An Assessment of the Relationships between Extreme Weather Events, Vulnerability, and the Impacts on Human Wellbeing in Latin America

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
1.1. Impacts of Climate Change and Extreme Weather Events on Human Wellbeing in Latin America
1.2. Defining Key Concepts: Human Wellbeing, Health Vulnerability to Climate, Environmental Health and Climate Change Adaptation
- (1)
- Human wellbeing is a holistic construct that goes well beyond the dimensions of biophysical health services, e.g., clean air, a safe and adequate water supply, and a global ecosystem that will continue to provide these services at an individual level. Its meaning is captured in the World Health Organization’s definition of health “a state of complete physical, mental and social wellbeing and not merely the absence of disease and infirmity” [24]. These biophysical health services are closely related to the life-supporting systems concept used by the Notre Dame Gain Index [25], as well as to environmental wellbeing.
- (2)
- The vulnerability is composed of three elements: Exposure-E, Sensitivity-S, and Adaptive Capacity-AC [4]. Human health vulnerability to climate is a function of:(i) Sensitivity: the extent to which health (or the systems on which health outcomes depend), are sensitive to changes in weather and climate (the exposure-response relationship) and the characteristics of the population; (ii) the exposure to the climate-related hazard (the character, magnitude, and rate of climate variation); and (iii) the adaptation actions that are in place to reduce the burden of a specific adverse health outcome (the adaptation baseline), the effectiveness of which may influence the exposure-response relationship [26].Vulnerability measures a country’s exposure, sensitivity, and ability to adapt to the negative impact of climate change in life-supporting services, where E is the nature and degree to which a system is exposed to significant climate change, independent of socioeconomic context, sensitivity is the extent to which a country is dependent upon a sector negatively affected by climate hazards, or the proportion of the population that is particularly susceptible to climate change hazards, and AC is the availability of social resources for sector-specific (current or potential) adaptation capacities. The ND-Gain health score (vulnerability of water, habitat, and health services sectors) captures a country’s of public health vulnerability to climate change, regarding the spread of communicable diseases and provision of health services [25].
- (3)
- Environmental health is the science and practice of preventing human injury and illness and promoting wellbeing by (i) identifying and evaluating environmental sources and hazardous agents and (ii) limiting exposures to hazardous physical, chemical, and biological agents in air, water, soil, food, and other environmental media or settings that may adversely affect human health [27].
- (4)
- Climate Change Adaptation (CCA) refers to “the process of adjustment to actual or expected climate and its effects” [4].
1.3. Research Framework
- (i)
- External climate drivers (threats) are (assumed) uncontrollable on the short- and medium-term (e.g., 2025–2040) at the local level, whereas socioeconomic driving determinants are (considered) (almost) to be uncontrollable on the short-term, but potentially modifiable [17];
- (ii)
- The drivers of this system are external: climate change and extreme weather events (assumed uncontrollable on the medium-term), and socio-economic determinants of public health (supposed modifiable on the short- to medium-term); internal: knowledge and values; human safety, public health infrastructure, and investment (assumed as controllable on the short-term but dependent on the level of socioeconomic development, perception of risks, and political willingness);
- (iii)
- The vulnerability is composed by (1) the exposure (climatic and geographical characteristics, e.g., climate type/sub-types, location, and population density) [1,25], assumed as being uncontrollable on the short- to medium-term, (2) the sensitivity (e.g., % of population affected by climate-hazards and their susceptibility [1,25,26]), and (3) the adaptability composed of the adaptive capacity and readiness [25]. The components ii and iii are moderately modifiable on the medium-term;
- (iv)
- The actions relate to the country-level decision-making level (anticipatory climate adaptation) that are both influenced by and influence the concepts and terms mentioned above. Measures that are not primarily intended to reduce the current climate vulnerability and socioeconomic determinants are close to disaster preparedness and response, such as weather forecasting, early warning systems, evacuation, and relief (assumed as modifiable on the short-term).
- (i)
- extreme weather events directly affect the human wellbeing of vulnerable people, particularly among the poor and those more exposed people, and influence public health policies;
- (ii)
- wellbeing and health impacts of extreme weather events are linked to the human and socioeconomic development determinants of the health inequality, and the expenditures in Public Health; and,
- (iii)
- building resilience to extreme weather events and policies to support it, linked with disaster risk reduction actions are needed.
2. Materials and Methods
- (i)
- Step 1: Identification of the sample of countries and compilation of a list of climate-stressors, geographical, human, and socioeconomic determinants of the health vulnerability and safety issues, extreme weather events (EWEs), and Climate-Sensitive Disasters (CSDs) in the studied countries;
- (ii)
- (iii)
- Step 3: Collection of opinions from a sample of LA climate and environmental researchers and practitioners about climate change, EWEs, health vulnerability to climate, and the main perceived barriers and possible solutions in LA; and,
- (iv)
- Step 4: A comparative qualitative and quantitative analysis of the geographic and socioeconomic determinants of the vulnerability in regards to EWEs, CSDs, and wellbeing and environmental health.
2.1. Identification of the Sample of Countries and Compilation of the Primary Determinants of Health Vulnerability to Climate and Adaptation to Extreme Weather Events (EWEs)
2.2. Extreme Climate and Weather Events and Climate-Sensitive Disaster Statistics (1988–2017) in the Seventeen Studied LA Countries
2.3. A Survey on Perceptions of the Health Impacts of Extreme Weather Events and Sea Level Rise in Latin America
2.4. Comparative Analysis of the Determinants of EWEs, CSDs, and Environmental Health
3. Results
3.1. Geographical, Socio-Economic and Vulnerability Setting
3.1.1. The Geographical and Climatic Setting of Extreme Weather Events (EWEs)
3.1.2. Human and Socio-Economic Development, and Health Vulnerability Status
3.1.3. Descriptors of Extreme Weather Events
3.1.4. A Few Selected Quantitative Relationships between Indices and EWEs
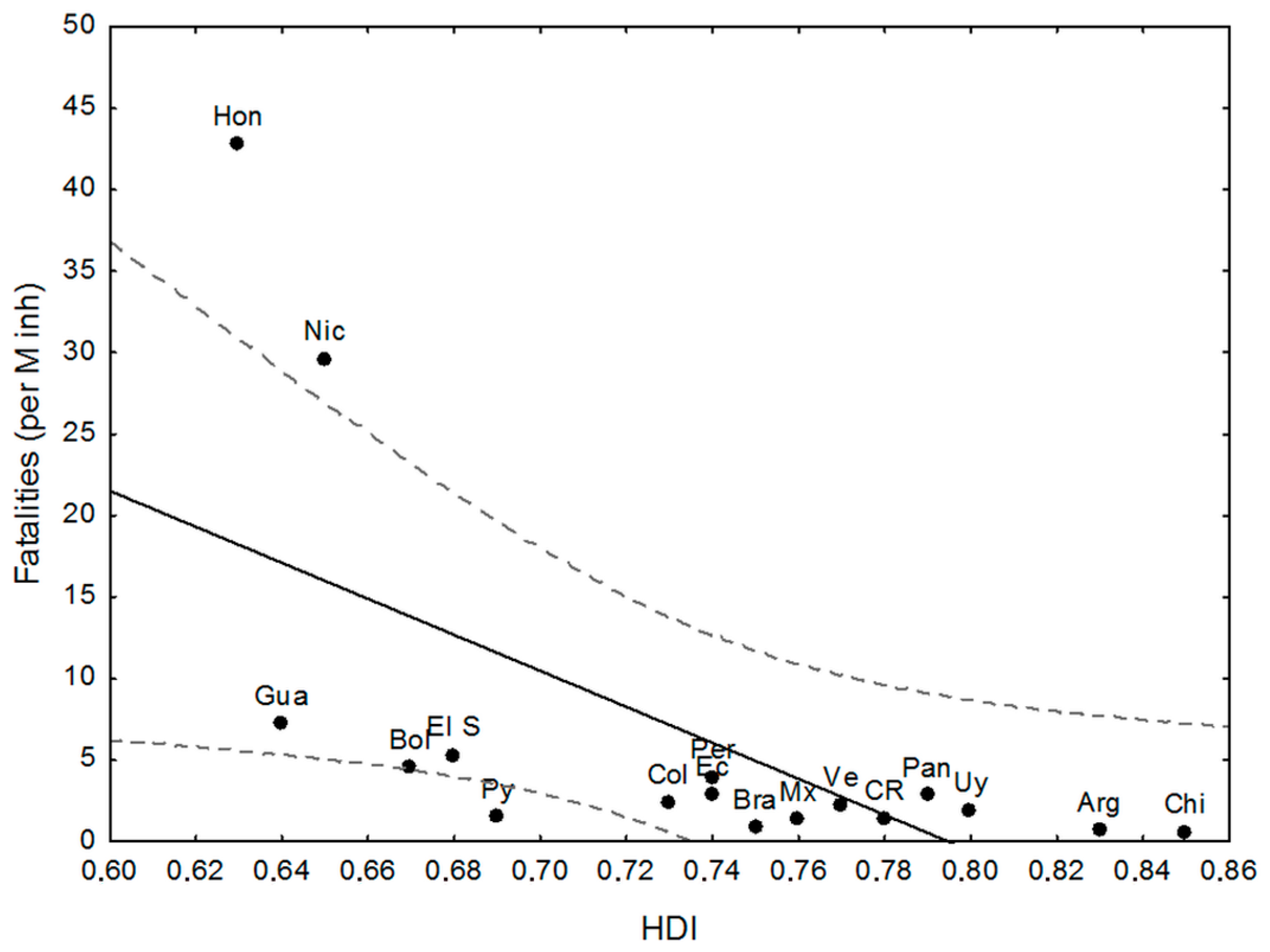
- there is a negative and significant relationship between HDI and the number of fatalities, including the outliers (high figures of Nicaragua and Honduras, and the low ones of Paraguay);
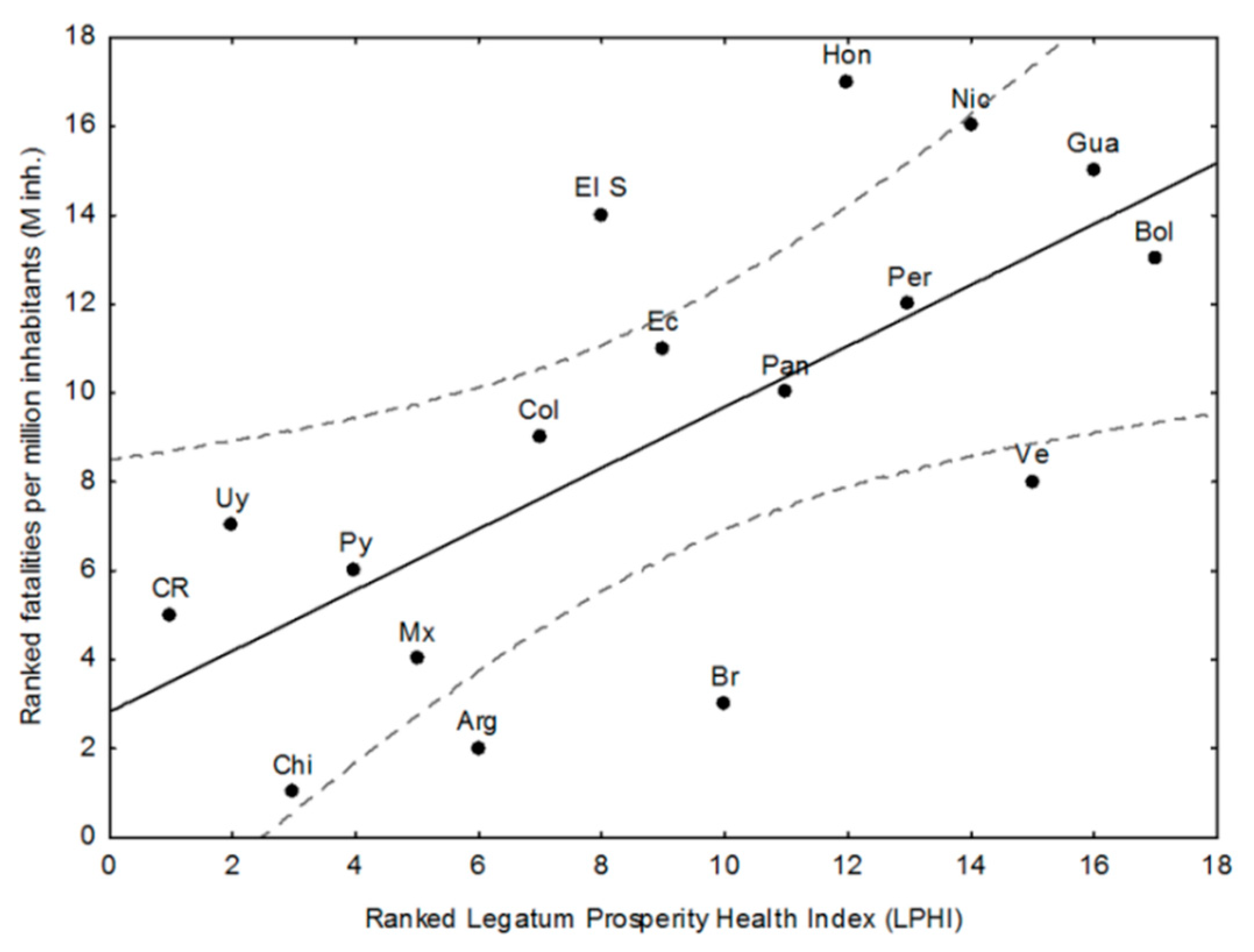
- Paraguay performs better than expected from HDI and in line with its good LPHI (ranked 4th, see Table 4), while Argentina, Brazil, and Mexico perform better than expected regarding their HDI, and Brazil and Argentina do the same regarding their LPHI;
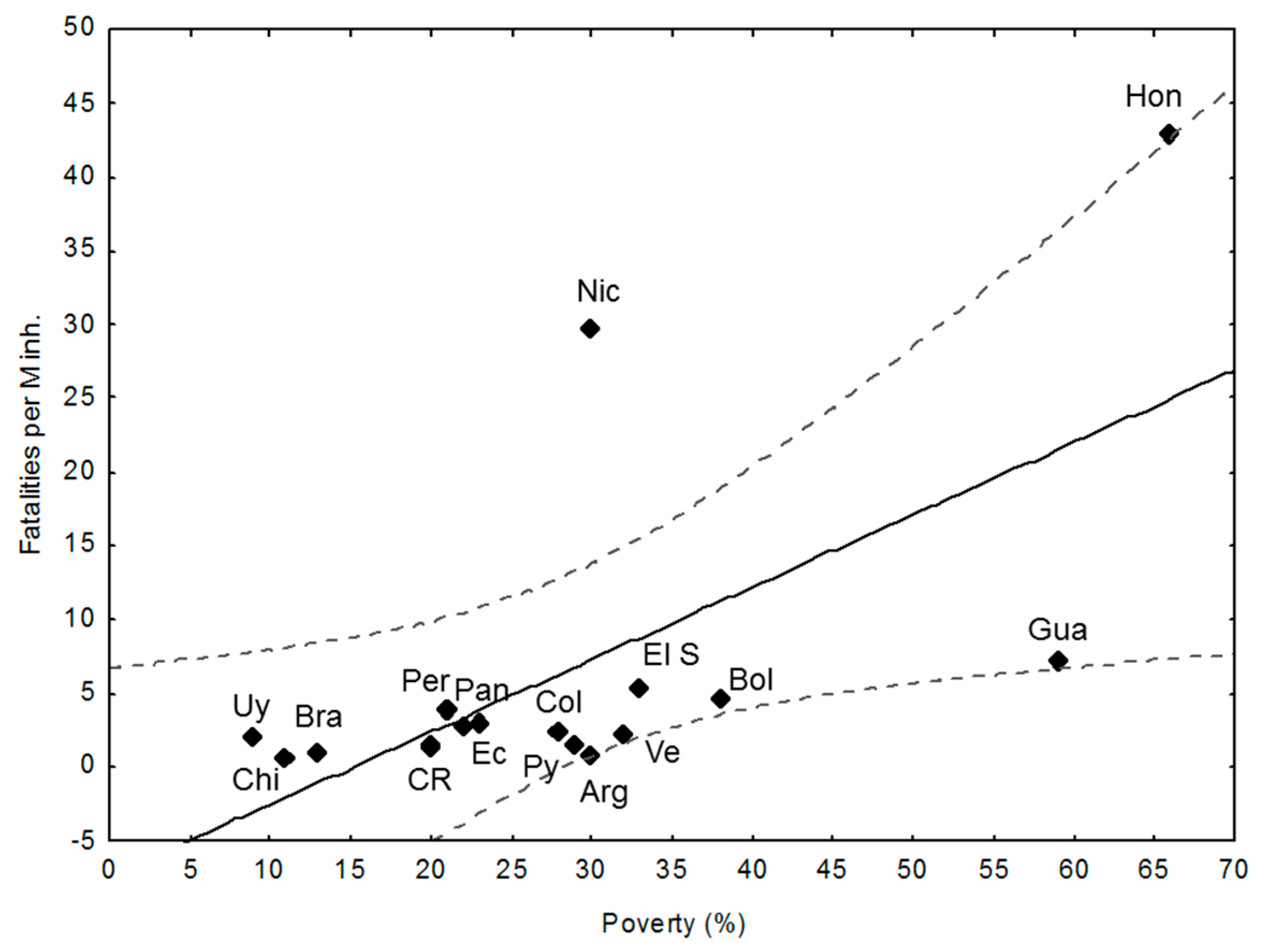
- there is a positive and significant linear trend between poverty (%) and fatalities per M inh. (r: 0.64, p < 0.01). Argentina, Paraguay, and Guatemala perform better than expected from this trend;
- the high and very high poverty percentages of Nicaragua (30%), El Salvador (33%), Bolivia (38%), Guatemala (59%), and Honduras (66%) are quite well correlated with fatalities, while Argentina (30%) and Paraguay (29%) perform better than expected from the trend, which is in line with their LPHI. Guatemala’s fatalities lie below expected from HDI, poverty, and LPHI;
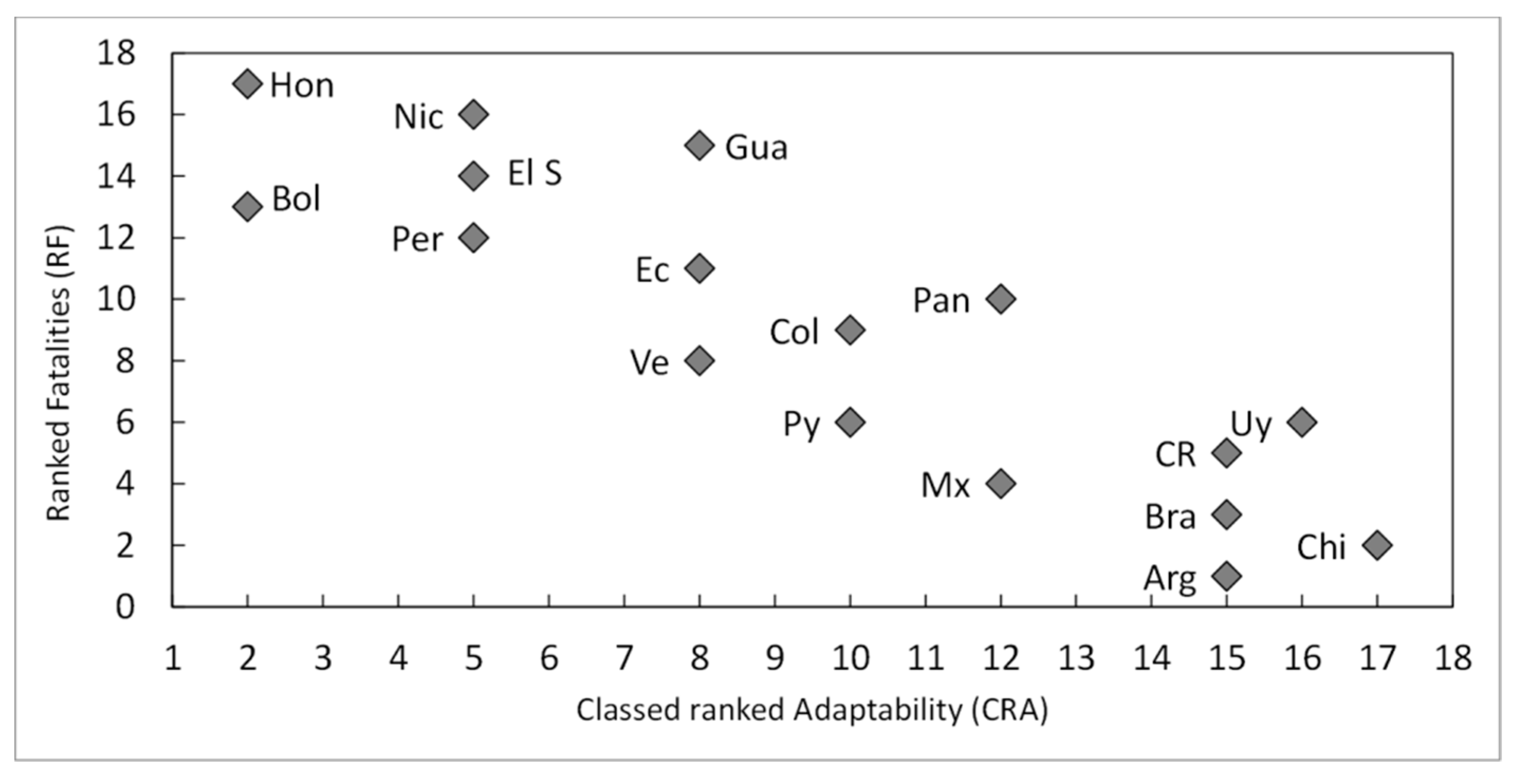
- the HDI index, the poverty rate (%), and the classed LPHI and CRV are quite well related to the fatalities per M inh. (and the RF), except for outliers Honduras and Nicaragua, which show terrible socio-economic and vulnerability indicators. There are a few examples of countries performing somewhat better (which does not mean well) than expected from the chosen descriptors (e.g., Argentina and Paraguay); and,
- the aggregated discrete adaptability (CRA) shows a good fit with the ranked fatalities (RF). The same, but less clear was for CRV (not shown here).
3.2. Online Survey: Perceptions of the impacts of Climatic Changes and Extreme Weather Events (EWEs) on Human Wellbeing and Health in LA Countries, and Possible Solutions
- (i)
- inundation and river floods (94%);
- (ii)
- storms (76%, 18% of which coastal storm surges);
- (iii)
- droughts (67%);
- (iv)
- fires (48%);
- (v)
- heat waves (47%); and,
- (vi)
- others (23%, e.g., hurricanes, sea-level rise, hail, landslides).
- (i)
- “The preliminary draft of the Framework Law on Climate Change, drafted for just over a year, is in the process of socialisation, seeking to put Paraguay among the first countries to address this problem at the global level”.
- (ii)
- “The XXI century needs the integration of self-care, care for the other, and care for the whole planetary ecosystem. There is a need for a new ethos (neoethos) in our health professions; we need to transform our paradigms of health”.
3.3. Linking Data to Perceptions
3.4. Classed Ranked Vulnerability and Adaptability, and Climate-Risk
4. Discussion
4.1. The Assessment of the Determinants of Vulnerability and Impacts
- (i)
- Inequity “A disparity in health outcomes that is systematic, avoidable, and unjust” [45];
- (ii)
- Inequality “Differences, variations, and disparities in the health achievements of individuals and groups of people” [46];
- (iii)
- Disparity “A type of difference in health that is closely linked with a social or economic disadvantage that negatively affects groups of people who have systematically experienced greater socioeconomic obstacles to health (e.g., socioeconomic status, geographic location)” [47].
4.2. Main Contributions to the Analysis Extracted from the Online Survey
4.3. Adaptation Strategies to cope with Extreme Weather Events
4.4. Potential Limitations of the Paper
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ebi, K.; Bowen, K. Extreme events as sources of health vulnerability: Drought as an example. Weather Clim. Extreme 2016, 11, 95–102. [Google Scholar] [CrossRef]
- Watts, N.; Amann, M.; Ayeb-Karlsson, S.; Belesova, K.; Bouley, T.; Boykoff, M. The Lancet Countdown on health and climate change: From 25 years of inaction to a global transformation for public health. Lancet 2018, 391, 581–630. [Google Scholar] [CrossRef]
- Field, C.B.; Barros, V.; Stocker, T.F.; Qin, D.; Dokken, D.J.; Ebi, K.L.; Mastrandrea, M.D.; Mach, K.J.; Plattner, G.K.; Allen, S.K. IPCC: Managing the Risks of Extreme Events and Disasters to Advance Climate Change Adaptation; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2012; p. 582. ISBN 978-1-107-60780-4. [Google Scholar]
- Field, C.B.; Barros, V.R.; Dokken, D.J.; Mach, K.J.; Mastrandrea, M.D.; Bilir, T.E.; Chatterjee, M.; Ebi, K.L.; Estrada, Y.O.; Genova, R.C. IPCC: Climate Change 2014: Impacts, Adaptation, and Vulnerability; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014; p. 1132. ISBN 978-1-107-41537-9. [Google Scholar]
- Banwell, N.; Rutherford, S.; Mackey, B.; Chu, C. Towards Improved Linkage of Disaster Risk Reduction and Climate Change Adaptation in Health: A Review. Int. J. Environ. Res. Public Health 2018, 15, 793. [Google Scholar] [CrossRef] [PubMed]
- Cai, W.; Borlace, S.; Lengaigne, M.; van Rensch, P.; Collins, M.; Vecchi, G.; Timmermann, A.; Santoso, A.; McPhaden, M.J.; Wu, L.; et al. Increasing frequency of extreme El Niño events due to greenhouse warming. Nat. Clim. Chang. 2014, 4, 111–116. [Google Scholar] [CrossRef] [Green Version]
- Hulme, M. Attributing weather extremes to ‘climate change’: A review. Prog. Phys. Geogr. 2014, 38, 499–511. [Google Scholar] [CrossRef]
- Yuan, X.-C.; Wei, Y.-M.; Wang, B.; Mi, Z. Risk management of extreme events under climate change. J. Clean. Prod. 2017, 166, 1169–1174. [Google Scholar] [CrossRef]
- Haines, A.; Kovats, R.S.; Campbell-Lendrum, D.; Corvalán, C. Climate change and human health: Impacts, vulnerability and public health. Public Health 2006, 120, 585–596. [Google Scholar] [CrossRef] [PubMed]
- WHO. Climate Change and Health. 2017. Available online: http://www.who.int/mediacentre/factsheets/fs266/en/ (accessed on 1 June 2018).
- Paavola, J. Health Impacts of Climate Change and Health and Social Inequalities in the UK. Environ. Health 2017. Available online: http://eprints.whiterose.ac.uk/115910 (accessed on 1 June 2018). [CrossRef] [PubMed]
- Leal-Filho, W.; Esteves de Freitas, L. Preface. In Climate Change Adaptation in Latin America: Managing Vulnerability, Fostering Resilience; Leal-Filho, W., Esteves Freitas, L., Eds.; Springer: Berlin, Germany, 2018; pp. v–xv. ISBN 9783319569451. [Google Scholar]
- Leal-Filho, W.; Azeiteiro, U.M.; Alves, F. Climate Change and Health: An Overview of the Issues and Needs. In Climate Change and Health; Leal-Filho, W., Azeiteiro, U.M., Alves, F., Eds.; Springer: Berlin, Germany, 2016; pp. 1–10. ISBN 9783319246604. [Google Scholar]
- Thomas, F.; Sabel, C.E.; Morton, K.; Hiscock, R.; Depledge, M.H. Extended impacts of climate change on health and wellbeing. Environ. Sci. Policy 2014, 44, 271–278. [Google Scholar] [CrossRef]
- Franchini, M.; Mannucci, P.M. Impact on human health of climate changes. Eur. J. Intern. Med. 2015, 26, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.D.; Harley, D. Primary, secondary and tertiary effects of eco-climatic change: The medical response. Postgrad. Med. J. 2010, 86, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Leal-Filho, W.; Al-Amin, A.Q.; Nagy, G.J.; Azeiteiro, U.M.; Wiesböck, L.; Ayal, D.Y.; Morgan, E.A.; Mugabe, P.; Aparicio-Effen, M.; Fudjumdjum, H. A comparative analysis of climate-risk and extreme event-related impacts on well-being and health: Policy implications. Int. J. Environ. Res. Public Health 2018, 15, 331. [Google Scholar] [CrossRef] [PubMed]
- PAHO/WHO. Health in the Americas 2017. Pan American Health Organization/World Health Organization. 2017. Available online: http://www.paho.org/hq/index (accessed on 2 June 2018).
- Magrin, G.O.; Marengo, J.A.; Boulanger, J.P.; Buckeridge, M.S.; Castellanos, E.; Poveda, G.; Scarano, F.R.; Vicuña, S. Central and South America. In Climate Change 2014: Impacts, Adaptation, and Vulnerability: Part B: Regional Aspects; Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Field, C.B., Barros, V., Stocker, T.F., Qin, D., Dokken, D.J., Ebi, K.L., Mastrandrea, M.D., Mach, K.J., Plattner, G.K., Allen, S.K., Eds.; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014; pp. 1499–1566. ISBN 978-1-107-68386-0. [Google Scholar]
- Yamamoto, L.; Serraglio, D.A.; Cavedon-Capdeville, F. Human mobility in the context of climate change and disasters: A South American approach. Int. J. Clim. Chang. Strateg. Manag. 2018, 10, 65–85. [Google Scholar] [CrossRef]
- McBreen, J. Regional Assessment on Ecosystem-Based Disaster Risk Reduction and Biodiversity in South America; A Report for the Resilience through Investing in Ecosystems—Knowledge, Innovation and Transformation of Risk Management (RELIEF Kit) Project; International Union for Conservation of Nature: Grand, Switzerland, 2016; Available online: https://www.iucn.org/sites/dev/files/content/documents/regional_assessment_eco-drr_and_biodiversity_in_south_america_2016_0.pdf (accessed on 2 June 2018).
- Murti, R.; Rizvi, A.R.; Buyck, C. Introduction. In Safe Havens: Protected Areas for Disaster Risk Reduction and Climate Change Adaptation; Murti, R., Buyck, C., Eds.; International Union for Conservation of Nature (IUCN): Gland, Switzerland, 2014; pp. v–xii. Available online: https://www.iucn.org/sites/dev/files/2014-038.pdf (accessed on 30 March 2018).
- Garlati, A. Climate Change and Extreme Weather Events in Latin America: An Exposure Index; Technical Note No. IDB-TN-490; Inter-American Development Bank Department of Research: Washington, DC, USA, 2013; Available online: http://www.iadb.org (accessed on 30 March 2018).
- Neller, A.H.; Neller, R.J. Environment Wellbeing and Human Wellbeing. In Encyclopedia of Life Support Systems (EOLSS), Developed under the Auspices of the UNESCO; EOLSS: Paris, France, 2009; Volume II, pp. 1–19. Available online: http://www.eolss.net (accessed on 2 June 2018).
- ND-Gain. ND-GAIN Country Index. The University of Notre Dame. 2016. Available online: http://index.gain.org/ (accessed on 1 March 2018).
- Ebi, K.L.; Kovats, R.S.; Menne, B. An Approach for Assessing Human Health Vulnerability and Public Health Interventions to Adapt to Climate Change. Research Mini-Monograph. Environ. Health Perspect. 2006, 114, 1930–1934. [Google Scholar] [CrossRef] [PubMed]
- National Environmental Health Association (NEHA). Environmental Health Definition. 2018. Available online: https://www.neha.org/about-neha/definitions-environmental-health (accessed on 1 June 2018).
- Coral, C.; Bokelmann, W. The Role of Analytical Frameworks for Systemic Research Design, Explained in the Analysis of Drivers and Dynamics of Historic Land-Use Changes. Systems 2017, 5, 20. [Google Scholar] [CrossRef]
- Guha-Sapir, D. The International Disaster Database; Centre for Research on the Epidemiology of Disasters (CRED): Louvain, Belgium, 2018; Available online: http://www.emdat.be/ (accessed on 1 March 2018).
- Eckstein, D.; Künzel, V.; Schäfer, L. Global Climate Index 2018. German Watch. 2018. Available online: www.germanwatch.org/en/cri (accessed on 1 March 2018).
- United Nations Development Program (UNDP). Fighting Climate Change: Human Solidarity in a Divided World; United Nations Development Program United Nations Development Program: New York, NY, USA, 2007; ISBN 978-0-230-54704-9. Available online: www.tr.undp.org/content/turkey/en/home/library/human_development/human_development_report_2007-2008.html (accessed on 3 June 2018).
- United Nations Development Program (UNDP). Human Development for Everyone; Human Development Report 2015; United Nations Development Program: New York, NY, USA, 2016; ISBN 978-92-1-126413-5. Available online: http://hdr.undp.org/sites/default/files/2016_human_development_report.pdf (accessed on 1 June 2018).
- Legatum Prosperity Index (LPI). 2017. Available online: www.prosperity.com (accessed on 31 March 2018).
- USAID. Design and use of Composite Indices in Assessments of Climate Change Vulnerability and Resilience. African and Latin American Resilience to Climate Change Project. 2014. Available online: www.ciesin.org/documents/Design_Use_of_Composite_Indices.pdf (accessed on 1 June 2018).
- World Bank. The Costs to Developing Countries of Adapting to Climate Change New Methods and Estimates. The Global Report on the Economics of Adaptation to Climate Change Study. 2009. Available online: https://es.scribd.com/document/111276310/Adapting-to-Climate-Change-Assessing-World-Bank-Group-Experience (accessed on 1 June 2018).
- Villamizar, A.; Gutiérrez, M.E.; Nagy, G.J.; Caffera, R.M.; Leal Filho, W. Climate adaptation in South America with emphasis in coastal areas: the state-of-the-art and case studies from Venezuela and Uruguay. Clim. Dev. 2017, 9, 364–382. [Google Scholar] [CrossRef]
- Leal Filho, W.; Modesto, F.; Nagy, G.J.; Saroar, M.; Ha’apio, M. Fostering coastal resilience to climate change vulnerability in Bangladesh, Brazil, Cameroon, and Uruguay: A cross-country comparison. J. Mitig. Adapt. Strateg. Glob. Chang. 2018, 23, 579–602. [Google Scholar] [CrossRef]
- Leal Filho, W.; Balogun, A.L.; Ayal, D.Y.; Bethurem, E.M.; Murambadoro, M.; Mambo, J.; Taddese, H.; Tefera, G.W.; Nagy, G.J.; Fudjumdjum, H. (Eds.) Strengthening climate change adaptation capacity in Africa- case studies from six major. African cities and policy implications. J. Environ. Sci. Policy 2018, 86, 29–37. [Google Scholar] [CrossRef]
- World Bank. “GNI, PPP (int. $)”. 2018. Available online: https://data.worldbank.org/indicator/NY.GNP.PCAP.PP.CD (accessed on 1 June 2018).
- Comisión Económica para América Latina y el Caribe (CEPAL). Panorama Social de América Latina; Documento Informative; Comisión Económica para América Latina y el Caribe (CEPAL) de las Naciones Unidas: Santiago de Chile, Chile, 2017; p. 203. Available online: www.cepal.org (accessed on 15 March 2018).
- Makoka, D.; Kaplan, M. Poverty and Vulnerability. Term Paper. Interdisciplinary Course International Doctoral Studies Programme. ZEF, University of Bonn. 2005. Available online: https://mpra.ub.uni-muenchen.de/6964/1/poverty_and_vulnerability.pdf (accessed on 15 July 2018).
- Worldometer. Countries in the World by Population. 2017. Available online: http://www.worldometers.info/world-population/population-by-country/ (accessed on 15 March 2018).
- CLIMATE-DATA.ORG. Climate Data for Cities Worldwide. 2017. Available online: https://en.climate-data.org/ (accessed on 5 March 2018).
- Nagy, G.J.; Caffera, R.M.; Aparicio, M.; Barrenechea, P.; Bidegain, M.; Giménez, J.C.; Lentini, J.; Magrin, G.; Murgida, A.; Nobre, C. Understanding the Potential Impacts of Climate Change and Variability in Latin America and the Caribbean; Report Prepared for the Stern Review on the Economics of Climate Change; Department for International Development-DFID, HM Treasury: London, UK, 2006; Available online: http://www.dfld.de/Presse/PMitt/2006/061030cA.pdf (accessed on 5 June 2018).
- Braveman, P.A. Monitoring equity in health and healthcare: A conceptual framework. J. Health Popul. Nutr. 2003, 21, 181–192. [Google Scholar] [PubMed]
- Kawachi, I.; Subramanian, S.V.; Almeida-Filho, N. A glossary for health inequalities. J. Epidemiol. Commun. Health 2002, 56, 647–652. [Google Scholar] [CrossRef] [Green Version]
- Department of Health and Human Services (USDHHS). Healthy People 2020. Department of Health and Human Services. U.S. Government Printing Office; 2018. Available online: https://www.healthypeople.gov/ (accessed on 1 June 2018).
- Commission on Social Determinants of Health (CSDH). Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health; Final Report of the Commission on Social Determinants of Health (CSDH); World Health Organization: Geneva, Switzerland, 2008; p. 247. Available online: www.who.int/social_determinants/thecommission/finalreport/en/ (accessed on 1 June 2018).
- Leal Filho, W.; Icaza, L.E.; Emanche, V.; Al-Amin, A.Q. An Evidence-Based Review of Impacts, Strategies and Tools to Mitigate Urban Heat Islands. Int. J. Environ. Res. Public Health 2017, 14, 1600. [Google Scholar] [CrossRef] [PubMed]
- Leal Filho, W.; Bönecke, J.; Spielmann, H.; Azeiteiro, U.M.; Alves, F.; de Carvalho, M.; Nagy, G.J. Climate change and health: An analysis of causal relations on the spread of vector-borne diseases in Brazil. J. Clean. Prod. 2018, 177, 589–596. [Google Scholar] [CrossRef]
- Economic Commission for Latin America and the Caribbean (ECLAC). The Inefficiency of Inequality; Summary (LC/SES.37/4); ECLAC: Santiago de Chile, Chile, 2018; Available online: https://www.cepal.org/en/.../43443-inefficiency-inequality (accessed on 15 July 2018).
- Coronel, G.; Pastén, M.; Báez, J.; Monte-Domecq, R.; Bidegain, M.; Nagy, G.J. Improving capacities and communication on climate threats for water resources adaptation in Paraguay. In Handbook of Climate Change Adaptation; Leal Filho, W., Ed.; Springer: Berlin, Germany, 2015; pp. 1091–1108. ISBN 978-3-642-38669-5. [Google Scholar]
- Nagy, G.J.; Coronel, G.; Pastén, M.; Báez, J.; Monte Domecq, R.; Galeano Rojas, A.; Flores, L.; Ciganda, C.; Bidegain, M.; Aparicio-Effen, M. Impacts on well-being and health of excessive rainfall and floods in Paraguay, Uruguay and Bolivia. In Climate Change and Health: Improving Resilience and Reducing Risks; Leal Filho, W., Azeiteiro, U., Alves, F., Eds.; Climate Change Management Series; Springer: Berlin, Germany, 2016; pp. 475–514. ISBN 978-3-319-244660-4. [Google Scholar]
- Aparicio-Effen, M.; Arana, I.; Aparicio, J.; Ocampo, M.; Roque, S.; Nagy, G.J. A successful early warning system for hydroclimatic extreme events: The case of La Paz City mega-landslide. In Climate Change Adaptation in Latin America 2018; Leal Filho, W., de Freitas, L.E., Eds.; Climate Change Management Series; Springer: Heidelberg, Germany, 2018; pp. 241–265. ISBN 978-3-319-24658-1. [Google Scholar]
- Nisbet, M. Communicating Climate Change: Why Frames Matter for Public Engagement. Environment 2009, 51, 12–23. [Google Scholar] [CrossRef]
- O’Neill, S.; Nicholson-Cole, S. Fear Won’t Do It’: Promoting Positive Engagement with Climate Change through Visual and Iconic Representations. Sci. Commun. 2009, 30, 355–379. [Google Scholar] [CrossRef]
- Olausson, U. We’re the ones to blame’: Citizens’ representations of climate change and the role of the media. Environ. Commun. 2011, 5, 281–299. [Google Scholar] [CrossRef]
- Zhao, X.; Leiserowitz, A.; Maibach, E.; Roser-Renouf, C. Attention to Science/Environment News Positively Predicts and Attention to Political News Negatively Predicts Global Warming Risk Perceptions and Policy Support. J. Commun. 2011, 61, 713–731. [Google Scholar] [CrossRef]
- LealFilho, W.; Morgan, E.A.; Godoy, E.S.; Azeiteiro, U.M.; Baceloar-Nicolau, P.; Veiga, L.; Mac-Lean, C.; Hugé, J. Implementing Climate Change Research at Universities: Barriers, Potential and Actions. J. Clean. Prod. 2018, 170, 269–277. [Google Scholar] [CrossRef]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development A/RES/70/1. 2015, p. 41. Available online: https://sustainabledevelopment.un.org/content/documents/21252030%20Agenda%20for%20Sustainable%20Development%20web.pdf (accessed on 3 June 2018).
- McMichael, A.J. Globalization, Climate Change, and Human Health. N. Engl. J. Med. 2013, 369, 95–96. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.D.; Wang, X.W.; Yang, X.F.; Ma, W.J.; Ai, H.; Wu, X.X. Impacts of Climate Change on Human Health and Adaptation Strategies in South China. Adv. Clim. Chang. Res. 2013, 4, 208–214. [Google Scholar] [CrossRef]
- Aitsi-Selmi, A.; Murray, V. The Sendai framework: Disaster risk reduction through a health lens. Bull. World Health Organ. 2015, 93, 362. [Google Scholar] [CrossRef] [PubMed]
- Aitsi-Selmi, A.; Murray, V. Protecting the health and well-being of populations from disasters: Health and health care in the Sendai framework for disaster risk reduction 2015–2030. Prehosp. Disaster Med. 2016, 31, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Global Climate Change and Extreme Weather Events: Understanding the Contributions to Infectious Disease Emergence: Workshop Summary; National Academies Press: Washington, DC, USA, 2008. [Google Scholar] [CrossRef]
- Smith, K.; Woodward, A.; Campbell-Lendrum, D.; Chadee, D.; Honda, Y.; Liu, Q.; Olwoch, J.; Revich, B.; Sauerborn, R. Human health: Impacts, adaptation and co-benefits. In Climate Change Impacts: Adaptation and Vulnerability: Part A: Global and Sectoral Aspects; Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Field, C.B., Barros, V.R., Dokken, D.J., Mach, K.J., Mastrandrea, M.D., Bilir, T.E., Chatterjee, M., Ebi, K.L., Estrada, Y.O., Genova, R.C., Eds.; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014; pp. 709–754. ISBN 978-1-107-68386-0. [Google Scholar]
- The Lancet Global Health. The right(s) Approach to Zika. Lancet Glob. Health 2016, 4, e427. [Google Scholar] [CrossRef]
- Corvalán, C.F.; Hales, S.; McMichael, A.J.; Butler, C.; Campbell-Lendrum, D.; Confalonieri, U.; Leitner, K.; Lewis, N.; Patz, P.; Sarukhán, J. Ecosystems and Human Well-Being Health Synthesis: A Report of the Millennium Ecosystem Assessment; World Health Organization: Geneva, Switzerland, 2005; Available online: http://www.who.int/iris/handle/10665/4335 (accessed on 1 June 2018).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country (Region) | Area Mkm2 | Pop Minh. | Main Climate Köppen Class. Types | Main Extreme Weather Events (EWEs) |
|---|---|---|---|---|
| Argentina (SA) | 2.7 | 44 | Temperate humid subtropical (Cfa) | Riverine floods, Storms, Wildfires, ext. (cold) temperatures, storm surges |
| Bolivia (SA) | 1.1 | 11 | Dry cold semi-arid (BSk) | Drought, landslides, wildfires, ext. temperatures (cold; heat wave) |
| Brazil (SA) | 8.3 | 209 | Tropical wet (Aw) | Riverine Floods; droughts; landslides, ext. (cold) temperatures |
| Chile (SA) | 0.7 | 18 | Temperate warm summer (Csb) | Riverine floods, wildfires, landslides, ext. (cold) temperatures |
| Colombia (SA) | 1.1 | 49 | Tropical rainforest (Af) | Riverine floods, landslides |
| Costa Rica (CA) | 0.51 | 5 | Tropical wet (Aw) | Storms, riverine floods, wildfires |
| Ecuador (SA) | 0.25 | 17 | Tropical wet (Aw) | Riverine floods, droughts, landslides, sea-floods |
| El Salvador (CA) | 0.02 | 6 | Tropical wet (Aw) | Storms, droughts, riverine floods |
| Guatemala (CA) | 0.11 | 17 | Tropical wet (Aw) | Droughts, storms, riverine floods, wildfires |
| Honduras (CA) | 0.11 | 9 | Tropical wet (Aw) | Droughts, storms, riverine floods, wildfires |
| Mexico | 1.9 | 129 | Hot semi-arid (BSh) | Storms, riverine floods, droughts, ext. (cold) temperatures |
| Nicaragua (CA) | 0.12 | 6 | Tropical wet (Aw) | Storms, riverine floods, droughts, wildfires |
| Panama (CA) | 0.74 | 4 | Tropical monsoon (Am) | Riverine floods, storms |
| Paraguay (SA) | 0.4 | 7 | Temperate humid subtropical (Cfa) | Riverine floods, droughts, wildfires, ext. (cold) temperatures |
| Peru (SA) | 1.3 | 32 | Oceanic (Cfb) | Riverine floods, ext. (cold) temperatures, droughts, storms, landslides |
| Uruguay (SA) | 0.18 | 3.4 | Temperate humid subtropical (Cfa) | Riverine floods, storms, ext. (cold) temperatures, storm surges |
| Venezuela (SA) | 0.9 | 32 | Tropical wet (Aw) | Riverine floods, landslides |
| Human and Socioeconomic Development Poverty (Pov) | ND-Gain Index (Discrete Values) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Discrete Vulnerability Indices and Aggregated Vulnerability (CRV) and Adaptability (CRA) | ||||||||||
| Country | Human 2016 | Socio-Economic 2017 | PHV | WV | HHV | E | S | Classed Ranked CRV and CRA. The Highest the Less Vulnerable/Most Adaptable | ||
| HDI 2016 Class | Pov (%) 2016 | Per Capita GNI | ||||||||
| Argentina | Very High | 30 | High | 2 | 2 | 2.5 | 3 | 1 | 15 | 15 |
| Bolivia | Med | 38 | Lower-Middle | 4.5 | 4 | 3.5 | 2.5 | 2.5 | 2 | 2 |
| Brazil | High | 13 | Upper-Middle | 2.5 | 1.5 | 2.5 | 4 | 1 | 12 | 15 |
| Chile | Very High | 11 | High | 1.5 | 2 | 2.5 | 1.5 | 1 | 17 | 17 |
| Colombia | High | 28 | Upper-Middle | 3.5 | 3.5 | 3 | 4 | 1 | 8 | 10 |
| Costa Rica | High | 20 | Upper-Middle | 1.5 | 2 | 3.5 | 2.5 | 2 | 12 | 15 |
| Ecuador | High | 23 | Upper-Middle | 3.5 | 2.5 | 4 | 4.5 | 2 | 4 | 8 |
| El Salvador | Med | 33 | Lower-Middle | 4.5 | 3.5 | 3.5 | 3 | 3 | 1 | 5 |
| Guatemala | Med | 59 | Lower-Middle | 4.5 | 2.5 | 3.5 | 3 | 3.5 | 2 | 8 |
| Honduras | Med | 66 | Lower-Middle | 4.5 | 2 | 3.5 | 2.5 | 3 | 5 | 2 |
| Mexico | High | 20 | Upper-Middle | 2 | 3 | 2 | 3 | 1 | 14 | 12 |
| Nicaragua | Med | 30 | Lower-Middle | 4.5 | 1 | 3.5 | 3.5 | 3 | 5 | 5 |
| Panama | High | 22 | Upper-Middle | 4 | 1 | 3 | 2.5 | 2.5 | 10 | 12 |
| Paraguay | Med | 29 | Upper-Middle | 2.5 | 5 | 3.5 | 2 | 1.5 | 9 | 10 |
| Peru | High | 21 | Upper-Middle | 4 | 3.5 | 4 | 2.5 | 1.5 | 5 | 5 |
| Uruguay | High | 9 | High | 2 | 1.5 | 4 | 2.5 | 2 | 11 | 16 |
| Venezuela | High | 32 | Upper-Middle | 3.5 | 1 | 2.5 | 2 | 1 | 16 | 8 |
| Country | GDP (2014–2015) | Expenditures in Health (% of Country’s GDP) | |||||
|---|---|---|---|---|---|---|---|
| Per Capita (Current US$, 2014–2015) | Public | Private | Total | Regional Rank | Per Capita | Regional Rank | |
| Argentina | 12,450 | 2.7 | 2.1 | 4.8 | 17 | 598 | 8 |
| Bolivia | 3000 | 4.6 | 1.8 | 6.4 | 13 | 192 | 16 |
| Brazil | 9900 | 3.8 | 4.5 | 8.3 | 7 | 822 | 5 |
| Chile | 14,100 | 3.9 | 3.9 | 7.8 | 9 | 1100 | 2 |
| Colombia | 7140 | 5.4 | 1.8 | 7.2 | 10 | 514 | 10 |
| Costa Rica | 10,400 | 6.8 | 2.6 | 9.4 | 2 | 978 | 3 |
| Ecuador | 6030 | 4.5 | 4.7 | 9.2 | 3 | 555 | 9 |
| El Salvador | 3800 | 4.5 | 2.3 | 6.8 | 11 | 258 | 13 |
| Guatemala | 3590 | 2.3 | 2.9 | 6.2 | 14 | 223 | 14 |
| Honduras | 2280 | 4.4 | 4.3 | 8.7 | 5 | 198 | 15 |
| Mexico | 9710 | 3.5 | 3.0 | 6.5 | 12 | 631 | 6 |
| Nicaragua | 1940 | 5.1 | 3.9 | 9.0 | 4 | 175 | 17 |
| Panama | 11,800 | 5.9 | 2.2 | 8.1 | 8 | 962 | 4 |
| Paraguay | 4190 | 4.5 | 5.3 | 9.8 | 1 | 411 | 11 |
| Perú | 6130 | 3.3 | 2.2 | 5.5 | 15 | 337 | 12 |
| Uruguay | 15,720 | 6.1 | 2.5 | 8.6 | 6 | 1352 | 1 |
| Venezuela | 11,780 | 1.5 | 3.7 | 5.2 | 16 | 613 | 7 |
| Median | 7140 | 4.5 | 2.9 | 7.8 | 555 | ||
| Country | GNI Per Capita (PPP) 2017 [39] | HDI 2016 [32] | CRI-2018 (1997–2016) [30] | LPHI 2017 [33] | EM-DAT Statistics 2018 [29] | Freq. Per Year | Geographical Exposure Classed as Pop. Density (PD) 1: Very Low 5: Very High | ||
|---|---|---|---|---|---|---|---|---|---|
| US$ × 1000 | Value/Reg. Rank | Reg. Rank | Fatal. Per M inh/Ranked Class | Reg Rank | Nb of Extreme Events. Time-Horizons: A: 1988–2017, B: 1997–2016 | Freq. over A Trend From A to B | |||
| A | B | Classed PD | |||||||
| Argentina | 20.3 | 0.83/2 | 5 | 0.7/1 | 6 | 76 | 57 | 2.5 ↗ | 1 |
| Bolivia | 7.3 | 0.67/14 | 13 | 0.45/13 | 17 | 66 | 48 | 2.2 ↗ | 2.5 |
| Brazil | 15.2 | 0.75/8 | 4 | 0.8/3 | 10 | 151 | 101 | 3.4 ≈ | 1 |
| Chile | 23.2 | 0.85/1 | 3 | 0.06/2 | 3 | 58 | 42 | 1.9 ↗ | 2 |
| Colombia | 14.2 | 0.73/11 | 10 | 2.4/9 | 7 | 101 | 67 | 1.9 ≈ | 3 |
| Costa Rica | 17.3 | 0.78/5 | 1 | 1.4/5 | 1 | 40 | 26 | 1.3 ≈ | 4 |
| Ecuador | 11.3 | 0.74 /9 | 9 | 2.9/11 | 9 | 44 | 28 | 1.5 ≈ | 4 |
| El Salvador | 7.5 | 0.68/13 | 14 | 5.3/14 | 8 | 46 | 28 | 1.5 ≈ | 5 |
| Guatemala | 8.0 | 0.64/16 | 15 | 7.2/15 | 16 | 67 | 48 | 2.2 ≈ | 4.5 |
| Honduras | 4.6 | 0.63/17 | 17 | 43/17 | 12 | 63 | 38 | 2.1 ↘ | 5 |
| Mexico | 17.7 | 0.76/7 | 11 | 1.3/4 | 5 | 169 | 126 | 4.2 ≈ | 2 |
| Nicaragua | 5.7 | 0.65/15 | 16 | 29.6/16 | 14 | 55 | 36 | 1.8 ≈ | 5 |
| Panama | 21.9 | 0.79/4 | 2 | 2.8/10 | 11 | 41 | 32 | 1.4 ↗ | 4 |
| Paraguay | 9.2 | 0.69/12 | 12 | 0.15/6 | 4 | 42 | 29 | 1.4 ≈ | 3 |
| Perú | 12.9 | 0.74/9 | 7 | 3.9/12 | 13 | 90 | 59 | 2.0 ≈ | 3 |
| Uruguay | 21.9 | 0.80/3 | 6 | 2/6 | 2 | 26 | 22 | 0.9 ↗ | 3.5 |
| Venezuela | NA | 0.77/6 | 8 | 2/8 | 15 | 40 | 26 | 1.3 ≈ | 1.5 |
| Country | TAP Nb of Top-Ten Extreme Weather Events | |||||||
|---|---|---|---|---|---|---|---|---|
| (Million People) Due to Top-Ten Events | Types of EWEs | TAP (%) | ||||||
| Rank | Nb of EWEs | Floods | Storms | Droughts | Landslides | Country-Level | ||
| Argentina | 6.6 | 5th | 10 | 10 | 0 | 0 | 0 | 15 |
| Bolivia | 2.7 | 8th | 10 | 7 | 0 | 3 | 0 | 25 |
| Brazil | 50.5 | 1st | 9 | 4 | 0 | 5 | 0 | 24 |
| Chile | 0.9 | 13th | 7 | 6 | 0 | 0 | 1 | 5 |
| Colombia | 9.1 | 4th | 9 | 9 | 0 | 0 | 0 | 18 |
| Costa Rica | 1.3 | 12st | 9 | 4 | 5 | 0 | 0 | 26 |
| Ecuador | 0.7 | 15th | 5 | 2 | 0 | 1 | 1 | 4 |
| El Salvador | 1.7 | 11th | 7 | 1 | 3 | 2 | 0 | 28 |
| Guatemala | 5.9 | 7th | 9 | 2 | 3 | 4 | 0 | 35 |
| Honduras | 6.0 | 6th | 10 | 3 | 3 | 4 | 0 | 67 |
| Mexico | 10.7 | 3rd | 10 | 3 | 6 | 1 | 0 | 8 |
| Nicaragua | 2.7 | 8th | 9 | 2 | 4 | 3 | 0 | 45 |
| Panama | 0.13 | 17th | 9 | 7 | 2 | 0 | 0 | 26 |
| Paraguay | 2.6 | 10th | 10 | 5 | 0 | 3 | 0 | 18 |
| Perú | 12.3 | 2nd | 9 | 3 | 1 | 2 | 0 | 38 |
| Uruguay | 0.19 | 16th | 10 | 10 | 0 | 0 | 0 | 5 |
| Venezuela | 0.9 | 13th | 10 | 9 | 0 | 0 | 0 | 3 |
| Total | 152 | 87 | 27 | 28 | 2 | Median: | ||
| % | 89 | 57 | 18 | 18 | 1 | 24 | ||
| Question/Statement | The Extent to Which the Participants Agree with the Statement (in %) | ||||
| Strongly Agree | Agree | Neither Agree nor Disagree | Disagree | Strongly Disagree | |
| “There is a connection between climate change and health.” | 86 | 12 | 2 | 0 | 0 |
| “There is enough information for the public about the health impacts of extreme events in my country.” | 2 | 16 | 12 | 48 | 22 |
| “I think the health system of my country is well-prepared and equipped to face health impacts from weather extremes and sea level rise.” | 2 | 4 | 12 | 50 | 32 |
| “I think the government of my country is doing enough to deal with the health impacts from weather extremes and sea level rise.” | 0 | 4 | 10 | 46 | 40 |
| “Is there anything else that you suggest could be done to ensure to protect human health and wellbeing from the impacts of extreme events?” | Yes | No | I don’t know | ||
| 82 | 6 | 12 | |||
| What could be done to ensure to protect human health and wellbeing from the impacts of extreme events? | |||||
| Suggestions made to ensure to protect human health and well-being from the impacts of extreme events | |||||
| Suggestion | Example | % | |||
| 1. Health capabilities | Health capacities; Promoting Health; Epidemiology of the identified priority vector-borne zoonotic diseases | 16 | |||
| 2. Climate Literacy | Climate Change Education; Information and Media; Training and Lifelong Learning | 16 | |||
| 3. Information systems in a changing climate | 13 | ||||
| 4. Early Warning Systems | 12 | ||||
| 5. Risk Assessment | 6 | ||||
| 6. Management and communication | 6 | ||||
| 7. Preparedness | 4 | ||||
| 8. Effective Implementation of National/Local Adaptation Plans (NAPs/LAPs) | Sectoral strategies (namely Agriculture, Health, and Economy) | 4 | |||
| 9. Climate Change Research and Capacity Building | 4 | ||||
| 10. Partnerships and participation | Stakeholders and partnerships. Participation in building resilience in a changing climate | 4 | |||
| 11. Others | 15 | ||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagy, G.J.; Filho, W.L.; Azeiteiro, U.M.; Heimfarth, J.; Verocai, J.E.; Li, C. An Assessment of the Relationships between Extreme Weather Events, Vulnerability, and the Impacts on Human Wellbeing in Latin America. Int. J. Environ. Res. Public Health 2018, 15, 1802. https://doi.org/10.3390/ijerph15091802
Nagy GJ, Filho WL, Azeiteiro UM, Heimfarth J, Verocai JE, Li C. An Assessment of the Relationships between Extreme Weather Events, Vulnerability, and the Impacts on Human Wellbeing in Latin America. International Journal of Environmental Research and Public Health. 2018; 15(9):1802. https://doi.org/10.3390/ijerph15091802
Chicago/Turabian StyleNagy, Gustavo J., Walter Leal Filho, Ulisses M. Azeiteiro, Johanna Heimfarth, José E. Verocai, and Chunlan Li. 2018. "An Assessment of the Relationships between Extreme Weather Events, Vulnerability, and the Impacts on Human Wellbeing in Latin America" International Journal of Environmental Research and Public Health 15, no. 9: 1802. https://doi.org/10.3390/ijerph15091802
APA StyleNagy, G. J., Filho, W. L., Azeiteiro, U. M., Heimfarth, J., Verocai, J. E., & Li, C. (2018). An Assessment of the Relationships between Extreme Weather Events, Vulnerability, and the Impacts on Human Wellbeing in Latin America. International Journal of Environmental Research and Public Health, 15(9), 1802. https://doi.org/10.3390/ijerph15091802