Risk Reduction Behaviors Regarding PM2.5 Exposure among Outdoor Exercisers in the Nanjing Metropolitan Area, China

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
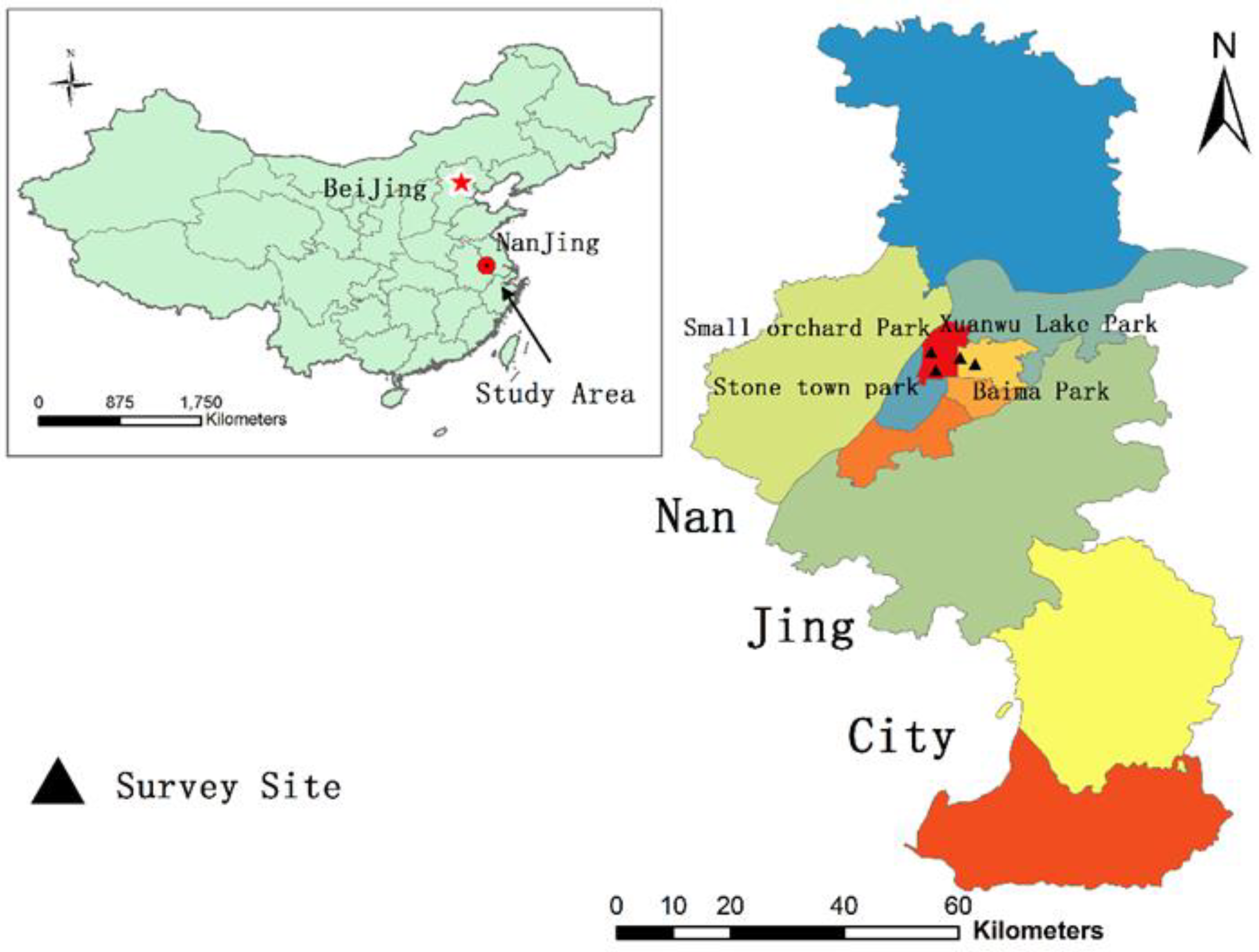
2.1. Study Design
2.2. Data Collection and Measures
2.3. Statistical Analysis
3. Results
3.1. Socio-Demographic Characteristics of the Study Population
3.2. Outdoor Physical Exercise Habits
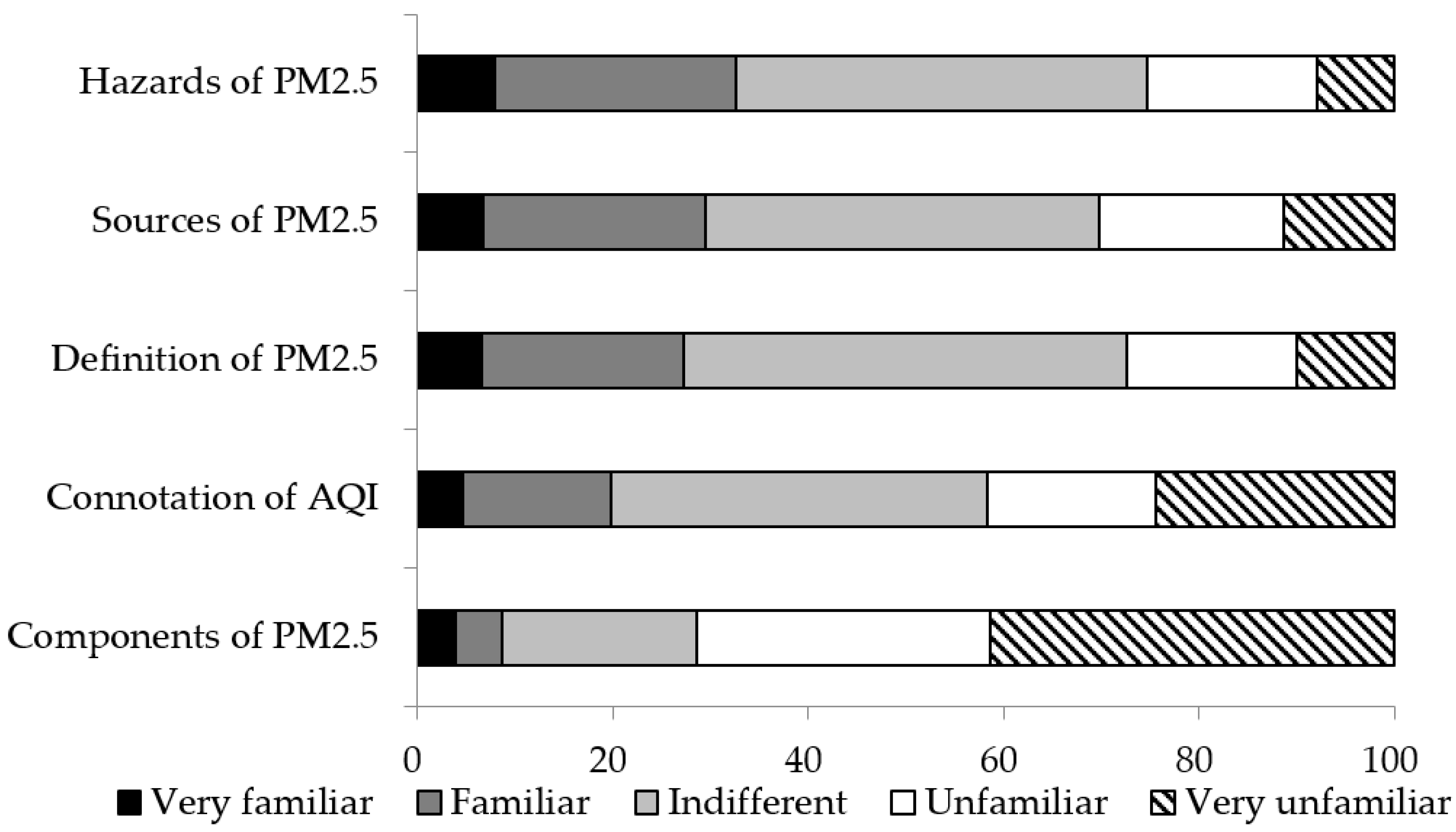
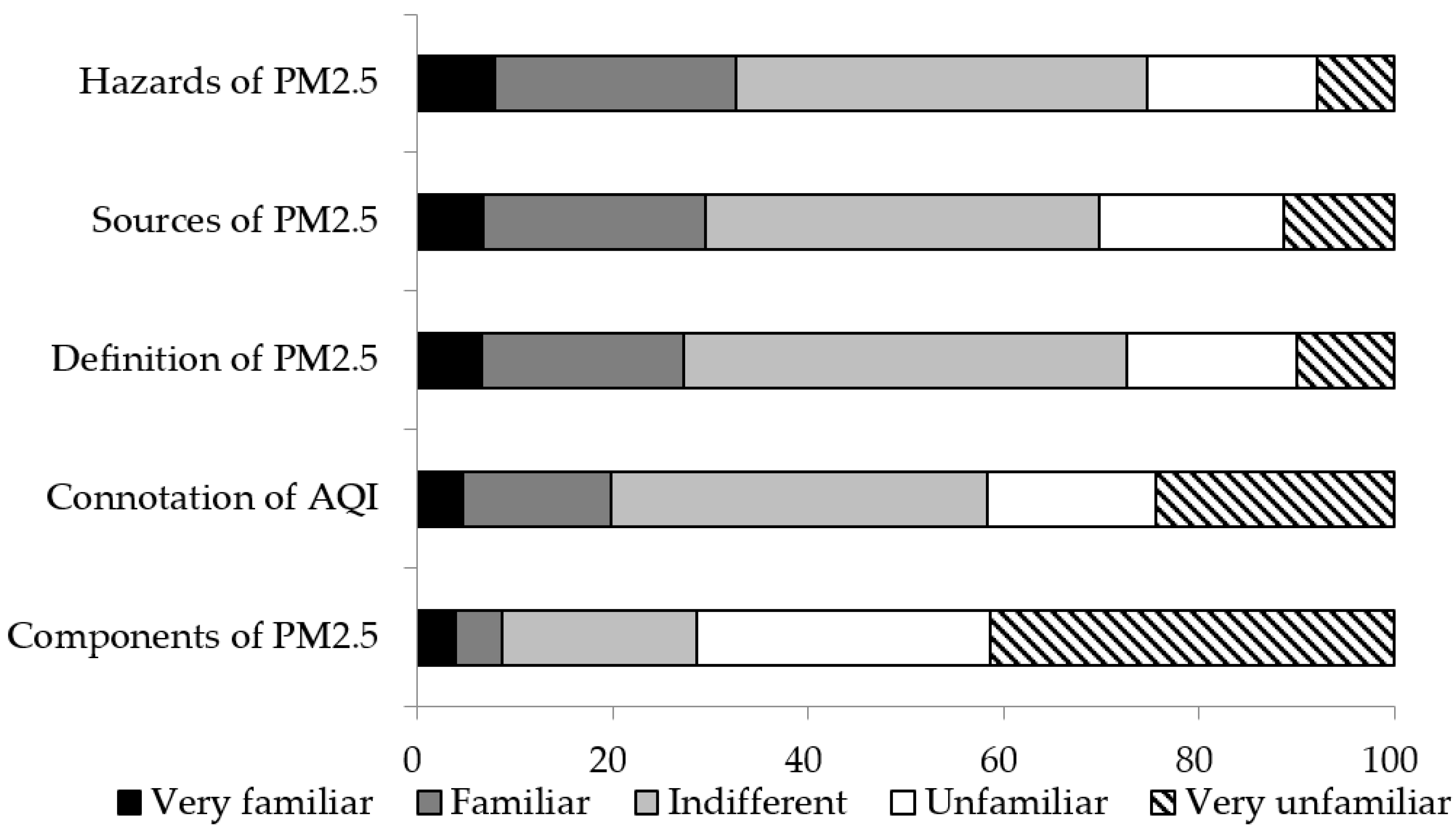
3.3. Self-Reported Extent of Knowledge about PM2.5
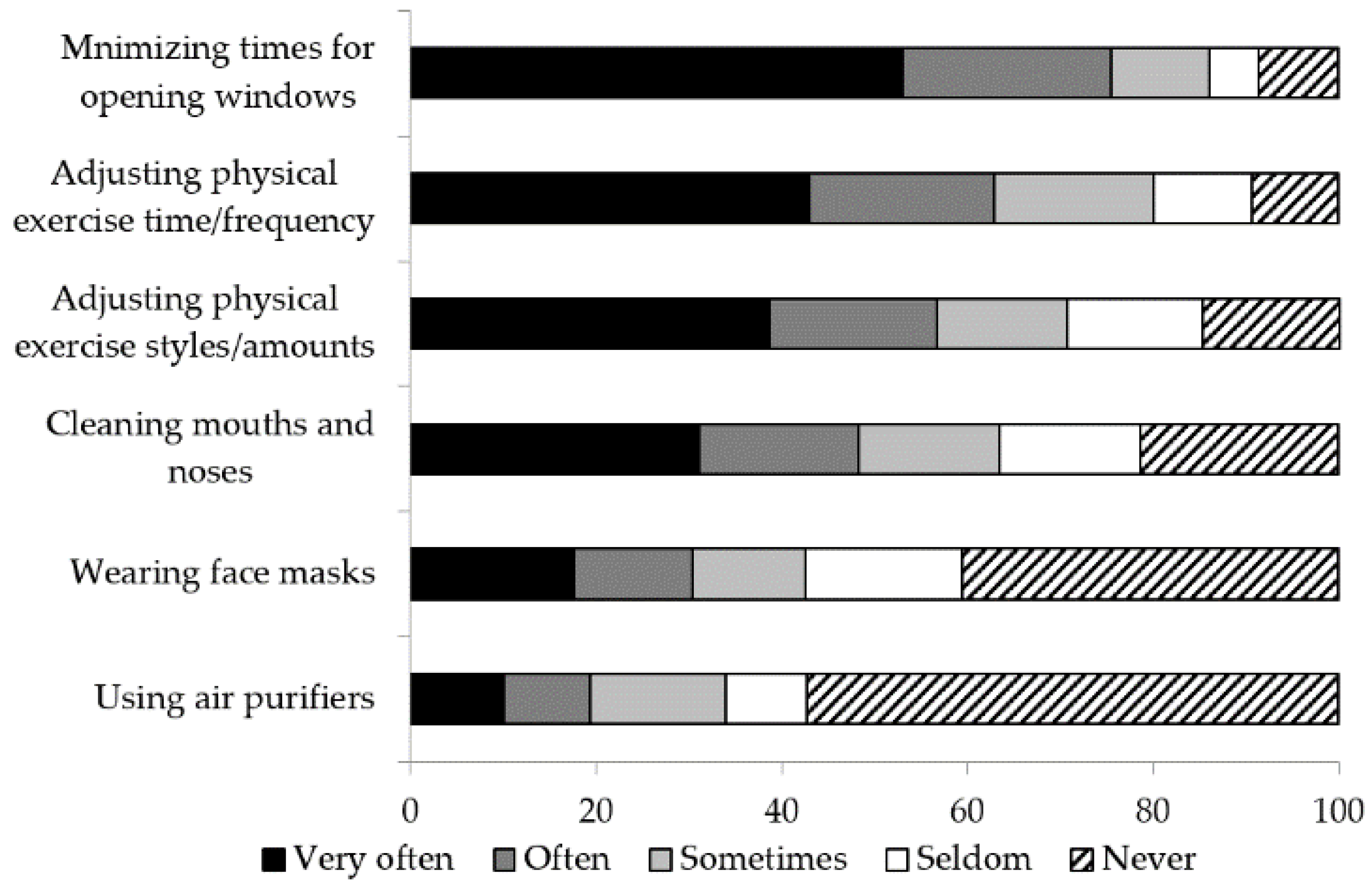
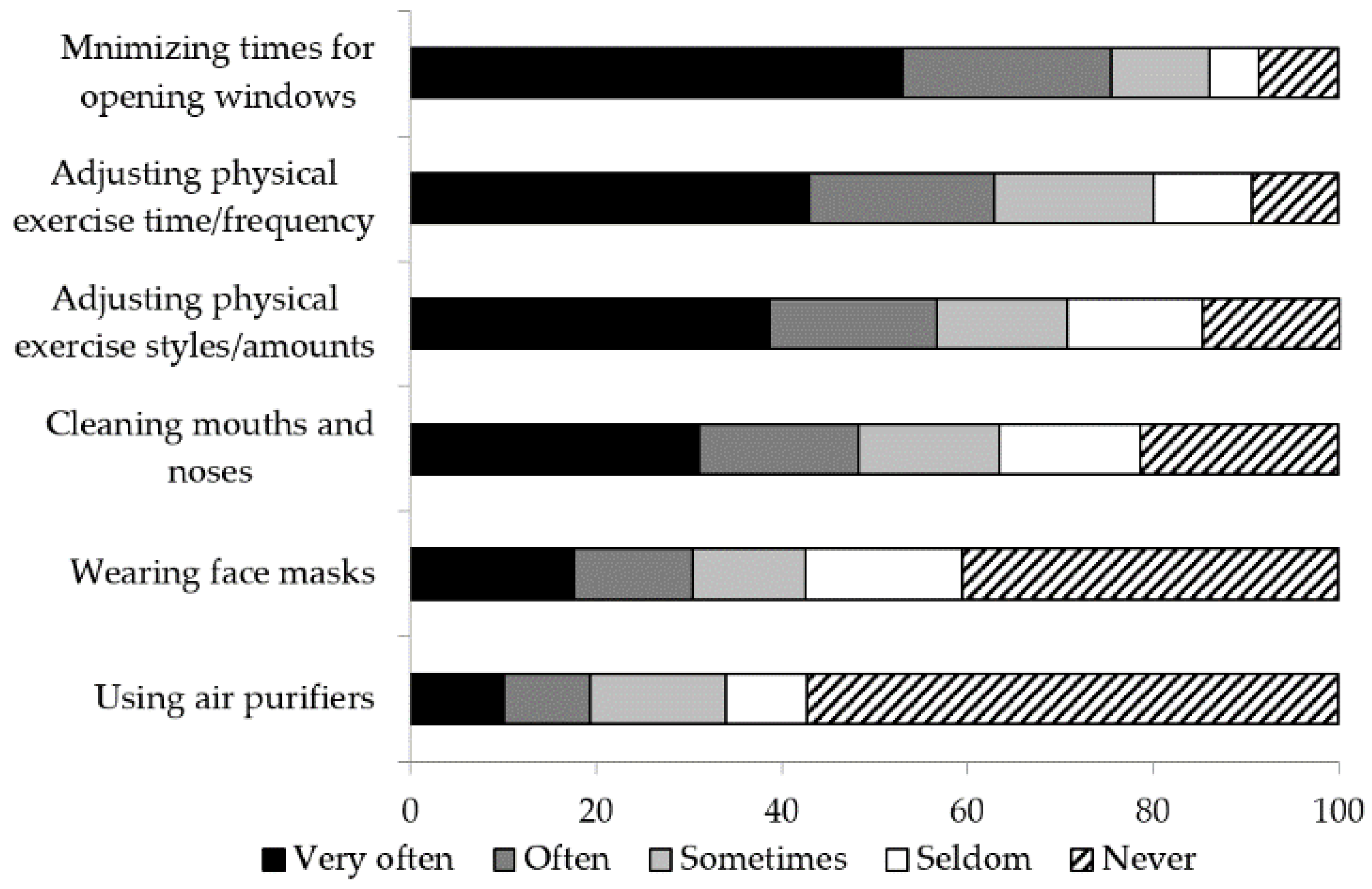
3.4. Risk Reduction Behavior of PM2.5
3.5. Factors that Influence the Adoption of Risk Reduction Behavior Regarding PM2.5
4. Discussion
4.1. Self-Reported the Extent of Knowledge and Risk Reduction Behavior of PM2.5
4.2. Predictor of the High-Level Risk Reduction Behavior
4.3. Limitations and Strength
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wang, J.; Zhao, B.; Wang, S.; Yang, F.; Xing, J.; Morawska, L.; Ding, A.; Kulmala, M.; Kerminen, V.M.; Kujansuu, J.; et al. Particulate matter pollution over China and the effects of control policies. Sci. Total Environ. 2017, 426–447, 584–585. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Huang, Y.; Ma, Z.; Jin, Z.; Liu, X.; Wang, H.; Liu, Y.; Wang, J.; Jantunen, M.; Bi, J.; et al. Spatial and temporal trends in the mortality burden of air pollution in China: 2004–2012. Environ. Int. 2017, 98, 75–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.; Chen, R.; Zhao, Y.; Ma, Z.; Bi, J.; Liu, Y.; Meng, X.; Wang, Y.; Chen, X.; Li, W.; et al. Associations between ambient fine particulate air pollution and hypertension: A nationwide cross-sectional study in China. Sci. Total Environ. 2017, 584–585, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Zhang, Y.; Zhang, W.; Li, S.; Williams, G.; Marks, G.B.; Jalaludin, B.; Abramson, M.J.; Luo, F.; Yang, D.; et al. Attributable risks of emergency hospital visits due to air pollutants in China: A multi-city study. Environ. Pollut. 2017, 228, 43–49. [Google Scholar] [CrossRef] [PubMed]
- He, M.Z.; Zeng, X.; Zhang, K.; Kinney, P.L. Fine Particulate Matter Concentrations in Urban Chinese Cities, 2005–2016: A Systematic Review. Int. J. Environ. Res. Public Health 2017, 14, 191. [Google Scholar] [CrossRef] [PubMed]
- Sinkemani, R.; Sinkemani, A.; Li, X.; Chen, R. Risk of Cardiovascular Disease Associated with the Exposure of Particulate Matter (PM2.5). J. Environ. Prot. 2018, 9, 607–618. [Google Scholar] [CrossRef]
- Khalili, R.; Bartell, S.M.; Hu, X.; Liu, Y.; Chang, H.H.; Belanoff, C.; Strickland, M.J.; Vieira, V.M. Early-life exposure to PM2.5 and risk of acute asthma clinical encounters among children in Massachusetts: A case-crossover analysis. Environ. Health 2018, 17, 20. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.; Xu, D.; Cheng, Y.; Dong, S.; Guo, C.; Jiang, X.; Zheng, X. Systematic review and meta-analysis of the adverse health effects of ambient PM2.5 and PM10 pollution in the Chinese population. Environ. Res. 2015, 136, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.Q.; Mei, X.D.; Feng, D. Air pollution and chronic airway diseases: What should people know and do? J. Thorac. Dis. 2016, 8, E31–E40. [Google Scholar] [PubMed]
- Wang, T.; Xia, Z.; Wu, M.; Zhang, Q.; Sun, S.; Yin, J.; Zhou, Y.; Yang, H. Pollution characteristics, sources and lung cancer risk of atmospheric polycyclic aromatic hydrocarbons in a new urban district of Nanjing, China. J. Environ. Sci. 2017, 55, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Aydin, S.; Cingi, C.; San, T.; Ulusoy, S.; Orhan, İ. The effects of air pollutants on nasal functions of outdoor runners. Eur. Arch. Oto-Rhino-Laryngol. 2014, 271, 713–717. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Liang, L.; Feng, Y.; Li, R.; Liu, Y. Air Pollution Exposure and Physical Activity in China: Current Knowledge, Public Health Implications, and Future Research Needs. Int. J. Environ. Res. Public Health 2015, 12, 14887–14897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, K.M.; Thompson, A.M.; Blair, S.N.; Sallis, J.F.; Powell, K.E.; Bull, F.C.; Bauman, A.E. Sport and exercise as contributors to the health of nations. Lancet 2012, 380, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Williams, P.T. Dose-response relationship of physical activity to premature and total all-cause and cardiovascular disease mortality in walkers. PLoS ONE 2013, 8, e78777. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.K.; Elumalai, S.P. Size-segregated particulate matter and its association with respiratory deposition doses among outdoor exercisers in Dhanbad City, India. J. Air Waste Manag. Assoc. 2017, 67, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Li, L.; Gao, W.; Wang, Y.; Yao, X. Interventions to reduce individual exposure of elderly individuals and children to haze: A review. J. Thorac. Dis. 2016, 8, E62–E68. [Google Scholar] [PubMed]
- Krewski, D.; Jerrett, M.; Burnett, R.T.; Ma, R.; Hughes, E.; Shi, Y.; Turner, M.C.; Pope, C.A.; Thurston, G.; Calle, E.E.; et al. Extended Follow-Up and Spatial Analysis of the American Cancer Society Study Linking Particulate Air Pollution and Mortality (No. 140); Health Effects Institute: Boston, MA, USA, 2009. [Google Scholar]
- Pope, C.A.; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 2002, 287, 1132–1141. [Google Scholar] [CrossRef] [PubMed]
- Cai, D.P.; He, Y.M. Daily lifestyles in the fog and haze weather. J. Thorac. Dis. 2016, 8, E75–77. [Google Scholar] [PubMed]
- Zhou, G.; Gan, Y.; Ke, Q.; Knoll, N.; Lonsdale, C.; Schwarzer, R. Avoiding exposure to air pollution by using filtering facemask respirators: An application of the health action process approach. Health Psychol. 2016, 35, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.; Shibata, T.; Wilson, J.; Maidin, A. Challenges in evaluating PM concentration levels, commuting exposure, and mask efficacy in reducing PM exposure in growing, urban communities in a developing country. Sci. Total Environ. 2016, 543, 416–424. [Google Scholar] [CrossRef] [PubMed]
- Laumbach, R.; Meng, Q.; Kipen, H. What can individuals do to reduce personal health risks from air pollution? J. Thorac. Dis. 2015, 7, 96–107. [Google Scholar] [PubMed]
- Zhao, X.G.; Duan, X.L.; Wang, B.B.; Jiang, Y.; Wang, L.M.; Tian-Xin, L.I.; Guo, J. Study on environmental exposure-related activity patterns of Chinese adults. J. Environ. Health 2014, 31, 941–944. [Google Scholar]
- Ministry of Environmental Protection of the People’s Republic of China. Report of Environmental Exposure Related Activity Patterns Research of Chinese Population (Adults); China Environmental Science Press: Beijing, China, 2013.
- Huang, L.; Rao, C.; van der Kuijp, T.J.; Bi, J.; Liu, Y. A comparison of individual exposure, perception, and acceptable levels of PM2.5 with air pollution policy objectives in China. Environ. Res. 2017, 157, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Qian, X.J.; Xu, G.Z.; Li, L.; Shen, Y.P.; He, T.F.; Liang, Y.J.; Yang, Z.Y.; Zhou, W.W.; Xu, J.Y. Knowledge and perceptions of air pollution in Ningbo, China. BMC Public Health 2016, 16, 1138. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.B. Experience with urban air pollution in Paterson, New Jersey and implications for air pollution communication. Risk Anal. 2012, 32, 39–53. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.J.; Balluz, L.; Mokdad, A. Association between media alerts of air quality index and change of outdoor activity among adult asthma in six states, BRFSS, 2005. J. Community Health 2009, 34, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Zhou, L.; Chen, X.; Bi, J.; Kinney, P.L. Acute effect of ozone exposure on daily mortality in seven cities of Jiangsu Province, China: No clear evidence for threshold. Environ. Res. 2017, 155, 235–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, F.; Meng, D.; Li, X.; Tan, J. Indoor-outdoor relationships of PM2.5 in four residential dwellings in winter in the Yangtze River Delta, China. Environ. Pollut. 2016, 215, 280–289. [Google Scholar] [CrossRef] [PubMed]
- Lou, C.R.; Liu, H.Y.; Li, Y.F.; Li, Y.L. Socioeconomic Drivers of PM2.5 in the Accumulation Phase of Air Pollution Episodes in the Yangtze River Delta of China. Int. J. Environ. Res. Public Health 2016, 13, 928. [Google Scholar] [CrossRef] [PubMed]
- Kang, F.; Mao, X.; Wang, X.; Wang, J.; Yang, B.; Gao, Y. Sources and health risks of polycyclic aromatic hydrocarbons during haze days in eastern China: A 1-year case study in Nanjing City. Ecotoxicol. Environ. Saf. 2017, 140, 76–83. [Google Scholar] [CrossRef] [PubMed]
- An, J.; Shi, Y.; Wang, J.; Zhu, B. Temporal Variations of O3 and NOx in the Urban Background Atmosphere of Nanjing, East China. Archiv. Environ. Contam. Toxicol. 2016, 71, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Huang, Y.; Jin, Z.; Ma, Z.; Liu, X.; Zhang, B.; Liu, Y.; Yu, Y.; Wang, J.; Bi, J.; et al. The nexus between urbanization and PM2.5 related mortality in China. Environ. Pollut. 2017, 227, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; He, J.; Lu, X.; She, J.; Guan, Z. Spatial and Temporal Variations of PM2.5 and Its Relation to Meteorological Factors in the Urban Area of Nanjing, China. Int. J. Environ. Res. Public Health 2016, 13, 921. [Google Scholar] [CrossRef] [PubMed]
- National Bureau of Statistics of China. 2016 Statistical Yearbook of Nanjing; China Statistics Press: Beijing, China, 2016.
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Antoni, D.; Smith, L.; Auyeung, V.; Weinman, J. Psychosocial and demographic predictors of adherence and non-adherence to health advice accompanying air quality warning systems: A systematic review. Environ. Health 2017, 16, 100. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Li, X.; Zhu, T.; Han, Y.; Lv, D. PM2.5-bound PAHs in three indoor and one outdoor air in Beijing: Concentration, source and health risk assessment. Sci. Total Environ. 2017, 586, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Gao, P.; Lei, T.; Jia, L.; Song, Y.; Lin, N.; Du, Y.; Feng, Y.; Zhang, Z.; Cui, F. Exposure and health risk assessment of PM2.5-bound trace metals during winter in university campus in Northeast China. Sci. Total Environ. 2017, 576, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.T.; Folmer, H.; Xue, J.H. Perception of Air Pollution in the Jinchuan Mining Area, China: A Structural Equation Modeling Approach. Int. J. Environ. Res. Public Health 2016, 13, 735. [Google Scholar] [CrossRef] [PubMed]
- Ji, W.; Zhao, B. Contribution of outdoor-originating particles, indoor-emitted particles and indoor secondary organic aerosol (SOA) to residential indoor PM2.5 concentration: A model-based estimation. Build. Environ. 2015, 90, 196–205. [Google Scholar] [CrossRef]
- Shi, J.J.; Yuan, D.; Zhao, Z.H. Residential indoor PM2.5 sources, concentration and influencing factors in China. J. Environ. Health 2015, 32, 825–829. [Google Scholar]
- Chen, R.; Zhao, A.; Chen, H.; Zhao, Z.; Cai, J.; Wang, C.; Yang, C.; Li, H.; Xu, X.; Ha, S.; et al. Cardiopulmonary benefits of reducing indoor particles of outdoor origin: A randomized, double-blind crossover trial of air purifiers. J. Am. Coll. Cardiol. 2015, 65, 2279–2287. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Cai, J.; Chen, R.; Zhao, Z.; Ying, Z.; Wang, L.; Chen, J.; Hao, K.; Kinney, P.L.; Chen, H.; et al. Particulate Matter Exposure and Stress Hormone Levels: A Randomized, Double-Blind, Crossover Trial of Air Purification. Circulation 2017, 136, 618–627. [Google Scholar] [CrossRef] [PubMed]
- De Pretto, L.; Acreman, S.; Ashfold, M.J.; Mohankumar, S.K.; Campos-Arceiz, A. The Link between Knowledge, Attitudes and Practices in Relation to Atmospheric Haze Pollution in Peninsular Malaysia. PLoS ONE 2015, 10, e0143655. [Google Scholar] [CrossRef] [PubMed]
- Sheeran, P.; Harris, P.R.; Epton, T. Does heightening risk appraisals change people’s intentions and behavior? A meta-analysis of experimental studies. Psychol. Bull. 2014, 140, 511–543. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | No. (%) | (N = 302) |
|---|---|---|
| Gender | ||
| Male | 52.3 | 158 |
| Female | 47.7 | 144 |
| Age group | ||
| ≤50 years old | 25.2 | 76 |
| 51–60 years old | 27.8 | 84 |
| 61–70 years old | 24.5 | 74 |
| ≥71 years old | 22.5 | 68 |
| Occupation | ||
| Government staff | 35.1 | 106 |
| Company employee | 42.4 | 128 |
| Self-Employed | 22.5 | 68 |
| Educational level | ||
| Junior high school or below | 26.5 | 80 |
| High school | 31.1 | 94 |
| Junior college | 19.9 | 60 |
| College or above | 22.5 | 68 |
| Whether or not have chronic illness | ||
| Yes | 53.0 | 160 |
| No | 47.0 | 142 |
| No. (%) | (N = 300) | |
| Whether or not household with chronic illness patients | ||
| Yes | 49.3 | 148 |
| No | 50.7 | 152 |
| Living area | ||
| Urban area | 92.7 | 278 |
| Rural area | 2.0 | 6 |
| Urban-rural marginal area | 5.3 | 16 |
| No. (%) | (N = 298) | |
| Individual income per month | ||
| ≤RMB 3000 | 27.5 | 82 |
| RMB 3001–5000 | 38.9 | 116 |
| RMB 5001–8000 | 24.8 | 74 |
| ≥RMB 8001 | 8.7 | 26 |
| Smoking status | ||
| None-smoker | 64.4 | 192 |
| Ex-smoker | 12.8 | 38 |
| ≤10 cigarettes smoked per day | 13.4 | 40 |
| >10 cigarettes smoked per day | 9.4 | 28 |
| Whether or not household with children | ||
| Yes | 14.8 | 44 |
| No | 85.2 | 254 |
| Characteristic | No. (%) | N |
|---|---|---|
| Average days spent on outdoor physical exercise per week | 298 | |
| <1 day | 3.4 | 10 |
| 2–3 days | 14.1 | 42 |
| 4–5 days | 20.8 | 62 |
| 6–7 days | 61.7 | 184 |
| Average time spent on outdoor physical exercise each time | 298 | |
| <30 min | 4.7 | 14 |
| 30 min–1 h | 36.9 | 110 |
| 1–2 h | 43.6 | 130 |
| >2 h | 14.8 | 44 |
| Period of outdoor physical exercise | 302 | |
| Before 8 a.m. | 43.4 | 131 |
| 8 a.m.–1 p.m. | 5.6 | 17 |
| 1–6 p.m. | 4.6 | 14 |
| After 6 p.m. | 46.4 | 140 |
| Physical exercise styles | 302 | |
| Walking | 39.1 | 118 |
| Running or brisk walking | 23.8 | 72 |
| Dancing | 7.9 | 24 |
| Two or more ways | 29.2 | 88 |
| Characteristic | Lower-Level | Higher-Level | p | OR | 95% CI | |
|---|---|---|---|---|---|---|
| No. (%) (N) | No. (%) (N) | Lower | Upper | |||
| Gender | ||||||
| Male (Reference) | 53.3 (82) | 46.8 (72) | ||||
| Female | 27.5 (38) | 72.5 (100) | 0.002 ** | 3.22 | 1.53 | 6.78 |
| Age group | ||||||
| ≤50 years old (Reference) | 50.0 (38) | 50.0 (38) | ||||
| 50–60 years old | 23.7 (18) | 76.3 (58) | 0.030 ** | 2.53 | 1.10 | 5.85 |
| 60–70 years old | 35.1 (26) | 64.9 (48) | 0.165 | 1.78 | 0.79 | 4.02 |
| ≥71 years old | 57.6 (38) | 42.4 (28) | 0.408 | 0.70 | 0.30 | 1.62 |
| Occupation | ||||||
| Government staff (Reference) | 36.0 (36) | 64.0 (64) | ||||
| Company employee | 36.5 (46) | 63.5 (80) | 0.476 | 1.35 | 0.59 | 3.06 |
| Self-Employed | 57.6 (38) | 42.5 (28) | 0.201 | 1.65 | 0.77 | 3.54 |
| Educational level | ||||||
| Junior high school (Reference) or below | 48.7 (38) | 51.3 (40) | 0.217 | 0.55 | 0.21 | 1.43 |
| High school | 40.0 (36) | 60.0 (54) | 0.809 | 0.90 | 0.38 | 2.13 |
| Junior college | 37.9 (22) | 62.1 (36) | 0.888 | 0.94 | 0.37 | 2.38 |
| College or above | 36.4 (24) | 63.6 (42) | 0.217 | 0.55 | 0.21 | 1.43 |
| Smoking status | ||||||
| None-smoker (Reference) | 31.1 (58) | 68.9 (128) | ||||
| Ex-smoker | 50.0 (20) | 50.0 (20) | 0.288 | 2.36 | 0.49 | 11.43 |
| ≤10 cigarettes smoked per day | 57.9 (22) | 42.1 (16) | 0.170 | 3.51 | 0.59 | 21.05 |
| >10 cigarettes smoked per day | 71.4 (20) | 28.6 (8) | 0.719 | 1.38 | 0.24 | 7.93 |
| Individual income per month | ||||||
| ≤RMB 3000 (Reference) | 35.5 (27) | 64.5 (50) | 0.945 | 0.94 | 0.16 | 5.52 |
| RMB 3001–5000 | 42.6 (49) | 57.4 (66) | 0.453 | 0.55 | 0.12 | 2.62 |
| RMB 5001–8000 | 49.3 (36) | 50.7 (37) | 0.473 | 0.57 | 0.12 | 2.66 |
| ≥RMB 8001 | 29.6 (8) | 70.4 (19) | 0.945 | 0.94 | 0.16 | 5.52 |
| Whether or not have chronic illness | ||||||
| No (Reference) | 43.4 (66) | 56.6 (86) | ||||
| Yes | 38.6 (54) | 61.4 (86) | 0.922 | 1.04 | 0.43 | 2.52 |
| Whether or not household with chronic illness patients | ||||||
| No (Reference) | 41.5 (61) | 58.8 (86) | ||||
| Yes | 40.7 (59) | 59.3 (86) | 0.758 | 1.11 | 0.59 | 2.09 |
| Whether or not household with children | ||||||
| No (Reference) | 43.6 (108) | 56.5 (140) | ||||
| Yes | 27.3 (12) | 72.7 (32) | 0.035 ** | 2.59 | 1.07 | 6.26 |
| Self-reported the extent of knowledge about PM2.5 | ||||||
| Very low (Reference) | 56.3 (36) | 43.8 (28) | ||||
| Low | 46.7 (70) | 53.3 (80) | 0.116 | 1.80 | 0.87 | 3.76 |
| High | 20.0 (12) | 80.0 (48) | 0.000 ** | 7.55 | 2.64 | 21.60 |
| Very high | 11.1 (2) | 88.9 (16) | 0.005 ** | 12.70 | 2.14 | 75.17 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiong, L.; Li, J.; Xia, T.; Hu, X.; Wang, Y.; Sun, M.; Tang, M. Risk Reduction Behaviors Regarding PM2.5 Exposure among Outdoor Exercisers in the Nanjing Metropolitan Area, China. Int. J. Environ. Res. Public Health 2018, 15, 1728. https://doi.org/10.3390/ijerph15081728
Xiong L, Li J, Xia T, Hu X, Wang Y, Sun M, Tang M. Risk Reduction Behaviors Regarding PM2.5 Exposure among Outdoor Exercisers in the Nanjing Metropolitan Area, China. International Journal of Environmental Research and Public Health. 2018; 15(8):1728. https://doi.org/10.3390/ijerph15081728
Chicago/Turabian StyleXiong, Lilin, Jie Li, Ting Xia, Xinyue Hu, Yan Wang, Maonan Sun, and Meng Tang. 2018. "Risk Reduction Behaviors Regarding PM2.5 Exposure among Outdoor Exercisers in the Nanjing Metropolitan Area, China" International Journal of Environmental Research and Public Health 15, no. 8: 1728. https://doi.org/10.3390/ijerph15081728