National Evaluation of Canadian Multi-Service FASD Prevention Programs: Interim Findings from the Co-Creating Evidence Study

Abstract
:1. Introduction
1.1. Emergence and Evaluation of FASD Prevention Programs
- Experience better and earlier access to prenatal care
- Reduce their substance use
- Improve their health and wellness outcomes and those of their children
- Retain and/or regain custody of their children
- Develop new social/support networks and friendships
- Acquire parenting skills
1.2. Co-Creating Evidence Evaluation Study
- What are common elements of these diverse, multi-service programs?
- How do the programs reflect their community’s context?
- What program components are most helpful from women’s perspectives?
- What are the programs’ impacts and outcomes for clients and their children?
2. Methodology and Materials
2.1. Study Design
2.2. Data Collection Processes and Instruments
2.3. On-Site Data Collection by Program Team
2.4. Participants and Sampling Approach
- 125 program participants/clients (of whom 123 completed the Questionnaire for Clients);
- 61 program staff; and
- 42 service partners
2.5. Data Analysis
2.6. Methodological Limitations
3. Results
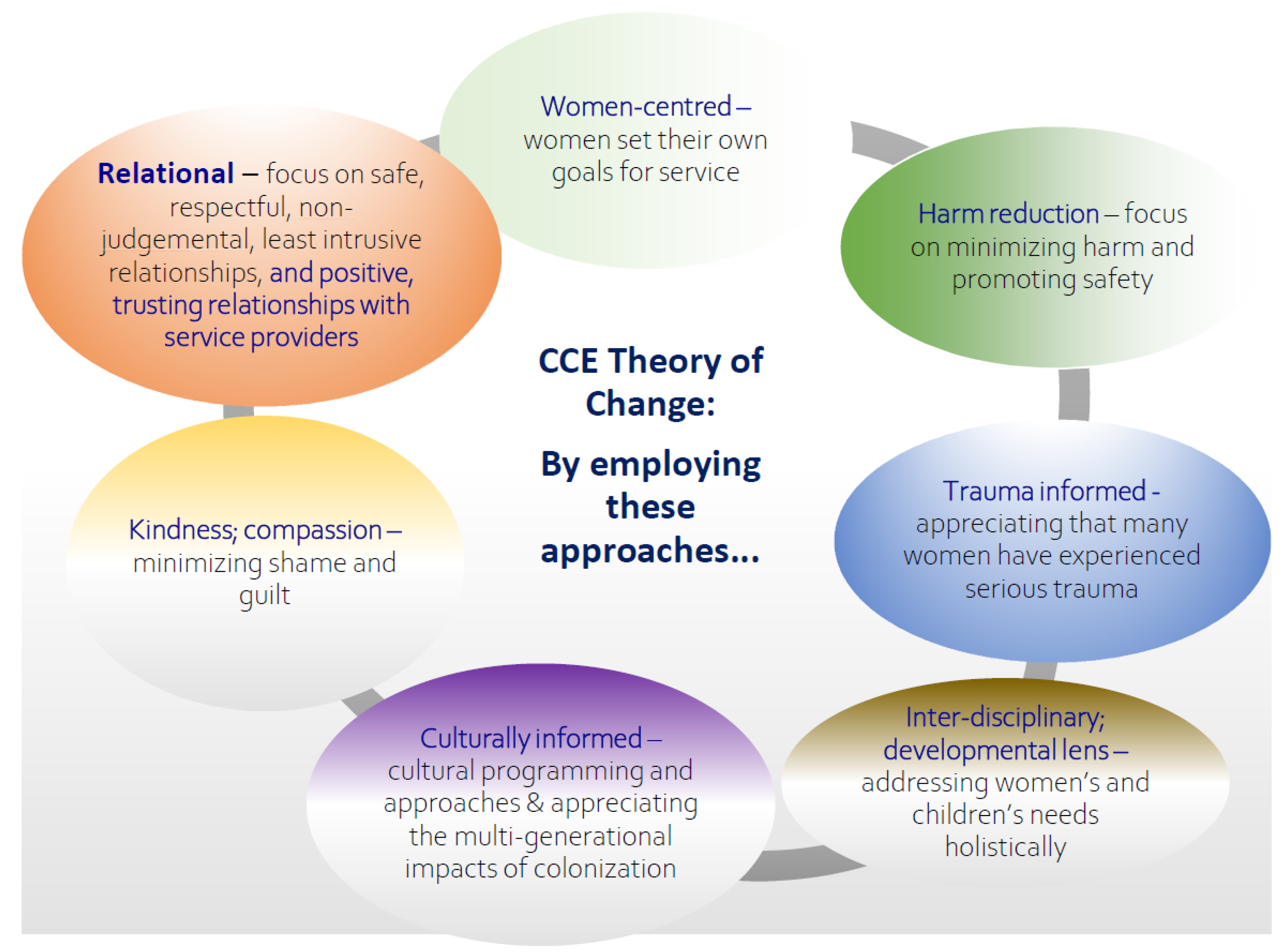
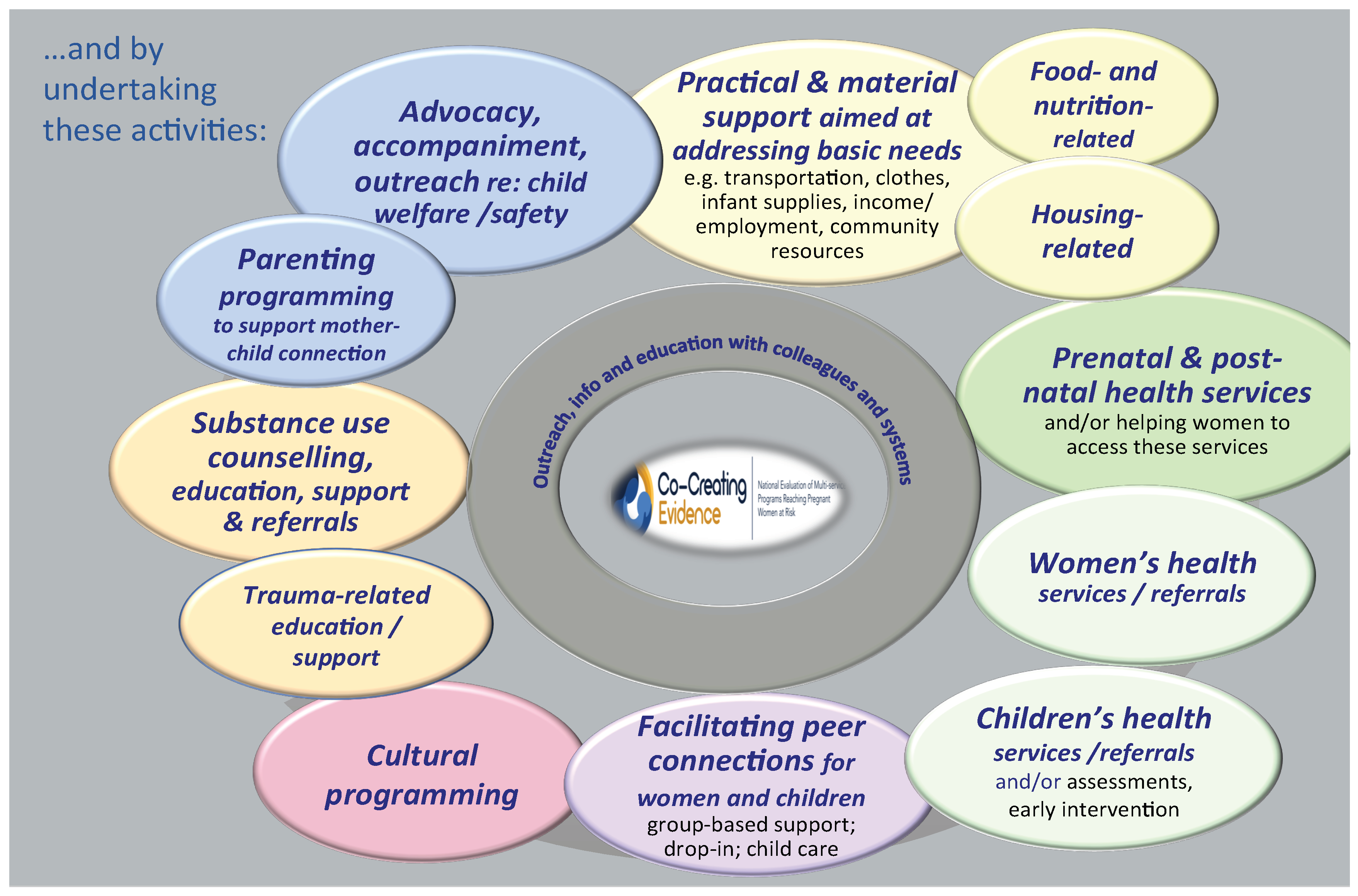
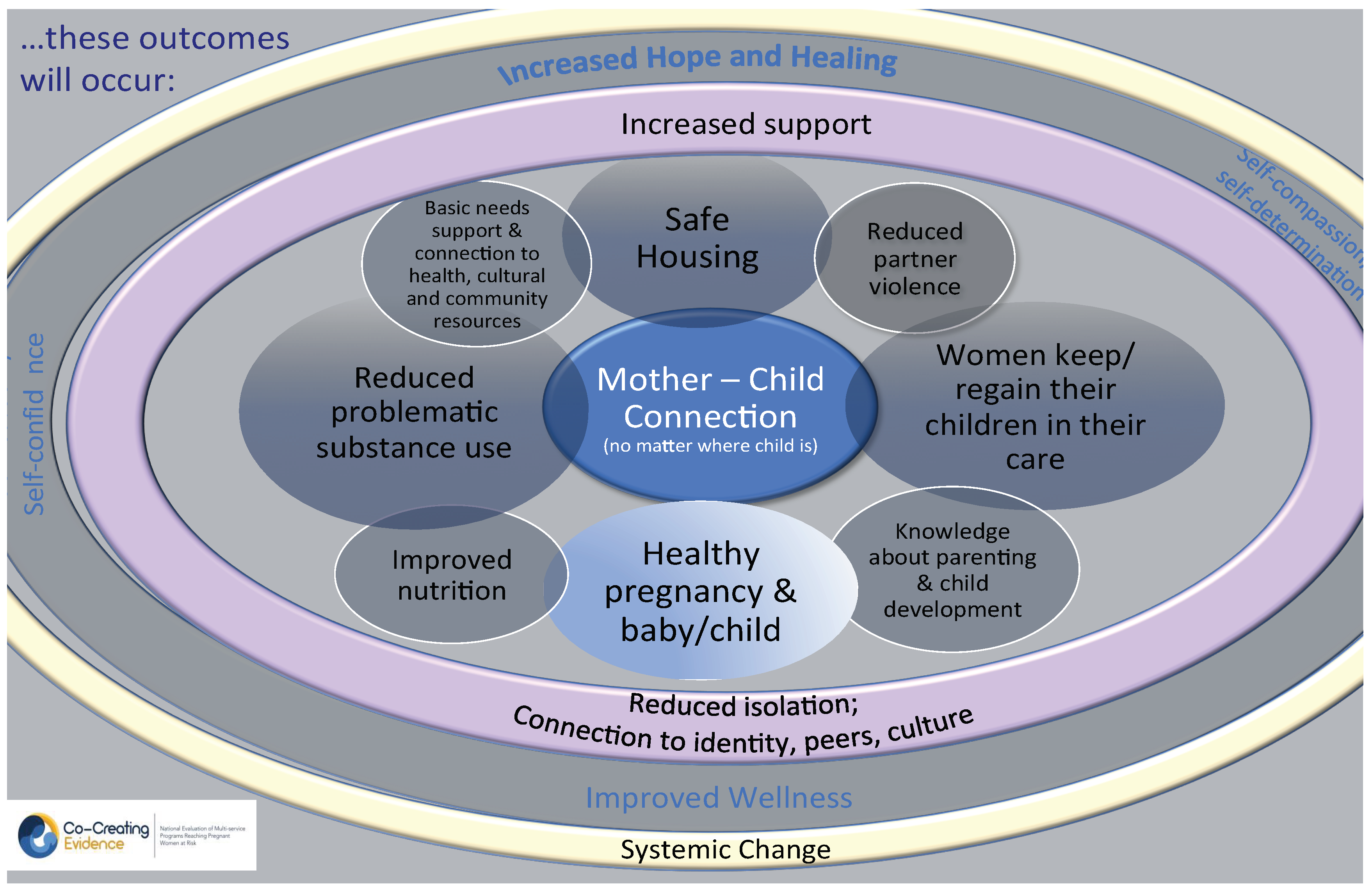
3.1. Theory of Change
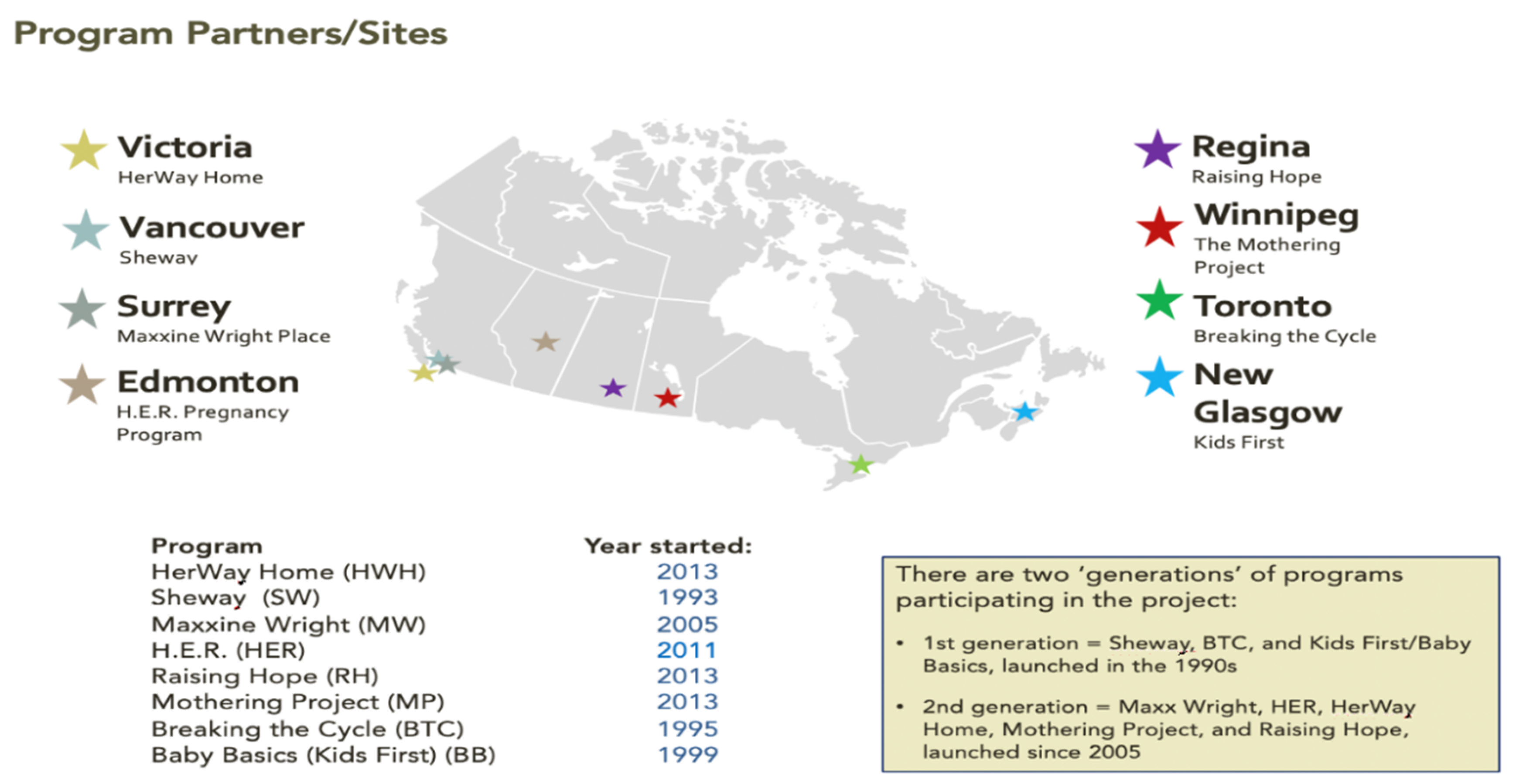
3.2. Overview of Programs’ Governance, Services and Activities
3.3. Client Characteristics
3.4. Clients’ Perspectives on Key Issues at Intake
- Substance use issues—yet readiness for change
- Unsafe or inadequate housing
- Maternal–child separations and/or child welfare involvement
- Violence, trauma and/or intimate partner violence
- Limited social support and/or isolation
- Mental health issues
3.4.1. Substance Use Intertwined with Other Issues, yet Pregnancy Sparks Readiness to Make Changes
I was pregnant. I quit using during the summer, but I was struggling with abuse, depression, anxiety and co-dependency.
I was pregnant but was determined to stay sober. My first daughter was apprehended at birth and was affected by alcohol, so I wanted to do it differently this time.
I was trying to quit doing drugs, hanging out with people using drugs. They were a bad influence. I was also pregnant with my sixth child; the five older children are all in care.
3.4.2. Housing Insecurity
I was working on the street and supporting my habit. I was homeless and couch-surfing.
I was living in a two-bedroom apartment with my mom, sister, two boys, my ex and sometimes my mom’s friends. There could be 13 people at a time in the apartment.
My partner didn’t respect my space—there was partying, and I was uncomfortable; the housing was unsafe. There was domestic violence.
3.4.3. Maternal–Child Separation
I was living in [supportive housing]; pregnant and then gave birth. I was depressed and wanted to address my drug and alcohol use. My son was apprehended at birth.
I had started using again. It wasn’t a good time; after I had the baby I dropped her off with (Child and Family Services)—I felt that I wasn’t able to care for my daughter and that it was for the baby’s own safety.
I was pregnant. I had just quit using drugs a month before that. I was living with my boyfriend’s parents at the time. I knew that I’d be better off here at [the program] if I wanted to get my kids back.
3.4.4. Violence, Trauma or Intimate Partner Violence
My partner assaulted me when I was two months pregnant. I have two older children and am a single parent with social anxiety, mental health issues and a long history of trauma.
3.4.5. Isolation/Limited Social Support
I didn’t have a lot of social support. I have no family and was raised in foster care and by my grandmother who is now deceased.
I was living in an SRO, using crystal meth and heroin every day. I almost never left the SRO. I didn’t like to go out. I was very much shut off from other people.
3.4.6. Mental Health Issues
I was fleeing an abusive relationship. My mental health was poor. I was addicted and not taking care of myself.
I was starting to fall back into drug use. I was depressed, and I was scared of my behaviour.
3.5. Clients’ Involvement in and Experience of Their Program’s Services/Activities
3.6. Clients’ Experiences: What Clients Like Best about Their Program
- Staff and their approach—caring, non-judgmental, supportive and helpful
- Friendships, social and peer support, sense of community
- “One-stop”—multiple services in one place
- Homey, safe, healthy environment
- Help with child protection issues
- Positive impacts for my child—friendships and socialization skills
3.6.1. Staff and Their Approach: Caring, Non-Judgmental, Supportive, and Helpful
The people that work at [the program], they aren’t judgmental. I feel like a person at [the program], not a nobody.
The staff—they give you endless support. When you tell them something, like if there’s been a slip, there’s no judgement. They’re very genuine. The right people work here.
[I like] that they never gave up on me. I was stubborn and had mood swings when I was coming off drugs. I really appreciate that they never gave up on me.
3.6.2. Friendships, Social and Peer Support, Sense of Community
Definitely, the friends I’ve met here. […]The moms are both in recovery and are new moms. It’s easy to relate to them and to get along; we have things in common and have the same aspirations and common goals.
It feels like a family. The staff genuinely care about everyone. They always have time for you. I’ve made good friends at [the program].
The sense of community. That’s the biggest thing. When we come here—because we see and hear other people—we get a more in-depth relationship with people here.
3.6.3. “One-Stop”—Multiple Services in One Place
I don’t have to go far to get to a doctor. There are all kinds of different resources here. There is a welfare worker, a housing worker, the tax lady, as well as food to eat. It’s awesome. There’s also a Walking Group and a Boxing Group.
There are lot of services in one place, such as the public health nurse, the nurse practitioner, and a social worker, which makes it easier to meet the Ministry’s goals and expectations. I don’t have to travel far to get to my appointments. It’s very convenient and close to housing.
I like that they are hands on with support. They have medical, counselling, and practical support; everything I need is in one place. And I like that it is a safe place and there is food.
I like that you can come here and get any support that you need—for example, I can get help getting welfare or with my addictions.
3.6.4. Homey, Safe, Healthy Environment
It’s a safe place for me no matter what is going on in my life—I won’t be judged by anyone. I can be myself. It is a place to connect with other women. I can be less guarded at [the program].
It’s a place to eat and relax and get away from my abusive ex. He can’t bug me at [the program].
The ladies—my peers—and the staff. And that it’s in the North End. There’s so much in the North End that’s dysfunctional, and the program here is the one thing that’s functional. It’s like a sanctuary.
3.6.5. Help with Child Protection Issues
I had a meeting with program social worker who encouraged me to meet with CFS and even inspected my house to give me suggestions for what CFS would be looking for. So, when we met with the CFS worker, I was surprised at how well the meeting went.
Plus, they are willing to support parents with kids in care. My two daughters have been removed again. [The program] is a support for me, helping me to get my children back.
That they are always available to help, no matter how I am feeling and no matter what is happening in my life. For example, they helped calm me down when the kids were apprehended. They gave me confidence and kept me on the right track. They gave me a lot of support. I had my supervised visits with my kids two to three times a week at [the program].
3.6.6. Positive Impacts for My Child—Friendships and Socialization Skills
Plus, my daughter gets so much out of it.
The best thing about [the program] is the drop-in. You meet other women and learn from them. You make friends. Plus, children get to make friends.
I like that it is geared towards children too. At first, I didn’t want my son involved because I didn’t want him around drug users but then I saw that the focus included children and that they were seen and assessed through [the program]—that [the program] was beneficial for children as well.
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Boyd, S.; Marcellus, L. With Child: Substance Use during Pregnancy: A Woman-Centred Approach; Fernwood Publishing: Halifax, NS, Canada, 2007. [Google Scholar]
- Marcellus, L.; MacKinnon, K.; Benoit, C.; Phillips, R.; Stengel, C. Re-envisioning success for programs supporting pregnant women with problematic substance use. Qual. Health Res. 2015, 25, 500–512. [Google Scholar] [CrossRef] [PubMed]
- Gelb, K.; Rutman, D. Substance Using Women with FASD and FASD Prevention: A Literature Review on Promising Approaches in Substance Use Treatment and Care for Women with FASD; University of Victoria School of Social Work: Victoria, BC, Canada, 2011. [Google Scholar]
- Pepler, D.; Motz, M.; Leslie, M.; Jenkins, J.; Espinet, S.; Reynolds, W. A Focus on Relationships; Mothercraft Press: Toronto, ON, Canada, 2014. [Google Scholar]
- Motz, M.; Leslie, M.; Pepler, D.; Moore, T.; Freeman, P. Breaking the Cycle: Measures of Progress 1995–2005. Special Supplement. J. FAS Int. 2006, 4, e22. [Google Scholar]
- Corse, S.; Smith, M. Reducing substance abuse during pregnancy: Discriminating among levels of response in a prenatal setting. J. Subst. Abuse Treat. 1998, 15, 457–467. [Google Scholar] [CrossRef]
- Poole, N.; Isaac, B. Apprehensions: Barriers to Treatment for Substance-Using Mothers; British Columbia Centre of Excellence for Women’s Health: Vancouver, BC, Canada, 2001. [Google Scholar]
- Nathoo, T.; Poole, N.; Bryans, M.; Dechief, L.; Hardeman, S.; Marcellus, L.; Poag, B.; Taylor, M. Voices from the Community: Developing Effective Community Programs to Support Pregnant and Early Parenting Women Who Use Alcohol and Other Substances. First Peoples Child Fam. Rev. 2013, 8, 94–107. [Google Scholar]
- Gopman, S. Prenatal and postpartum care of women with substance use disorders. Obstet. Gynecol. Clin. N. Am. 2014, 41, 213–228. [Google Scholar] [CrossRef] [PubMed]
- Nathoo, T.; Marcellus, L.; Bryans, M.; Clifford, D.; Louie, S.; Penaloza, D.; Seymour, A.; Taylor, M.; Poole, N. Harm Reduction and Pregnancy: Community-based Approaches to Prenatal Substance Use in Western Canada; University of Victoria School of Nursing and British Columbia Centre of Excellence for Women’s Health: Victoria, BC, Canada; Vancouver, BC, Canada, 2015. [Google Scholar]
- Rutman, D.; Callahan, M.; Lundquist, A.; Jackson, S.; Field, B. Substance Use and Pregnancy: Conceiving Women in the Policy Process; Status of Women Canada: Ottawa, ON, Canada, 2000. [Google Scholar]
- Network Action Team on FASD Prevention from a Women’s Health Determinants Perspective. Consensus on 10 Fundamental Components of FASD Prevention from a Women’s Health Determinants Perspective; BC Centre of Excellence for Women’s Health: Vancouver, BC, Canada, 2010. [Google Scholar]
- Sword, W.; Jack, S.; Niccols, A.; Milligan, K.; Henderson, J.; Thabane, L. Integrated programs for women with substance use issues and their children: A qualitative meta-synthesis of processes and outcomes. Harm Reduct. J. 2009, 9, 32. [Google Scholar] [CrossRef] [PubMed]
- Tarasoff, L.; Milligan, K.; Le, T.; Usher, A.; Urbanowski, K. Integrated treatment programs for pregnant and parenting women with problematic substance use: Service descriptions and client perceptions of care. J. Subst. Abuse Treat. 2018, 90, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Latuskie, K.A.; Leibson, T.; Andrews, N.; Motz, M.; Pepler, D.; Ito, S. Substance Use in pregnancy among vulnerable women seeking addiction and parenting support. Int. J. Ment. Health Addict. 2018, 17, 137–150. [Google Scholar] [CrossRef]
- Kruger, D.J.; Morrel-Samuels, S.; Davis-Satterla, L.; Harris-Ellis, B.J.; Slonim, A. Developing a cross-site evaluation tool for diverse health interventions. Health Promot. Pract. 2010, 11, 555–561. [Google Scholar] [CrossRef]
- Rutman, D.; Hubberstey, C.; Poole, N.; Hume, S.; Van Bibber, M. Developing and using a common framework to evaluate FASD programs: Results of a three-year Canadian project. Int. J. Ment. Health Addict. 2015. [Google Scholar] [CrossRef]
- Marshall, S.; Charles, G.; Hare, J.; Ponzetti, J.; Stokl, M. Sheway’s services for substance using pregnant and parenting women: Evaluating the outcomes for infants. Can. J. Community Ment. Health 2005, 24, 19–33. [Google Scholar] [CrossRef]
- Poole, N. Evaluation Report of the Sheway Project for High-Risk, Pregnant and Parenting Women; British Columbia Centre of Excellence for Women’s Health: Vancouver, BC, Canada, 2000. [Google Scholar]
- Pepler, D.; Moore, T.; Motz, M.; Leslie, M. Breaking the Cycle: The Evaluation Report (1995–2000); Breaking the Cycle: Toronto, ON, Canada, 2002. [Google Scholar]
- Racine, N.; Motz, M.; Leslie, M.; Pepler, D. Breaking the Cycle Pregnancy Outreach Program: Reaching out to improve the health and well-being of pregnant substance involved mothers. J. Assoc. Res. Mothering 2009, 11, 279–290. [Google Scholar]
- Wodinski, L. Impact Evaluation of the Healthy, Empowered and Resilient (H.E.R.) Program—Stakeholder Perceptions Final Report; Alberta Centre for Child, Family & Community Research: Edmonton, AB, Canada, 2013. [Google Scholar]
- Wodinski, L.; Wanke, M. Impact Evaluation of the Healthy, Empowered and Resilient (H.E.R.) Program—Photovoice Final Report; Alberta Centre for Child, Family & Community Research: Edmonton, AB, Canada, 2013. [Google Scholar]
- Wodinski, L.; Wanke, M.; Khan, F. Impact Evaluation of the Healthy, Empowered and Resilient (H.E.R.) Program—Summary Final Report; Alberta Centre for Child, Family & Community Research: Edmonton, AB, Canada, 2013. [Google Scholar]
- Nota Bene Consulting Group. HerWay Home Final Evaluation Report; Nota Bene Consulting Group: Victoria, BC, Canada, 2017. [Google Scholar]
- BC Centre of Excellence for Women’s Health. Treatment and Care for Pregnant Who Use Alcohol and Other Drugs: Information for Service Providers. Coalescing on Women and Substance Use. Available online: http://bccewh.bc.ca/wp-content/uploads/2014/08/FASD-Sheet-4_Alcohol-Pregnancy-Tx-Care-Dec-6.pdf (accessed on 22 March 2019).
- Handmaker, N.; Miller, W.; Manicke, M. Findings of a pilot study of motivational interviewing with pregnant drinkers. J. Stud. Alcohol 1999, 60, 285–287. [Google Scholar] [CrossRef] [PubMed]
- Poole, N.; Schmidt, R.; Green, C.; Hemsing, N. Prevention of Fetal Alcohol Spectrum Disorder: Current Canadian efforts and analysis of gaps. Subst. Abuse Res. Treat. 2016, 10, 1. [Google Scholar] [CrossRef]
- Berghold, J.; Thomas, S. Participatory research methods: A methodological approach in motion. Qual. Soc. Res. 2012, 13, 30. [Google Scholar]
- Cousins, J.; Whitmore, E.; Shulha, L.; Al Hubib, H.; Gilbert, N. Principles to Guide Collaborative Approaches to Evaluation. Canadian Evaluation Society, 2015. Available online: https://evaluationcanada.ca/sites/default/files/20170131_caebrochure_en.pdf (accessed on 22 March 2019).
- Shulha, L.; Whitmore, E.; Cousins, J.B.; Gilbert, N.; Al Hudib, H. Introducing evidence-based principles to guide collaborative approaches to evaluation: Results of an empirical process. Am. J. Eval. 2016, 37, 193–217. [Google Scholar] [CrossRef]
- Patton, M. Qualitative Evaluation and Research Methods; Sage: Newbury Park, CA, USA, 1990. [Google Scholar]
- Davies, R.; Dart, J. The ‘Most Significant Change’ (MSC) Technique: A Guide to Its Use; CARE International: London, UK, 2005. [Google Scholar]
- Fallot, R.; Harris, M. Creating Cultures of Trauma-Informed Care (CCTIC): A Self-Assessment and Planning Protocol; Community Connections: Washington, DC, USA, 2009. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Thorne, S. Data analysis in qualitative research. Evid. Based Nurs. 2000, 3, 68–70. [Google Scholar] [CrossRef] [Green Version]
- Poole, N. Mother and child reunion: Preventing Fetal Alcohol Spectrum Disorder by Promoting Women’s Health; British Columbia Centre of Excellence for Women’s Health: Vancouver, BC, Canada, 2003. [Google Scholar]
- BC Ministry of Health. Following the Evidence, Preventing Harms from Substance Use in BC; BC Ministry of Health: Victoria, BC, Canada, 2006.
- Kelty Mental Health Resource Centre. Addiction and Substance Use. Available online: http://keltymentalhealth.ca/substance-use/addiction-substance-use-overview (accessed on 22 February 2019).
- Heaman, M.I.; Moffatt, M.; Elliott, L.; Sword, W.; Helewa, M.E.; Morris, H.; Gregory, P.; Tjaden, L.; Cook, C. Barriers, motivators and facilitators related to prenatal care utilization among inner-city women in Winnipeg, Canada: A case-control study. BMC Pregnancy Childb. 2014, 14, 227. [Google Scholar] [CrossRef]
- Lange, S.; Probst, C.; Quere, M.; Rehm, J.; Popova, S. Alcohol use, smoking and their co-occurrence during pregnancy among Canadian women, 2003 to 2011/12. Addict. Behav. 2015, 50, 102–109. [Google Scholar] [CrossRef]
- Lange, S.; Quere, M.; Shield, K.; Rehm, J.; Popova, S. Alcohol use and self-perceived mental health status among pregnant and breastfeeding women in Canada: A secondary data analysis. BJOG 2015, 123, 900–909. [Google Scholar] [CrossRef] [PubMed]
- Meixner, T.; Milligan, K.; Urbanoski, K.; McShane, K. Conceptualizing integrated service delivery for pregnant and parenting women with e addictions: Defining key factors and processes. Can. J. Addict. 2016, 7, 57–65. [Google Scholar]
- Andrews, N.; Motz, M.; Pepler, D.; Jeong, J.; Khoury, J. Engaging mothers with substance use issues and their children in early intervention: Understanding use of service and outcomes. Child Abuse Negl. 2018, 83, 10–20. [Google Scholar] [CrossRef]
- Marcellus, L. A grounded theory of mothering in the early years for women recovering from substance use. J. Fam. Nurs. 2017, 23, 341–365. [Google Scholar] [CrossRef] [PubMed]
- Network Action Team on FASD Prevention from a Women’s Health Determinants Perspective. Supporting Pregnant and Parenting Women Who Use Substances: What Communities Are Doing to Help. Available online: http://bccewh.bc.ca/wp-content/uploads/2012/05/2012_SupportingPregnantandParentingWomenWhoUseSubstances.pdf (accessed on 22 March 2019).
- Urbanoski, K.; Joordens, C.; Kolla, G.; Milligan, K. Community networks of services for pregnant and parenting women with problematic substance use. PLoS ONE 2018, 13, e0206671. [Google Scholar] [CrossRef]
- Greaves, L.; Poole, N.; Boyle, E. Transforming Addiction: Gender, Trauma, Transdisciplinarity; Routledge: New York, NY, USA, 2015. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Service/Activity | Number of Programs Offering Service/Activity on Site via Program Staff or Service Partners | Number of Programs Linking Clients to Service/Activity via Referral to Service Partners | Total Number of Programs Offering or Facilitating Access to Service |
|---|---|---|---|
| Basic needs support | 8 | 0 | 8 |
| Child assessment and early intervention | 5 | 2 | 7 |
| Child care on site | 7 | 0 | 7 |
| Child health | 6 | 2 | 8 |
| Child welfare support | 7 | 0 | 7 |
| Cultural programming | 5 | 1 | 6 |
| Drop in; peer connection | 8 | 0 | 8 |
| Food; nutrition | 8 | 0 | 8 |
| Health; medical services | 6 | 2 | 8 |
| Housing | 4 | 4 | 8 |
| Life skills | 6 | 1 | 7 |
| Mental health; trauma | 8 | 0 | 8 |
| Outreach | 6 | 0 | 6 |
| Parenting programs | 7 | 1 | 8 |
| Prenatal; postnatal care | 7 | 1 | 8 |
| Substance use counselling | 7 | 1 | 8 |
| HWH | SW | MW | HER | RH | MP | BTC | BB | Total | |
|---|---|---|---|---|---|---|---|---|---|
| Number of clients | 95 | 327 | 82 | 50 | 24 | 37 | 66 | 31 | 712 |
| Age | |||||||||
| <16 | 1% | 0% | 0% | 0% | 0% | 0% | 0% | 3% | 0% |
| 16–24 | 37% | 16% | 28% | 26% | 25% | 49% | 24% | 94% | 27% |
| 25–30 | 39% | 35% | 48% | 26% | 54% | 35% | 30% | 3% | 35% |
| >31 | 23% | 49% | 24% | 46% | 21% | 16% | 44% | 0% | 37% |
| Pregnant | 79% | 92% | 100% | 96% | 63% | 65% | 50% | 68% | 84% |
| Substance Use | |||||||||
| Problematic use | 21% | 52% | 28% | 62% | 46% | 70% | 18% | 3% | 41% |
| Harm reduction | 0% | 21% | 5% | 10% | 0% | 27% | 17% | 7% | 14% |
| In recovery/abstaining | 41% | 8% | 35% | 4% | 4% | 0% | 36% | 3% | 17% |
| New to recovery | 37% | 17% | 22% | 0% | 46% | 0% | 26% | 0% | 19% |
| Non-problematic use | 0% | 2% | 5% | 4% | 0% | 0% | 0% | 16% | 2% |
| Housing | |||||||||
| Not housed/ homeless | 33% | 29% | 12% | 46% | 50% | 11% | 12% | 0% | 26% |
| Unsafe/inadequate | 32% | 33% | 38% | 28% | 38% | 60% | 26% | 39% | 34% |
| Safe and stable | 36% | 37% | 43% | 10% | 13% | 27% | 42% | 26% | 34% |
| Indigenous (self-identified) | 42% | 67% | 23% | 81% | 77% | 97% | 10% | 0% | 56% |
| Program Activity | Clients’ Experiences—in Their Words |
|---|---|
| Food/nutrition | I do the Breakfast Club, and we always feel free to use the kitchen—there’s a client fridge. And they have feasts, and kids have food. They don’t serve junk food; it’s healthy. Breakfast is made by the moms. It helps to learn new recipes/ideas and to try new foods. There are multiple foods that I now include in my diet that I wouldn’t have prior to coming here. |
| Housing/basic needs support | They helped me get into social housing when I was pregnant; it is housing with rules. I had to stay sober for 18 months and then once I graduated I got to take over the lease myself. I get anxious when I have to call “official” people. They did a letter of support for me so I could access disability funding. They also helped with transportation (bus tokens), and they gave me a gift card so I could buy a bathing suit, so I could go swimming with my daughter. |
| Pre/post-natal health support | They got me connected to an OBGYN, nurses, ultrasound; they drove me to appointments and followed up with me to see if I went. If I missed the appointment, we rebooked. I have check-ups here and get prenatal vitamins regularly. |
| Women’s health services | I see the nurse practitioner or doctor for birth control. It is such a comfort to have someone I know and trust to put the IUD in for me. I have sexual trauma and could not go to a stranger. The public health nurse makes sure I am healthy, have a regular pap test, etc. She was key in making sure I had proper care when I broke my arm. |
| Children’s health, assessment, referrals | My sons had vaccinations with public health nurse and saw the dental hygienist. He is getting dental surgery soon as a result. We were referred to Sunny Hill hospital and introduced to a dentist for the children. The staff made sure the children were up to date for their immunizations and referred them to an Infant Development worker. |
| Support/advocacy re: child welfare | When I was pregnant, the program helped with our anxiety about meeting with the social worker, and then she closed our file. Without the program, they wouldn’t have closed our file as soon. From the beginning the program has been at all the meetings with me. Because of their presence, there were no hidden agendas in terms of what I had to do to get my children back. |
| Alcohol and drug counselling, education, and support | Addiction services come here; I had a referral for family treatment. There is lots of support for relapse. I just signed up for the SWAG (Struggling With Addictions Group) program. I feel grateful. |
| Peer/social connections and groups | That’s huge here. I think that’s the main focus for me right now. All the women who did prenatal together, now our children are all the same age. I have connected with two women who are sober and parenting. I like connecting with them. That is what happens with all of the groups and for the kids as well—they get peer/social connections too. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rutman, D.; Hubberstey, C. National Evaluation of Canadian Multi-Service FASD Prevention Programs: Interim Findings from the Co-Creating Evidence Study. Int. J. Environ. Res. Public Health 2019, 16, 1767. https://doi.org/10.3390/ijerph16101767
Rutman D, Hubberstey C. National Evaluation of Canadian Multi-Service FASD Prevention Programs: Interim Findings from the Co-Creating Evidence Study. International Journal of Environmental Research and Public Health. 2019; 16(10):1767. https://doi.org/10.3390/ijerph16101767
Chicago/Turabian StyleRutman, Deborah, and Carol Hubberstey. 2019. "National Evaluation of Canadian Multi-Service FASD Prevention Programs: Interim Findings from the Co-Creating Evidence Study" International Journal of Environmental Research and Public Health 16, no. 10: 1767. https://doi.org/10.3390/ijerph16101767