The Role of Psychosocial Stress on a Family-Based Treatment for Adolescents with Problematic Behaviors


Abstract
1. Introduction
1.1. Interventions Involving Adolescents with Problematic Behaviors. The Scene-Based Psychodramatic Family Therapy
1.2. Present Study
2. Materials and Methods
2.1. Study Design
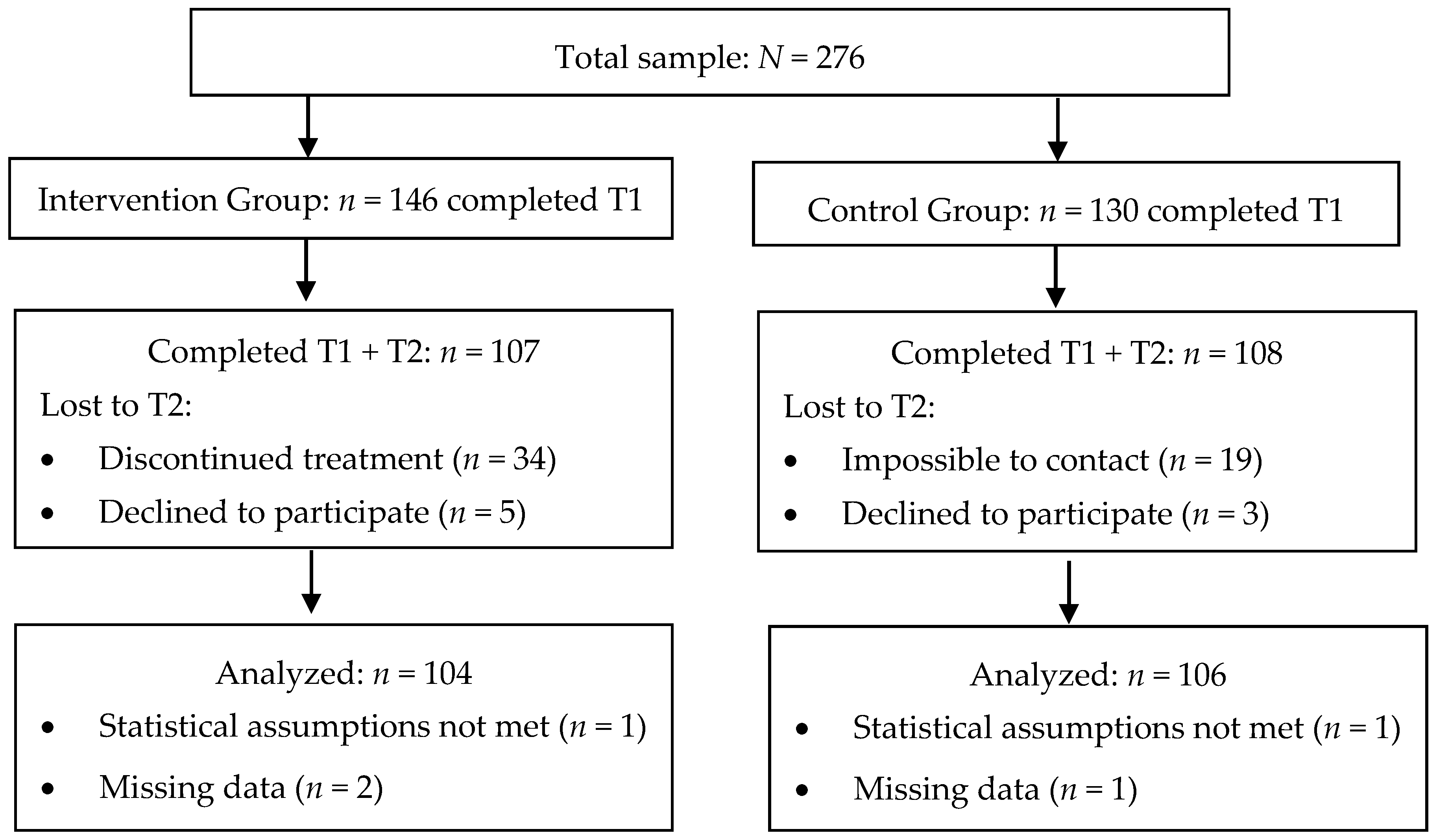
2.2. Participants
2.3. Measures
2.4. Procedure
2.5. Data Analyses
3. Results
3.1. Psychosocial Adjustment of Adolescents with Problematic Behaviors According to Their Stress Profiles
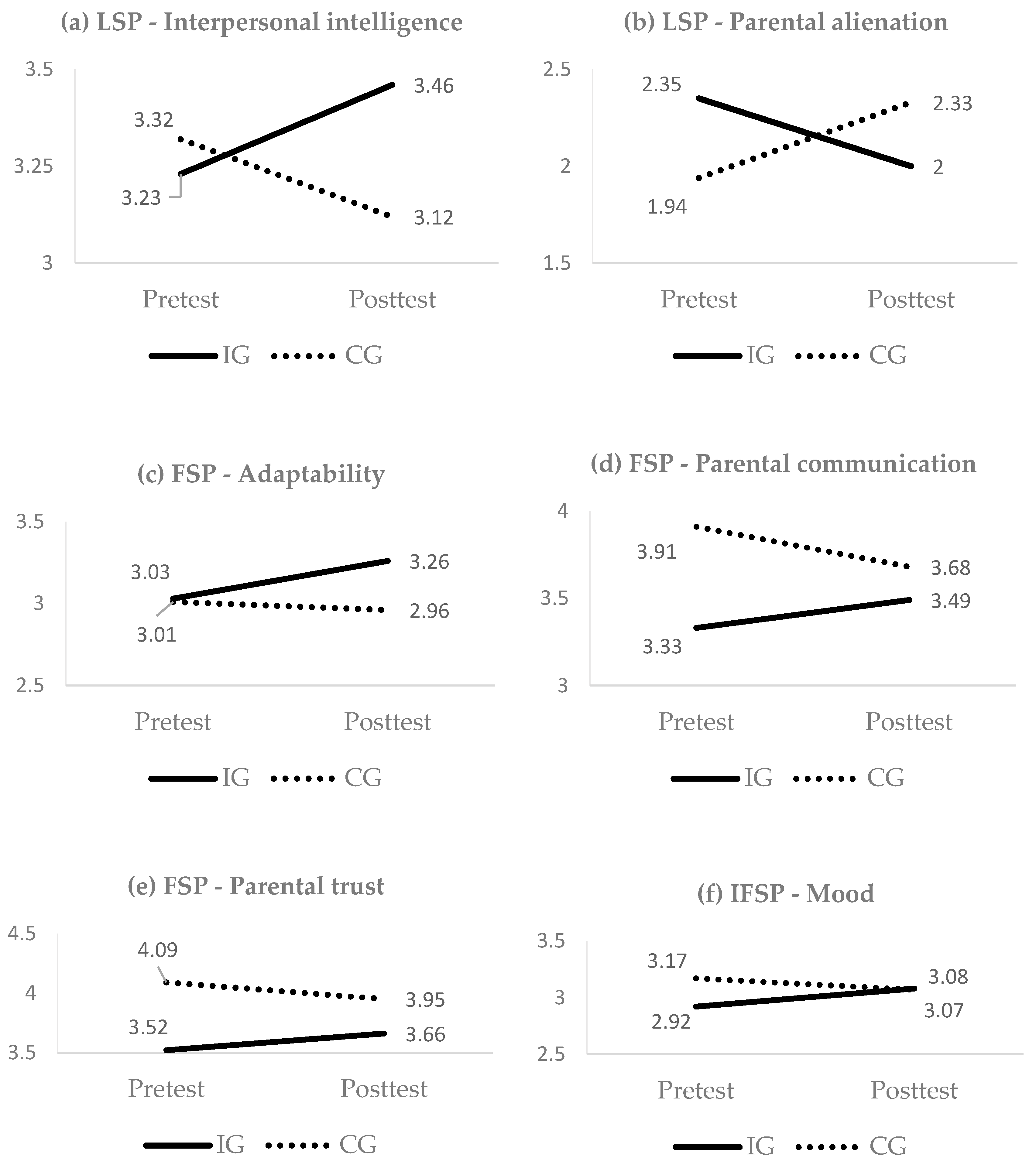
3.2. SB-PFT Effectiveness by Stress Profile
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Susman, E.J.; Dorn, L.D. Puberty: Its role in development. In Handbook of Adolescent Psychology, 3rd ed.; Lerner, R.M., Steinberg, L., Eds.; Wiley: Hoboken, NJ, USA, 2009; Volume 1, pp. 116–151. [Google Scholar]
- Grant, K.E.; Compas, B.E.; Stuhlmacher, A.F.; Thurm, A.E.; McMahon, S.D.; Halpert, J.A. Stressors and Child and Adolescent Psychopathology: Moving from Markers to Mechanisms of Risk. Psychol. Bull. 2003, 129, 447–466. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal and Coping; Springer: New York, NJ, USA, 1984. [Google Scholar]
- Grant, K.E.; Compas, B.E.; Thurm, A.E.; McMahon, S.D.; Gipson, P.Y. Stressors and Child and Adolescent Psychopathology: Measurement Issues and Prospective Effects. J. Clin. Child Adolesc. Psychol. 2004, 33, 412–425. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.; Munford, R.; Boden, J. The Impact of the Social Context on Externalizing Risks—Implications for the Delivery of Programs to Vulnerable Youth. Child. Youth Serv. Rev. 2018, 85, 107–116. [Google Scholar] [CrossRef]
- Roberts, Y.H.; English, D.; Thompson, R.; White, C.R. The Impact of Childhood Stressful Life Events on Health and Behavior in At-Risk Youth. Child. Youth Serv. Rev. 2018, 85, 117–126. [Google Scholar] [CrossRef]
- Weaver, J.M.; Schofield, T.J. Mediation and Moderation of Divorce Effects on Children’s Behavior Problems. J. Fam. Psychol. 2015, 29, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Petersen, I.T.; Bates, J.E.; Dodge, K.A.; Lansford, J.E.; Pettit, G.S. Describing and Predicting Developmental Profiles of Externalizing Problems from Childhood to Adulthood. Dev. Psychopathol. 2015, 27, 791–818. [Google Scholar] [CrossRef] [PubMed]
- Conger, R.D.; Conger, K.J.; Martin, M.J. Socioeconomic Status, Family Processes, and Individual Development. J. Marriage Fam. 2010, 72, 685–704. [Google Scholar] [CrossRef] [PubMed]
- Ngo, H.M.; Le, T.N. Stressful Life Events, Culture, and Violence. J. Immigr. Minor. Health 2007, 9, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Yue, L.; Dajun, Z.; Yinghao, L.; Tianquiang, H. Meta-Analysis of the Relationship between Life Events and Depression in Adolescents. J. Pediatr. Care 2016, 2, 1. [Google Scholar] [CrossRef]
- Baker, C.K.; Hishinuma, E.S.; Chang, J.Y.; Nixon, D.C. The Relationship among Exposure to Stressful Life Events, Drug Use, and Violence Perpetration in a Sample of Native Hawaiian, Samoan, and Filipino Adolescents. J. Interpers. Violence 2010, 25, 379–399. [Google Scholar] [CrossRef] [PubMed]
- Pereda, N.; Guilera, G.; Abad, J. Victimization and Polyvictimization of Spanish Children and Youth: Results from a Community Sample. Child Abus. Negl. 2014, 38, 640–649. [Google Scholar] [CrossRef] [PubMed]
- Turner, H.A.; Finkelhor, D.; Hamby, S.L.; Shattuck, A.; Ormrod, R.K. Specifying Type and Location of Peer Victimization in a National Sample of Children and Youth. J. Youth Adolesc. 2011, 40, 1052–1067. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, S.; Bussey, K. The Development of the Social Bullying Involvement Scales. Aggress. Behav. 2011, 37, 177–192. [Google Scholar] [CrossRef] [PubMed]
- Hawker, D.S.J.; Boulton, M.J. Twenty Years’ Research on Peer Victimization and Psychosocial Maladjustment: A Meta-Analytic Review of Cross-Sectional Studies. J. Child Psychol. Psychiatry 2000, 41, 441–455. [Google Scholar] [CrossRef] [PubMed]
- Stadler, C.; Feifel, J.; Rohrmann, S.; Vermeiren, R.; Poustka, F. Peer-Victimization and Mental Health Problems in Adolescents: Are Parental and School Support Protective? Child Psychiatry Hum. Dev. 2010, 41, 371–386. [Google Scholar] [CrossRef] [PubMed]
- Troop-Gordon, W.; Ladd, G.W. Trajectories of Peer Victimization and Perceptions of the Self and Schoolmates: Precursors to Internalizing and Externalizing Problems. Child Dev. 2005, 76, 1072–1091. [Google Scholar] [CrossRef] [PubMed]
- Serafini, G.; Pompili, M.; Borgwardt, S.; Houenou, J.; Geoffroy, P.A.; Jardri, R.; Girardi, P.; Amore, M. Brain Changes in Early-onset Bipolar and Unipolar Depressive Disorders: A Systematic Review in Children and Adolescents. Eur. Child Adolesc. Psychiatry 2014, 23, 1023–1041. [Google Scholar] [CrossRef] [PubMed]
- Bourassa, C. Co-Occurrence of Interparental Violence and Child Physical Abuse and It’s Effect on the Adolescents’ Behavior. J. Fam. Viol. 2007, 22, 691–701. [Google Scholar] [CrossRef]
- Ho, J. Community violence exposure of Southeast Asian American adolescents. J. Interpers. Violence 2008, 23, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Tocker, L.; Ben-Amitay, G.; Horesh-Reinman, N.; Lask, M.; Toren, P. Predictors of Clinical Outcomes in Sexually Abused Adolescents. J. Child Sex. Abus. 2017, 26, 487–505. [Google Scholar] [CrossRef] [PubMed]
- Giroux, M.E.; Chong, K.; Coburn, P.I.; Connolly, D.A. Differences in Child Sexual Abuse Cases Involving Child versus Adolescent Complainants. Child Abus. Negl. 2018, 79, 224–233. [Google Scholar] [CrossRef] [PubMed]
- McCuish, E.C.; Cale, J.; Corrado, R.R. Abuse Experiences of Family Members, Child Maltreatment, and the Development of Sex Offending among Incarcerated Adolescent Males: Differences Between Adolescent Sex Offenders and Adolescent Non-Sex Offenders. Int. J. Offender Ther. Comp. Criminol. 2017, 61, 127–149. [Google Scholar] [CrossRef] [PubMed]
- Agnew, R. Foundation for a General Strain Theory of Crime and Delinquency. Criminology 1992, 30, 47–87. [Google Scholar] [CrossRef]
- Berkowitz, L. Frustration-Aggression Hypothesis: Examination and Reformulation. Psychol. Bull. 1989, 106, 59–73. [Google Scholar] [CrossRef] [PubMed]
- Finkel, E.J. The I3 Model: Metatheory, theory and evidence. In Advances in Experimental Social Psychology; Olson, J.M., Zanna, M.P., Eds.; ElServier: San Diego, CA, USA, 2014; Volume 49, pp. 1–104. [Google Scholar]
- Slotter, E.B.; Finkel, E.J. I3 Theory: Instigating, impelling, and inhibiting factors in aggression. In Human Aggression and Violence: Causes, Manifestations, and Consequences; Shaver, P.R., Mikulincer, M., Eds.; American Psychological Association: Washington, DC, USA, 2011; pp. 35–52. [Google Scholar]
- Grant, K.E.; Compas, B.E.; Thurm, A.E.; McMahon, S.D.; Gipson, P.Y.; Campbell, A.J.; Krochock, K.; Westerholm, R.I. Stressors and Child and Adolescent Psychopathology: Evidence of Moderating and Mediating Effects. Clin. Psychol. Rev. 2006, 26, 257–283. [Google Scholar] [CrossRef] [PubMed]
- Rutter, M. Resilience: Some Conceptual Considerations. J. Adolesc. Health 1993, 14, 626–631. [Google Scholar] [CrossRef]
- Cejudo, J.; Rodrigo-Ruiz, D.; López-Delgado, M.; Losada, L. Emotional Intelligence and Its Relationship with Levels of Social Anxiety and Stress in Adolescents. Int. J. Environ. Res. Public Health 2018, 15, 1073. [Google Scholar] [CrossRef] [PubMed]
- Krishnakumar, A.; Buehler, C. Interparental Conflict and Parenting Behaviors: A Meta-analytic Review. Fam. Relat. 2000, 49, 25–44. [Google Scholar] [CrossRef]
- Otis, K.L.; Huebner, E.S.; Hills, K.J. Origins of Early Adolescents’ Hope: Personality, Parental Attachment, and Stressful Life Events. Can. J. Sch. Psychol. 2016, 31, 102–121. [Google Scholar] [CrossRef]
- Lippold, M.A.; Davis, K.D.; McHale, S.M.; Buxton, O.M.; Almeida, D.M. Daily Stressor Reactivity during Adolescence: The Buffering Role of Parental Warmth. Health Psychol. 2016, 35, 1027–1035. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.S.; Silk, J.S.; Steinberg, L.; Myers, S.S.; Robinson, L.R. The Role of the Family Context in the Development of Emotion regulation. Soc. Dev. 2007, 16, 361–388. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Zhang, W.; Wang, Y. Parental Behavioral Control, Psychological Control and Chinese Adolescents’ Peer Victimization: The Mediating Role of Self-Control. J. Child Fam. Stud. 2015, 24, 628–637. [Google Scholar] [CrossRef]
- Rasalingam, A.; Clench-Aas, J.; Raanaas, R.K. Peer Victimization and Related Mental Health Problems in Early Adolescence: The Mediating Role of Parental and Peer Support. J. Early Adolesc. 2017, 37, 1142–1162. [Google Scholar] [CrossRef]
- Abdollahi, A.; Carlbring, P.; Khanbani, M.; Ghahfarokhi, S.A. Emotional Intelligence Moderates Perceived Stress and Suicidal Ideation Among Depressed Adolescent Inpatients. Personal. Individ. Differ. 2016, 102, 223–228. [Google Scholar] [CrossRef]
- Villanueva, L.; Montoya-Castilla, I.; Prado-Gascó, V. The Importance of Trait Emotional Intelligence and Feelings in the Prediction of Perceived and Biological Stress in Adolescents: Hierarchical Regressions and fsQCA Models. Stress 2017, 20, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Extremera, N.; Durán, A.; Rey, L. Perceived Emotional Intelligence and Dispositional Optimism-Pessimism: Analyzing Their Role in Predicting Psychological Adjustment Among Adolescents. Personal. Individ. Differ. 2007, 42, 1069–1079. [Google Scholar] [CrossRef]
- Hsieh, Y.-P.; Wei, H.-S.; Hwa, H.-L.; Shen, A.C.-T.; Feng, J.-Y.; Huang, C.-Y. The Effects of Peer Victimization on Children’s Internet Addiction and Psychological Distress: The Moderating Roles of Emotional and Social Intelligence. J. Child Fam. Stud. 2018. [Google Scholar] [CrossRef]
- Timmermans, M.; van Lier, P.A.C.; Koot, H.M. The Role of Stressful Events in the Development of Behavioural and Emotional Problems from Early Childhood to Late Adolescence. Psychol. Med. 2010, 40, 1659–1668. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.F.; Waldron, H.B.; Robbins, M.S.; Neeb, A.A. Functional Family Therapy for Adolescent Behavior Problems; American Psychological Association: Washington, DC, USA, 2013. [Google Scholar]
- Sexton, T. Functional Family Therapy in Clinical Practice: An Evidence-based Treatment Model for Working with Troubled Adolescents; Routledge: New York, NY, USA, 2011. [Google Scholar]
- Andretta, J.R.; McKay, M.T.; Harvey, S.A.; Perry, J.L. Inventory of Parent and Peer Attachment-Revised Scores in Adolescents: A Psychometric and Person-Oriented Study. Fam. Relat. 2017, 66, 527–540. [Google Scholar] [CrossRef]
- Berry, M.; McLean, S. Family Preservation. In Child Welfare for the Twenty-First Century. A Handbook of Practices, Policies, and Programs, 2nd ed.; Mallon, G.P., Hess, P.M., Eds.; Colombia University Press: New York, NY, USA, 2014; pp. 270–287. [Google Scholar]
- Blueprints for Healthy Youth Development. Available online: https://www.blueprintsprograms.org/ (accessed on 4 July 2018).
- Henggeler, S.W.; Schoenwald, S.K.; Bordin, C.M.; Rowland, M.D.; Cunningham, P.B. Multisystemic Therapy for Antisocial Behavior in Children and Adolescents, 2nd ed.; Guilford: New York, NY, USA, 2009. [Google Scholar]
- Robbins, M.S.; Alexander, J.F.; Turner, C.W.; Hollimon, A. Evolution of Functional Family Therapy as an Evidence-Based Practice for Adolescents with Disruptive Behavior Problems. Fam. Process 2016, 55, 543–557. [Google Scholar] [CrossRef] [PubMed]
- Xuan, J.; Restrepo, M.L. Efficacy of Multisystemic Therapy in Youths Aged 10–17 with Severe Antisocial Behaviour and Emotional Disorders: Systemic Review. Lond. J. Prim. Care 2017, 9, 95–103. [Google Scholar]
- Lorence, B.; Mora-Díaz, M.; Maya, J. Description and Analysis of the Quality of Programs for the Treatment of Antisocial Behavior in the City of Huelva. J. Res. Soc. Ped. 2018, 32, 109–121. [Google Scholar]
- Maya, J.; Jiménez, L.; Lorence, B.; del Moral, G.; Hidalgo, V. Scene-Based Psychodramatic Family Therapy with Troubled Adolescents and Parents. A Pilot Study. Fam. Process. in press.
- Gutiérrez, J.A. Intervención Comunitaria desde el Enfoque Psicoescénico. Mosaico 2015, 60, 86–94. [Google Scholar]
- Minuchin, S.; Fishman, H.C. Family Therapy Techniques; Harvard University Press: Cambridge, MA, UK, 1981. [Google Scholar]
- Cruz, A.; Sales, C.M.D.; Alves, P.; Moita, G. The Core Techniques of Morenian Psychodrama: A Systematic Review of Literature. Front. Psychol. 2018, 9, 1263. [Google Scholar] [CrossRef] [PubMed]
- Keiley, M.K.; Zaremba-Morgan, A.; Datubo-Brown, C.; Pyle, R.; Cox, M. Multiple-family Group Intervention for Incarcerated Male Adolescents Who Sexually Offend and Their Families: Change in Maladaptive Emotion Regulation Predicts Adaptive Change in Adolescent Behaviors. J. Marital Fam. Ther. 2015, 41, 324–339. [Google Scholar] [CrossRef] [PubMed]
- Yalom, I.D.; Leszcz, M. The Theory and Practice of Group Psychotherapy, 5th ed.; Basic Books: New York, NY, USA, 2005. [Google Scholar]
- Kellermann, P.F. The Place of Catharsis in Psychodrama. J. Group Psychother. Psychodrama Sociom. 1984, 37, 1–13. [Google Scholar]
- Jonson-Reid, M. Child Welfare Services and Delinquency: The Need to Know More. Child Welf. 2004, 83, 157–173. [Google Scholar]
- Jiménez, L.; Menéndez, S.; Hidalgo, M.V. An Analysis of Stressful Life Events during Adolescence. Psychol. Spain 2009, 13, 1–8. [Google Scholar]
- Bar-On, R.; Parker, J.D.A. The Bar-On Emotional Quotient Inventory: Youth Version (EQ-i:YV): Technical Manual; Multi-Health Systems: Toronto, ON, Canada, 2006. [Google Scholar]
- Armsden, G.C.; Greenberg, M.T. The Inventory of Parent and Peer Attachment: Individual Differences and Their Relationship to Psychological Well-being in Adolescence. J. Youth Adolesc. 1987, 16, 427–454. [Google Scholar] [CrossRef] [PubMed]
- Buss, A.H.; Perry, M. The Aggression Questionnaire. J. Personal. Soc. Psychol. 1992, 63, 452–459. [Google Scholar] [CrossRef]
- Santisteban, C.; Alvarado, J.M. The Aggression Questionnaire for Spanish Preadolescents and Adolescents: AQ-PA. Span. J. Psychol. 2009, 12, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Bonate, P.L. Analysis of Pretest-Posttest Designs; Chapman and Hall/CRC: Boca Raton, FL, USA, 2000; ISBN 9781584881735. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 5th ed.; Pearson Education: Boston, MA, USA, 2007. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Hidalgo, V.; Pérez-Padilla, J.; Sánchez, J.; Ayala-Nunes, L.; Maya, J.; Grimaldi, V.; Menéndez, S. An Analysis of Different Resources and Programmes Supporting At-Risk Families in Spain. Early Child Dev. Care 2018. [Google Scholar] [CrossRef]
- Flay, B.R.; Biglan, A.; Boruch, R.F.; Castro, F.G.; Gottfredson, D.; Kellam, S.; Mościcki, E.K.; Schinke, S.; Valentine, J.C.; Ji, P. Standards of Evidence: Criteria for Efficacy, Effectiveness and Dissemination. Prev. Sci. 2005, 6, 151–175. [Google Scholar] [CrossRef] [PubMed]
- Gottfredson, D.C.; Cook, T.D.; Gardner, F.E.; Gorman-Smith, D.; Howe, G.W.; Sandler, I.N.; Zafft, K.M. Standards of evidence for efficacy, effectiveness, and scale-up research in prevention science: Next generation. Prev. Sci. 2015, 16, 893–926. [Google Scholar] [CrossRef] [PubMed]
- Friedlander, M.L.; Escudero, V.; Heatherington, L.; Diamond, G.M. Alliance in Couple and Family Therapy. Psychotherapy 2011, 48, 25–33. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Profile | Total (n = 210) | IG (n = 104) | CG (n = 106) | Differences |
|---|---|---|---|---|
| Adolescents | ||||
| Girls | 50.50% | 49.00% | 52.00% | χ2 = 0.17 n.s. |
| Age | M = 14.34, SD = 1.47 | M = 14.16, SD = 1.48 | M = 14.52, SD = 1.44 | F = 3.07 n.s. |
| Families | ||||
| Two-parent structure | 61.86% | 58.33% | 65.42% | χ2 = 0.86 n.s. |
| Number of members | M = 4.00, SD = 1.10 | M = 4.07, SD = 1.16 | M = 3.94, SD = 1.05 | F = 0.68 n.s. |
| Family-related stressful events | ||||
| Severe financial problems | 46.20% | 48.10% | 44.30% | χ2 = 0.29 n.s. |
| Chronic parental conflict | 40.00% | 47.10% | 33.00% | χ2 = 4.35 * (0.14) 1 |
| Parents’ divorce | 28.60% | 34.60% | 22.60% | χ2 = 3.69 n.s. |
| Parent’s new partner | 24.80% | 34.60% | 15.10% | χ2 = 10.74 ** (0.23) 1 |
| Parent’s mental or physical illness | 24.30% | 30.80% | 17.90% | χ2 = 4.71 * (0.15) 1 |
| Individual stressful events | ||||
| Bullying (peer victimization) | 28.10% | 31.70% | 24.50% | χ2 = 1.35 n.s. |
| Victim of intra-family violence | 16.70% | 21.20% | 12.30% | χ2 = 2.99 n.s. |
| Sexual harassment or abuse | 6.70% | 8.70% | 4.70% | χ2 = 1.31 n.s. |
| Variables | LSP M (SD) | FSP M (SD) | IFSP M (SD) | Differences | |
|---|---|---|---|---|---|
| F (η2partial) | DMS | ||||
| Emotional intelligence | |||||
| Intrapersonal | 2.59 (0.52) | 2.61 (0.67) | 2.34 (0.54) | 4.14 * (0.04) | LSP-IFSP * FSP-IFSP ** |
| Interpersonal | 3.30 (0.49) | 3.24 (0.46) | 3.26 (0.46) | 0.22 n.s. | - |
| Adaptability | 2.97 (0.62) | 3.01 (0.51) | 3.01 (0.55) | 0.08 n.s. | - |
| Stress management | 2.57 (0.49) | 2.43 (0.63) | 2.24 (0.65) | 3.74 * (0.04) | LSP-IFSP ** |
| General mood | 3.37 (0.56) | 3.36 (0.48) | 3.03 (0.59) | 8.72 *** (0.09) | LSP-IFSP ** FSP-IFSP *** |
| Aggressive behavior | |||||
| Anger | 2.80 (0.82) | 3.09 (0.79) | 3.26 (0.85) | 3.90 * (0.04) | LSP-IFSP ** |
| Hostility | 2.42 (0.71) | 2.59 (0.61) | 3.01 (0.72) | 11.37 *** (0.11) | LSP-IFSP *** FSP-IFSP *** |
| Parent attachment | |||||
| Communication | 4.02 (0.72) | 3.61 (0.93) | 3.53 (0.99) | 3.72 * (0.04) | LSP-FSP * LSP-IFSP ** |
| Trust | 4.19 (0.50) | 3.80 (0.83) | 3.55 (1.00) | 6.89 *** (0.07) | LSP-FSP * LSP-IFSP *** |
| Alienation | 2.05 (0.78) | 2.38 (0.82) | 2.69 (0.72) | 8.36 *** (0.08) | LSP-FSP * LSP-IFSP *** FSP-IFSP * |
| Variables | IG | CG | LSP | IG | CG | FSP | IG | CG | IFSP | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1/T2 M (SD) | T1/T2 M (SD) | F (η2partial) | T1/T2 M (SD) | T1/T2 M (SD) | F (η2partial) | T1/T2 M (SD) | T1/T2 M (SD) | F (η2partial) | ||||||||
| Emotional intelligence | Intrapersonal | 2.59 (0.63) | 2.65 (0.80) | 2.59 (0.50) | 2.45 (0.64) | 0.84 n.s. | 2.71 (0.63) | 2.56 (0.64) | 2.50 (0.70) | 2.68 (0.64) | 3.70 n.s. | 2.24 (0.52) | 2.25 (0.58) | 2.46 (0.55) | 2.34 (0.65) | 1.03 n.s. |
| Interpersonal | 3.23 (0.65) | 3.46 (0.40) | 3.32 (0.45) | 3.12 (0.51) | 4.53 * (0.12) | 3.18 (0.45) | 3.36 (0.46) | 3.30 (0.46) | 3.34 (0.41) | 2.61 n.s. | 3.23 (0.51) | 3.25 (0.45) | 3.32 (0.38) | 3.28 (0.46) | 0.32 n.s. | |
| Adaptability | 2.88 (0.71) | 2.74 (0.85) | 3.01 (0.62) | 3.06 (0.53) | 0.57 n.s. | 3.03 (0.46) | 3.26 (0.60) | 3.01 (0.56) | 2.96 (0.48) | 5.72 * (0.06) | 2.93 (0.53) | 3.06 (0.51) | 3.13 (0.56) | 3.08 (0.54) | 2.94 n.s. | |
| Stress management | 2.43 (0.27) | 2.55 (0.74) | 2.62 (0.55) | 2.51 (0.53) | 1.06 n.s. | 2.30 (0.64) | 2.32 (0.76) | 2.54 (0.60) | 2.60 (0.45) | 0.13 n.s. | 2.07 (0.57) | 2.13 (0.50) | 2.48 (0.70) | 2.46 (0.67) | 0.35 n.s. | |
| General mood | 3.33 (0.71) | 3.43 (0.53) | 3.39 (0.53) | 3.27 (0.56) | 1.18 n.s. | 3.31 (0.50) | 3.38 (0.48) | 3.43 (0.47) | 3.40 (0.41) | 2.00 n.s. | 2.92 (0.59) | 3.08 (0.49) | 3.17 (0.58) | 3.07 (0.63) | 5.92 * (0.08) | |
| Aggressive | Anger | 3.00 (0.94) | 2.68 (0.77) | 2.74 (0.77) | 2.69 (0.87) | 0.72 n.s. | 3.18 (0.72) | 3.06 (0.95) | 3.00 (0.86) | 2.89 (0.81) | 0.01 n.s. | 3.39 (0.86) | 3.33 (0.85) | 3.10 (0.81) | 3.06 (0.82) | 0.01 n.s. |
| Hostility | 2.23 (0.81) | 3.36 (1.03) | 2.52 (0.67) | 2.52 (0.77) | 0.20 n.s. | 2.54 (0.64) | 2.33 (0.68) | 2.65 (0.60) | 2.59 (0.72) | 0.95 n.s. | 2.96 (0.67) | 2.89 (0.68) | 3.10 (0.77) | 2.94 (0.80) | 0.12 n.s. | |
| Parent attachment | Communication | 3.88 (0.62) | 3.62 (0.92) | 4.08 (0.76) | 3.72 (0.86) | 0.08 n.s. | 3.33 (0.98) | 3.49 (0.89) | 3.91 (0.77) | 3.68 (0.82) | 5.88 * (0.06) | 3.43 (0.97) | 3.31 (0.97) | 3.74 (0.95) | 3.57 (0.92) | 0.04 n.s. |
| Trust | 4.29 (0.40) | 4.08 (0.46) | 4.16 (0.54) | 3.93 (0.78) | 0.01 n.s. | 3.52 (0.90) | 3.66 (0.87) | 4.09 (0.62) | 3.95 (0.71) | 4.31 * (0.05) | 3.25 (1.04) | 3.32 (0.90) | 3.99 (0.78) | 3.84 (0.80) | 2.48 n.s. | |
| Alienation | 2.35 (1.00) | 2.00 (0.68) | 1.94 (0.66) | 2.33 (0.93) | 4.35 * (0.11) | 2.62 (0.85) | 2.70 (0.86) | 2.13 (0.70) | 2.23 (0.73) | 0.02 n.s. | 2.84 (0.73) | 2.92 (0.67) | 2.45 (0.67) | 2.45 (1.04) | 0.19 n.s. | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maya, J.; Lorence, B.; Hidalgo, V.; Jiménez, L. The Role of Psychosocial Stress on a Family-Based Treatment for Adolescents with Problematic Behaviors. Int. J. Environ. Res. Public Health 2018, 15, 1867. https://doi.org/10.3390/ijerph15091867
Maya J, Lorence B, Hidalgo V, Jiménez L. The Role of Psychosocial Stress on a Family-Based Treatment for Adolescents with Problematic Behaviors. International Journal of Environmental Research and Public Health. 2018; 15(9):1867. https://doi.org/10.3390/ijerph15091867
Chicago/Turabian StyleMaya, Jesús, Bárbara Lorence, Victoria Hidalgo, and Lucía Jiménez. 2018. "The Role of Psychosocial Stress on a Family-Based Treatment for Adolescents with Problematic Behaviors" International Journal of Environmental Research and Public Health 15, no. 9: 1867. https://doi.org/10.3390/ijerph15091867
APA StyleMaya, J., Lorence, B., Hidalgo, V., & Jiménez, L. (2018). The Role of Psychosocial Stress on a Family-Based Treatment for Adolescents with Problematic Behaviors. International Journal of Environmental Research and Public Health, 15(9), 1867. https://doi.org/10.3390/ijerph15091867