Compliance with Standard Precautions among Clinical Nurses: Validity and Reliability of the Italian Version of the Compliance with Standard Precautions Scale (CSPS-It)

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
- (1)
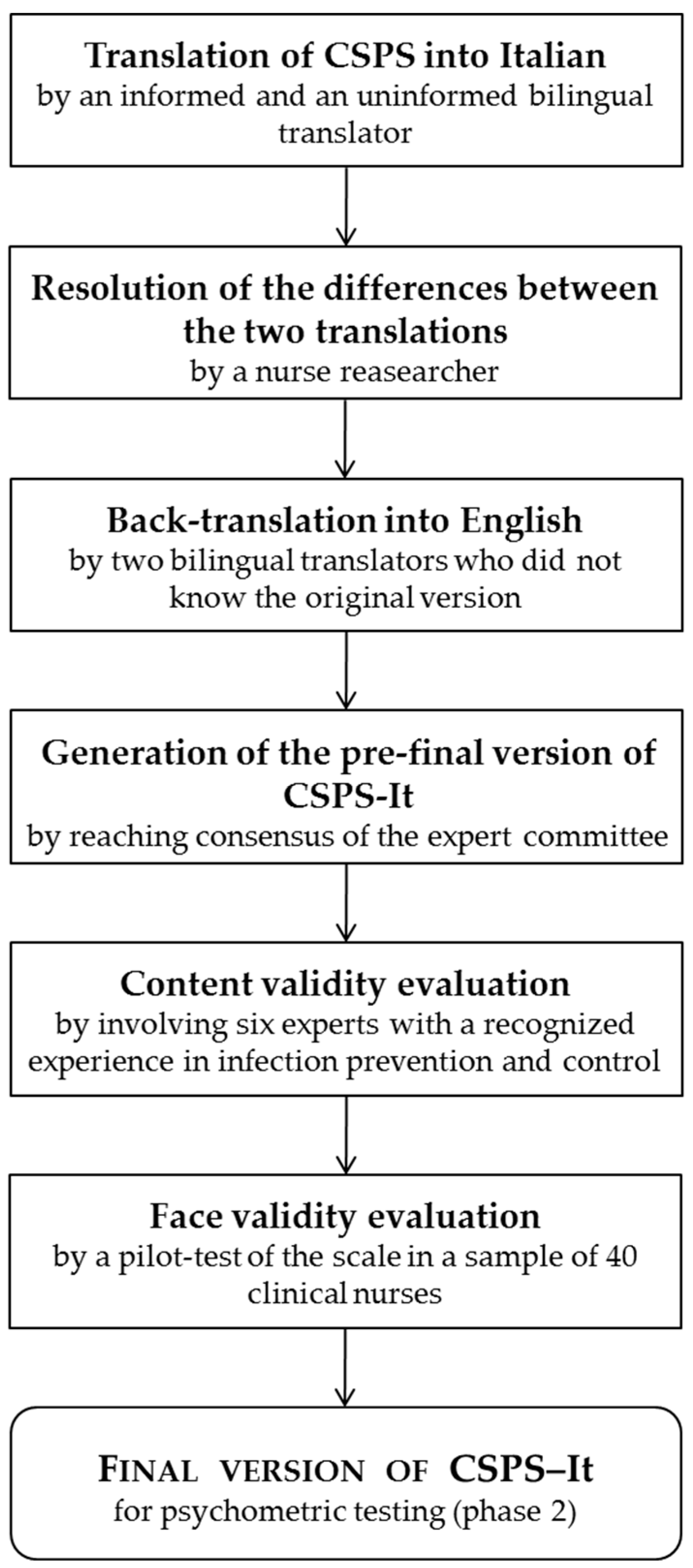
- Translation into Italian and cross-cultural adaptation of the CSPS (Figure 1); and
- (2)
- Validity and reliability evaluation of the CSPS–Italian version (CSPS-It).
2.2. Ethical Considerations
2.3. Instruments
2.4. Phase 1
2.4.1. Translation and Cross-Cultural Adaptation Process
2.4.2. Content Validity Evaluation
2.4.3. Face Validity Evaluation
2.5. Phase 2
2.5.1. Participants
2.5.2. Data Collection
2.5.3. Statistical Analysis
3. Results
3.1. Phase 1
3.1.1. Translation and Cross-Cultural Adaptation Process
3.1.2. Content and Face Validity of CSPS-It
3.2. Phase 2
3.2.1. Demographic Characteristics of the Sample
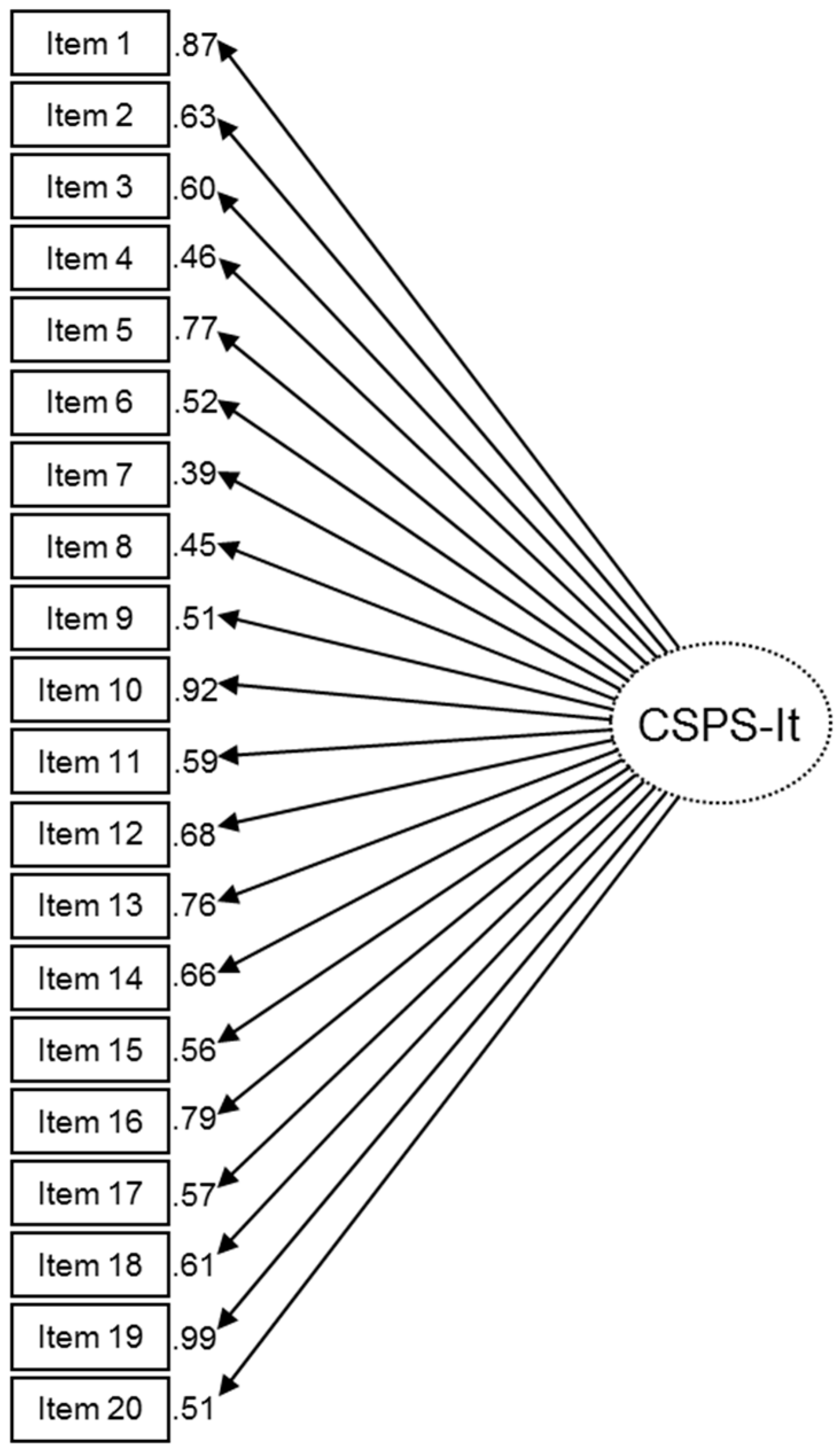
3.2.2. Confirmatory Factor Analysis
3.2.3. Hypothesis Testing
3.2.4. Reliability of CSPS-It
3.2.5. Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO Report on the Burden of Endemic Health Care-Associated Infection Worldwide. A Systematic Review of the Literature. 2011. Available online: www.who.int/gpsc/countrywork/burdenhcai/en/index.html (accessed on 17 September 2017).
- Bates, D.W.; Larizgoitia, I.; Prasopa-Plaizier, N.; Jha, A.K. Research Priority Setting Working Group of the WHO World Alliance for Patient Safety. Global priorities for patient safety research. BMJ 2009, 338, b1775. [Google Scholar] [CrossRef] [PubMed]
- Allegranzi, B.; Nejad, S.B.; Combescure, C.; Graafmans, W.; Attar, H.; Donaldson, L.; Pittet, D. Burden of endemic health-care-associated infection in developing countries: Systematic review and meta-analysis. Lancet 2011, 377, 228–241. [Google Scholar] [CrossRef]
- Andersson, A.E.; Bergh, I.; Karlsson, J.; Nilsson, K. Patients’ experiences of acquiring a deep surgical site infection: An interview study. Am. J. Infect. Control 2010, 38, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Siegel, J.D.; Rhinehart, E.; Jackson, M.; Chiarello, L. Health Care Infection Control Practices Advisory Committee. 2007 Guideline for isolation precautions: Preventing transmission of infectious agents in health care settings. Am. J. Infect. Control 2007, 35 (Suppl. 2), S65–S164. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Supplement I: Infection Control in Healthcare, Home, and Community Settings. Appendix II: Recommendations for Application of Standard Precautions for the Care of All Patients in Health Care Settings; CDC: Atlanta, GA, USA, 2004. Available online: http://www.cdc.gov/sars/guidance/I-infection/app1.pdf (accessed on 18 December 2017).
- World Health Organization. Regional Office for the Western Pacific. Practical Guidelines for Infection Control in Health Care Facilities; WHO Regional Office for the Western Pacific: Manila, Philippines, 2004; Available online: http://www.who.int/iris/handle/10665/206946 (accessed on 20 December 2017).
- Pereira, F.M.V.; Lam, S.C.; Chan, J.H.M.; Malaguti-Toffano, S.E.; Gir, E. Difference in compliance with Standard Precautions by nursing staff in Brazil versus Hong Kong. Am. J. Infect. Control 2015, 43, 769–772. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.C. Validation and cross-cultural pilot testing of compliance with standard precautions scale: Self-administered instrument for clinical nurses. Infect. Control Hosp. Epidemiol. 2014, 35, 547–555. [Google Scholar] [CrossRef]
- Stilo, A.; Troiano, G.; Melcarne, L.; Gioffrè, M.F.; Nante, N.; Messina, G.; Laganà, P. Hand washing in operating room: a procedural comparison. Epidemiol. Biostat. Public Health 2016, 13. [Google Scholar] [CrossRef]
- Adebayo, O.; Labiran, A.; Imarhiagbe, L. Standard Precautions in clinical practices: A review. Int. J. Health Sci. Res. 2015, 5, 521–528. [Google Scholar]
- Powers, D.; Armellino, D.; Dolansky, M.; Fitzpatrick, J. Factors influencing nurse compliance with Standard Precautions. Am. J. Infect. Control 2016, 44, 4–7. [Google Scholar] [CrossRef]
- Cheung, K.; Chan, C.K.; Chang, M.Y.; Chu, P.H.; Fung, W.F.; Kwan, K.C.; Lau, N.Y.; Li, W.K.; Mak, H.M. Predictors for compliance of standard precautions among nursing students. Am. J. Infect. Control 2015, 43, 729–734. [Google Scholar] [CrossRef]
- Kermode, M.; Jolley, D.; Langkham, B.; Thomas, M.S.; Holmes, W.; Gifford, S.M. Compliance with Universal/Standard Precautions among health care workers in rural north India. Am. J. Infect. Control 2005, 33, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; He, G.-P.; Zhou, J.-W.; Luo, Y. Factors impacting compliance with standard precautions in nursing, China. Int. J. Infect. Dis. 2010, 14, e1106–e1114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moralejo, D.; El Dib, R.; Prata, R.A.; Barretti, P.; Corrêa, I. Improving adherence to Standard Precautions for the control of health care-associated infections. Cochrane Database Syst. Rev. 2018, 26, CD010768. [Google Scholar] [CrossRef]
- Melia, K.M. When the body is past fixing: Caring for bodies, caring for people. J. Clin. Nurs. 2014, 23, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.M.; Kim, M.A.; Chung, Y.S.; Kim, N.C. Knowledge and performance of the universal precautions by nursing and medical students in Korea. Am. J. Infect. Control 2001, 29, 295–300. [Google Scholar] [CrossRef]
- Pratt, R.J.; Pellowe, C.M.; Wilson, J.A.; Loveday, H.P.; Harper, P.J.; Jones, S.R.L.J.; McDougall, C.; Wilcox, M.H. epic2: National evidence-based guidelines for preventing healthcare-associated infections in NHS hospitals in England. J. Hosp. Infect. 2007, 65 (Suppl. 1), S1–S64. [Google Scholar] [CrossRef]
- Hayes, R.B. Introduction in Compliance in Healthcare; John Hopkins: Baltimore, MD, USA, 1979. [Google Scholar]
- Valim, M.D.; Marziale, M.H.P.; Richart-Martínez, M.; Sanjuan-Quiles, Á. Instruments for evaluating compliance with infection control practices and factors that affect it: An integrative review. J. Clin. Nurs. 2014, 23, 1502–1519. [Google Scholar] [CrossRef]
- Chan, R.; Molassiotis, A.; Eunice, C.; Virene, C.; Becky, H.; Chit-ying, L.; Pauline, L.; Frances, S.; Ivy, Y. Nurses’ knowledge of and compliance with universal precautions in an acute care hospital. Int. J. Nurs. Stud. 2002, 39, 157–163. [Google Scholar] [CrossRef]
- Lam, S.C.; Fung, E.S.-S.; Hon, L.K.-Y.; Ip, M.P.-Y.; Chan, J.H.-T. Nursing students’ compliance with universal precautions in Hong Kong. J. Clin. Nurs. 2010, 19, 3247–3250. [Google Scholar] [CrossRef]
- Lam, S.C. Universal to standard precautions in disease prevention: Preliminary development of compliance scale for clinical nursing. Int. J. Nurs. Stud. 2011, 48, 1533–1539. [Google Scholar] [CrossRef]
- Cruz, J.P.; Colet, P.C.; Al-Otaibi, J.H.; Soriano, S.S.; Cacho, G.M.; Cruz, C.P. Validity and reliability assessment of the Compliance with Standard Precautions Scale Arabic version in Saudi nursing students. J. Infect. Public Health 2016, 9, 645–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, F.M.V.; Lam, S.C.; Gir, E. Cultural adaptation and reliability of the Compliance with Standard Precautions Scale (CSPS) for nurses in Brazil. Rev. Lat. Am. Enfermagem 2017, 25, e2850. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Sun, L.; Liu, G.; Zhang, X. Standard precautions among emergency department medical personnel: Status quo and analysis. Med. J. Qilu 2014, 29, 235–237. [Google Scholar]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. The content validity index: Are you sure you know what’s being reported? Critique and recommendations. Res. Nurs. Health 2006, 29, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Lynn, M.R. Determination and quantification of content validity. Nurs. Res. 1986, 35, 382–385. [Google Scholar] [CrossRef] [PubMed]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide Statistical Analysis with Latent Variables, 7th ed.; Muthén & Muthén—References—Scientific Research Publishing: Los Angeles, CA, USA, 1998–2012; Available online: http://www.scirp.org/(S(i43dyn45teexjx455qlt3d2q))/reference/ReferencesPapers.aspx?ReferenceID=1736196 (accessed on 28 July 2018).
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Nunnally, J.; Bernstein, I. Psychometric Theory; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Furr, R.M. Psychometrics: An Introduction, 3rd ed.; SAGE Publications, Inc.: Los Angeles, CA, USA, 2017; 568p. [Google Scholar]
- Efstathiou, G.; Papastavrou, E.; Raftopoulos, V.; Merkouris, A. Compliance of Cypriot nurses with standard precautions to avoid exposure to pathogens. Nurs. Health Sci. 2011, 13, 53–59. [Google Scholar] [CrossRef]
- Al-Rawajfah, O.M.; Hweidi, I.M.; Alkhalaileh, M.; Khader, Y.S.; Alshboul, S.A. Compliance of Jordanian registered nurses with infection control guidelines: A national population-based study. Am. J. Infect. Control 2013, 41, 1065–1068. [Google Scholar] [CrossRef]
- Colet, P.C.; Cruz, J.P.; Alotaibi, K.A.; Colet, M.K.A.; Islam, S.M.S. Compliance with standard precautions among baccalaureate nursing students in a Saudi university: A self-report study. J. Infect. Public Health 2017, 10, 421–430. [Google Scholar] [CrossRef] [Green Version]
- Streiner, D.L.; Norman, G.R.; Cairney, J. Health Measurement Scales: A Practical Guide to Their Development and Use, 5th ed.; Oxford University Press: New York, NY, USA, 2015. [Google Scholar]
- Arafat, S.M.Y.; Chowdhury, H.R.; Qusar, M.S.; Hafez, M.A. Cross Cultural Adaptation & Psychometric Validation of Research Instruments: A Methodological Review. J. Behav. Health 2016, 5, 129–136. [Google Scholar]



{kind=link}
{kind=link}
| Variable | n | % |
|---|---|---|
| Sex | ||
| Male | 37 | 14.6 |
| Female | 216 | 85.4 |
| Age | ||
| <25 | 24 | 9.5 |
| 26–30 | 71 | 28.1 |
| 31–35 | 76 | 30.0 |
| 36–40 | 46 | 18.2 |
| >40 | 36 | 14.2 |
| Education | ||
| Degree | 118 | 46.6 |
| Master | 106 | 41.9 |
| Master’s degree | 29 | 11.5 |
| Clinical experience (years) | ||
| <3 | 36 | 14.2 |
| 3–6 | 51 | 20.2 |
| 7–10 | 84 | 33.2 |
| 11–14 | 36 | 14.2 |
| >14 | 46 | 18.2 |
| Clinical setting | ||
| Adult medical-surgical | 143 | 56.5 |
| Intensive care unit | 19 | 7.5 |
| Operation theater | 44 | 17.4 |
| Outpatient units | 47 | 18.6 |
| SPs training * | ||
| Yes | 217 | 85.8 |
| No | 36 | 14.2 |
| Variable | Mean (SD) | p |
|---|---|---|
| SPs training * | ||
| Yes | 14.66 (3.08) | <0.001 |
| No | 9.92 (3.94) |
| Item | Frequency of Endorsement, % | Compliance Rate % | Corrected Item-Total Correlation | |||
|---|---|---|---|---|---|---|
| Never | Seldom | Sometimes | Always | |||
| 1. I wash my hands between patient contacts | 0.0 | 0.0 | 22.5 | 77.5 | 77.5 | 0.608 |
| 2. I only use water for hand washing | 74.3 | 19.8 | 5.9 | 0.00 | 74.3 | 0.444 |
| 3. I use alcohol hand rubs as an alternative if my hands are not visibly soiled | 0.0 | 0.8 | 33.6 | 65.6 | 65.6 | 0.426 |
| 4. I recap used needles after giving an injection | 77.1 | 19.8 | 3.2 | 0.0 | 77.1 | 0.323 |
| 5. I put used sharp articles into sharps boxes | 0.0 | 0.0 | 6.7 | 93.3 | 93.3 | 0.439 |
| 6. The sharps box is only disposed when it is full | 46.6 | 49.4 | 2.4 | 1.6 | 46.6 | 0.404 |
| 7. I remove PPE in a designated area | 0.0 | 1.6 | 32.8 | 65.6 | 65.6 | 0.311 |
| 8. I take a shower in case of extensive splashing even after I have put on PPE | 0.8 | 4.7 | 57.7 | 36.8 | 36.8 | 0.314 |
| 9. I cover my wound(s) or lesion(s) with waterproof dressing before patient contacts | 0.0 | 0.4 | 32.4 | 67.2 | 67.2 | 0.320 |
| 10. I wear gloves when I am exposed to body fluids, blood products, and any excretion of patients | 0.0 | 0.4 | 7.9 | 91.7 | 91.7 | 0.385 |
| 11. I change gloves between each patient contact | 0.0 | 0.0 | 11.1 | 88.9 | 88.9 | 0.364 |
| 12. I decontaminate my hands immediately after removal of gloves | 0.0 | 1.2 | 33.6 | 65.2 | 65.2 | 0.495 |
| 13. I wear a surgical mask alone or in combination with goggles, face shield, and apron whenever there is a possibility of a splash or splatter | 0.0 | 1.6 | 39.5 | 58.9 | 58.9 | 0.516 |
| 14. My mouth and nose are covered when I wear a mask | 0.0 | 0.4 | 7.1 | 92.5 | 92.5 | 0.342 |
| 15. I reuse mask or disposable PPE | 71.9 | 26.1 | 2.0 | 0.0 | 71.9 | 0.422 |
| 16. I wear a gown or apron when exposed to blood, body fluids, or any patient excretions | 0.0 | 1.6 | 45.5 | 53.0 | 53.0 | 0.580 |
| 17. Waste contaminated with blood, body fluids, secretion, and excretion are placed in red plastic bags irrespective of patient’s infective status | 0.4 | 1.6 | 38.7 | 59.3 | 59.3 | 0.443 |
| 18. I decontaminate surfaces and equipment after use | 1.2 | 2.4 | 40.3 | 56.1 | 56.1 | 0.498 |
| 19. I wear gloves to decontaminate used equipment with visible soils | 0.0 | 0.0 | 7.9 | 92.1 | 92.1 | 0.443 |
| 20. I clean up spillage of blood or other body fluid immediately with disinfectants | 1.2 | 4.0 | 30.0 | 64.8 | 64.8 | 0.391 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donati, D.; Biagioli, V.; Cianfrocca, C.; De Marinis, M.G.; Tartaglini, D. Compliance with Standard Precautions among Clinical Nurses: Validity and Reliability of the Italian Version of the Compliance with Standard Precautions Scale (CSPS-It). Int. J. Environ. Res. Public Health 2019, 16, 121. https://doi.org/10.3390/ijerph16010121
Donati D, Biagioli V, Cianfrocca C, De Marinis MG, Tartaglini D. Compliance with Standard Precautions among Clinical Nurses: Validity and Reliability of the Italian Version of the Compliance with Standard Precautions Scale (CSPS-It). International Journal of Environmental Research and Public Health. 2019; 16(1):121. https://doi.org/10.3390/ijerph16010121
Chicago/Turabian StyleDonati, Daniele, Valentina Biagioli, Claudia Cianfrocca, Maria Grazia De Marinis, and Daniela Tartaglini. 2019. "Compliance with Standard Precautions among Clinical Nurses: Validity and Reliability of the Italian Version of the Compliance with Standard Precautions Scale (CSPS-It)" International Journal of Environmental Research and Public Health 16, no. 1: 121. https://doi.org/10.3390/ijerph16010121