Patients’ and Caregivers’ Conceptualisations of Pressure Ulcers and the Process of Decision-Making in the Context of Home Care

 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Sample and Data Collection
2.3. Ethical Issues
2.4. Data Analysis
2.5. Validity
3. Results
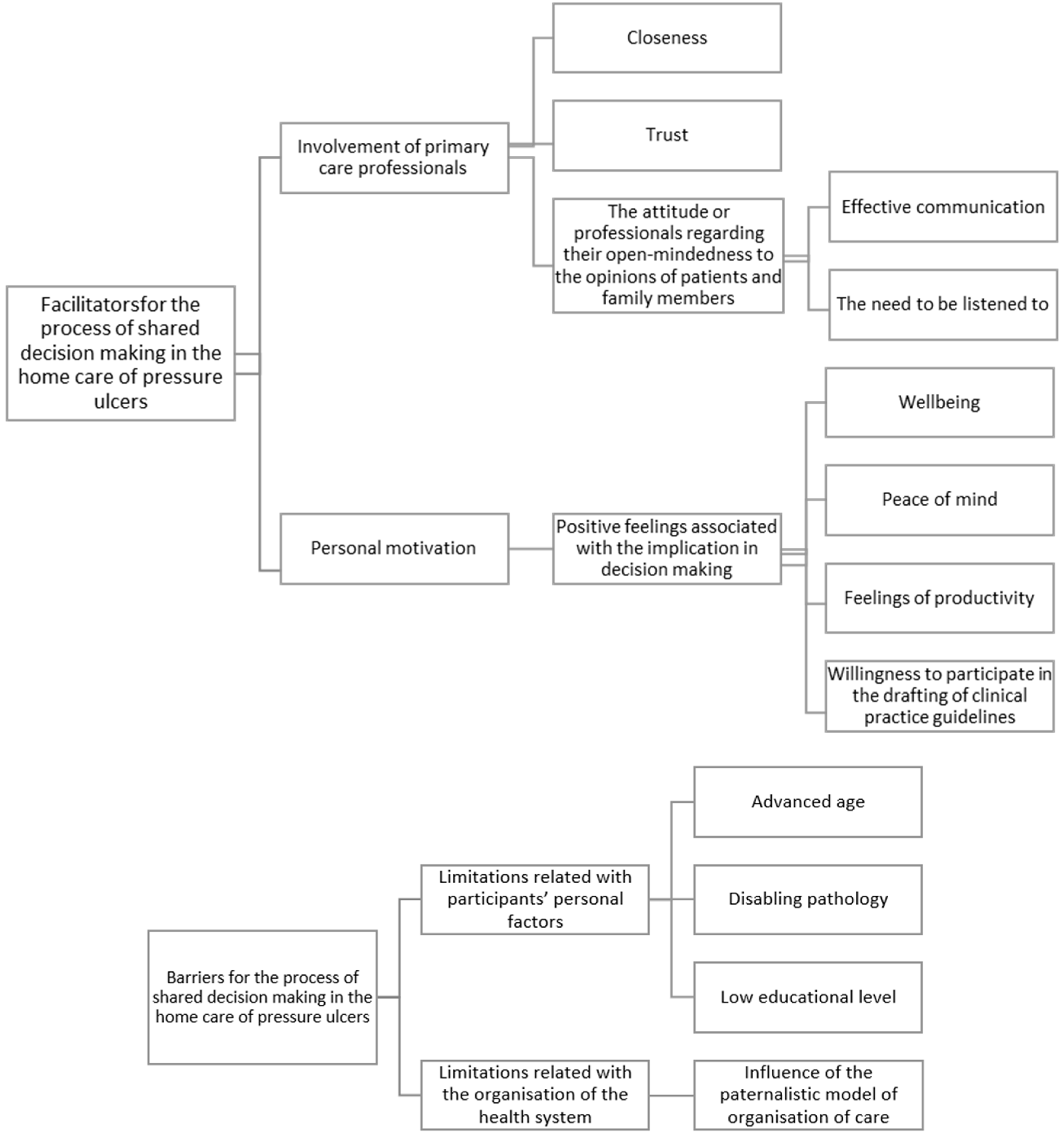
3.1. Facilitating Elements for the Process of Shared Decision Making in the Home Care of Pressure Ulcers
3.1.1. Involvement of Primary Care Professionals
3.1.2. Closeness and Trust
3.1.3. The Attitude of Professionals Regarding Their Open-Mindedness to the Opinions of Patients and Family Members
3.1.4. Personal Motivation
3.1.5. Positive Feelings Associated with Involvement in the Process of Decision Making
3.1.6. Wellbeing
3.1.7. Peace of Mind
3.1.8. Feelings of Productivity
3.1.9. Willingness to Participate in the Drafting of Clinical Practice Guidelines
3.2. Barriers for the Process of Shared Decision Making in the Home Care of People with Pressure Ulcers
3.2.1. Limitations Related to Participants’ Personal Factors
3.2.2. Advanced Age
3.2.3. Disabling Pathology
3.2.4. Low Educational Level
3.2.5. Influence of the Paternalistic Model of Organisation of Care
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Grimshaw, J.; Eccles, M.; Thomas, R.; MacLennan, G.; Ramsay, C.; Fraser, C.; Vale, L. Toward Evidence-Based Quality Improvement. J. Gen. Intern. Med. 2006, 21, S14–S20. [Google Scholar] [CrossRef] [PubMed]
- Satterfield, J.M.; Spring, B.; Brownson, R.C.; Mullen, E.J.; Newhouse, R.P.; Walker, B.B.; Whitlock, E.P. Toward a Transdisciplinary Model of Evidence-Based Practice. Milbank Q. 2009. [Google Scholar] [CrossRef] [PubMed]
- Légaré, F.; Adekpedjou, R.; Stacey, D.; Turcotte, S.; Kryworuchko, J.; Graham, I.D.; Lyddiatt, A.; Politi, M.C.; Thomson, R.; Elwyn, G.; et al. Interventions for increasing the use of shared decision making by healthcare professionals. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef] [PubMed]
- Stacey, D.; Légaré, F.; Lewis, K.; Barry, M.J.; Bennett, C.L.; Eden, K.B.; Holmes-Rovner, M.; Llewellyn-Thomas, H.; Lyddiatt, A.; Thomson, R.; et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [PubMed]
- Bastiaens, H.; Van Royen, P.; Pavlic, D.R.; Raposo, V.; Baker, R. Older people’s preferences for involvement in their own care: A qualitative study in primary health care in 11 European countries. Patient Educ. Couns. Elsevier 2007, 68, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Barry, M.J.; Edgman-Levitan, S. Shared Decision Making—The Pinnacle of Patient-Centered Care. N. Engl. J. Med. Mass. Med. Soc. 2012, 366, 780–781. [Google Scholar] [CrossRef] [PubMed]
- Florin, J.; Ehrenberg, A.; Ehnfors, M. Patient participation in clinical decision-making in nursing: A comparative study of nurses’ and patients’ perceptions. J. Clin. Nurs. 2006, 15, 1498–1508. [Google Scholar] [CrossRef] [PubMed]
- Committee on Quality of Health Care in America (Institute of Medicine). Crossing the Quality Chasm. In Crossing the Quality Chasm: A New Health System for the 21st Century; BMJ: London, UK, 2001; p. 323. [Google Scholar]
- Friesen-Storms, J.H.H.M.; Bours, G.J.J.W.; van der Weijden, T.; Beurskens, A.J.H.M. Shared decision making in chronic care in the context of evidence based practice in nursing. Int. J. Nurs. Stud. 2015, 52, 393–402. [Google Scholar] [CrossRef]
- Zoffmann, V.; Harder, I.; Kirkevold, M. A Person-Centered Communication and Reflection Model: Sharing Decision-Making in Chronic Care. Qual. Health Res. 2008, 18, 670–685. [Google Scholar] [CrossRef]
- Bodenheimer, T.; Lorig, K.; Holman, H.; Grumbach, K. Patient Self-management of Chronic Disease in Primary Care. JAMA Am. Med. Assoc. 2002, 288, 2469. [Google Scholar] [CrossRef]
- Clark, N.M.; Nelson, B.W.; Valerio, M.A.; Gong, Z.M.; Taylor-Fishwick, J.C.; Fletcher, M. Consideration of shared decision making in nursing: A review of clinicians’ perceptions and interventions. Open Nurs. J. 2009, 3, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Freund, T.; Gensichen, J.; Goetz, K.; Szecsenyi, J.; Mahler, C. Evaluating self-efficacy for managing chronic disease: Psychometric properties of the six-item Self-Efficacy Scale in Germany. J. Eval. Clin. Pract. 2013, 19, 39–43. [Google Scholar] [CrossRef] [PubMed]
- The Angiogenesis Foundation. Patient-Centered Outcomes in Wound Care; The Angiogenesis Foundation: Cambridge, MA, USA, 2013. [Google Scholar]
- Latimer, S.; Chaboyer, W. Patient participation in pressure injury prevention: Giving patient’s a voice. Scand. J. 2014, 28, 648–656. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.; Camosso-Stefinovic, J.; Gillies, C.; Shaw, E.J.; Cheater, F.; Flottorp, S.; Robertson, N.; Wensing, M.; Fiander, M.; Eccles, M.P.; et al. Tailored interventions to address determinants of practice. Cochrane Database Syst Rev. 2015, CD005470. [Google Scholar] [CrossRef]
- Fretheim, A.; Oxman, A.D.; Flottorp, S. Improving prescribing of antihypertensive and cholesterol-lowering drugs: A method for identifying and addressing barriers to change. BMC Health Serv. Res. 2004, 4, 23. [Google Scholar] [CrossRef]
- Perestelo-Pérez, L.; Salcedo-Fernández, F.; Toledo-Chávarri, A.; Álvarez-Pérez, Y.V.-E.M.; Abt-Sacks, A.; Trujillo, M.M.; del Pino, T.; Alonso-Coello, P.; Rivero-Santana, A.R.-M.B.; Cuéllar-Pompa, L.S.-A.P. Desarrollo de Herramientas de Ayuda Para la Toma de Decisiones Compartida Derivadas de las Recomendaciones de las Guías de Práctica Clínica; Ministerio de Sanidad, Servicios Sociales e Igualdad. Servicio de Evaluación del Servicio Canario de la Salud: Madrid, Spain, 2017.
- Roddis, J.K.; Liversedge, H.L.; Ryder, I.; Woodhouse, M. Incorporating the patient experience into clinical guidelines: Recommendations for researchers and guideline developers. BMJ Evid. Based Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Ptacek, S.; Dahlrup, B.; Edlund, A.-K.; Wijk, H.; Eriksdotter, M. The caregiving phenomenon and caregiver participation in dementia. Scand. J. Caring Sci. 2018. [Google Scholar] [CrossRef]
- García-Sánchez, F.J.; Martínez-Vizcaíno, V.; Rodríguez-Martín, B. Conceptualisations on home care for pressure ulcers in Spain: Perspectives of patients and their caregivers. Scand. J. Caring Sci. 2019. [Google Scholar] [CrossRef]
- Artico, M.; Dante, A.; D’angelo, D.; Lamarca, L.; Mastroianni, C.; Petitti, T.; Piredda, M.; De Marinis, M.G. Prevalence, incidence and associated factors of pressure ulcers in home palliative care patients: A retrospective chart review. Palliat. Med. 2018, 32, 299–307. [Google Scholar] [CrossRef]
- Beitz, J.M.; Goldberg, E. The Lived Experience of Having A Chronic Wound: A Phenomenologic Study. Medsurg Nurs. 2005, 14, 51–82. [Google Scholar]
- Spilsbury, K.; Nelson, A.; Cullum, N.; Iglesias, C.; Nixon, J.; Mason, S. Pressure ulcers and their treatment and effects on quality of life: Hospital inpatient perspectives. J. Adv. Nurs. 2007, 57, 494–504. [Google Scholar] [CrossRef] [PubMed]
- Caron, C.B.B. Method and application of dimensional analysis: A contribution to concept and Knowledge devolepment in nursing. In Concept Devolopment in Nursing: Foundations, Thecniques and Applications; Saunders, Ed.; Saunders: Philadelphia, PA, USA, 2000; pp. 285–320. [Google Scholar]
- Glaser, B.; Strauss, A. The Discovery of Grounded Theory; Aldine, Ed.; Aldine: Chicago, IL, USA, 1967. [Google Scholar]
- Strauss, A.L.; Corbin, J.M. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory; SAGE Publications, Ed.; SAGE Publications: London, UK, 1998. [Google Scholar]
- Pancorbo-Hidalgo, P.L.; García-Fernández, F.P.; Torra Bou, J.-E.; Verdú Soriano, J.; Javier Soldevilla-Agreda, J. Epidemiología de las úlceras por presión en España en 2013: 4.° Estudio Nacional de Prevalencia. Gerokomos 2014, 25, 162–170. [Google Scholar] [CrossRef]
- National Pressure Ulcer Advisory Panel EPUAP and PPPIA (NPUAP/EPUAP/PPPIA). Prevention and Treatment of Pressure Ulcers: Quick Reference Guide; Haesler, E., Ed.; Cambridge Media: Osborne Park, WA, Australian, 2014. [Google Scholar]
- Silverman, D. Interpreting Qualitative Data: Methods for Analyzing Talk, Text, and Interaction; Sage Publications: London, UK, 2006. [Google Scholar]
- Rodríguez-Martín, B.; Martínez-Andrés, M.; Cervera-Monteagudo, B.; Notario-Pacheco, B.; Martínez-Vizcaíno, V. Perception of quality of care among residents of public nursing-homes in Spain: A grounded theory study. BMC Geriatr. 2013, 13, 65. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Martín, B.; Martínez-Andrés, M.; Cervera-Monteagudo, B.; Notario-Pacheco, B.; Martínez-Vizcaíno, V. Preconceptions about institutionalisation at public nursing homes in Spain: Views of residents and family members. Ageing Soc. 2014, 34, 547–568. [Google Scholar] [CrossRef]
- Bernard, H.R.; Wutich, A.; Ryan, G.W. Analyzing Qualitative Data: Systematic Approaches; SAGE Publications: California, CA, USA, 2010. [Google Scholar]
- Jeon, Y.H. The application of grounded theory and symbolic interactionism. Scand. J. Caring Sci. 2004, 18, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Diaz del Campo, P.; Gracia, J.; Blasco, J.A.; Andradas, E. A strategy for patient involvement in clinical practice guidelines: Methodological approaches. BMJ Qual. Saf. 2011, 20, 779–784. [Google Scholar] [CrossRef] [PubMed]
- Kojima, M.; Nakayama, T.; Otani, T.; Hasegawa, M.; Kawahito, Y.; Kaneko, Y.; Kishimoto, M.; Hirata, S.; Seto, Y.; Endo, H.; et al. Integrating patients’ perceptions into clinical practice guidelines for the management of rheumatoid arthritis in Japan. Mod. Rheumatol. 2017, 27, 924–929. [Google Scholar] [CrossRef]
- Krahn, M.; Naglie, G. The Next Step in Guideline Development. JAMA 2008, 300, 436. [Google Scholar] [CrossRef]
- MacLean, S.; Mulla, S.; Akl, E.A.; Jankowski, M.; Vandvik, P.O.; Ebrahim, S.; McLeod, S.; Bhatnagar, N.; Guyatt, G.H. Patient Values and Preferences in Decision Making for Antithrombotic Therapy: A Systematic Review. Chest 2012, 141, e1S–e23S. [Google Scholar] [CrossRef]
- Sainio, C.; Lauri, S.; Eriksson, E. Cancer Patients’ Views and experiences of participation in care and decision making. Nurs. Ethics 2001, 8, 97–113. [Google Scholar] [CrossRef]
- Bae, J.-M. Shared decision making: Relevant concepts and facilitating strategies. Epidemiol. Health 2017. [Google Scholar] [CrossRef] [PubMed]
- Kiesler, D.J.; Auerbach, S.M. Optimal matches of patient preferences for information, decision-making and interpersonal behavior: Evidence, models and interventions. Patient Educ. Couns. 2006. [Google Scholar] [CrossRef] [PubMed]
- Guadagnoli, E.; Ward, P. Patient participation in decision-making. Soc. Sci. Med. 1998, 47, 329–339. [Google Scholar] [CrossRef]
- Chewning, B.; Bylund, C.L.; Shah, B.; Arora, N.K.; Gueguen, J.A.; Makoul, G. Patient preferences for shared decisions: A systematic review. Patient Educ. Couns. 2012. [Google Scholar] [CrossRef] [PubMed]
- Deber, R.B.; Kraetschmer, N.; Urowitz, S.; Sharpe, N. Do people want to be autonomous patients? Preferred roles in treatment decision-making in several patient populations. Health Expect. 2007, 10, 248–258. [Google Scholar] [CrossRef] [PubMed]
- Stella, F.; Forlenza, O.V.; Laks, J.; de Andrade, L.P.; de Castilho Cação, J.; Govone, J.S.; de Medeiros, K.; Lyketsos, C.G. Caregiver report versus clinician impression: Disagreements in rating neuropsychiatric symptoms in Alzheimer’s disease patients. Int. J. Geriatr. Psychiatr. 2015, 30, 1230–1237. [Google Scholar] [CrossRef]
- Andrén, S.; Elmståhl, S. The relationship between caregiver burden, caregivers’ perceived health and their sense of coherence in caring for elders with dementia. J. Clin. Nurs. 2008, 17, 790–799. [Google Scholar] [CrossRef] [PubMed]
- López, J.; López-Arrieta, J.; Crespo, M. Factors associated with the positive impact of caring for elderly and dependent relatives. Arch. Gerontol. Geriatr. 2005, 41, 81–94. [Google Scholar] [CrossRef]
- Mausbach, B.T.; Coon, D.W.; Depp, C.; Rabinowitz, Y.G.; Wilson-Arias, E.; Kraemer, H.C.; Thompson, L.W.; Lane, G.; Gallagher-Thompson, D. Ethnicity and Time to Institutionalization of Dementia Patients: A Comparison of Latina and Caucasian Female Family Caregivers. J. Am. Geriatr. Soc. 2004, 52, 1077–1084. [Google Scholar] [CrossRef]
- Fearns, N.; Kelly, J.; Callaghan, M.; Graham, K.; Loudon, K.; Harbour, R.; Santesso, N.; McFarlane, E.; Thornton, J.; Treweek, S. What do patients and the public know about clinical practice guidelines and what do they want from them? A qualitative study. BMC Health Serv. Res. 2016, 16, 74. [Google Scholar] [CrossRef]
- van der Weijden, T.; Boivin, A.; Burgers, J.; Schünemann, H.J.; Elwyn, G. Clinical practice guidelines and patient decision aids. An inevitable relationship. J. Clin. Epidemiol. 2012, 65, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Murray, L.M.; Laditka, S.B. Care transitions by older adults from nursing homes to hospitals: Implications for long-term care practice, geriatrics education, and research. J. Am. Med. Dir. Assoc. 2010, 231–238. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| P/CP | Sex | Age | Pressure Ulcer (PU) Category | Location of PU | Evolution of PU in Days |
|---|---|---|---|---|---|
| P1 | Female | 48 | 3 | Heel | 365 |
| P2 | Female | 60 | 2 | Sacrum | 180 |
| P3 | Male | 74 | 2 | Heel | 270 |
| P4 | Male | 93 | 2 | Toes | 90 |
| P5 | Male | 63 | 4 | Heel | 120 |
| P6 | Female | 88 | 2 | Sacrum | 180 |
| P7 | Female | 75 | 2 | Other | 120 |
| P8 | Female | 90 | 3 | Heel | 450 |
| P9 | Female | 81 | 2 | Sacrum | 90 |
| P10 | Male | 85 | 2 | Heel | 90 |
| CP1 | Female | 57 | 2 | Heel | 450 |
| CP2 | Female | 28 | 3 | Sacrum | 180 |
| CP3 | Female | 74 | 4 | Sacrum | 450 |
| CP4 | Female | 70 | 3 | Sacrum | 545 |
| CP5 | Female | 35 | 2 | Trochanter | 180 |
| CP6 | Female | 68 | 2 | Heel | 270 |
| CP7 | Female | 89 | 3 | Toes | 90 |
| CP8 | Female | 23 | 2 | Trochanter | 730 |
| CP9 | Female | 63 | 2 | Heel | 120 |
| CP10 | Male | 68 | 3 | Sacrum | 730 |
| CP11 | Male | 55 | 3 | Sacrum | 180 |
| CP12 | Female | 65 | 4 | Sacrum | 90 |
| CP13 | Male | 82 | 2 | Trocanter | 365 |
| CP14 | Male | 87 | 4 | Sacrum | 90 |
| CP15 | Male | 85 | 3 | Sacrum | 550 |
| Variables | Men | Women | |
|---|---|---|---|
| Age | 45–65 years | 1 | 2 |
| 66–85 years | 2 | 2 | |
| >86 years | 1 | 2 | |
| Civil status | Single | 1 | 0 |
| Married | 3 | 4 | |
| Widow | 0 | 2 | |
| Level of studies | Primary studies | 4 | 5 |
| University studies | 0 | 1 | |
| Pressure ulcer (PU) category according to the European Pressure Ulcer Advisory Panel (EPUAP) classification | 2 | 2 | 4 |
| 3 | 0 | 2 | |
| 4 | 2 | 0 | |
| Location of PU | Sacrum | 0 | 3 |
| Heels | 3 | 2 | |
| Toes | 1 | 0 | |
| Other sites | 0 | 1 | |
| Place where PU developed | Hospital | 1 | 3 |
| Home | 3 | 3 | |
| Evolution of PU in days | ≤90 days | 2 | 1 |
| 91–180 days | 1 | 3 | |
| 181–365 days | 1 | 1 | |
| >365 days | 0 | 1 | |
| Pain according to the numerical pain rating scale * | 7 | 1 | 2 |
| 8 | 1 | 2 | |
| 9 | 0 | 2 | |
| 10 | 2 | 0 | |
| Variables | Men | Women | |
|---|---|---|---|
| Age of caregivers | 25–45 years | 0 | 3 |
| 46–65 years | 1 | 3 | |
| 66–85 years | 4 | 3 | |
| >85 years | 0 | 1 | |
| Civil status of caregiver | Single | 1 | 3 |
| Married | 1 | 4 | |
| Widow | 3 | 3 | |
| Relationship with the patient | Spouse | 3 | 3 |
| Son/daughter | 2 | 4 | |
| Grandchild | 0 | 1 | |
| Sibling | 0 | 1 | |
| Neighbour | 0 | 1 | |
| Caregiver’s level of studies | Primary education | 5 | 7 |
| Secondary education | 0 | 1 | |
| University studies | 0 | 2 | |
| Caregiver’s work status | Unemployed | 1 | 1 |
| Housework | 0 | 2 | |
| Employed outside the home | 0 | 3 | |
| Retired | 4 | 4 | |
|
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Sánchez, F.J.; Martínez-Vizcaíno, V.; Rodríguez-Martín, B. Patients’ and Caregivers’ Conceptualisations of Pressure Ulcers and the Process of Decision-Making in the Context of Home Care. Int. J. Environ. Res. Public Health 2019, 16, 2719. https://doi.org/10.3390/ijerph16152719
García-Sánchez FJ, Martínez-Vizcaíno V, Rodríguez-Martín B. Patients’ and Caregivers’ Conceptualisations of Pressure Ulcers and the Process of Decision-Making in the Context of Home Care. International Journal of Environmental Research and Public Health. 2019; 16(15):2719. https://doi.org/10.3390/ijerph16152719
Chicago/Turabian StyleGarcía-Sánchez, Francisco José, Vicente Martínez-Vizcaíno, and Beatriz Rodríguez-Martín. 2019. "Patients’ and Caregivers’ Conceptualisations of Pressure Ulcers and the Process of Decision-Making in the Context of Home Care" International Journal of Environmental Research and Public Health 16, no. 15: 2719. https://doi.org/10.3390/ijerph16152719
APA StyleGarcía-Sánchez, F. J., Martínez-Vizcaíno, V., & Rodríguez-Martín, B. (2019). Patients’ and Caregivers’ Conceptualisations of Pressure Ulcers and the Process of Decision-Making in the Context of Home Care. International Journal of Environmental Research and Public Health, 16(15), 2719. https://doi.org/10.3390/ijerph16152719