Surveying Alcohol Outlet Density in Four Neighborhoods of Beirut Lebanon: Implications for Future Research and National Policy

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
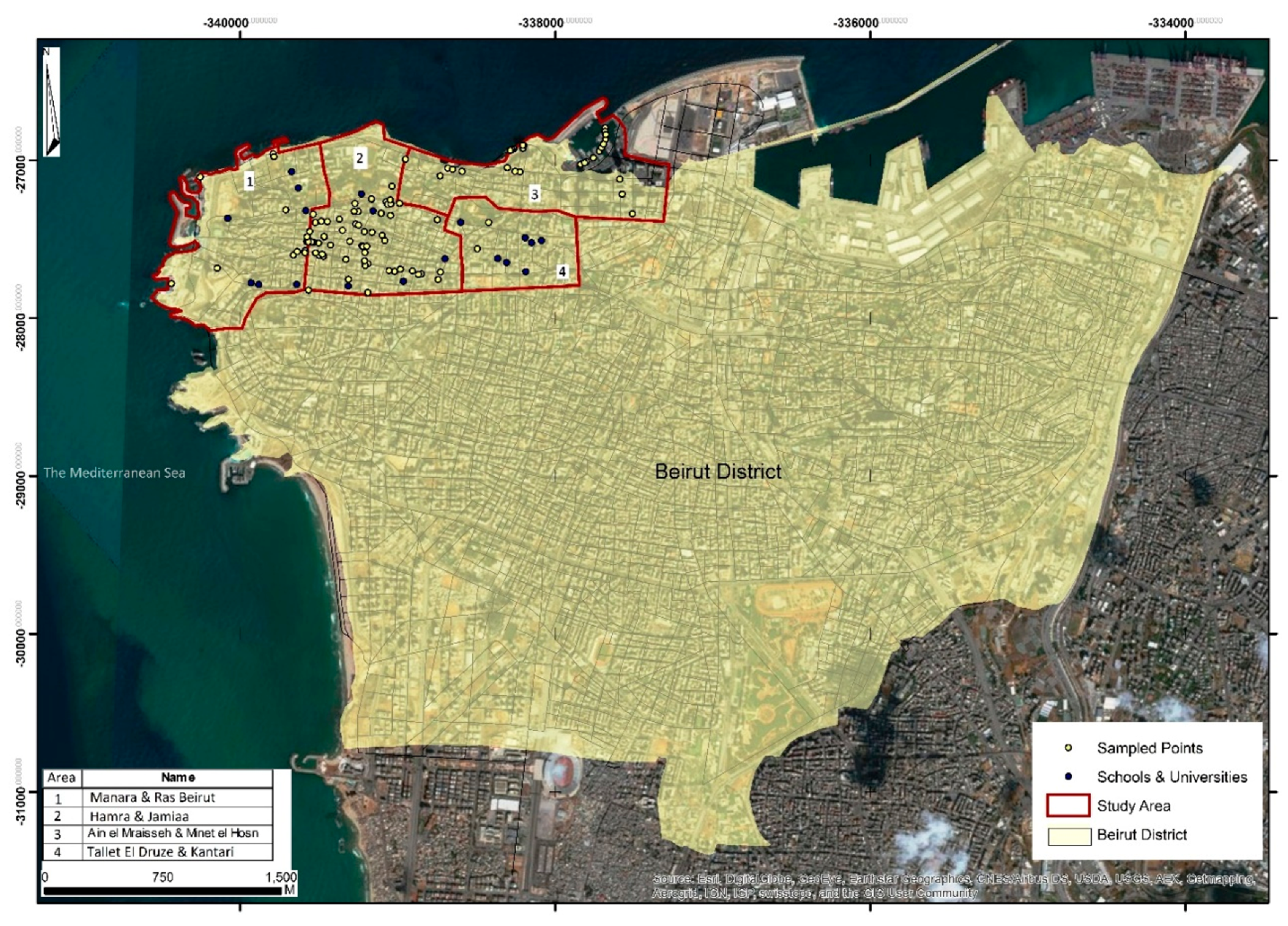
2.1. Field Work
2.2. Data Analysis
3. Results
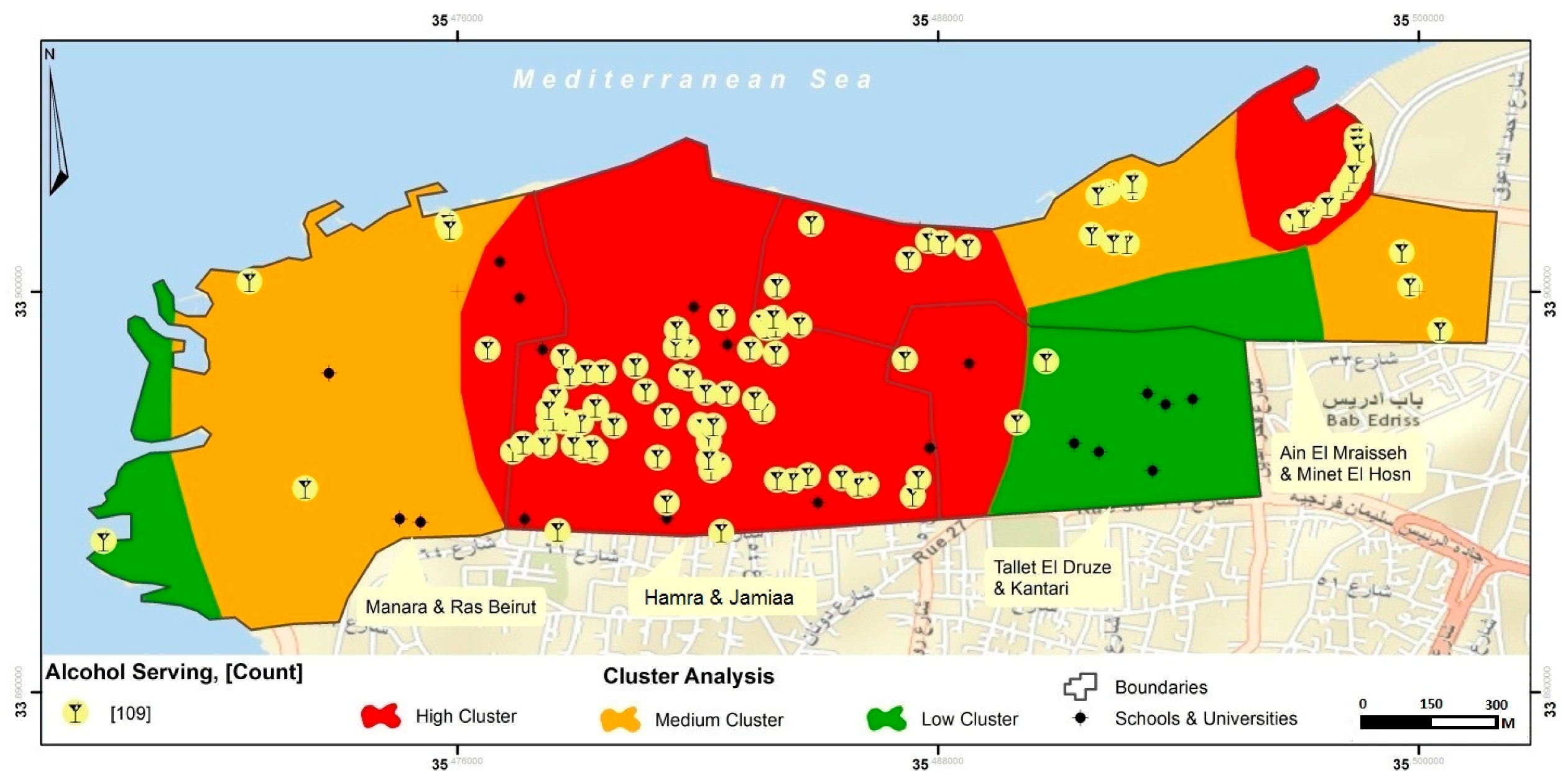
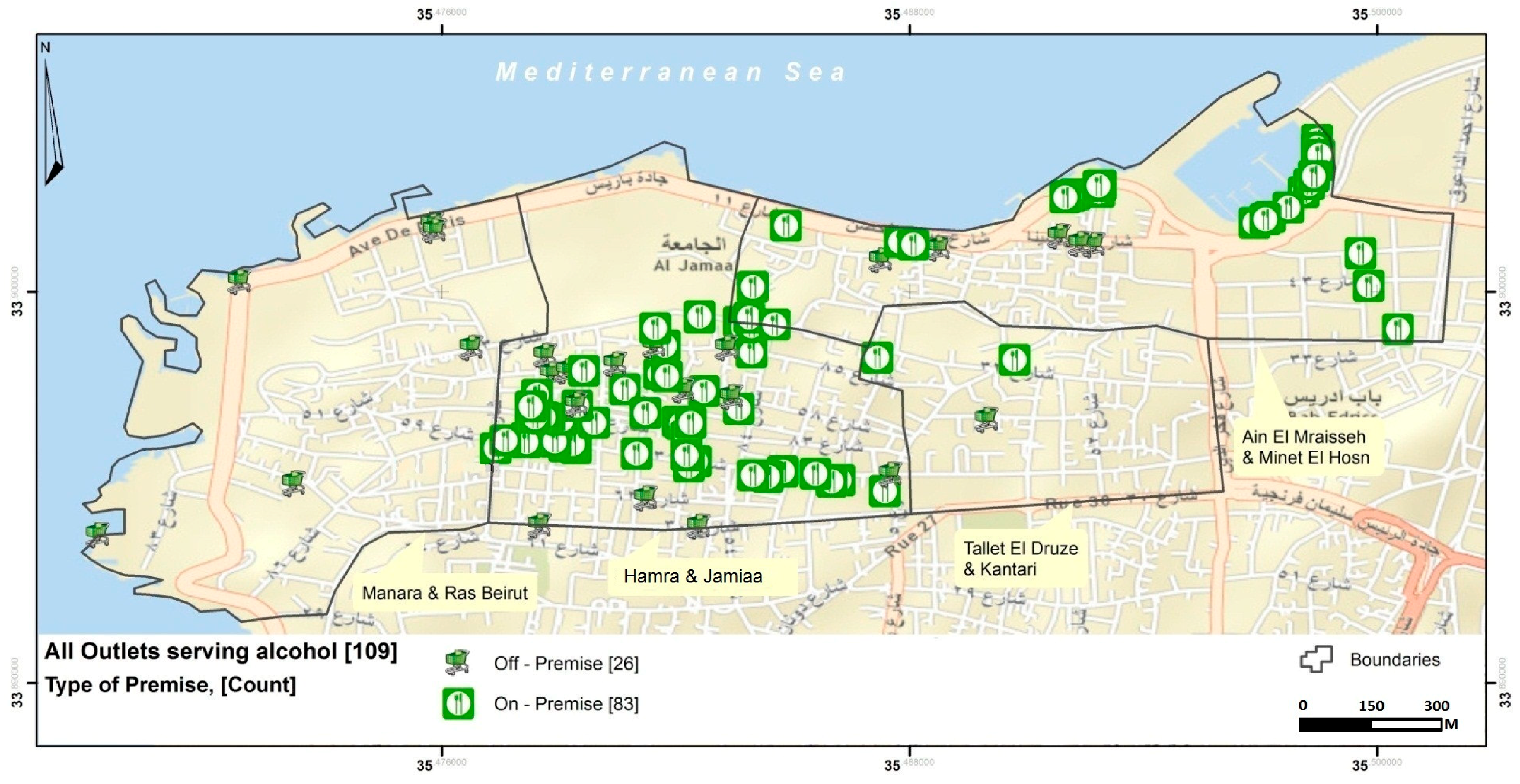
3.1. Density of Outlets
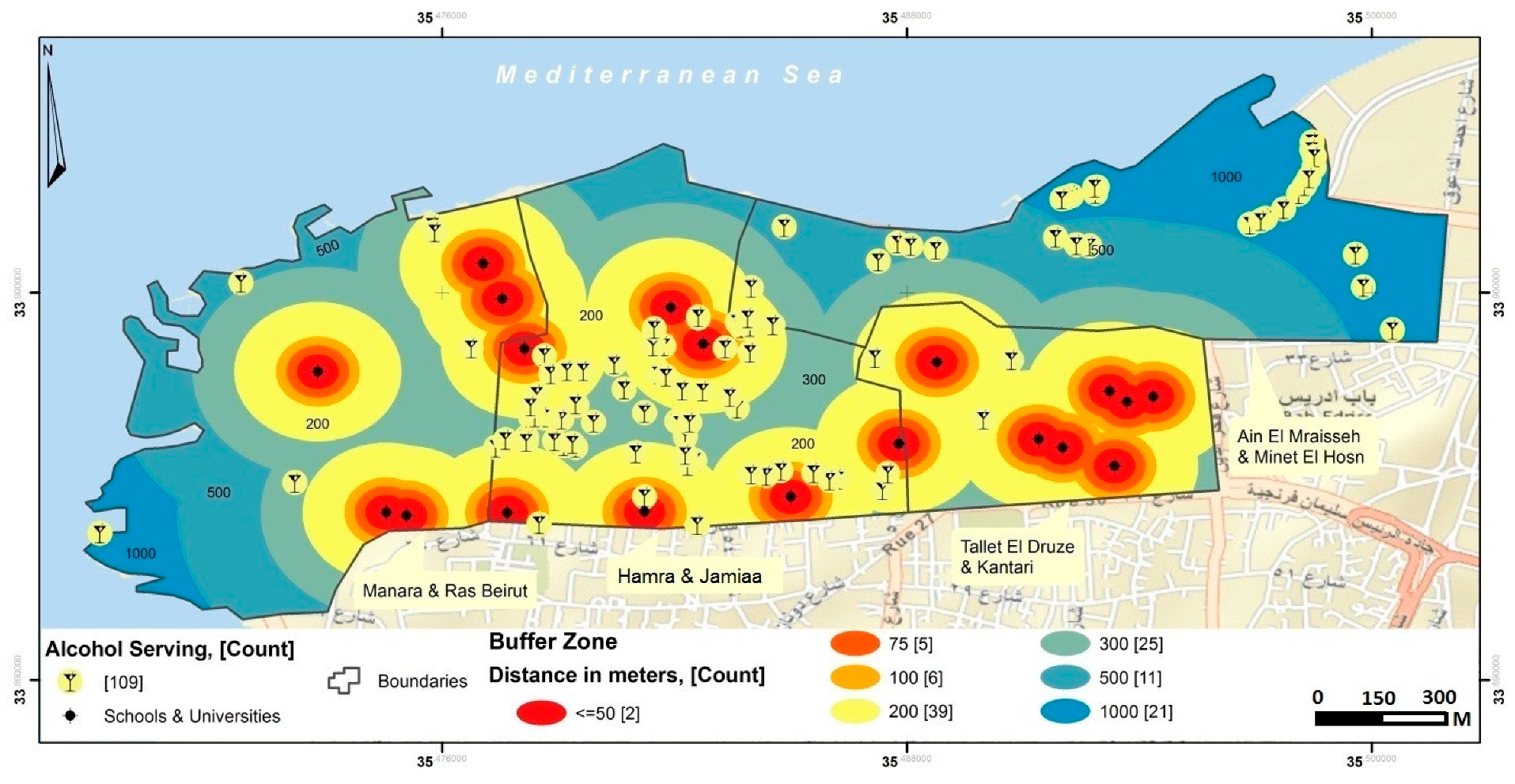
3.2. Distances from Educational Institutions
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mokdad, A.H.; Forouzanfar, M.H.; Daoud, F.; Mokdad, A.A.; El Bcheraoui, C.; Moradi-Lakeh, M.; Kyu, H.H.; Barber, R.M.; Wagner, J.; Cercy, K. Global burden of diseases, injuries, and risk factors for young people’s health during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2016, 387, 2383–2401. [Google Scholar] [CrossRef]
- Ansari, W.E.; Stock, C.; Mills, C. Is alcohol consumption associated with poor academic achievement in university students? Int. J. Prev. Med. 2013, 1, 1175–1188. [Google Scholar]
- Groves, S.A.; Stanley, B.H.; Sher, L. Ethnicity and the relationship between adolescent alcohol use and suicidal behavior. Int. J. Adolesc. Med. Health 2007, 19, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Shield, K.D.; Joharchi, N.; Shuper, P.A. Alcohol consumption and the intention to engage in unprotected sex: Systematic review and meta-analysis of experimental studies. Addiction 2012, 107, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Grunbaum, J.A.; Kann, L.; Kinchen, S.; Ross, J.; Hawkins, J.; Lowry, R.; Harris, W.A.; McManus, T.; Chyen, D.; Collins, J. Youth Risk Behavior Surveillance—United States, 2003; Morbidity and Mortality Weekly Report; Surveillance Summaries: Washington, DC, USA, 2004; Volume 53, pp. 1–96. [Google Scholar]
- Newbury-Birch, D. Impact of Alcohol Consumption on Young People: A Systematic Review of Published Reviews. Available online: https://www.drugsandalcohol.ie/12292/3/Review_of_existing_reviews.pdf (accessed on 6 September 2018).
- DeWit, D.J.; Adlaf, E.M.; Offord, D.R.; Ogborne, A.C. Age at first alcohol use: A risk factor for the development of alcohol disorders. Am. J. Psychiatry 2000, 157, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Hingson, R.W.; Heeren, T.; Winter, M.R. Age at drinking onset and alcohol dependence: Age at onset, duration, and severity. Arch. Pediatr. Adolesc. Med. 2006, 160, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Grant, B.F.; Dawson, D.A. Age at onset of alcohol use and its association with DSM-IV alcohol abuse and dependence: Results from the National Longitudinal Alcohol Epidemiologic Survey. J. Subst. Abuse 1997, 9, 103–110. [Google Scholar] [CrossRef]
- Rehm, J.; Mathers, C.; Popova, S.; Thavorncharoensap, M.; Teerawattananon, Y.; Patra, J. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet 2009, 373, 2223–2233. [Google Scholar] [CrossRef]
- Babor, T.; Caetano, R.; Casswell, S.; Edwards, G.; Giesbrecht, N.; Graham, K.; Grube, J.; Hill, L.; Holder, H.; Homel, R.; et al. Alcohol: No Ordinary Commodity—A summary of the second edition. Addiction 2010, 105, 769–779. [Google Scholar]
- Smith, L.A.; Foxcroft, D.R. The effect of alcohol advertising, marketing and portrayal on drinking behaviour in young people: Systematic review of prospective cohort studies. BMC Public Health 2009, 9, 51. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Status Report on Alcohol and Health 2014. 2014. Available online: http://apps.who.int/iris/bitstream/handle/10665/112736/9789240692763_eng.pdf;jsessionid=0C51E26D30156690F4897DFED5064122?sequence=1 (accessed on 6 September 2018).
- Anderson, P.; Chisholm, D.; Fuhr, D.C. Effectiveness and cost-effectiveness of policies and programmes to reduce the harm caused by alcohol. Lancet 2009, 373, 2234–2246. [Google Scholar] [CrossRef]
- Casswell, S.; Thamarangsi, T. Reducing harm from alcohol: Call to action. Lancet 2009, 373, 2247–2257. [Google Scholar] [CrossRef]
- Sparks, M.; Jernigan, D.H.; Mosher, J.F. Regulating Alcohol Outlet Density: An Action Guide. 2011. Available online: http://www.camy.org/_docs/resources/reports/alcohol-availability/strategizer-55-regulating-alcohol-outlet-density.pdf (accessed on 6 September 2018).
- Task Force on Community Preventive Services. Recommendations for reducing excessive alcohol consumption and alcohol-related harms by limiting alcohol outlet density. Am. J. Prev. Med. 2009, 37, 570–571.
- Campbell, C.A.; Hahn, R.A.; Elder, R.; Brewer, R.; Chattopadhyay, S.; Fielding, J.; Naimi, T.S.; Toomey, T.; Lawrence, B.; Middleton, J.C. The effectiveness of limiting alcohol outlet density as a means of reducing excessive alcohol consumption and alcohol-related harms. Am. J. Prev. Med. 2009, 37, 556–569. [Google Scholar] [CrossRef] [PubMed]
- Livingston, M.; Chikritzhs, T.; Room, R. Changing the density of alcohol outlets to reduce alcohol-related problems. Drug Alcohol Rev. 2007, 26, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Kuntsche, E.; Kuendig, H.; Gmel, G. Alcohol outlet density, perceived availability and adolescent alcohol use: A multilevel structural equation model. J. Epidemiol. Community Health 2008, 62, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Reboussin, B.A.; Song, E.Y.; Wolfson, M. The impact of alcohol outlet density on the geographic clustering of underage drinking behaviors within census tracts. Alcohol Clin. Exp. Res. 2011, 35, 1541–4549. [Google Scholar] [CrossRef] [PubMed]
- Rowland, B.; Toumbourou, J.W.; Livingston, M. The Association of Alcohol Outlet Density With Illegal Underage Adolescent Purchasing of Alcohol. J. Adolesc. Health 2015, 56, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Rowland, B.C.; Hall, J.K.; Kremer, P.J.; Miller, P.G.; Toumbourou, J.W. Underage purchasing of alcohol from packaged liquor outlets: An Australian study. Health Promot. Int. 2016, 32, 790–799. [Google Scholar] [CrossRef] [PubMed]
- Rowland, B.; Evans-Whipp, T.; Hemphill, S.; Leung, R.; Livingston, M.; Toumbourou, J. The density of alcohol outlets and adolescent alcohol consumption: An Australian longitudinal analysis. Health Place 2016, 37, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Rowland, B.; Toumbourou, J.; Satyen, L.; Tooley, G.; Hall, J.; Livingston, M.; Williams, J. Associations between alcohol outlet densities and adolescent alcohol consumption: A study in Australian students. Addict. Behav. 2014, 39, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Community Anti-Drug Coalitions of America. Distance Limitations Applied to New Alcohol Outlets Near Universities, Colleges, and Primary and Secondary Schools. 2015. Available online: https://www.myctb.org/wst/iowapfs/Shared%20Documents/Implementation/Alcohol%20Outlet%20Density/Distance_limitations_applied_to_new_alcohol_outlets.pdf (accessed on 6 September 2018).
- Chen, M.J.; Grube, J.W.; Gruenewald, P.J. Community alcohol outlet density and underage drinking. Addiction 2010, 105, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Hahn, R.A.; Middleton, J.C.; Elder, R.; Brewer, R.; Fielding, J.; Naimi, T.S.; Toomey, T.L.; Chattopadhyay, S.; Lawrence, B.; Campbell, C.A. Effects of alcohol retail privatization on excessive alcohol consumption and related harms: A community guide systematic review. Am. J. Prev. Med. 2012, 42, 418–427. [Google Scholar] [CrossRef] [PubMed]
- Treno, A.J.; Grube, J.W.; Martin, S.E. Alcohol availability as a predictor of youth drinking and driving: A hierarchical analysis of survey and archival data. Alcohol. Clin. Exp. Res. 2003, 27, 835–840. [Google Scholar] [CrossRef] [PubMed]
- Richardson, E.; Hill, S.; Mitchell, R.; Pearce, J.; Shortt, N. Is local alcohol outlet density related to alcohol-related morbidity and mortality in Scottish cities? Health Place 2015, 33, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Scribner, R.; Carlin, B.; Theall, K.; Simonsen, N.; Ghosh-Dastidar, B.; Cohen, D.; Mason, K. Multilevel spatio-temporal dual changepoint models for relating alcohol outlet destruction and changes in neighbourhood rates of assaultive violence. Geospat. Health 2008, 2, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Hatcher, B.; Clarkson, L.; Holt, J.; Bagchi, S.; Kanny, D.; Brewer, R.D. Changes in Density of On-Premises Alcohol Outlets and Impact on Violent Crime, Atlanta, Georgia, 1997–2007. Prev. Chronic Dis. 2015, 12, 140317. [Google Scholar] [CrossRef] [PubMed]
- Popova, S.; Giesbrecht, N.; Bekmuradov, D.; Patra, J. Hours and days of sale and density of alcohol outlets: Impacts on alcohol consumption and damage: A systematic review. Alcohol Alcohol. 2009, 44, 500–516. [Google Scholar] [CrossRef] [PubMed]
- Österberg, E.; Karlsson, T. Alcohol Policies in EU Member States and Norway. 2002. Available online: https://ec.europa.eu/health/ph_projects/1998/promotion/fp_promotion_1998_a01_27_en.pdf (accessed on 6 September 2018).
- Ghandour, L.; Chalak, A.; El-Aily, A.; Yassin, N.; Nakkash, R.; Tauk, M.; El Salibi, N.; Heffron, M.; Afifi, R. Alcohol consumption in the Arab region: What do we know, why does it matter, and what are the policy implications for youth harm reduction? Int. J. Drug Policy 2016, 28, 10–33. [Google Scholar] [CrossRef] [PubMed]
- Ghandour, L.; Afifi, R.; Fares, S.; El-Salibi, N.; Rady, A. Time trends and policy gaps: The case of alcohol misuse among adolescents in Lebanon. Subst. Use Misuse 2015, 50, 1826–1839. [Google Scholar] [CrossRef] [PubMed]
- Zahlan, L.; Ghandour, L.; Yassin, N.; Afifi, R.; Martins, S.S. Double trouble: Exploring the association between waterpipe tobacco smoking and the nonmedical use of psychoactive prescription drugs among adolescents. Drug Alcohol Depend. 2014, 145, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Ghandour, L.A.; El Sayed, D.S.; Martins, S.S. Prevalence and patterns of commonly abused psychoactive prescription drugs in a sample of university students from Lebanon: An opportunity for cross-cultural comparisons. Drug Alcohol Depend. 2012, 121, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Halonen, J.I.; Kivimäki, M.; Virtanen, M.; Pentti, J.; Subramanian, S.V.; Kawachi, I.; Vahtera, J. Living in proximity of a bar and risky alcohol behaviours: A longitudinal study. Addiction 2013, 108, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Young, R.; Macdonald, L.; Ellaway, A. Associations between proximity and density of local alcohol outlets and alcohol use among Scottish adolescents. Health Place 2013, 19, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Bowers, Y.; Rendall-Mkosi, K.; Davids, A.; Nel, E.; Jacobs, N.; London, L. Liquor outlet density, deprivation and implications for foetal alcohol syndrome prevention in the Bergriver municipality in the Western Cape, South Africa. S. Afr. Geogr. J. 2014, 96, 153–165. [Google Scholar] [CrossRef]
- Van der Horst, K.; Oenema, A.; van de Looij-Jansen, P.; Brug, J. The ENDORSE study: Research into environmental determinants of obesity related behaviors in Rotterdam schoolchildren. BMC Public Health 2008, 8, 142. [Google Scholar]
- Thaikla, K.; Jiraporncharoen, W.; Semmahasak, S.; Likhitsathian, S.; Angkurawaranon, C. Recent trends in alcohol outlet density, distances from educational institutions and sales campaigns in Chiang Mai Municipality (Metropolitan), Thailand: Should we be worried for our youths? Alcohol Alcohol. 2015, 51, 210–214. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Strategy to Reduce the Harmful Use of Alcohol; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Matheson, F.I.; Creatore, M.I.; Gozdyra, P.; Park, A.L.; Ray, J.G. A population-based study of premature mortality in relation to neighbourhood density of alcohol sales and cheque cashing outlets in Toronto, Canada. BMJ Open 2014, 4, e006032. [Google Scholar] [CrossRef] [PubMed]
- Ahern, J.; Margerison-Zilko, C.; Hubbard, A.; Galea, S. Alcohol outlets and binge drinking in urban neighborhoods: The implications of nonlinearity for intervention and policy. Am. J. Public Health 2013, 103, e81–e87. [Google Scholar] [CrossRef] [PubMed]
- Laranjeira, R.; Hinkly, D. Evaluation of Alcohol Outlet Density and Its Relation With Violence. Revista de Saude Publica 2002, 36, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Kypri, K.; Bell, M.L.; Hay, G.C.; Baxter, J. Alcohol outlet density and university student drinking: A national study. Addiction 2008, 103, 1131–1138. [Google Scholar] [CrossRef] [PubMed]
- Weitzman, E.R.; Folkman, A.; Folkman, M.K.L.; Wechsler, H. The relationship of alcohol outlet density to heavy and frequent drinking and drinking-related problems among college students at eight universities. Health Place 2003, 9, 1–6. [Google Scholar] [CrossRef]
- Scribner, R.A.; Mason, K.E.; Simonsen, N.R.; Theall, K.; Chotalia, J.; Johnson, S.; Schneider, S.K.; DeJong, W. An Ecological Analysis of Alcohol-Outlet Density and Campus-Reported Violence at 32 US Colleges. J. Stud. Alcohol Drugs 2010, 71, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Treno, A.J.; Ponicki, W.R.; Remer, L.G.; Gruenewald, P.J. Alcohol Outlets, Youth Drinking, and Self-Reported Ease of Access to Alcohol: A Constraints and Opportunities Approach. Alcohol. Clin. Exp. Res. 2008, 32, 1372–1379. [Google Scholar] [CrossRef] [PubMed]
- Azar, D.; White, V.; Coomber, K.; Faulkner, A.; Livingston, M.; Chikritzhs, T.; Room, R.; Wakefield, M. The association between alcohol outlet density and alcohol use among urban and regional Australian adolescents. Addiction 2016, 111, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Livingston, M. Alcohol outlet density: The challenge of linking research findings to policy. Aust. Epidemiol. 2014, 21, 22–24. [Google Scholar]
- CDC. Guide for Measuring Alcohol Outlet Density. 2017. Available online: https://www.cdc.gov/alcohol/pdfs/CDC-Guide-for-Measuring-Alcohol-Outlet-Density.pdf (accessed on 6 September 2018).
- Bloom, D.E.; Chisholm, D.; Jané-Llopis, E.; Prettner, K.; Stein, A.; Feigl, A. From Burden to “Best Buys”: Reducing the Economic Impact of Non-Communicable Disease in Low-and Middle-Income Countries. 2011. Available online: http://www.who.int/nmh/publications/best_buys_summary.pdf (accessed on 6 September 2018).
- Toomey, T.L.; Wagenaar, A.C. Environmental policies to reduce college drinking: Options and research findings. J. Stud. Alcohol 2002, 14, 193–205. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outlet Characteristics | All (n = 109) | On-Premise n = 83 (76%) | Off-Premise n = 26 (24%) |
|---|---|---|---|
| Type of outlet n (%) | |||
| Large market/store or Supermarket | 2 (2%) | - | 2 (8%) |
| Mini-market/small grocery store | 20 (18%) | - | 20 (77%) |
| Convenience stores (gas station) | 2 (2%) | - | 2 (8%) |
| Liquor stores | 2 (2%) | - | 2 (8%) |
| Restaurants | 60 (55%) | 60 (72%) | - |
| Pubs/Bars | 23 (21%) | 23 (28%) | - |
| Type of drinks sold n (%) | |||
| Spirits (whiskey, Arak, rum, tequila, vodka, et al.) | 78 (72%) | 57 (37%) | 44 (68%) |
| Beer | 103 (95%) | 80 (51%) | 23 (35%) |
| Wine | 95 (87%) | 75 (48%) | 20 (31%) |
| Mixed energy alcoholic drinks | 48 (44%) | 24 (15%) | 24 (37%) |
| More than one type | 96 (88%) | 73 (88%) | 23 (88%) |
| All types | 42 (39%) | 24 (29%) | 18 (69%) |
| Proximity to educational institutions in meters n (%) | |||
| ≤100 | 13 (12%) | 7 (8%) | 6 (23%) |
| ≤200 | 52 (48%) | 37 (71%) | 15 (29%) |
| ≤300 | 77 (70%) | 59 (77%) | 18 (23%) |
| Display “No alcohol sale for <18” sign | |||
| Yes | 6 (5.5%) | 6 (7%) | 0 |
| No | 103 (94.5%) | 77 (93%) | 26 (100%) |
| Neighborhood | Area in km2 | Number of Outlets | Number of Alcohol Outlets | Outlet Density (Number of outlets/km2) | ||||
|---|---|---|---|---|---|---|---|---|
| All | On-Premise | Off-Premise | All | On-Premise | Off-Premise | |||
| Area 1 Manara & Ras Beirut | 0.89 | 26 | 6 | 0 | 6 | 29.35 | 0 | 6.74 |
| Area 2 Hamra & Jamiaa | 0.86 | 144 | 68 | 55 | 13 | 80.95 | 63.95 | 15.11 |
| Area 3 Ain ElMraisseh & Minet El Hosn | 0.64 | 44 | 32 | 26 | 6 | 50.37 | 40.62 | 9.37 |
| Area 4 Tallet El druze & Kantari | 0.38 | 7 | 3 | 2 | 1 | 18.30 | 5.26 | 2.63 |
| Total | 2.75 | 221 | 109 | 83 | 26 | 39.63 | 30.18 | 9.45 |
| Proximity of Alcohol Outlets to Schools and Universities | All Educational Institutions | |
|---|---|---|
| Schools (n = 12) | Universities (n = 7) | |
| The shortest distance in meters to an educational institution by outlet type | ||
| On premise alcohol outlet | 74.2 | 71.1 |
| Off premise alcohol outlet | 51.7 | 42.6 |
| The shortest distance in meters to an educational institution by area | ||
| Area 1 Ras Beirut & Manara | 127.37 | 146.9 |
| Area 2 Hamra & Jamiaa | 51.7 | 42.6 |
| Area 2 Ain Al Mraisseh & Minet El Hosn | 174.6 | 199.5 |
| Area 4 Tallet Jounblat & Kantari | 143.4 | 148.8 |
| Number of outlets […….] meters away from educational institutions n (%) | ||
| ≤75 | 3 (3%) | 4 (4%) |
| ≤100 | 9 (8%) | 6 (6%) |
| ≤200 | 37 (34%) | 32 (29%) |
| ≤300 | 72 (66%) | 66 (61%) |
| Outlet Characteristics | Outlets ≤100 m Away from Schools n (%) | Outlets >100 m Away from Schools n (%) | p-Value |
|---|---|---|---|
| Type of drinks sold | 0.296 | ||
| Spirits | 0 | 1 (1%) | |
| Beer | 2 (15%) | 5 (5%) | |
| Wine | 0 | 2 (2%) | |
| Mixed energy alcoholic drinks | 1 (33%) | 2 (2%) | |
| More than one type | 10 (77%) | 86 (90%) | |
| Type of outlet | 0.076 | ||
| On-premise | 6 (46%) | 20 (21%) | |
| Off-premise | 7 (54%) | 76 (79%) | |
| Display “No sale for <18’ sign” | |||
| Yes | 0 | 6 (6%) | 1.000 |
| No | 13 (100%) | 90 (94%) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakkash, R.; Ghandour, L.A.; Anouti, S.; Nicolas, J.; Chalak, A.; Yassin, N.; Afifi, R. Surveying Alcohol Outlet Density in Four Neighborhoods of Beirut Lebanon: Implications for Future Research and National Policy. Int. J. Environ. Res. Public Health 2018, 15, 2006. https://doi.org/10.3390/ijerph15092006
Nakkash R, Ghandour LA, Anouti S, Nicolas J, Chalak A, Yassin N, Afifi R. Surveying Alcohol Outlet Density in Four Neighborhoods of Beirut Lebanon: Implications for Future Research and National Policy. International Journal of Environmental Research and Public Health. 2018; 15(9):2006. https://doi.org/10.3390/ijerph15092006
Chicago/Turabian StyleNakkash, Rima, Lilian A. Ghandour, Sirine Anouti, Jessika Nicolas, Ali Chalak, Nasser Yassin, and Rima Afifi. 2018. "Surveying Alcohol Outlet Density in Four Neighborhoods of Beirut Lebanon: Implications for Future Research and National Policy" International Journal of Environmental Research and Public Health 15, no. 9: 2006. https://doi.org/10.3390/ijerph15092006
APA StyleNakkash, R., Ghandour, L. A., Anouti, S., Nicolas, J., Chalak, A., Yassin, N., & Afifi, R. (2018). Surveying Alcohol Outlet Density in Four Neighborhoods of Beirut Lebanon: Implications for Future Research and National Policy. International Journal of Environmental Research and Public Health, 15(9), 2006. https://doi.org/10.3390/ijerph15092006