Built Environment, Psychosocial Factors and Active Commuting to School in Adolescents: Clustering a Self-Organizing Map Analysis




Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.2.1. Study Outcome: Active Commuting to and from School
2.2.2. Built-Environment Factors
2.2.3. Psychosocial Factors
2.3. Data Analysis
3. Results
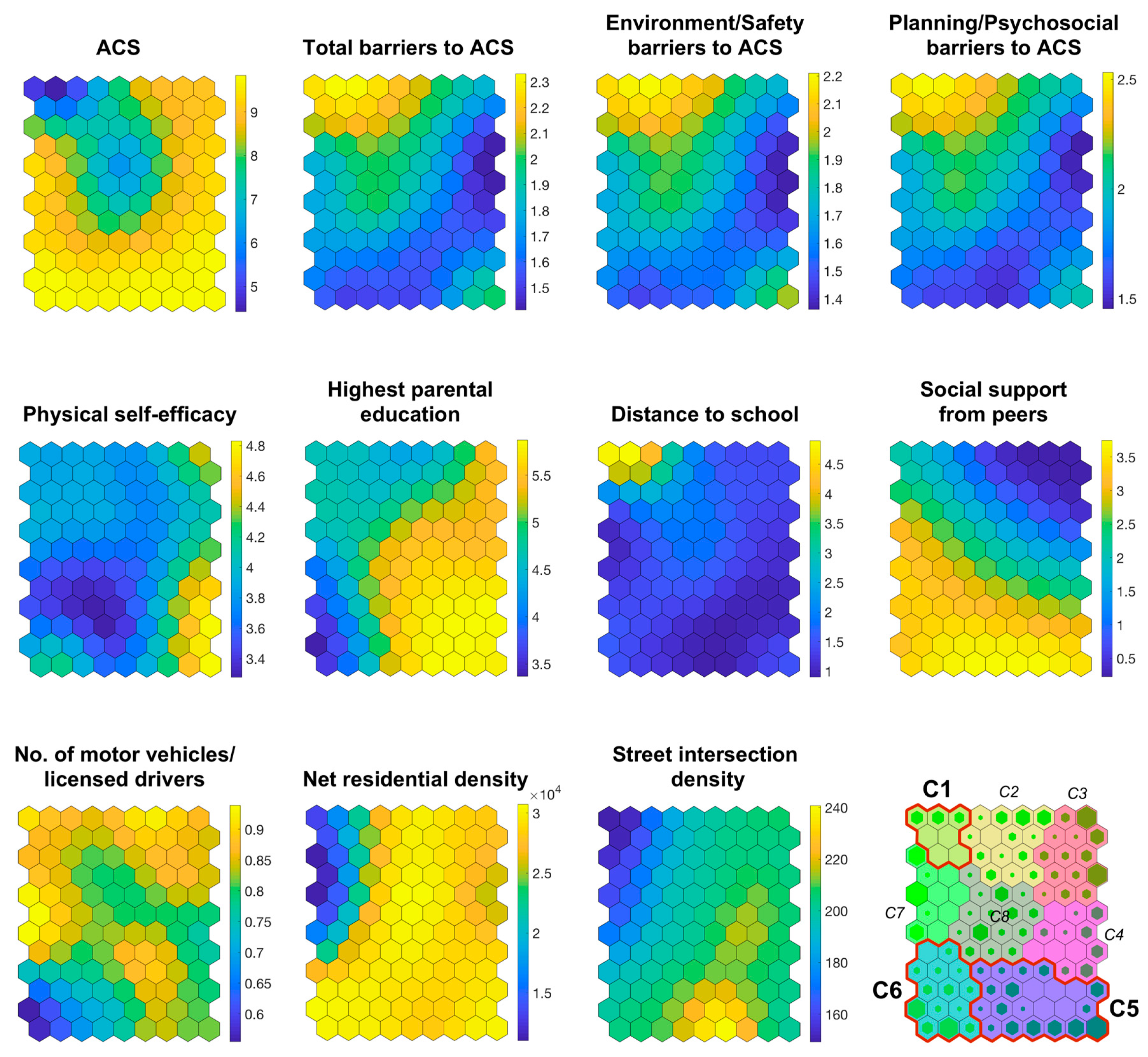
3.1. Number and Description of Clusters
3.2. Comparison of Clusters
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneve, Switzerland, 2018; ISBN 978-92-4-151418-7. [Google Scholar]
- Chillón, P.; Ortega, F.B.; Ruiz, J.R.; Veidebaum, T.; Oja, L.; Mäestu, J.; Sjöström, M. Active commuting to school in children and adolescents: An opportunity to increase physical activity and fitness. Scand. J. Public Health 2010, 38, 873–879. [Google Scholar] [CrossRef]
- Lubans, D.R.; Boreham, C.A.; Kelly, P.; Foster, C.E. The relationship between active travel to school and health-related fitness in children and adolescents: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 5. [Google Scholar] [CrossRef]
- Villa-González, E.; Ruiz, J.R.; Chillón, P. Associations between active commuting to school and health-related physical fitness in Spanish school-aged children: A cross-sectional study. Int. J. Environ. Res. Public Health 2015, 12, 10362–10373. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Ariza, A.; de la Torre-Cruz, M.J.; Redecillas-Peiró, M.T.; Martínez-López, E.J. Influence of active commuting on happiness, well-being, psychological distress and body shape in adolescents. Gac. Sanit. 2015, 29, 454–457. [Google Scholar] [CrossRef] [PubMed]
- Frank, L.D.; Greenwald, M.J.; Winkelman, S.; Chapman, J.; Kavage, S. Carbonless footprints: Promoting health and climate stabilization through active transportation. Prev. Med. 2010, 50 (Suppl. 1), S99–S105. [Google Scholar] [CrossRef] [PubMed]
- Giles-Corti, B.; Foster, S.; Shilton, T.; Falconer, R. The co-benefits for health of investing in active transportation. N. S. W. Public Health Bull. 2010, 21, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Giles-Corti, B.; Kelty, S.; Zubrick, S.; Villanueva, K. Encouraging walking for transport and physical activity in children and adolescents: How important is the built environment? Sports Med. 2009, 39, 995–1009. [Google Scholar] [CrossRef] [PubMed]
- Buliung, R.N.; Mitra, R.; Faulkner, G. Active school transportation in the Greater Toronto Area, Canada: An exploration of trends in space and time (1986–2006). Prev. Med. 2009, 48, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Chillón, P.; Martínez-Gómez, D.; Ortega, F.B.; Pérez-López, I.J.; Díaz, L.E.; Veses, A.M.; Veiga, O.L.; Marcos, A.; Delgado-Fernández, M. Six-year trend in active commuting to school in Spanish adolescents. The AVENA and AFINOS Studies. Int. J. Behav. Med. 2013, 20, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Dygrýn, J.; Mitáš, J.; Gába, A.; Rubín, L.; Frömel, K. Changes in Active Commuting to School in Czech Adolescents in Different Types of Built Environment across a 10-Year Period. Int. J. Environ. Res. Public Health 2015, 12, 12988–12998. [Google Scholar] [CrossRef] [Green Version]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An Ecological Approach to Creating Active Living Communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Owen, N. Ecological models of health behavior. In Health Behavior: Theory, Research, and Practice; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2015; pp. 43–64. ISBN 978-0-7879-9614-7. [Google Scholar]
- McGrath, L.J.; Hopkins, W.G.; Hinckson, E.A. Associations of objectively measured built-environment attributes with youth moderate-vigorous physical activity: A systematic review and meta-analysis. Sports Med. Auckl. NZ 2015, 45, 841–865. [Google Scholar] [CrossRef]
- Lord, S.; Manlhiot, C.; Tyrrell, P.N.; Dobbin, S.; Gibson, D.; Chahal, N.; Stearne, K.; Fisher, A.; McCrindle, B.W. Lower socioeconomic status, adiposity and negative health behaviours in youth: A cross-sectional observational study. BMJ Open 2015, 5, e008291. [Google Scholar] [CrossRef] [PubMed]
- Molina-García, J.; Queralt, A.; Adams, M.A.; Conway, T.L.; Sallis, J.F. Neighborhood built environment and socio-economic status in relation to multiple health outcomes in adolescents. Prev. Med. 2017, 105, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.A.; Sallis, J.F.; Kerr, J.; Conway, T.L.; Saelens, B.E.; Frank, L.D.; Norman, G.J.; Cain, K.L. Neighborhood environment profiles related to physical activity and weight status: A latent profile analysis. Prev. Med. 2011, 52, 326–331. [Google Scholar] [CrossRef] [Green Version]
- Christiansen, L.B.; Madsen, T.; Schipperijn, J.; Ersbøll, A.K.; Troelsen, J. Variations in active transport behavior among different neighborhoods and across adult lifestages. J. Transp. Health 2014, 1, 316–325. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Cerin, E.; Conway, T.L.; Adams, M.A.; Frank, L.D.; Pratt, M.; Salvo, D.; Schipperijn, J.; Smith, G.; Cain, K.L.; et al. Physical activity in relation to urban environments in 14 cities worldwide: A cross-sectional study. Lancet 2016, 387, 2207–2217. [Google Scholar] [CrossRef]
- Frank, L.D.; Sallis, J.F.; Saelens, B.E.; Leary, L.; Cain, K.; Conway, T.L.; Hess, P.M. The development of a walkability index: Application to the Neighborhood Quality of Life Study. Br. J. Sports Med. 2010, 44, 924–933. [Google Scholar] [CrossRef]
- Forsyth, A.; Oakes, J.M.; Schmitz, K.H.; Hearst, M. Does Residential Density Increase Walking and Other Physical Activity? Urban Stud. 2007, 44, 679–697. [Google Scholar] [CrossRef]
- Chaudhury, H.; Mahmood, A.; Michael, Y.L.; Campo, M.; Hay, K. The influence of neighborhood residential density, physical and social environments on older adults’ physical activity: An exploratory study in two metropolitan areas. J. Aging Stud. 2012, 26, 35–43. [Google Scholar] [CrossRef]
- Handy, S.L.; Boarnet, M.G.; Ewing, R.; Killingsworth, R.E. How the built environment affects physical activity: Views from urban planning. Am. J. Prev. Med. 2002, 23, 64–73. [Google Scholar] [CrossRef]
- Carlson, J.A.; Saelens, B.E.; Kerr, J.; Schipperijn, J.; Conway, T.L.; Frank, L.D.; Chapman, J.E.; Glanz, K.; Cain, K.L.; Sallis, J.F. Association between neighborhood walkability and GPS-measured walking, bicycling and vehicle time in adolescents. Health Place 2015, 32, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Queralt, A.; Molina-García, J. Physical activity and active commuting in relation to objectively measured built environment attributes among adolescents. J. Phys. Act. Health. under review.
- Wong, B.Y.-M.; Faulkner, G.; Buliung, R. GIS measured environmental correlates of active school transport: A systematic review of 14 studies. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 39. [Google Scholar] [CrossRef] [Green Version]
- Verhoeven, H.; Simons, D.; Van Dyck, D.; Van Cauwenberg, J.; Clarys, P.; De Bourdeaudhuij, I.; de Geus, B.; Vandelanotte, C.; Deforche, B. Psychosocial and Environmental Correlates of Walking, Cycling, Public Transport and Passive Transport to Various Destinations in Flemish Older Adolescents. PLoS ONE 2016, 11, e0147128. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Conway, T.L.; Cain, K.L.; Carlson, J.A.; Frank, L.D.; Kerr, J.; Glanz, K.; Chapman, J.E.; Saelens, B.E. Neighborhood built environment and socioeconomic status in relation to physical activity, sedentary behavior, and weight status of adolescents. Prev. Med. 2018, 110, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Aznar, S.; Queralt, A.; García-Massó, X.; Villarrasa-Sapiña, I.; Molina-García, J. Multifactorial combinations predicting active vs inactive stages of change for physical activity in adolescents considering built environment and psychosocial factors: A classification tree approach. Health Place 2018, 53, 150–154. [Google Scholar] [CrossRef] [PubMed]
- De Meester, F.; Van Dyck, D.; De Bourdeaudhuij, I.; Deforche, B.; Cardon, G. Do psychosocial factors moderate the association between neighborhood walkability and adolescents’ physical activity? Soc. Sci. Med. 2013, 81, 1–9. [Google Scholar] [CrossRef]
- Wang, X.; Conway, T.L.; Cain, K.L.; Frank, L.D.; Saelens, B.E.; Geremia, C.; Kerr, J.; Glanz, K.; Carlson, J.A.; Sallis, J.F. Interactions of psychosocial factors with built environments in explaining adolescents’ active transportation. Prev. Med. 2017, 100, 76–83. [Google Scholar] [CrossRef]
- Panter, J.R.; Jones, A.P.; van Sluijs, E.M. Environmental determinants of active travel in youth: A review and framework for future research. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 34. [Google Scholar] [CrossRef] [Green Version]
- Chillón, P.; Panter, J.; Corder, K.; Jones, A.P.; Van Sluijs, E.M.F. A longitudinal study of the distance that young people walk to school. Health Place 2015, 31, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Molina-García, J.; Queralt, A. Neighborhood Built Environment and Socio-Economic Status in Relation to Active Commuting to School in Children. J. Phys. Act. Health 2017, 14, 761–765. [Google Scholar] [CrossRef] [PubMed]
- Herrero-Herrero, M.; García-Massó, X.; Martínez-Corralo, C.; Prades-Piñón, J.; Sanchis-Alfonso, V. Relationship between the practice of physical activity and quality of movement in adolescents: A screening tool using self-organizing maps. Phys. Sportsmed. 2017, 45, 271–279. [Google Scholar] [CrossRef]
- Janssen, E.; Sugiyama, T.; Winkler, E.; de Vries, H.; te Poel, F.; Owen, N. Psychosocial correlates of leisure-time walking among Australian adults of lower and higher socio-economic status. Health Educ. Res. 2010, 25, 316–324. [Google Scholar] [CrossRef]
- Estevan, I.; Queralt, A.; Molina-García, J. Biking to School: The Role of Bicycle-Sharing Programs in Adolescents. J. Sch. Health 2018, 88, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control (CDC) Kids-Walk-to-School Program. Available online: http://www.cdc.gov/nccdphp/dnpa/kidswalk/resources.htm (accessed on 1 December 2012).
- Molina-García, J.; Queralt, A.; Estevan, I.; Álvarez, O.; Castillo, I. Perceived barriers to active commuting to school: Reliability and validity of a scale. Gac. Sanit. 2016, 30, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Timperio, A.; Ball, K.; Salmon, J.; Roberts, R.; Giles-Corti, B.; Simmons, D.; Baur, L.A.; Crawford, D. Personal, family, social, and environmental correlates of active commuting to school. Am. J. Prev. Med. 2006, 30, 45–51. [Google Scholar] [CrossRef]
- Villanueva, K.; Knuiman, M.; Nathan, A.; Giles-Corti, B.; Christian, H.; Foster, S.; Bull, F. The impact of neighborhood walkability on walking: Does it differ across adult life stage and does neighborhood buffer size matter? Health Place 2014, 25, 43–46. [Google Scholar] [CrossRef] [Green Version]
- Bentley, R.; Blakely, T.; Kavanagh, A.; Aitken, Z.; King, T.; McElwee, P.; Giles-Corti, B.; Turrell, G. A Longitudinal Study Examining Changes in Street Connectivity, Land Use, and Density of Dwellings and Walking for Transport in Brisbane, Australia. Environ. Health Perspect. 2018, 126, 057003. [Google Scholar] [CrossRef] [Green Version]
- Van Loon, J.; Frank, L.D.; Nettlefold, L.; Naylor, P.-J. Youth physical activity and the neighbourhood environment: Examining correlates and the role of neighbourhood definition. Soc. Sci. Med. 2014, 104, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Ryckman, R.M.; Robbins, M.A.; Thornton, B.; Cantrell, P. Development and validation of a physical self-efficacy scale. J. Pers. Soc. Psychol. 1982, 42, 891–900. [Google Scholar] [CrossRef]
- Molina-García, J.; Queralt, A.; Castillo, I.; Sallis, J.F. Changes in Physical Activity Domains during the Transition out of High School: Psychosocial and Environmental Correlates. J. Phys. Act. Health 2015, 12, 1414–1420. [Google Scholar] [CrossRef] [PubMed]
- Norman, G.J.; Sallis, J.F.; Gaskins, R. Comparability and reliability of paper- and computer-based measures of psychosocial constructs for adolescent physical activity and sedentary behaviors. Res. Q. Exerc. Sport 2005, 76, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Vesanto, J.; Himberg, J.; Alhoniemi, E.; Parhankangas, J. Self-organizing map in Matlab: The SOM Toolbox. In Proceedings of the Matlab DSP Conference, Espoo, Finland, 16–17 November 1999; Volume 99, pp. 35–40. [Google Scholar]
- Pellicer-Chenoll, M.; Garcia-Massó, X.; Morales, J.; Serra-Añó, P.; Solana-Tramunt, M.; González, L.-M.; Toca-Herrera, J.-L. Physical activity, physical fitness and academic achievement in adolescents: A self-organizing maps approach. Health Educ. Res. 2015, 30, 436–448. [Google Scholar] [CrossRef] [PubMed]
- Oliver, E.; Vallés Pérez, I.; Rivera, B.; María, R.; Martí, C.I.; Josep, A.; Botella Arbona, C.; Soria Olivas, E. Visual data mining with self-organizing maps for “self-monitoring” data analysis. Sociol. Methods Res. 2016, 45, 1–15. [Google Scholar] [CrossRef]
- Estevan, I.; García-Massó, X.; Molina-García, J.; Barnett, L.M. Identifying profiles of children at risk of being less physically active: An exploratory study using a self-organised map approach for motor competence. J. Sports Sci. 2019. [Google Scholar] [CrossRef] [PubMed]
- Davies, D.L.; Bouldin, D.W. A cluster separation measure. IEEE Trans. Pattern Anal. Mach. Intell. 1979, 1, 224–227. [Google Scholar] [CrossRef]
- Valencia-Peris, A.; Devís-Devís, J.; García-Massó, X.; Lizandra, J.; Pérez-Gimeno, E.; Peiró-Velert, C. Competing Effects Between Screen Media Time and Physical Activity in Adolescent Girls: Clustering a Self-Organizing Maps Analysis. J. Phys. Act. Health 2016, 13, 579–586. [Google Scholar] [CrossRef]
- Peiró-Velert, C.; Valencia-Peris, A.; González, L.M.; García-Massó, X.; Serra-Añó, P.; Devís-Devís, J. Screen media usage, sleep time and academic performance in adolescents: Clustering a self-organizing maps analysis. PLoS ONE 2014, 9, e99478. [Google Scholar] [CrossRef]
- Verhoeven, H.; Ghekiere, A.; Van Cauwenberg, J.; Van Dyck, D.; De Bourdeaudhuij, I.; Clarys, P.; Deforche, B. Subgroups of adolescents differing in physical and social environmental preferences towards cycling for transport: A latent class analysis. Prev. Med. 2018, 112, 70–75. [Google Scholar] [CrossRef]
- Carlson, J.A.; Sallis, J.F.; Conway, T.L.; Saelens, B.E.; Frank, L.D.; Kerr, J.; Cain, K.L.; King, A.C. Interactions between psychosocial and built environment factors in explaining older adults’ physical activity. Prev. Med. 2012, 54, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Sallis, J.F.; Conway, T.L.; Saelens, B.E.; Frank, L.D.; Cain, K.L.; Slymen, D.J. Interactive effects of built environment and psychosocial attributes on physical activity: A test of ecological models. Ann. Behav. Med. Publ. Soc. Behav. Med. 2012, 44, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Barnett, A.; Sit, C.H.P.; Mellecker, R.R.; Cerin, E. Associations of socio-demographic, perceived environmental, social and psychological factors with active travel in Hong Kong adolescents: The iHealt(H) cross-sectional study. J. Transp. Health 2018. [Google Scholar] [CrossRef]
- Rodríguez-López, C.; Salas-Fariña, Z.M.; Villa-González, E.; Borges-Cosic, M.; Herrador-Colmenero, M.; Medina-Casaubón, J.; Ortega, F.B.; Chillón, P. The Threshold Distance Associated with Walking from Home to School. Health Educ. Behav. 2017, 44, 857–866. [Google Scholar] [CrossRef] [PubMed]
- De Meester, F.; Van Dyck, D.; De Bourdeaudhuij, I.; Deforche, B.; Cardon, G. Does the perception of neighborhood built environmental attributes influence active transport in adolescents? Int. J. Behav. Nutr. Phys. Act. 2013, 10, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, D.; Sallis, J.F.; Kerr, J.; Lee, S.; Rosenberg, D.E. Neighborhood environment and physical activity among youth a review. Am. J. Prev. Med. 2011, 41, 442–455. [Google Scholar] [CrossRef] [PubMed]
- Larouche, R.; Mammen, G.; Rowe, D.A.; Faulkner, G. Effectiveness of active school transport interventions: A systematic review and update. BMC Public Health 2018, 18, 206. [Google Scholar] [CrossRef] [PubMed]
- Henderson, S.; Tanner, R.; Klanderman, N.; Mattera, A.; Martin Webb, L.; Steward, J. Safe routes to school: A public health practice success story—Atlanta, 2008–2010. J. Phys. Act. Health 2013, 10, 141–142. [Google Scholar] [CrossRef] [PubMed]
- Mandic, S.; Flaherty, C.; Ergler, C.; Kek, C.C.; Pocock, T.; Lawrie, D.; Chillón, P.; García Bengoechea, E. Effects of cycle skills training on cycling-related knowledge, confidence and behaviour in adolescent girls. J. Transp. Health 2018, 9, 253–263. [Google Scholar] [CrossRef]
- Buckley, A.; Lowry, M.B.; Brown, H.; Barton, B. Evaluating safe routes to school events that designate days for walking and bicycling. Transp. Policy 2013, 30, 294–300. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Range | Mean (SD) or % |
|---|---|---|
| Gender (female) | - | 55.1 |
| Age | 14–18 | 16.5 (0.78) |
| SES (highest parental education) | 1–6 | 5.06 (1.22) |
| ACS (trips per week) | 0–10 | 8.79 (3.08) |
| Variable | H (7) | p-Value |
|---|---|---|
| ACS | 81.57 | <0.001 |
| Total barriers to ACS | 77.15 | <0.001 |
| Environment/Safety barriers to ACS | 77.23 | <0.001 |
| Planning/Psychosocial barriers to ACS | 77.88 | <0.001 |
| Physical self-efficacy | 34.81 | <0.001 |
| Higher parental education | 88.53 | <0.001 |
| Distance to school | 81.69 | <0.001 |
| Social support from peers | 94.45 | <0.001 |
| No. of motor vehicles per licensed driver | 59.18 | <0.001 |
| Net residential density | 56.77 | <0.001 |
| Street intersection density | 79.97 | <0.001 |
| Cluster | ACS (Trips per Week) | Total Barriers to ACS | Environment/Safety Barriers to ACS | Planning/Psychosocial Barriers to ACS | Physical Self-Efficacy | Higher Parental Education | Distance to School (km) | Social Support from Peers | Nº. of Motor Vehicles per Licensed Drivers | Net Residential Density (per km2) | Street Intersection Density (per km2) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 (n = 7) | 5.86 | 2.24 | 2.12 | 2.42 | 3.88 | 4.62 | 3.83 | 1.98 | 0.87 | 17491.18 | 160.62 |
| (1.19) 5,6 | (0.08) 5,6 | (0.07) 5,6 | (0.10) 5,6 | (0.02) | (0.04) 5 | (0.95) 5,6 | (0.24) 5,6 | (0.02) 6 | (3648.23) 5,6 | (10.23) 5 | |
| 2 (n = 14) | 7.50 | 2.08 | 1.98 | 2.23 | 3.82 | 4.65 | 2.04 | 0.98 | 0.85 | 28,939.04 | 195.97 |
| (0.77) | (0.12) | (0.11) | (0.12) | (0.07) | (0.27) | (0.52) | (0.48) | (0.04) | (1545.41) | (6.82) | |
| 3 (n = 14) | 8.89 | 1.68 | 1.61 | 1.78 | 4.05 | 5.28 | 1.42 | 0.55 | 0.86 | 27,789.62 | 205.77 |
| (0.38) | (0.16) | (0.14) | (0.20) | (0.20) | (0.18) | (0.09) | (0.35) | (0.02) | (1177.75) | (2.27) | |
| 4 (n = 12) | 9.13 | 1.55 | 1.49 | 1.66 | 4.23 | 5.66 | 1.14 | 2.14 | 0.81 | 28,393.93 | 209.88 |
| (0.37) | (0.08) | (0.08) | (0.08) | (0.32) | (0.12) | (0.13) | (0.47) | (0.03) | (1012.26) | (3.82) | |
| 5 (n = 22) | 9.50 | 1.67 | 1.65 | 1.70 | 3.95 | 5.68 | 1.11 | 3.40 | 0.81 | 29,140.54 | 215.75 |
| (0.35) 1 | (0.13) 1 | (0.12) 1 | (0.15) 1 | (0.53) | (0.25) 1,6 | (0.17) 1 | (0.26) 1 | (0.05) | (555.91) 1 | (11.31) 1 | |
| 6 (n = 14) | 9.43 | 1.67 | 1.62 | 1.75 | 3.70 | 4.03 | 1.39 | 3.39 | 0.70 | 28,833.79 | 200.22 |
| (0.36) 1 | (0.11) 1 | (0.10) 1 | (0.12) 1 | (0.29) | (0.44) 5 | (0.12) 1 | (0.14) 1 | (0.09) 1 | (2211.95) 1 | (7.05) | |
| 7 (n = 10) | 8.79 | 1.90 | 1.82 | 2.02 | 3.80 | 4.54 | 1.44 | 2.88 | 0.89 | 16,032.84 | 170.24 |
| (0.50) | (0.10) | (0.09) | (0.12) | (0.14) | (0.24) | (0.37) | (0.32) | (0.03) | (4152.00) | (9.74) | |
| 8 (n = 15) | 7.41 | 1.92 | 1.84 | 2.04 | 3.60 | 5.27 | 1.71 | 2.43 | 0.82 | 29,194.15 | 199.54 |
| (0.64) | (0.10) | (0.08) | (0.12) | (0.16) | (0.29) | (0.16) | (0.46) | (0.02) | (1639.97) | (5.92) | |
| Total (n = 108) | 8.52 | 1.80 | 1.74 | 1.90 | 3.88 | 5.05 | 1.60 | 2.30 | 0.82 | 26,855.30 | 199.19 |
| (1.20) | (0.23) | (0.21) | (0.27) | (0.35) | (0.63) | (0.74) | (1.09) | (0.07) | (4873.48) | (17.59) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molina-García, J.; García-Massó, X.; Estevan, I.; Queralt, A. Built Environment, Psychosocial Factors and Active Commuting to School in Adolescents: Clustering a Self-Organizing Map Analysis. Int. J. Environ. Res. Public Health 2019, 16, 83. https://doi.org/10.3390/ijerph16010083
Molina-García J, García-Massó X, Estevan I, Queralt A. Built Environment, Psychosocial Factors and Active Commuting to School in Adolescents: Clustering a Self-Organizing Map Analysis. International Journal of Environmental Research and Public Health. 2019; 16(1):83. https://doi.org/10.3390/ijerph16010083
Chicago/Turabian StyleMolina-García, Javier, Xavier García-Massó, Isaac Estevan, and Ana Queralt. 2019. "Built Environment, Psychosocial Factors and Active Commuting to School in Adolescents: Clustering a Self-Organizing Map Analysis" International Journal of Environmental Research and Public Health 16, no. 1: 83. https://doi.org/10.3390/ijerph16010083
APA StyleMolina-García, J., García-Massó, X., Estevan, I., & Queralt, A. (2019). Built Environment, Psychosocial Factors and Active Commuting to School in Adolescents: Clustering a Self-Organizing Map Analysis. International Journal of Environmental Research and Public Health, 16(1), 83. https://doi.org/10.3390/ijerph16010083