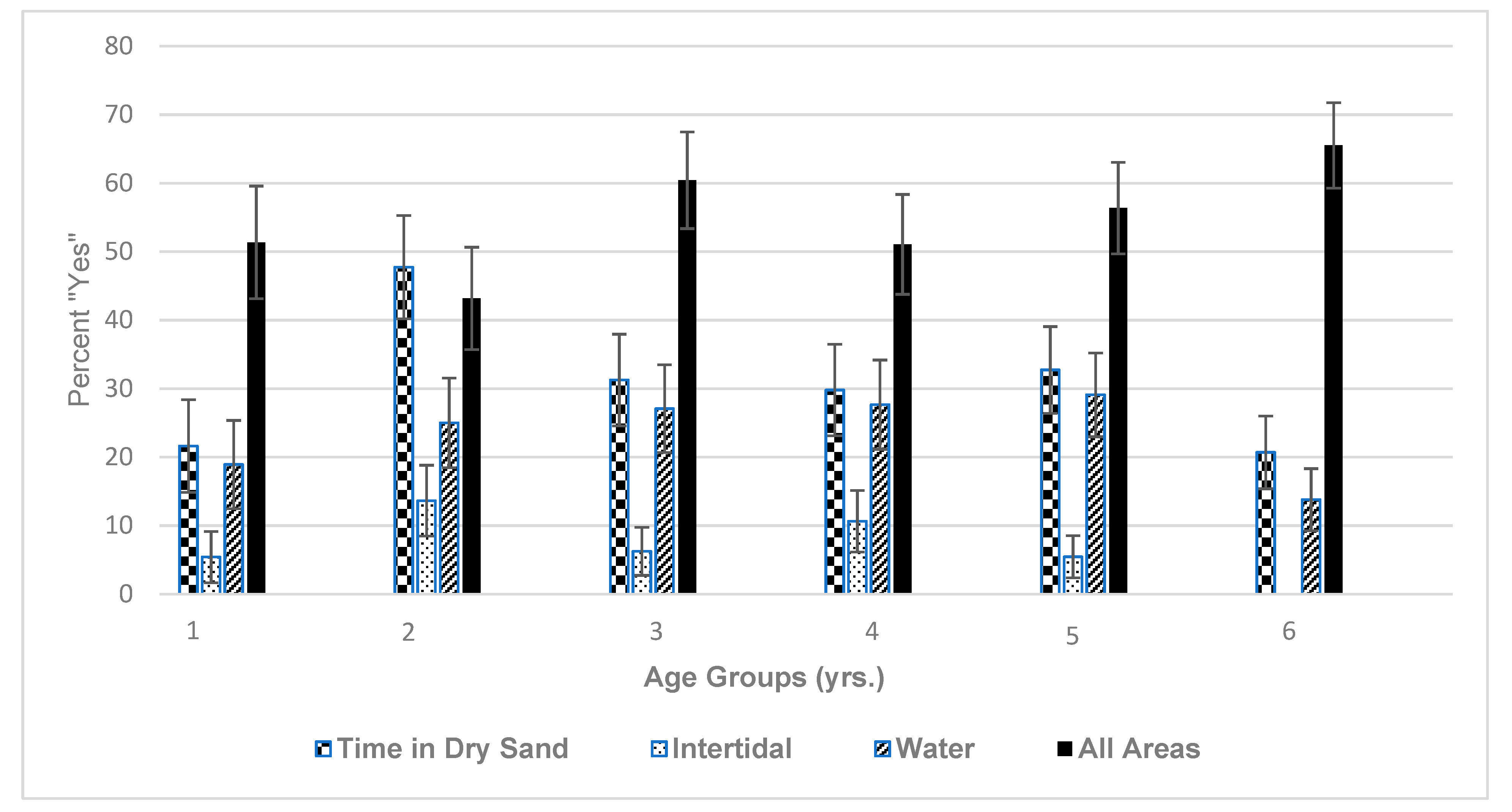
3.2.1. Exposure Subsection 1
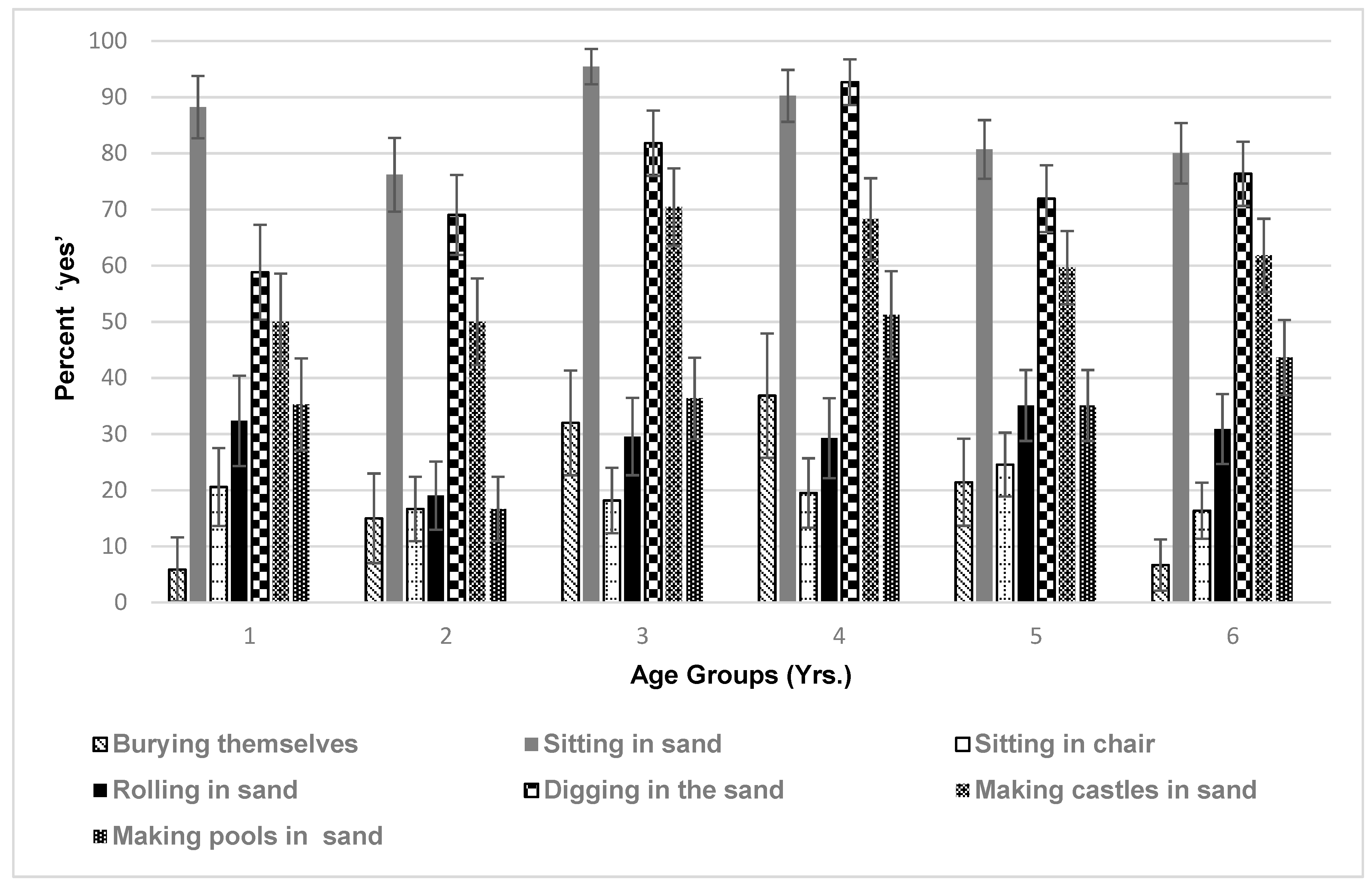
3.2.2. Exposure Subsection 2
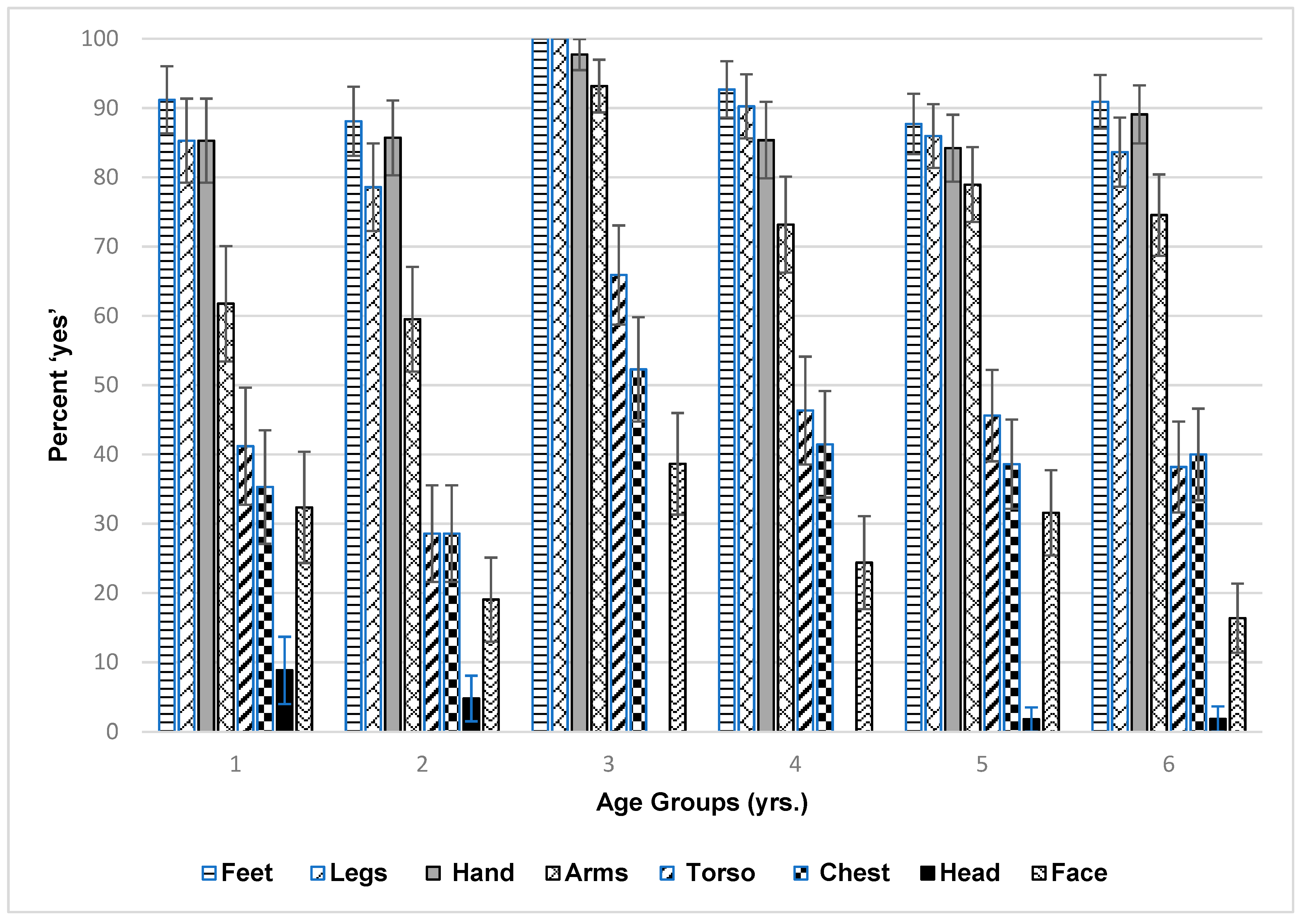
3.2.3. Exposure Subsection 3
3.3. Risk Perception Results
3.4. Key Comparison of Demographics, Exposure, and Risk Perceptions by Race
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Polson, J. BP Oil Still Ashore One Year after End of Gulf Spill. Bloomberg Business. 15 July 2011. Available online: http://www.bloomberg.com/news/articles/2011-07-15/bp-oil-still-washing-ashore-one-year-after-end-of-gulf-spill (accessed on 22 April 2019).
- Drofman, M.; Rosselot, K.S. Testing the Waters: A Guide to Water Quality at Vacation Beaches. Natural Resources Council. 2011. Available online: https://www.nrdc.org/sites/default/files/ttw2011.pdf (accessed on 18 May 2019).
- McGowan, C.J.; Kwok, R.K.; Engel, L.S.; Stenzel, M.R.; Stewart, P.A.; Sandler, D.P. Respiratory, dermal, and eye irritation symptoms associated with CorexitTM EC9527A/EC9500A following the Deepwater Horizon oil spill: Findings from the GuLF STUDY. Environ. Health Perspect. 2017, 125, 097015. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, M.A.; Reddy, G.K. Health consequences among subjects involved in Gulf Oil Spill clean-up activities. Am. J. Med. 2013, 126, 966–974. [Google Scholar] [CrossRef] [PubMed]
- Ashbullby, K.J.; Pahl, S.; Webley, P.; White, M.P. The beach as a setting for families’ health promotion: A qualitative study with parents and children living in coastal regions in Southwest England. Health Place 2013, 23, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Beamer, P.I.; Luik, C.E.; Canales, R.A.; Leckie, J.O. Quantified outdoor micro-activity data for children aged 7–12-years old. J. Expo. Sci. Environ. Epidemiol. 2012, 22, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Black, K.; Shalat, S.L.; Freeman, N.C.; Jimenez, M.; Donnelly, K.C.; Calvin, J.A. Children’s mouthing and food-handling behavior in an agricultural community on the US/Mexico border. J. Expo. Sci. Environ. Epidemiol. 2005, 15, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Freeman, N.C.; Hore, P.; Black, K.; Jimenez, M.; Sheldon, L.; Tulve, N.; Lioy, P.J. Contributions of children’s activities to pesticide hand loadings following residential pesticide application. J. Expo. Sci. Environ. Epidemiol. 2005, 15, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Freeman, N.C.; Jimenez, M.; Reed, K.J.; Gurunathan, S.; Edwards, R.D.; Roy, A.; Lioy, P.J. Quantitative analysis of children’s microactivity patterns: The Minnesota Children’s Pesticide Exposure Study. J. Expo. Sci. Environ. Epidemiol. 2001, 11, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Shalat, S.; Donnelly, K.; Freeman, N.; Calvin, J.; Ramesh, S.; Jimenez, M.; Black, K.; Coutinho, C.; Needham, L.; Barr, D.; et al. Nondietary ingestion of pesticides by children in an agricultural community on the US/Mexico border: Preliminary results. J. Expo. Sci. Environ. Epidemiol. 2003, 13, 42–50. [Google Scholar] [CrossRef] [Green Version]
- Shalat, S.L.; Solo-Gabriele, H.M.; Fleming, L.E.; Buckley, B.T.; Black, K.; Jimenez, M.; Shibata, T.; Durbin, M.; Graygo, J.; Stephan, W.; et al. A Pilot Study of Children’s Exposure to CCA-Treated Wood from Playground Equipment. Sci. Total Environ. 2006, 367, 80–88. [Google Scholar] [CrossRef]
- Xue, J.; Zartarian, V.; Tulve, N.; Moya, J.; Freeman, N.; Auyeung, W.; Beamer, P. A meta-analysis of children’s object-to-mouth frequency data for estimating non-dietary ingestion exposure. J. Expo. Sci. Environ. Epidemiol. 2010, 20, 536–545. [Google Scholar] [CrossRef]
- Shoaf, M.B.; Shirai, J.H.; Kedan, G.; Schaum, J.; Kissel, J.C. Child dermal sediment loads following play in a tide flat. J. Expo. Sci. Environ. Epidemiol. 2005, 15, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Chance, G.W.; Harmsen, E. Children are different: Environmental contaminants and children’s health. Can. J. Public Health 1998, 89 (Suppl. 1). S9-13, S10-5. [Google Scholar] [PubMed]
- Shah, A.H.; Abdelzaher, A.M.; Phillips, M.; Hernandez, R.; Solo-Gabriele, H.M.; Kish, J.; Fleming, L.E. Indicator microbes correlate with pathogenic bacteria, yeasts and helminthes in sand at a subtropical recreational beach site. J. Appl. Microbiol. 2011, 110, 1571–1583. [Google Scholar] [CrossRef] [PubMed]
- Wright, M.E.; Abdelzaher, A.M.; Solo-Gabriele, H.M.; Elmir, S.; Fleming, L.E. The inter-tidal zone is the pathway of input of enterococci to a subtropical recreational marine beach. Water Sci. Technol. 2011, 63, 542–549. [Google Scholar] [CrossRef]
- Heaney, C.; Sams, E.; Dufour, A.; Brenner, K.; Haugland, R.; Chern, E.; Wing, S.; Marshall, S.; Love, D.; Serre, M.; et al. Fecal indicators in sand, sand contact, and risk of enteric illness among beachgoers. Epidemiology 2012, 23, 95–106. [Google Scholar] [CrossRef] [PubMed]
- Heaney, C.; Sams, E.; Wing, S.; Marshall, S.; Brenner, K.; Dufour, A.P.; Wade, T. Contact with beach sand among beachgoers and risk of illness. Am. J. Epidemiol. 2009, 170, 164–172. [Google Scholar] [CrossRef]
- van Polanen Petel, T.; Bunce, A. Understanding beach users’ behavior, awareness, and attitudes to shorebird conservation in central Queensland: Tools for effective shorebird conservation. Coast. Manag. 2012, 50, 501–509. [Google Scholar] [CrossRef]
- de Freitas, C.R. Weather and place-based human behavior: Recreational preferences and sensitivity. Int. J. Biometeorol. 2015, 50, 55–63. [Google Scholar] [CrossRef]
- Ibarra, E.M. The use of webcam images to determine tourist–climate aptitude: Favorable weather types for sun and beach tourism on the Alicante coast (Spain). Int. J. Biometeorol. 2011, 55, 373–385. [Google Scholar] [CrossRef]
- Dwight, R.H.; Brinks, M.V.; SharavanaKumar, G.; Semenza, J.C. Beach attendance and bathing rates for Southern California beaches. Ocean Coast. Manag. 2007, 50, 847–858. [Google Scholar] [CrossRef]
- Christensen, J.; King, P. Summary Statistics from Beach Intercept Surveys Conducted in Southern California in Summer 2016. 2016. Available online: https://www.ioes.ucla.edu/wp-content/uploads/UCLA-Beach-Surveys-Summary-Statistics.pdf (accessed on 18 May 2019).
- Pendleton, L.; Martin, N.; Webster, D.G. Public perceptions of environmental quality: A survey study of beach use and perceptions in Los Angeles County. Mar. Pollut. Bull. 2001, 42, 1155–1160. [Google Scholar] [CrossRef]
- Vanderbilt. Research Electronic Data Capture (REDCap). 2019. Available online: https://projectredcap.org/about/ (accessed on 19 April 2019).
- National Oceanic and Atmospheric Administration (NOAA). What Is the Intertidal Zone. 2018. Available online: https://oceanservice.noaa.gov/facts/intertidal-zone.html (accessed on 18 May 2019).
- Centers for Disease Control and Prevention (CDC). How Can I Protect My Children from the Sun. 2018. Available online: https://www.cdc.gov/cancer/skin/basic_info/children.htm (accessed on 22 April 2019).
- Fleisher, J.M.; Fleming, L.E.; Solo-Gabriele, H.M.; Kish, J.K.; Sinigalliano, C.D.; Plano, L.R.W.; Elmir, S.M.; Wang, J.D.; Withum, K.; Shibata, T.; et al. The BEACHES study: Health effects and exposures from non-point source microbial contaminants in subtropical recreational marine waters. Int. J. Epidemiol. 2010, 39, 1291–1298. [Google Scholar] [CrossRef]
- Leonard, A.; Singer, A.; Ukoumunne, O.; Gaze, W.; Garside, R. Is it safe to go back into the water? A systematic review and meta-analysis of the risk of acquiring infections from the recreational exposure to seawater. Int. J. Epidemiol. 2018, 47, 572–585. [Google Scholar] [CrossRef] [PubMed]
- Colford, J.; Wade, T.; Schiff, K.; Wright, C.; Griffith, J.; Sandhu, S.; Burns, S.; Sobsey, M.; Lovelace, G.; Weisberg, S. Water quality indicators and the risk of illness at beaches with nonpoint sources of fecal contamination. Epidemiology 2007, 18, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Arnold, B.F.; Schiff, K.; Griffin, J.; Gruber, J.; Yau, V.; Wright, C.; Wade, T.; Burns, S.; Hayes, J.; McGee, C.; et al. Swimmer illness associated with marine water exposure and water quality indicators: Impact of widely used assumptions. Epidemiology 2013, 24, 845–853. [Google Scholar] [CrossRef] [PubMed]
- DeFlorio-Barker, S.; Arnold, B.; Sams, E.; Dufour, A.; Colford, J.; Weisburgy, S.; Schiff, K.; Wade, T. Child environmental exposure to water and sand at beach: Findings for studies of over 68,000 subjects at 12 beaches. J. Expo. Sci. Environ. Epidemiol. 2018, 28, 93–100. [Google Scholar] [CrossRef]
- Tresaugue, M. Oil Spills in Galveston Bay a Routine Occurrence. Houston Chronicle. 6 April 2014. Available online: https://www.houstonchronicle.com/news/science-environment/article/Oil-spills-in-Galveston-Bay-a-routine-occurrence-5381283.php (accessed on 22 April 2019).
- Bell, S.L.; Hollenbeck, J.; Lovell, R.; White, M.; Depledge, M.H. The shadows of risk and inequality within salutogenic coastal waters. In Blue Space, Health, and Wellbeing; Foley, R., Kearns, R., Kistemann, T., Wheeler, B., Eds.; Routledge, Taylor & Francis Group: London, UK, 2019; Chapter 10. [Google Scholar]
- United States Census Bureau. Quickfacts: United States. 2018. Available online: https://www.census.gov/quickfacts/fact/table/US/SEX255217 (accessed on 22 April 2019.
- Black, J.C.; Welday, J.N.; Buckley, B.; Ferguson, A.; Gurian, P.L.; Mena, K.D.; Yang, I.; McCandlish, E.; Solo-Gabriele, H.M. Risk assessment for children exposed to beach sands impacted by oil spill chemicals. Int. J. Environ. Res. Public Health 2016, 13, 853. [Google Scholar] [CrossRef] [PubMed]
- Shibata, T.; Solo-Gabriele, H.M. Quantitative microbial risk assessment of human illness from exposure to marine beach sand. Environ. Sci. Technol. 2012, 46, 2799–2805. [Google Scholar] [CrossRef]
- Whitman, R.L.; Przybyla-Kelly, K.; Shively, D.A.; Nevers, M.B.; Byappanahalli, M.N. Hand-mouth transfer and potential for exposure to E. coli and F+ coliphage in beach sand, Chicago, Illinois. J. Water Health 2009, 7, 623–629. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| % Yes | % No | % Sometimes | % Uncertain | NR a % | ||
| Stay longer at beach if bathroom available | 47.8 | 31.0 | 11.1 | 10.1 | 3.3 | |
| Children wash hands before eating | 56.5 | 23.2 | 12.5 | 1.8 | 21.3 | |
| Go to other places after the beach | 30 | 24.8 | 43.9 | 1.3 | 3.3 | |
| Use of shower to rinse yourself | 63.4 | 22.3 | 12.5 | 1.8 | 3.8 | |
| Use of shower to rinse children | 62.5 | 24.2 | 12.8 | 0.6 | 10.0 | |
| Use foot rinse for children | 68.1 | 20 | 10 | 1.9 | 10.0 | |
| Take soap to beach | 9.6 | 82.5 | 7.1 | 0.8 | 1.3 | |
| EveryHour | Couple Hours | BeforeMeals | Before Going Home | Never/Uncertain | ||
| How often is soap and water applied to children’s hands | 3.4 | 13.6 | 55.9 | 47.5 | 5.1/5.1 | 85.3 |
| How often is soap and water applied to your hands | 5.1 | 12.8 | 48.7 | 48.7 | 5.1/7.7 | 90.3 |
| Timing of children have a bath or shower upon arrival at home | Right away: 74.1% | Within 1 h: 15.8% | Within couple h: 6.5% | Later that night: 3.0% | Next day/uncertain: 0/0.5% | 0.5 |
| Mean Percent in Ranking # | NR a % | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Danger/ranking # | 10 | 9 | 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | |
| Infections | 39.7 | 6.1 | 7.4 | 4.7 | 4.7 | 8.1 | 3.0 | 6.4 | 5.7 | 14.1 | 25.8 |
| Shark attacks | 31.8 | 5.8 | 3.9 | 5.1 | 6.8 | 5.8 | 5.1 | 6.8 | 15.8 | 13.2 | 22.3 |
| Strong waves | 23.4 | 7.5 | 12.3 | 9.4 | 5.2 | 13 | 6.2 | 8.1 | 5.8 | 9.1 | 23.0 |
| Rip tides | 29.2 | 8.2 | 10.5 | 7.2 | 7.5 | 8.5 | 6.9 | 5.2 | 7.2 | 9.5 | 23.8 |
| Hurricanes or strong storms | 35.4 | 5.7 | 4.7 | 5.7 | 6.4 | 5.7 | 2.7 | 6.7 | 6.7 | 20.2 | 25.8 |
| Chemical or oil spill | 34.7 | 8.1 | 5.7 | 4.0 | 4.0 | 9.1 | 3.4 | 5.1 | 9.8 | 16.2 | 25.8 |
| Other | 35.7 | 7.1 | 0.0 | 7.1 | 0 | 21.4 | 7.1 | 7.1 | 0 | 14.3 | 96.5 |
| Characteristics | Overall (N = 359) | White (N = 271) | Black African American (N = 66) |
|---|---|---|---|
| Age | |||
| Mean (SE) | 37.95 (0.58) | 37.51 (0.71) | 39.81 (1.47) |
| Median (IQR) | 37 (30–44) | 36 (29–43) | 39 (32.5–41) |
| Sex | |||
| Male | 28.2% | 28.8% | 25.86% |
| Female | 71.8% | 71.2% | 74.14% |
| Income | |||
| Mean Range | 30,001–100,000 | 30,001–100,000 | 20,001–50,000 |
| Median Range | 50,001–100,000 | 30,001–100,000 | 30,001–50,000 |
| Hours Worked in Primary Job (SE) | 38.30 (0.78) | 37.96 (1.04) | 40.14 (1.58) |
| Mean Range Distance Live From Beach | 10–30 | 5–20 | 10–30 |
| Mean Range Frequency to Beach | Once a week–Once a month | Once a week–Once a month | Once a week–Once a month |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferguson, A.; Del Donno, C.; Obeng-Gyasi, E.; Mena, K.; Kaur Altomare, T.; Guerrero, R.; Gidley, M.; Montas, L.; Solo-Gabriele, H.M. Children Exposure-Related Behavior Patterns and Risk Perception Associated with Recreational Beach Use. Int. J. Environ. Res. Public Health 2019, 16, 2783. https://doi.org/10.3390/ijerph16152783
Ferguson A, Del Donno C, Obeng-Gyasi E, Mena K, Kaur Altomare T, Guerrero R, Gidley M, Montas L, Solo-Gabriele HM. Children Exposure-Related Behavior Patterns and Risk Perception Associated with Recreational Beach Use. International Journal of Environmental Research and Public Health. 2019; 16(15):2783. https://doi.org/10.3390/ijerph16152783
Chicago/Turabian StyleFerguson, Alesia, Courtney Del Donno, Emmanuel Obeng-Gyasi, Kristina Mena, Tanu Kaur Altomare, Rosalía Guerrero, Maribeth Gidley, Larissa Montas, and Helena M. Solo-Gabriele. 2019. "Children Exposure-Related Behavior Patterns and Risk Perception Associated with Recreational Beach Use" International Journal of Environmental Research and Public Health 16, no. 15: 2783. https://doi.org/10.3390/ijerph16152783
APA StyleFerguson, A., Del Donno, C., Obeng-Gyasi, E., Mena, K., Kaur Altomare, T., Guerrero, R., Gidley, M., Montas, L., & Solo-Gabriele, H. M. (2019). Children Exposure-Related Behavior Patterns and Risk Perception Associated with Recreational Beach Use. International Journal of Environmental Research and Public Health, 16(15), 2783. https://doi.org/10.3390/ijerph16152783