Spatiotemporal Clustering of Middle East Respiratory Syndrome Coronavirus (MERS-CoV) Incidence in Saudi Arabia, 2012–2019

Abstract
:1. Introduction
2. Materials and Methods
2.1. MERS-CoV Data
2.2. Spatial Data
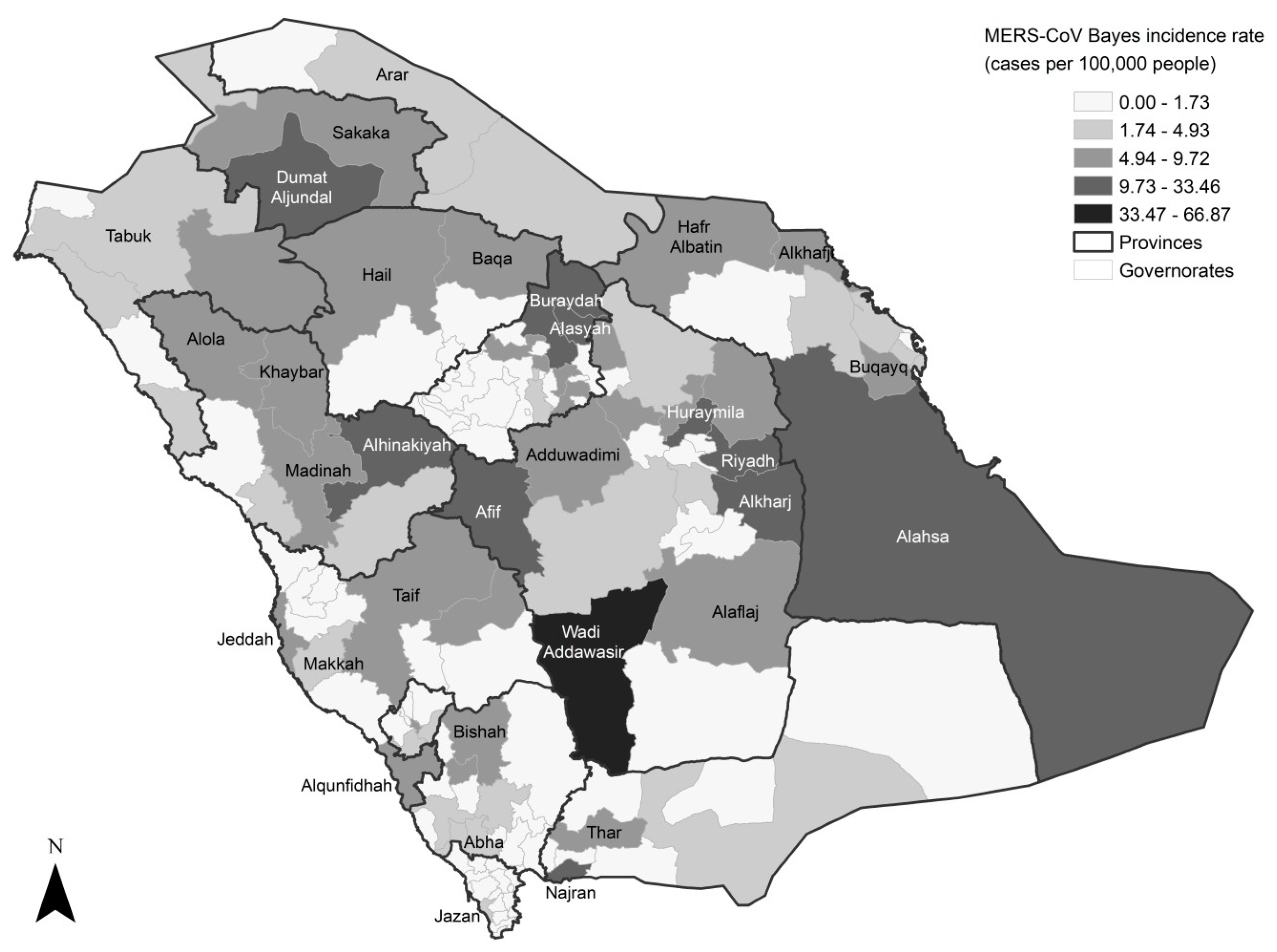
2.3. Empirical Bayes (EB) Smoothed Rate Maps
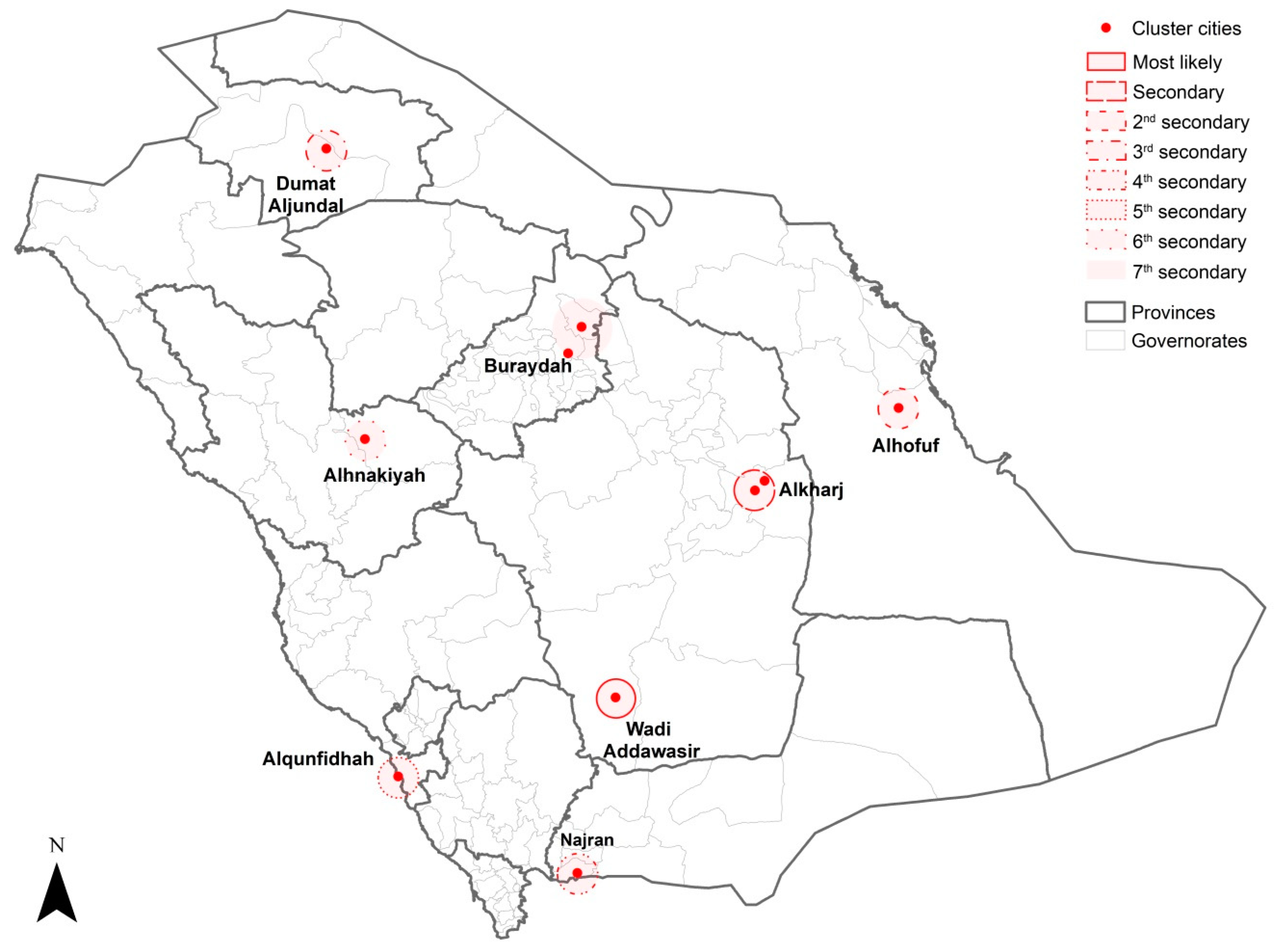
2.4. Spatial Cluster Analysis
3. Results
3.1. Overall
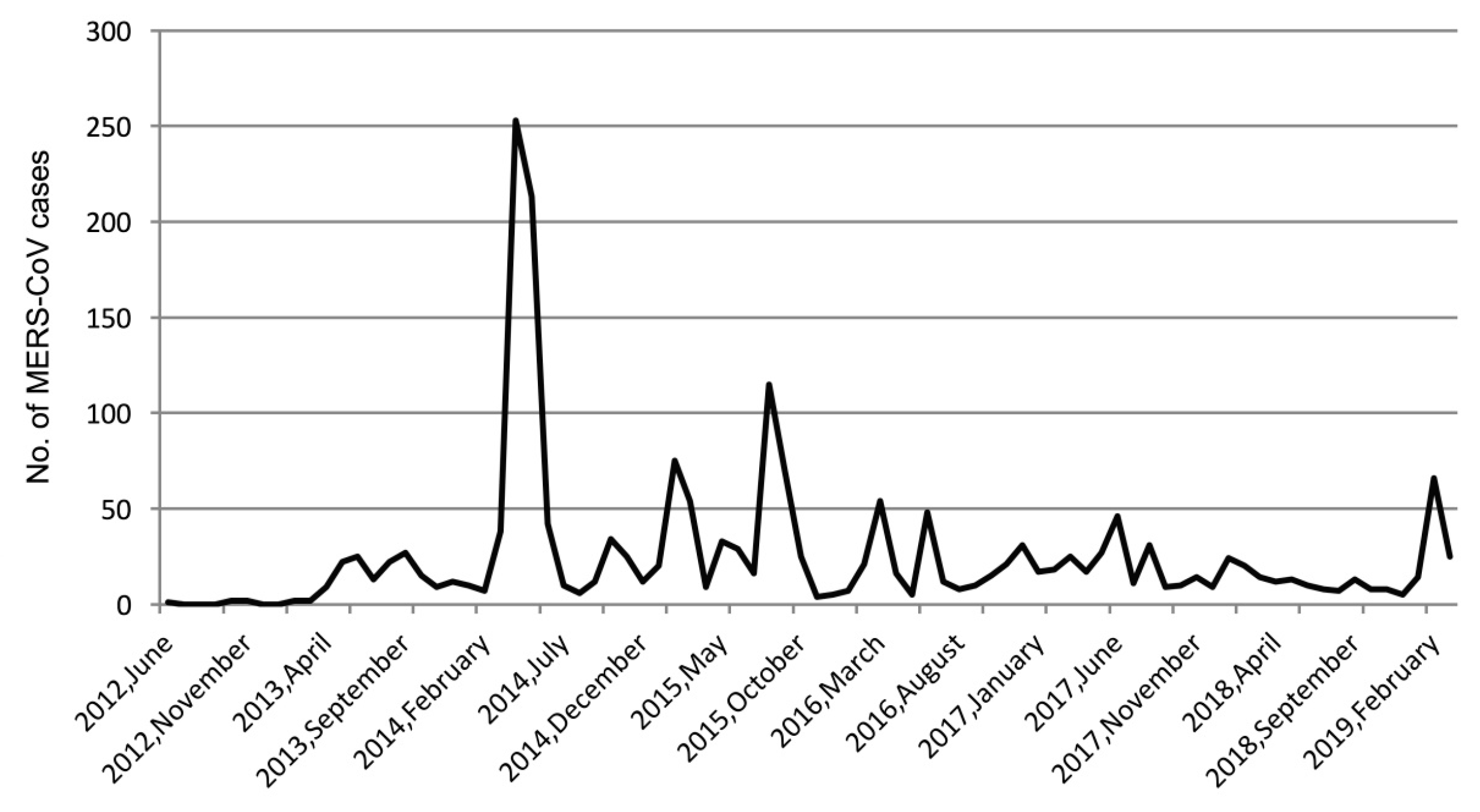
3.2. Temporal Trend of MERS-CoV Infection
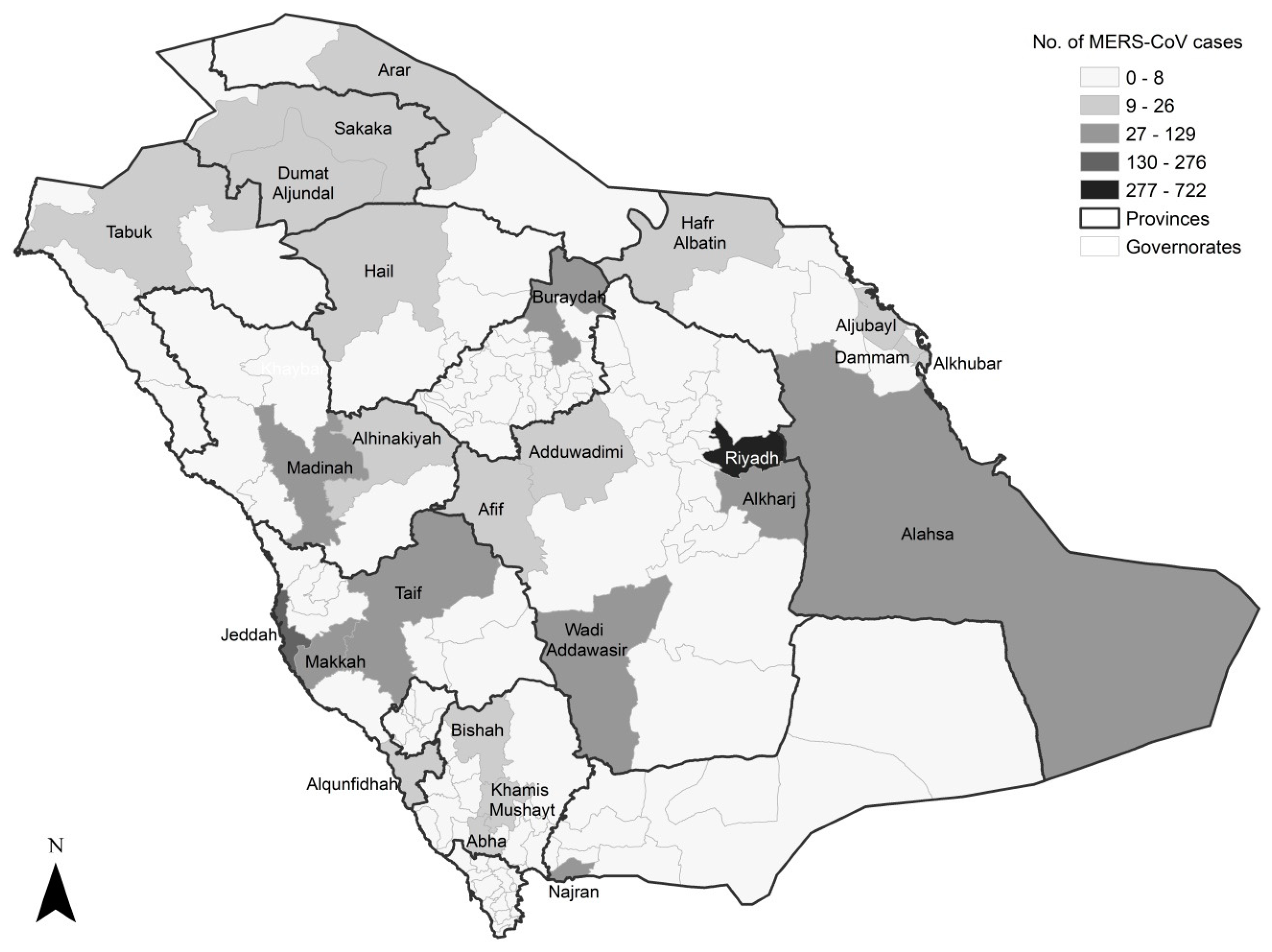
3.3. Spatial Pattern of MERS-CoV Infection
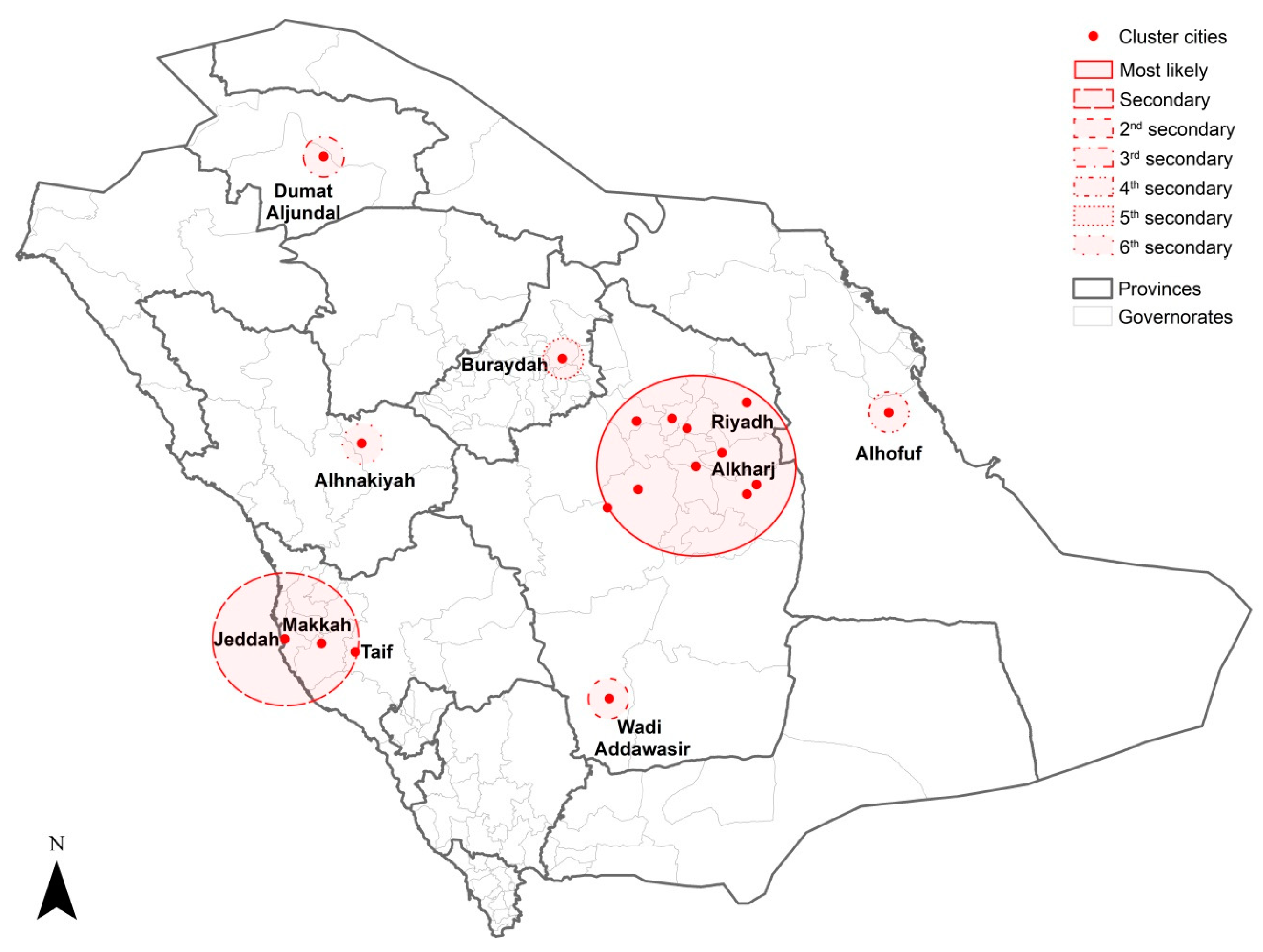
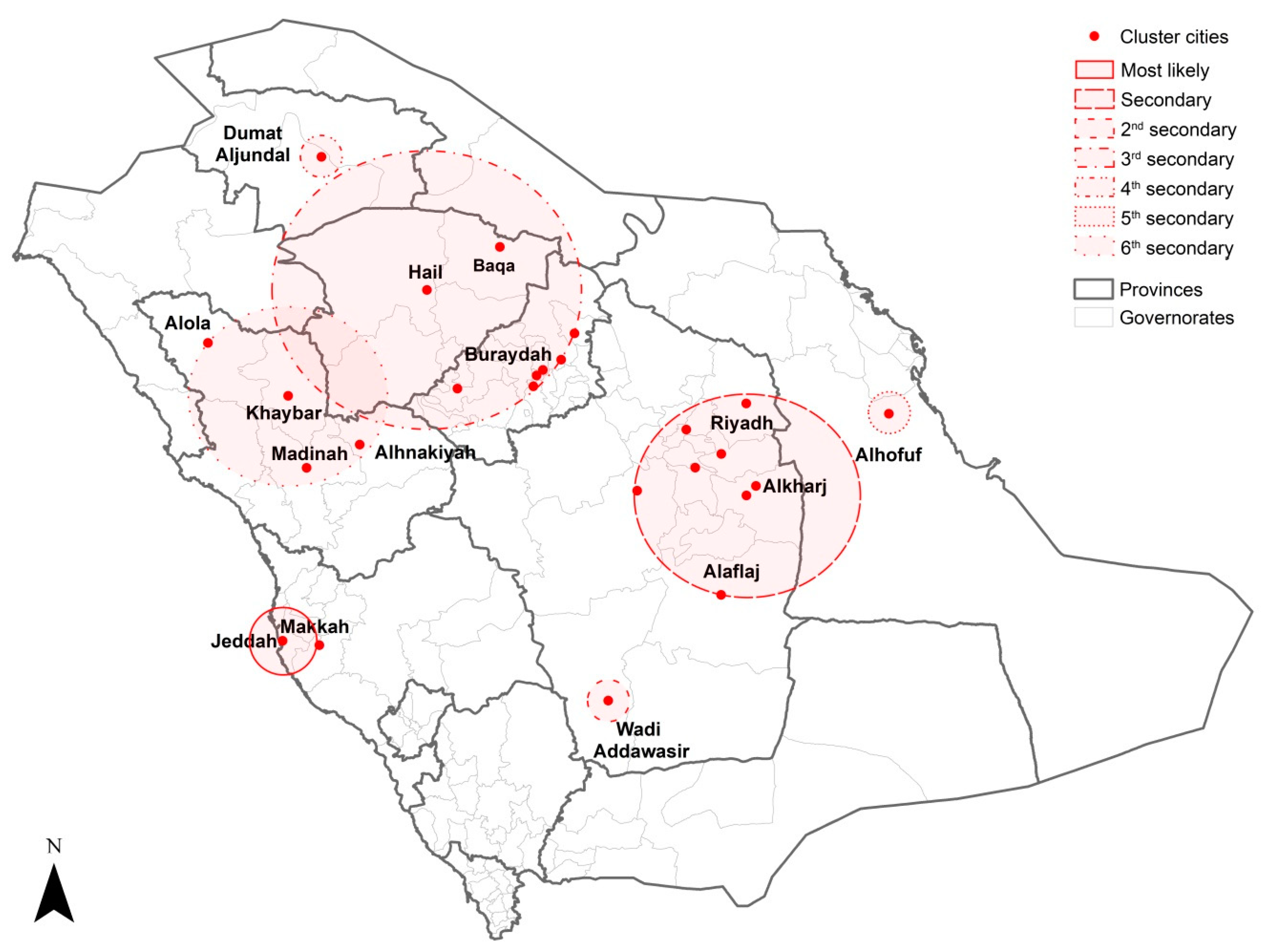
3.4. Spatiotemporal Clustering of MERS-CoV Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zaki, A.M.; van Boheemen, S.; Bestebroer, T.M.; Osterhaus, A.D.; Fouchier, R.A. Isolation of a novel Coronavirus from a man with pneumonia in Saudi Arabia. N. Engl. J. Med. 2012, 367, 1814–1820. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Emergencies: Middle East Respiratory Syndrome Coronavirus (MERS-CoV). Available online: https://www.who.int/emergencies/mers-cov/en/ (accessed on 27 April 2019).
- Azhar, E.I.; El-Kafrawy, S.A.; Farraj, S.A.; Hassan, A.M.; Al-Saeed, M.S.; Hashem, A.M.; Madani, T.A. Evidence for camel-to-human transmission of MERS Coronavirus. N. Engl. J. Med. 2014, 370, 2499–2505. [Google Scholar] [CrossRef] [PubMed]
- Memish, Z.A.; Cotten, M.; Watson, S.J.; Kellam, P.; Zumla, A.; Alhakeem, R.F.; Assiri, A.; Rabeeah, A.A.; Al-Tawfiq, J.A. Community case clusters of middle east respiratory syndrome Coronavirus in Hafr Al-Batin, Kingdom of Saudi Arabia: A descriptive genomic study. Int. J. Infect. Dis. 2014, 23, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Sikkema, R.S.; Farag, E.A.B.A.; Islam, M.; Atta, M.; Reusken, C.B.E.M.; Al-Hajri, M.M.; Koopmans, M.P.G. Global status of middle east respiratory syndrome Coronavirus in dromedary camels: A systematic review. Epidemiol. Infect. 2019, 147, e84. [Google Scholar] [CrossRef] [PubMed]
- Muller, M.A.; Meyer, B.; Corman, V.M.; Al-Masri, M.; Turkestani, A.; Ritz, D.; Sieberg, A.; Aldabbagh, S.; Bosch, B.J.; Lattwein, E.; et al. Presence of middle east respiratory syndrome Coronavirus antibodies in Saudi Arabia: A nationwide, cross-sectional, serological study. Lancet Infect. Dis. 2015, 15, 559–564. [Google Scholar] [CrossRef]
- Alshukairi, A.N.; Zheng, J.; Zhao, J.; Nehdi, A.; Baharoon, S.A.; Layqah, L.; Bokhari, A.; Al Johani, S.M.; Samman, N.; Boudjelal, M.; et al. High prevalence of MERS-CoV infection in Camel workers in Saudi Arabia. MBio 2018, 9, e01985-18. [Google Scholar] [CrossRef] [PubMed]
- Khudhair, A.; Killerby, M.E.; Al Mulla, M.; Abou Elkheir, K.; Ternanni, W.; Bandar, Z.; Weber, S.; Khoury, M.; Donnelly, G.; Al Muhairi, S.; et al. Risk factors for MERS-CoV seropositivity among animal market and slaughterhouse workers, Abu Dhabi, United Arab Emirates, 2014–2017. Emerg. Infect. Dis. 2019, 25, 927. [Google Scholar] [CrossRef] [PubMed]
- Kayali, G.; Peiris, M. A more detailed picture of the epidemiology of middle east respiratory syndrome Coronavirus. Lancet Infect. Dis. 2015, 15, 495–497. [Google Scholar] [CrossRef]
- FAO. Faostat. Available online: http://www.fao.org/faostat/en/#data (accessed on 19 June 2019).
- Faye, B. Camel meat in the world. In Camel Meat and Meat Products; Kadim, I., Maghoub, O., Faye, B., Farouk, M., Eds.; CABI: Oxfordshire, UK, 2013; pp. 7–16. [Google Scholar]
- Babiker, I.A. Peri-urban Camel (Camelus dromendarius) Production System in Saudi Arabia: A note. J. Anim. Res. 2014, 4, 53–57. [Google Scholar] [CrossRef]
- Ministry of Environment, Water, and Agriculture in Saudi Arabia. Available online: https://Www.Mewa.Gov.Sa/Ar/Pages/Default.Aspx (accessed on 19 June 2019).
- Saudi Press Agency. Numbering and Tracking Camels Electronically. Available online: https://www.spa.gov.sa/viewstory.php?lang=ar&newsid=1936043 (accessed on 19 June 2019).
- Drosten, C.; Meyer, B.; Müller, M.A.; Corman, V.M.; Al-Masri, M.; Hossain, R.; Madani, H.; Sieberg, A.; Bosch, B.J.; Lattwein, E.; et al. Transmission of MERS-Coronavirus in household contacts. N. Engl. J. Med. 2014, 371, 828–835. [Google Scholar] [CrossRef]
- Hui, D.S.; Azhar, E.I.; Kim, Y.J.; Memish, Z.A.; Oh, M.D.; Zumla, A. Middle east respiratory syndrome Coronavirus: Risk factors and determinants of primary, household, and nosocomial transmission. Lancet Infect. Dis. 2018, 18, e217–e227. [Google Scholar] [CrossRef]
- Assiri, A.; McGeer, A.; Perl, T.M.; Price, C.S.; Al Rabeeah, A.A.; Cummings, D.A.; Alabdullatif, Z.N.; Assad, M.; Almulhim, A.; Makhdoom, H.; et al. Hospital outbreak of middle east respiratory syndrome Coronavirus. N. Engl. J. Med. 2013, 369, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Memish, Z.A.; Al-Tawfiq, J.A.; Assiri, A. Hospital-associated middle east respiratory syndrome Coronavirus infections. N. Engl. J. Med. 2013, 369, 1761–1762. [Google Scholar] [CrossRef] [PubMed]
- Alenazi, T.H.; Al Arbash, H.; El-Saed, A.; Alshamrani, M.M.; Baffoe-Bonnie, H.; Arabi, Y.M.; Al Johani, S.M.; Hijazi, R.; Alothman, A.; Balkhy, H.H. Identified transmission dynamics of middle east respiratory syndrome Coronavirus infection during an outbreak: Implications of an overcrowded emergency department. Clin. Infect. Dis. 2017, 65, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Hastings, D.; Tokars, J.; Aziz, I.; Alkhaldi, K.; Bensadek, A.; Alraddadi, B.; Jokhdar, H.; Jernigan, J.A.; Garout, M.A. Outbreak of middle east respiratory syndrome at tertiary care hospital, Jeddah, Saudi Arabia, 2014. Emerg. Infect. Dis. 2016, 22, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Arwady, M.A.; Alraddadi, B.; Basler, C.; Azhar, E.I.; Abuelzein, E.; Sindy, A.I.; Sadiq, B.M.; Althaqafi, A.O.; Shabouni, O.; Banjar, A.; et al. Middle east respiratory syndrome Coronavirus transmission in extended family, Saudi Arabia, 2014. Emerg. Infect. Dis. 2016, 22, 1395–1402. [Google Scholar] [CrossRef]
- Aly, M.; Elrobh, M.; Alzayer, M.; Aljuhani, S.; Balkhy, H. Occurrence of the middle east respiratory syndrome Coronavirus (MERS-CoV) across the Gulf corporation council countries: Four years update. PLoS ONE 2017, 12, e0183850. [Google Scholar] [CrossRef]
- Alraddadi, B.M.; Watson, J.T.; Almarashi, A.; Abedi, G.R.; Turkistani, A.; Sadran, M.; Housa, A.; Almazroa, M.A.; Alraihan, N.; Banjar, A.; et al. Risk factors for primary middle east respiratory syndrome Coronavirus illness in humans, Saudi Arabia, 2014. Emerg. Infect. Dis. 2016, 22, 49–55. [Google Scholar] [CrossRef]
- Alqahtani, F.Y.; Aleanizy, F.S.; Ali El-Hadi Mohamed, R.; Alanazi, M.S.; Mohamed, N.; Alrasheed, M.M.; Abanmy, N.; Alhawassi, T. Prevalence of comorbidities in cases of middle east respiratory syndrome Coronavirus: A retrospective study. Epidemiol. Infect. 2018, 147, e35. [Google Scholar] [CrossRef]
- Congdon, P. Spatiotemporal frameworks for infectious disease diffusion and epidemiology. Int. J. Environ. Res. Public Health 2016, 13, 1261. [Google Scholar] [CrossRef]
- Cromley, E.K. GIS and disease. Annu. Rev. Public Health 2003, 24, 7–24. [Google Scholar] [CrossRef] [PubMed]
- Ruankaew, N. GIS and epidemiology. J. Med. Assoc. Thail. 2005, 88, 1735–1738. [Google Scholar]
- Smith, C.M.; Le Comber, S.C.; Fry, H.; Bull, M.; Leach, S.; Hayward, A.C. Spatial methods for infectious disease outbreak investigations: Systematic literature review. EuroSurveillance 2015, 20. [Google Scholar] [CrossRef] [PubMed]
- Reeves, T.; Samy, A.M.; Peterson, A.T. MERS-CoV geography and ecology in the middle east: Analyses of reported camel exposures and a preliminary risk map. BMC Res. Notes 2015, 8, 801. [Google Scholar] [CrossRef] [PubMed]
- Adegboye, O.A.; Gayawan, E.; Hanna, F. Spatial modelling of contribution of individual level risk factors for mortality from middle east respiratory syndrome Coronavirus in the Arabian Peninsula. PLoS ONE 2017, 12, e0181215. [Google Scholar] [CrossRef] [PubMed]
- Gikonyo, S.; Kimani, T.; Matere, J.; Kimutai, J.; Kiambi, S.G.; Bitek, A.O.; Ngeiywa, K.J.Z.J.; Makonnen, Y.J.; Tripodi, A.; Morzaria, S.; et al. Mapping potential amplification and transmission hotspots for MERS-CoV, Kenya. Ecohealth 2018, 15, 372–387. [Google Scholar] [CrossRef]
- Poletto, C.; Colizza, V.; Boelle, P.Y. Quantifying spatiotemporal heterogeneity of MERS-CoV transmission in the middle east region: A combined modelling approach. Epidemics 2016, 15, 1–9. [Google Scholar] [CrossRef]
- Ministry of Health in Saudi Arabia. Command and Control Center. Available online: https://www.moh.gov.sa/en/CCC/Pages/default.aspx (accessed on 30 April 2019).
- World Health Organization. Emergencies Preparedness, Response. Disease Outbreaks by Year. Available online: https://www.who.int/csr/don/archive/year/en/ (accessed on 30 April 2019).
- Ministry of Health in Saudi Arabia. Middle East Respiratory Syndrome Coronavirus; Guidelines for Healthcare Professionals. Version 5.1. Available online: https://www.moh.gov.sa/CCC/healthp/regulations/Documents/MERS-CoV%20Guidelines%20for%20Healthcare%20Professionals%20-%20May%202018%20-%20v5.1%20%281%29.pdf (accessed on 17 June 2019).
- Lawson, A.B. Bayesian Disease Mapping: Hierarchical Modeling in Spatial Epidemiology; CRC: Boca Raton, FL, USA, 2009. [Google Scholar]
- GeoDaTM v1.12. Software for Exploratory Spatial Data Analysis (ESDA). Available online: https://geodacenter.github.io/download.html (accessed on 28 September 2018).
- General Authority for Statistics Saudi Arabia. The General Population and Housing Census. Available online: https://www.stats.gov.sa/en/13 (accessed on 13 February 2018).
- SaTScanTM v9.6. Software for the Spatial and Space-Time Scan Statistics. Information Management Services. Available online: https://www.satscan.org/ (accessed on 5 January 2018).
- Kulldorff, M. SaTScanTM User Guide for Version 9.6. Available online: https://www.satscan.org/cgi-bin/satscan/register.pl/SaTScan_Users_Guide.pdf?todo=process_userguide_download (accessed on 25 March 2018).
- Faye, B.; Bonnet, P. Camel sciences and economy in the world: Current situation and perspectives. In Proceedings of the 3rd ISOCARD Conference, 29 January–1 February 2012; Johnson, E., Mahgoub, O., Eljack, A., Kadim, I., Bobade, P., Tageldin, M., Al-Marzooqi, W., Ahmed, Y., Eds.; Sultan Qaboos University: Mascate, Oman, 2012; pp. 2–15. [Google Scholar]
- Gaili, E.S.E.; Al-Eknah, M.; Mansour, H. Systems of camel management in Saudi Arabia. Arab J. Agric. Res. 2000, 116, 148–156. [Google Scholar]
- Almutairi, S.E.; Boujenane, I.; Musaad, A.; Awad-Acharari, F. Genetic and nongenetic effects for milk yield and growth traits in Saudi camels. Trop. Anim. Health Prod. 2010, 42, 1845–1853. [Google Scholar] [CrossRef]
- Khalafalla, A.I.; Lu, X.; Al-Mubarak, A.I.A.; Dalab, A.H.S.; Al-Busadah, K.A.S.; Erdman, D.D. MERS-CoV in upper respiratory tract and lungs of dromedary camels, Saudi Arabia, 2013–2014. Emerg. Infect. Dis. 2015, 21, 1153–1158. [Google Scholar] [CrossRef]
- Chen, X.; Chughtai, A.A.; Dyda, A.; MacIntyre, C.R. Comparative epidemiology of middle east respiratory syndrome Coronavirus (MERS-CoV) in Saudi Arabia and South Korea. Emerg. Microbes Infect. 2017, 6, e51. [Google Scholar] [CrossRef] [PubMed]
- Eifan, S.A.; Nour, I.; Hanif, A.; Zamzam, A.M.M.; AlJohani, S.M. A pandemic risk assessment of middle east respiratory syndrome Coronavirus (MERS-CoV) in Saudi Arabia. Saudi J. Biol. Sci. 2017, 24, 1631–1638. [Google Scholar] [CrossRef] [PubMed]
- Nassar, M.S.; Bakhrebah, M.A.; Meo, S.A.; Alsuabeyl, M.S.; Zaher, W.A. Global seasonal occurrence of middle east respiratory syndrome Coronavirus (MERS-CoV) infection. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 3913–3918. [Google Scholar] [CrossRef] [PubMed]
- Sharif-Yakan, A.; Kanj, S.S. Emergence of MERS-CoV in the middle east: Origins, transmission, treatment, and perspectives. PLoS Pathog. 2014, 10, e1004457. [Google Scholar] [CrossRef] [PubMed]
- Zumla, A.; Hui, D.S. Infection control and MERS-CoV in health-care workers. Lancet 2014, 383, 1869–1871. [Google Scholar] [CrossRef] [Green Version]
- Kasem, S.; Qasim, I.; Al-Doweriej, A.; Hashim, O.; Alkarar, A.; Abu-Obeida, A.; Saleh, M.; Al-Hofufi, A.; Al-Ghadier, H.; Hussien, R.; et al. The prevalence of middle east respiratory syndrome Coronavirus (MERS-CoV) infection in livestock and temporal relation to locations and seasons. J. Infect. Public Health 2018, 11, 884–888. [Google Scholar] [CrossRef] [PubMed]
- Breban, R.; Riou, J.; Fontanet, A. Interhuman transmissibility of middle east respiratory syndrome Coronavirus: Estimation of pandemic risk. Lancet 2013, 382, 694–699. [Google Scholar] [CrossRef]
- He, D.; Chiu, A.P.; Lin, Q.; Cowling, B.J. Differences in the seasonality of middle east respiratory syndrome Coronavirus and influenza in the middle east. Int. J. Infect. Dis. 2015, 40, 15–16. [Google Scholar] [CrossRef]
- Al-Tawfiq, J.A.; Benkouiten, S.; Memish, Z.A. A systematic review of emerging respiratory viruses at the Hajj and possible coinfection with Streptococcus pneumoniae. Travel Med. Infect. Dis. 2018, 23, 6–13. [Google Scholar] [CrossRef]
- Assiri, A.M.; Biggs, H.M.; Abedi, G.R.; Lu, X.; Saeed, A.B.; Abdalla, O.; Mohammed, M.; Al-Abdely, H.M.; Algarni, H.S.; Alhakeem, R.F.; et al. Increase in middle east respiratory syndrome-Coronavirus cases in Saudi Arabia linked to hospital outbreak with continued circulation of recombinant virus, 1 July–31 August 2015. Open Forum Infect. Dis. 2016, 3, ofw165. [Google Scholar] [CrossRef]
- World Health Organization. Emergencies Preparedness, Response: Disease Outbreak News: Middle East Respiratory Syndrome Coronavirus (MERS-CoV)—The Kingdom of Saudi Arabia. Available online: https://www.who.int/csr/don/24-April-2019-mers-saudi-arabia/en/ (accessed on 24 April 2019).
- Ministry of Health Saudi Arabia. Weekly Monitor, MERS-CoV; 15 March 2016. Available online: https://www.moh.gov.sa/en/CCC/Documents/Volume-2-Issue-11-Tuesday-March-15-2016.pdf (accessed on 20 April 2018).
- World Health Organization. WHO MERS-CoV Global Summary and Assessment of Risk. Available online: https://www.who.int/csr/disease/coronavirus_infections/risk-assessment-august-2018.pdf?ua=1 (accessed on 25 August 2018).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Timeframe | Observed Cases | Expected Cases | LLR | Relative Risk | p-Value |
|---|---|---|---|---|---|
| 2014 to 2016 | 1364 | 592 | 320 | 3.12 | 0.001 |
| April 2014 to May 2014 | 466 | 49 | 677 | 11.98 | 0.001 |
| April 5, 2014 to May 24, 2014 | 446 | 41 | 709 | 13.87 | 0.001 |
| April to May | 629 | 296 | 161 | 2.54 | 0.001 |
| Cluster Type | No. of Cities in the Cluster | Observed Cases | Expected Cases | LLR | Relative Risk | p-Value |
|---|---|---|---|---|---|---|
| Most likely | 1 | 81 | 9 | 104 | 8.92 | <0.001 |
| Secondary | 2 | 70 | 15 | 55 | 4.92 | <0.001 |
| Second secondary | 1 | 128 | 67 | 23 | 1.97 | <0.001 |
| Third secondary | 1 | 21 | 3 | 21 | 6.42 | <0.001 |
| Fourth secondary | 1 | 68 | 30 | 18 | 2.30 | <0.001 |
| Fifth secondary | 1 | 14 | 2 | 13 | 5.67 | <0.001 |
| Sixth secondary | 1 | 11 | 2 | 11 | 6.52 | <0.001 |
| Seventh secondary | 2 | 85 | 50 | 10 | 1.73 | <0.001 |
| Cluster Type | Timeframe (year) | No. of Cities in the Cluster | Observed Cases | Expected Cases | LLR | Relative Risk | p-Value |
|---|---|---|---|---|---|---|---|
| Most likely | 2014 to 2016 | 10 | 491 | 163 | 245 | 3.67 | <0.001 |
| Secondary | 2014 to 2015 | 3 | 315 | 84 | 201 | 4.28 | <0.001 |
| Second secondary | 2018 to 2019 | 1 | 56 | 1 | 153 | 41.57 | <0.001 |
| Third secondary | 2017 to 2018 | 1 | 21 | 0 | 59 | 43.70 | <0.001 |
| Fourth secondary | 2015 to 2016 | 1 | 50 | 10 | 41 | 5.17 | <0.001 |
| Fifth secondary | 2015 to 2016 | 1 | 33 | 7 | 25 | 4.79 | <0.001 |
| Sixth secondary | 2014 to 2015 | 1 | 9 | 0 | 23 | 36.28 | <0.001 |
| Cluster Type | Timeframe (month/year) | No. of Cities in the Cluster | Observed Cases | Expected Cases | LLR | Relative Risk | p-Value |
|---|---|---|---|---|---|---|---|
| Most likely | 04/2014 to 05/2015 | 2 | 252 | 13 | 532 | 22.83 | <0.001 |
| Secondary | 03/2014 to 10/2015 | 8 | 500 | 135 | 326 | 4.58 | <0.001 |
| Second secondary | 02/2019 | 1 | 47 | 0 | 240 | 452.96 | <0.001 |
| Third secondary | 03/2016 | 8 | 39 | 1 | 98 | 32.90 | <0.001 |
| Fourth secondary | 08/2017 | 1 | 19 | 0 | 98 | 465.20 | <0.001 |
| Fifth secondary | 05/2015 to 06/2015 | 1 | 38 | 2 | 83 | 23.54 | <0.001 |
| Sixth secondary | 04/2014 to 06/2014 | 4 | 38 | 4 | 49 | 8.94 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Ahmadi, K.; Alahmadi, S.; Al-Zahrani, A. Spatiotemporal Clustering of Middle East Respiratory Syndrome Coronavirus (MERS-CoV) Incidence in Saudi Arabia, 2012–2019. Int. J. Environ. Res. Public Health 2019, 16, 2520. https://doi.org/10.3390/ijerph16142520
Al-Ahmadi K, Alahmadi S, Al-Zahrani A. Spatiotemporal Clustering of Middle East Respiratory Syndrome Coronavirus (MERS-CoV) Incidence in Saudi Arabia, 2012–2019. International Journal of Environmental Research and Public Health. 2019; 16(14):2520. https://doi.org/10.3390/ijerph16142520
Chicago/Turabian StyleAl-Ahmadi, Khalid, Sabah Alahmadi, and Ali Al-Zahrani. 2019. "Spatiotemporal Clustering of Middle East Respiratory Syndrome Coronavirus (MERS-CoV) Incidence in Saudi Arabia, 2012–2019" International Journal of Environmental Research and Public Health 16, no. 14: 2520. https://doi.org/10.3390/ijerph16142520