A Nationwide Registry-Based Study on Mortality Due to Rare Congenital Anomalies

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
Research Ethics
3. Results
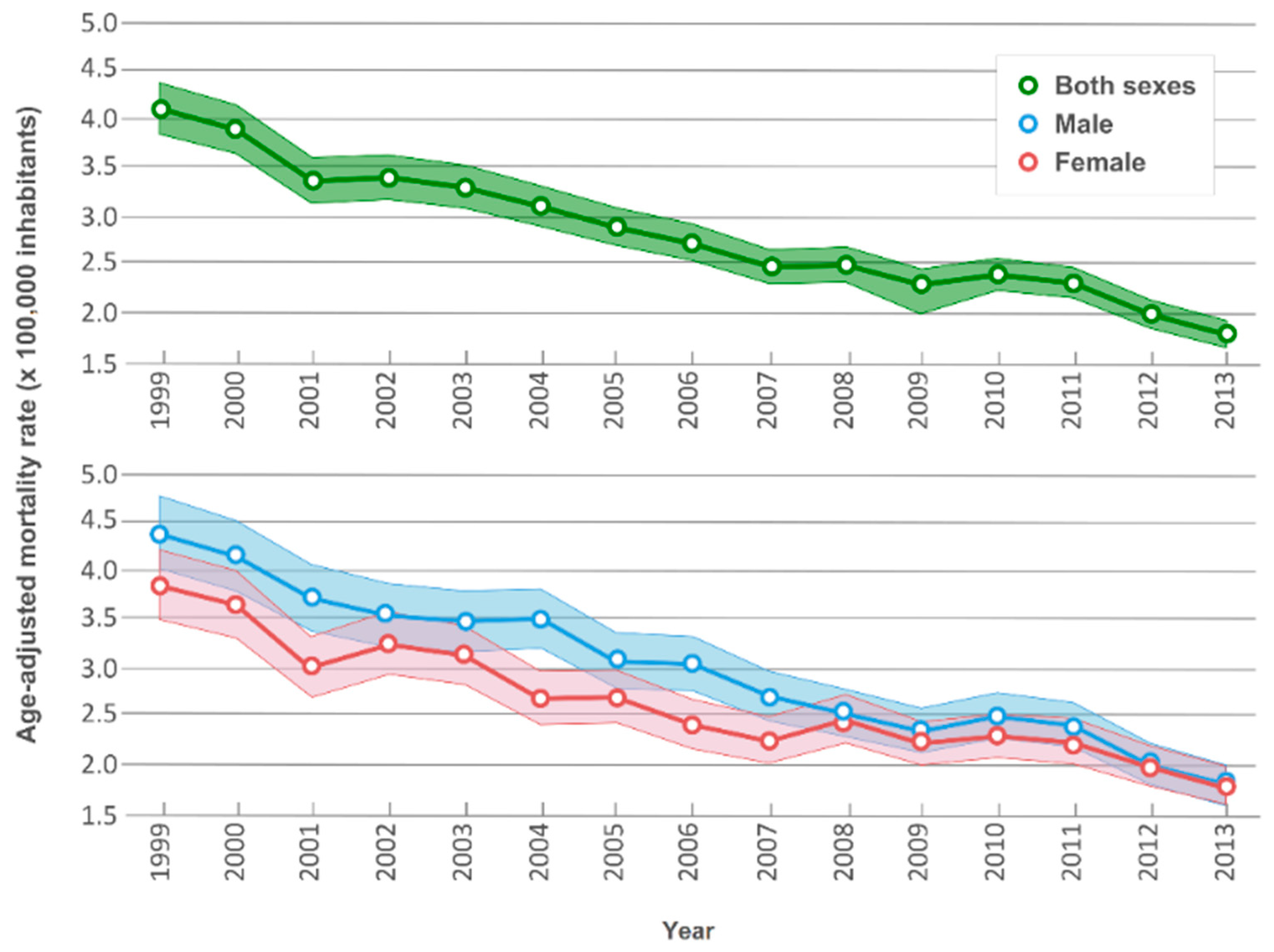
3.1. Time Trends
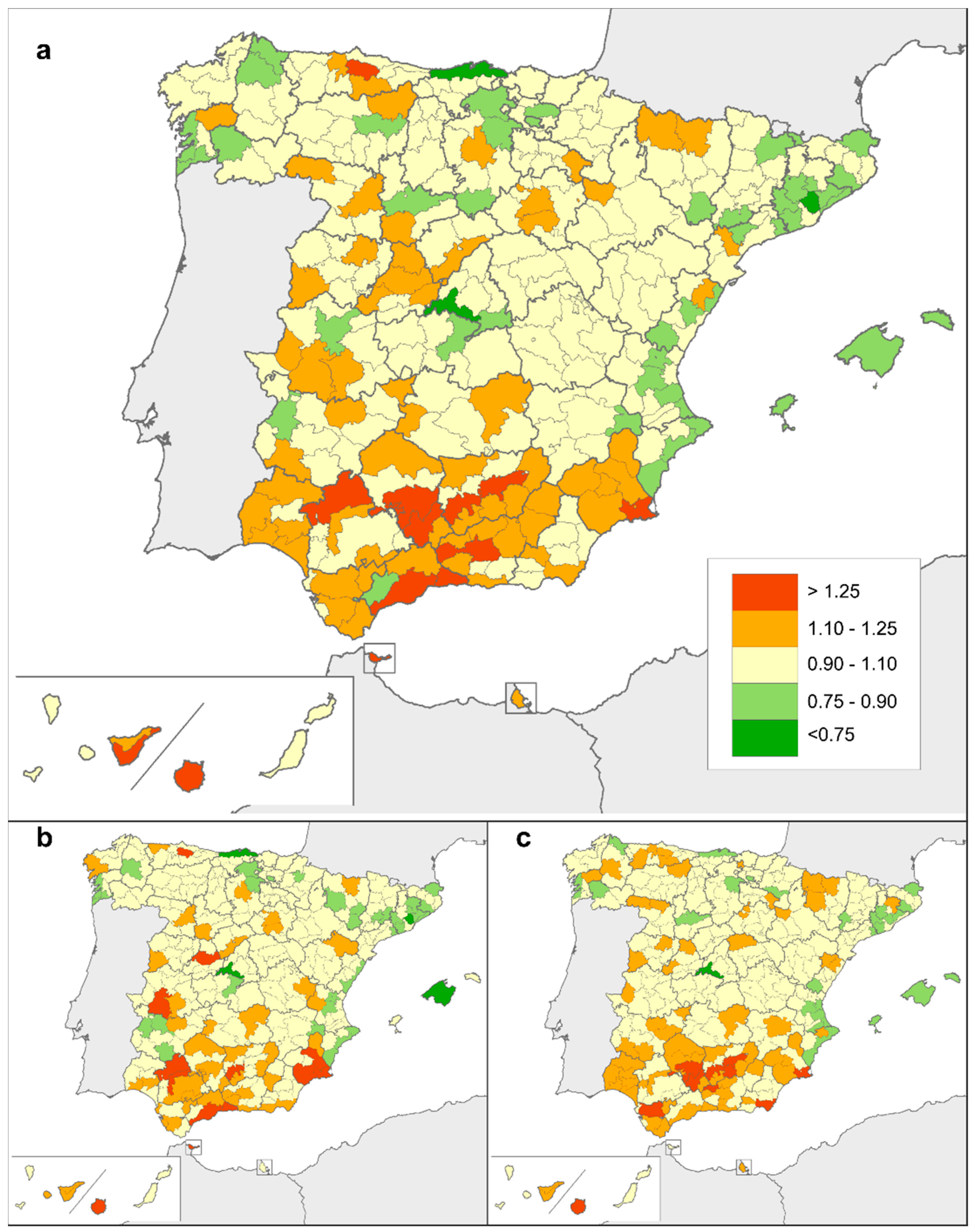
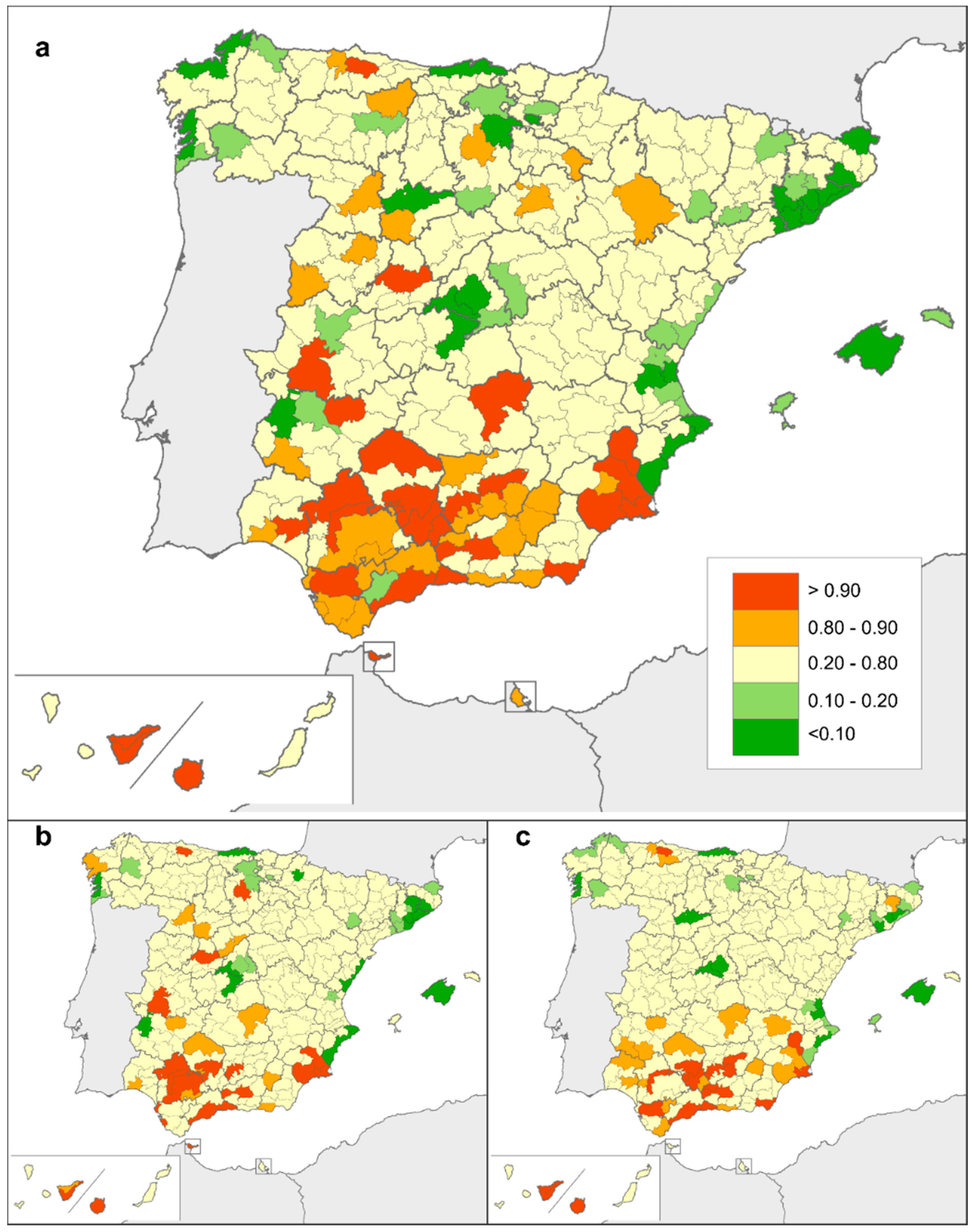
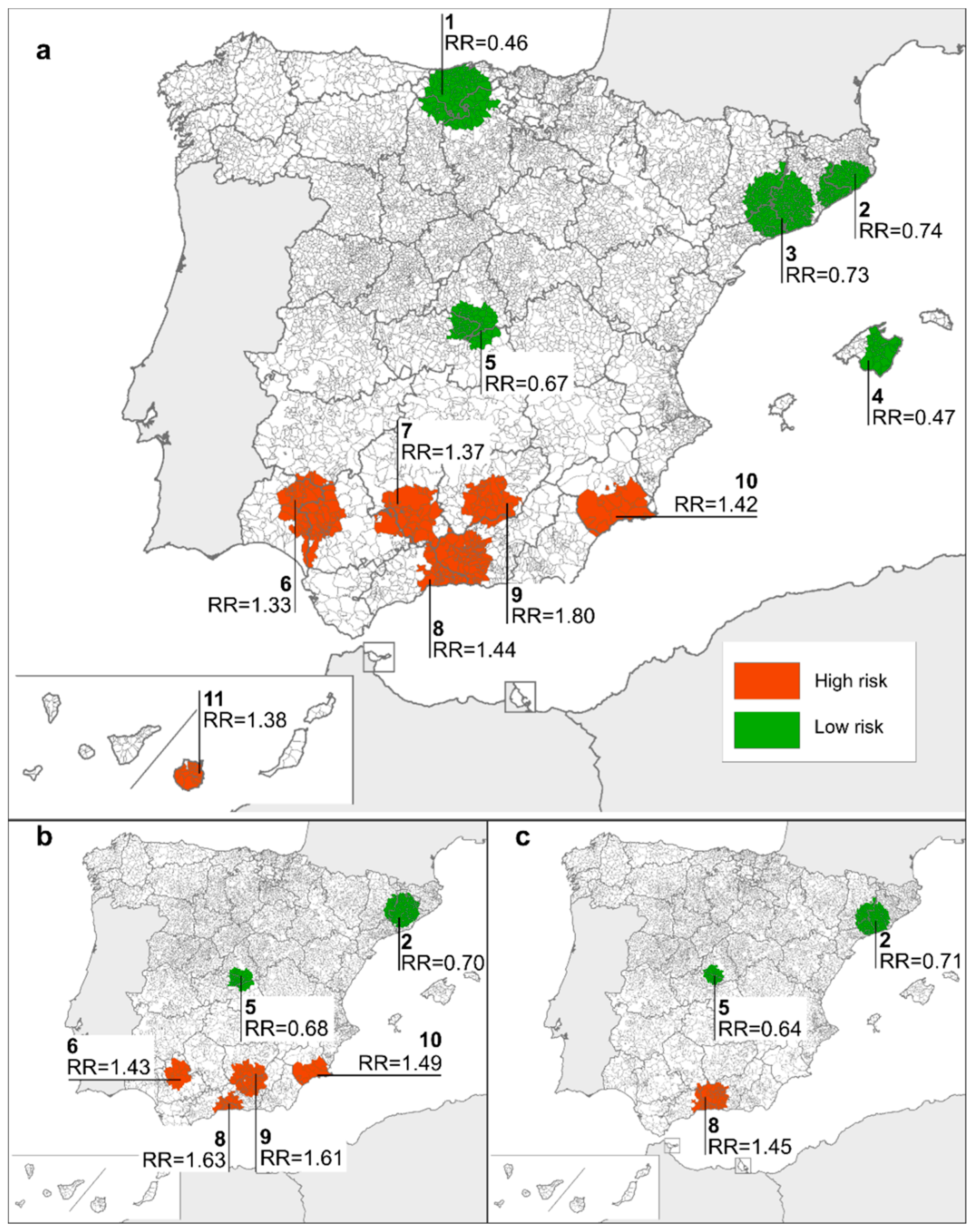
3.2. Geographical Distribution
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000–2015: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef]
- Oza, S.; Lawn, J.E.; Hogan, D.R.; Mathers, C.; Cousens, S.N. Neonatal cause-of-death estimates for the early and late neonatal periods for 194 countries: 2000–2013. Bull. World Health Organ. 2015, 93, 19–28. [Google Scholar] [CrossRef] [PubMed]
- European Surveillance of Congenital Anomalies, EUROCAT. Available online: http://www.eurocat-network.eu/ (accessed on 25 June 2018).
- International Clearinghouse for Birth Defects Surveillance and Research, ICBDSR. Available online: http://www.icbdsr.org/ (accessed on 25 June 2018).
- Kinsner-Ovaskainen, A.; Lanzoni, M.; Garne, E.; Loane, M.; Morris, J.; Neville, A.; Nicholl, C.; Rankin, J.; Rissmann, A.; Tucker, D.; et al. A Sustainable Solution for the Activities of the European Network for Surveillance of Congenital Anomalies: EUROCAT as Part of the EU Platform on Rare Diseases Registration. Eur. J. Med. Genet. 2018. [CrossRef] [PubMed]
- Coi, A.; Santoro, M.; Pierini, A.; Marrucci, S.; Pieroni, F.; Bianchi, F. Prevalence Estimates of Rare Congenital Anomalies by Integrating Two Population-Based Registries in Tuscany, Italy. Public Health Genom. 2017, 20, 229–234. [Google Scholar] [CrossRef] [PubMed]
- De la Paz, M.P.; Villaverde-Hueso, A.; Alonso, V.; János, S.; Zurriaga, O.; Pollán, M.; Abaitua-Borda, I. Rare diseases epidemiology research. Adv. Exp. Med. Biol. 2010, 686, 17–39. [Google Scholar] [CrossRef] [PubMed]
- Arias Merino, G.; Sánchez Díaz, G.; Villaverde-Hueso, A.; Posada de la Paz, M.; Alonso Ferreira, V. Mortality Statistics and their Contribution to Improving the Knowledge of Rare Diseases Epidemiology: The Example of Hereditary Ataxia in Europe. Adv. Exp. Med. Biol. 2017, 1031, 521–533. [Google Scholar] [CrossRef] [PubMed]
- Olsen, S.F.; Martuzzi, M.; Elliott, P. Cluster analysis and disease mapping—Why, when, and how? A step-by-step guide. BMJ 1996, 313, 863–866. [Google Scholar] [CrossRef] [PubMed]
- Bermejo-Sánchez, E.; Posada de la Paz, M. Congenital Anomalies: Cluster Detection and Investigation. Adv. Exp. Med. Biol. 2017, 1031, 535–557. [Google Scholar] [CrossRef] [PubMed]
- Yazdy, M.M.; Werler, M.M.; Feldkamp, M.L.; Shaw, G.M.; Mosley, B.S.; Vieira, V.M.; National Birth Defects Prevention Study. Spatial analysis of gastroschisis in the National Birth Defects Prevention Study. Birth Defects Res. A Clin. Mol. Teratol. 2015, 103, 544–553. [Google Scholar] [CrossRef] [PubMed]
- Castilla, E.E.; Mastroiacovo, P.; López-Camelo, J.S.; Saldarriaga, W.; Isaza, C.; Orioli, I.M. Sirenomelia and cyclopia cluster in Cali, Colombia. Am. J. Med. Genet. A 2008, 146A, 2626–2636. [Google Scholar] [CrossRef] [PubMed]
- Bronberg, R.; Gili, J.; Chaves, E.; Dipierri, J. Infant mortality due to congenital malformation in Argentina (1998–2009): Temporal and spatial analysis of neonatal and postneonatal components. J. Community Genet. 2013, 4, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Fazzo, L.; Belli, S.; Minichilli, F.; Mitis, F.; Santoro, M.; Martina, L.; Pizzuti, R.; Comba, P.; Martuzzi, M.; Bianchi, F.; the Working Group. Cluster analysis of mortality and malformations in the provinces of Naples and Caserta (Campania Region). Ann. Ist. Super. Sanita 2008, 44, 99–111. [Google Scholar] [PubMed]
- Armstrong, B.G.; Dolk, H.; Pattenden, S.; Vrijheid, M.; Loane, M.; Rankin, J.; Dunn, C.E.; Grundy, C.; Abramsky, L.; Boyd, P.A.; et al. Geographic variation and localised clustering of congenital anomalies in Great Britain. Emerg. Themes Epidemiol. 2007, 4, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyle, B.; Addor, M.C.; Arriola, L.; Barisic, I.; Bianchi, F.; Csáky-Szunyogh, M.; de Walle, H.E.K.; Dias, C.M.; Draper, E.; Gatt, M.; et al. Estimating Global Burden of Disease due to congenital anomaly: An analysis of European data. Arch. Dis. Child. Fetal. Neonatal 2018, 103, F22–F28. [Google Scholar] [CrossRef] [PubMed]
- The Spanish Rare Diseases Registries Research Network, SpainRDR. Available online: https://spainrdr.isciii.es/ (accessed on 25 June 2018).
- Arias López, M. La Comarca Como Entidad Natural, Histórica Y Administrativa; Dykinson, S.L.: Madrid, Spain, 2013; pp. 1–518. [Google Scholar]
- Sánchez-Díaz, G.; Arias-Merino, G.; Villaverde-Hueso, A.; Morales-Piga, A.; Abaitua-Borda, I.; Hens, M.; Bermejo-Sánchez, E.; Posada de la Paz, M.; Alonso-Ferreira, V. Monitoring Huntington’s Disease Mortality across a 30-Year Period: Geographic and Temporal Patterns. Neuroepidemiology 2016, 47, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Besag, J.E.; York, J.; Molliè, A. A Bayesian image restoration with two applications in spatial statistics. Ann. Inst. Stat. Math. 1991, 43, 1–59. [Google Scholar] [CrossRef]
- Kulldorf, M.; Mostashari, F.; Duczmal, L.; Katherine, Y.W.; Kleinman, K.; Platt, R. Multivariate scan statistics for disease surveillance. Stat. Med. 2007, 26, 1824–1833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization, WHO. Mortality. Available online: http://apps.who.int/healthinfo/statistics/mortality/whodpms/ (accessed on 25 June 2018).
- Gupta, N.; Leven, L.; Stewart, M.; Cheung, M.; Patel, N. Transport of infants with congenital heart disease: Benefits of antenatal diagnosis. Eur. J. Pediatr. 2014, 173, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.K.; Springett, A.L.; Greenlees, R.; Loane, M.; Addor, M.C.; Arriola, L.; Barisic, I.; Bergman, J.E.H.; Csaky-Szunyogh, M.; Dias, C.; et al. Trends in congenital anomalies in Europe from 1980 to 2012. PLoS ONE 2018, 13, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Lara, D.A.; Fixler, D.E.; Ethen, M.K.; Canfield, M.A.; Nembhard, W.N.; Morris, S.A. Prenatal diagnosis, hospital characteristics, and mortality in transposition of the great arteries. Birth Defects Res. A Clin. Mol. Teratol. 2016, 106, 739–748. [Google Scholar] [CrossRef] [PubMed]
- Arth, A.C.; Tinker, S.C.; Simeone, R.M.; Ailes, E.C.; Cragan, J.D.; Grosse, S.D. Inpatient Hospitalization Costs Associated with Birth Defects Among Persons of All Ages—United States, 2013. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 41–46. [Google Scholar] [CrossRef] [PubMed]
- GBD 2016. Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef]
- Modell, B.; Berry, R.J.; Boyle, C.A.; Christianson, A.; Darlison, M.; Dolk, H.; Howson, C.P.; Mastroiacovo, P.; Mossey, P.; Rankin, J. Global regional and national causes of child mortality. Lancet 2012, 380, 1556. [Google Scholar] [CrossRef]
- Johansson, L.; Westerling, R. Comparing hospital discharge records with death certificates: Can the differences be explained? J. Epidemiol. Community Health 2002, 56, 301–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rare CAs as Cause of Death | Number of Deaths | |||
|---|---|---|---|---|
| Total | Men | Women | ||
| Rare CAs of the Nervous System | ||||
| Nervous system | Q00, Q01, Q02, Q03, Q04, Q05, Q06, Q07 | 1251 | 645 | 606 |
| Neural Tube Defects | Q00, Q01, Q05 | 272 | 140 | 132 |
| Anencephalus and similar | Q00 | 97 | 49 | 48 |
| Encephalocele | Q01 | 15 | 10 | 5 |
| Myelomeningocele/Spina Bifida | Q05 | 160 | 81 | 79 |
| Hydrocephalus | Q03 | 199 | 119 | 80 |
| Severe microcephaly | Q02 | 54 | 24 | 30 |
| Arhinencephaly/holoprosencephaly | Q04.1, Q04.2 | 59 | 24 | 35 |
| Rare CAs of the Eye, Ear, Face and Neck | ||||
| Eye | Q10–Q15 | 1 | 0 | 1 |
| Anophthalmos/microphthalmos | Q11.0, Q11.1, Q11.2 | 1 | 0 | 1 |
| Anophthalmos | Q11.0, Q11.1 | 0 | 0 | 0 |
| Congenital cataract | Q12.0 | 0 | 0 | 0 |
| Congenital glaucoma | Q15.0 | 0 | 0 | 0 |
| Ear, face and neck | Q16, Q17, Q18 | 0 | 0 | 0 |
| Anotia | Q16.0 | 0 | 0 | 0 |
| Rare CAs of the Circulatory System | ||||
| Congenital Heart Defects (CHD) | Q20–Q26 | 4927 | 2780 | 2147 |
| Severe CHD | Q20.0, Q20.1, Q20.3, Q20.4, Q21.2, Q21.3, Q22.0, Q22.4, Q22.5, Q22.6, Q23.0, Q23.2, Q23.3, Q23.4, Q25.1, Q25.2, Q26.2 | 1475 | 841 | 634 |
| Common arterial truncus | Q20.0 | 44 | 20 | 24 |
| Double outlet right ventricle | Q20.1 | 19 | 12 | 7 |
| Transposition of great vessels | Q20.3 | 235 | 151 | 84 |
| Single ventricle | Q20.4 | 75 | 40 | 35 |
| AVSD | Q21.2 | 126 | 52 | 74 |
| Tetralogy of Fallot | Q21.3 | 360 | 210 | 150 |
| Triscuspid atresia and stenosis | Q22.4 | 34 | 15 | 19 |
| Ebstein’s anomaly | Q22.5 | 75 | 32 | 43 |
| Pulmonary valve stenosis | Q22.1 | 6 | 4 | 2 |
| Pulmonary valve atresia | Q22.0 | 5 | 2 | 3 |
| Aortic valve atresia/stenosis | Q23.0 | 57 | 37 | 20 |
| Mitral valve anomalies | Q23.2, Q23.3 | 27 | 15 | 12 |
| Hypoplastic left heart | Q23.4 | 256 | 155 | 101 |
| Hypoplastic right heart | Q22.6 | 5 | 3 | 2 |
| Coarctation of aorta | Q25.1 | 150 | 93 | 57 |
| Total anomalous pulmonary venous return | Q26.2 | 7 | 4 | 3 |
| PDA as only CHD in term infants (GA + 37 weeks) | Q25.0 | 290 | 155 | 135 |
| Rare CAs of the Respiratory System | ||||
| Respiratory | Q30.0, Q32–Q34 | 347 | 203 | 144 |
| Choanal atresia | Q30.0 | 8 | 5 | 3 |
| Cleft lip and Cleft Palate | ||||
| Oro-facial clefts | Q35–Q37 | 4 | 1 | 3 |
| Cleft lip with or without cleft palate | Q36, Q37 | 0 | 0 | 0 |
| Cleft palate | Q35 | 4 | 1 | 3 |
| Rare CAs of the Digestive System | ||||
| Digestive system | Q38–Q45 | 1092 | 593 | 499 |
| Oesophageal atresia with or without tracheaoesophageal fistula | Q39.0–Q39.1 | 107 | 55 | 52 |
| Duodenal atresia or stenosis | Q41.0 | 11 | 7 | 4 |
| Atresia or stenosis of other parts of small intestine | Q41.1–Q41.8 | 17 | 9 | 8 |
| Ano-rectal atresia and stenosis | Q42.0–Q42.3 | 6 | 4 | 2 |
| Hirschsprung’s disease | Q43.1 | 47 | 27 | 20 |
| Atresia of bile ducts | Q44.2 | 55 | 30 | 25 |
| Annular pancreas | Q45.1 | 0 | 0 | 0 |
| Rare CAs of the Urinary System | ||||
| Urinary | Q60–Q64, Q79.4 | 756 | 393 | 363 |
| Bilateral renal agenesis including Potter syndrome | Q60.1, Q60.6 | 84 | 53 | 31 |
| Renal dysplasia | Q61.4 | 28 | 20 | 8 |
| Bladder exstrophy and/or epispadia | Q64.0, Q64.1 | 2 | 2 | 0 |
| Posterior urethral valve and/or prune belly | Q64.2, Q64.3, Q79.4 | 7 | 6 | 1 |
| Rare CAs of Genital Organs | ||||
| Genital | Q50–Q52, Q54–Q56 | 1 | 1 | 0 |
| Hypospadias | Q54 | 1 | 1 | 0 |
| Indeterminate sex | Q56 | 0 | 0 | 0 |
| Rare CAs of the Musculoskeletal System | ||||
| Craniosynostosis | Q75.0 | 6 | 3 | 3 |
| Diaphragmatic hernia | Q79.0 | 339 | 191 | 148 |
| Limb | Q65–Q74 | 56 | 24 | 32 |
| Limb reduction defects | Q71–Q73 | 0 | 0 | 0 |
| Polydactyly | Q69 | 0 | 0 | 0 |
| Syndactyly | Q70 | 0 | 0 | 0 |
| Abdominal wall defects | Q79.2, Q79.3, Q79.5 | 66 | 42 | 24 |
| Gastroschisis | Q79.3 | 44 | 30 | 14 |
| Omphalocele | Q79.2 | 22 | 12 | 10 |
| Other Rare Congenital Malformations | ||||
| Other anomalies/syndromes | ||||
| Congenital skin disorders | Q80–Q82 | 93 | 62 | 31 |
| Fetal alcohol syndrome | Q86.0 | 2 | 2 | 0 |
| Situs inversus | Q89.3 | 31 | 16 | 15 |
| Conjoined twins | Q89.4 | 11 | 2 | 9 |
| Rare Chromosomal Abnormalities, not elsewhere classified | ||||
| Chromosomal | Q90–Q92, Q93, Q96–Q99 | 2312 | 1068 | 1244 |
| Patau syndrome/trisomy 13 | Q91.4–Q91.7 | 143 | 62 | 81 |
| Edwards syndrome / trisomy 18 | Q91.0–Q91.3 | 288 | 81 | 207 |
| Turner syndrome | Q96 | 23 | 1 | 22 |
| Klinefelter syndrome | Q98.0–Q98.4 | 3 | 3 | 0 |
| Year | Rare CAs of the Nervous System | Neural Tube Defects | ||||||||||
| Both Sexes | Men | Women | Both Sexes | Men | Women | |||||||
| n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | |
| 1999 | 93 | 0.37 (0.29–0.45) | 47 | 0.35 (0.25–0.47) | 46 | 0.39 (0.28–0.53) | 23 | 0.10 (0.06–0.15) | 11 | 0.08 (0.04–0.15) | 12 | 0.12 (0.06–0.20) |
| 2000 | 95 | 0.36 (0.29–0.45) | 51 | 0.37 (0.27–0.50) | 44 | 0.35 (0.25–0.48) | 25 | 0.10 (0.06–0.15) | 12 | 0.09 (0.05–0.16) | 13 | 0.10 (0.05–0.18) |
| 2001 | 87 | 0.34 (0.27–0.43) | 54 | 0.42 (0.32–0.56) | 33 | 0.26 (0.17–0.37) | 24 | 0.09 (0.06–0.14) | 15 | 0.11 (0.06–0.19) | 9 | 0.07 (0.03–0.14) |
| 2002 | 79 | 0.29 (0.23–0.37) | 34 | 0.25 (0.17–0.35) | 45 | 0.35 (0.25–0.47) | 15 | 0.07 (0.04–0.11) | 9 | 0.08 (0.04–0.15) | 6 | 0.06 (0.02–0.12) |
| 2003 | 93 | 0.34 (0.27–0.42) | 47 | 0.34 (0.25–0.46) | 46 | 0.34 (0.25–0.46) | 20 | 0.07 (0.04–0.11) | 14 | 0.10 (0.05–0.17) | 6 | 0.05 (0.02–0.10) |
| 2004 | 95 | 0.31 (0.32–0.39) | 56 | 0.38 (0.28–0.50) | 39 | 0.26 (0.18–0.36) | 18 | 0.06 (0.03–0.10) | 9 | 0.05 (0.02–0.11) | 9 | 0.06 (0.03–0.13) |
| 2005 | 82 | 0.26 (0.21–0.33) | 45 | 0.29 (0.21–0.40) | 37 | 0.24 (0.16–0.33) | 16 | 0.05 (0.03–0.09) | 10 | 0.07 (0.03–0.13) | 6 | 0.03 (0.01–0.08) |
| 2006 | 80 | 0.25 (0.21–0.33) | 46 | 0.28 (0.20–0.37) | 34 | 0.23 (0.16–0.32) | 21 | 0.06 (0.04–0.10) | 12 | 0.06 (0.03–0.12) | 9 | 0.06 (0.03–0.11) |
| 2007 | 80 | 0.25 (0.20–0.31) | 41 | 0.25 (0.18–0.34) | 39 | 0.25 (0.18–0.35) | 16 | 0.05 (0.03–0.08) | 6 | 0.04 (0.01–0.09) | 10 | 0.06 (0.03–0.11) |
| 2008 | 73 | 0.22 (0.18–0.28) | 35 | 0.21 (0.14–0.29) | 38 | 0.25 (0.17–0.34) | 16 | 0.05 (0.03–0.08) | 11 | 0.07 (0.03–0.12) | 5 | 0.03 (0.01–0.08) |
| 2009 | 74 | 0.21 (0.17–0.27) | 33 | 0.19 (0.13–0.26) | 41 | 0.24 (0.17–0.34) | 20 | 0.06 (0.03–0.09) | 8 | 0.05 (0.02–0.10) | 12 | 0.07 (0.03–0.12) |
| 2010 | 93 | 0.26 (0.21–0.32) | 42 | 0.24 (0.17–0.32) | 51 | 0.28 (0.21–0.38) | 12 | 0.03 (0.01–0.05) | 4 | 0.02 (0.01–0.06) | 8 | 0.04 (0.01–0.08) |
| 2011 | 82 | 0.22 (0.17–0.27) | 44 | 0.23 (0.16–0.31) | 38 | 0.20 (0.14–0.29) | 18 | 0.04 (0.02–0.07) | 6 | 0.03 (0.01–0.06) | 12 | 0.06 (0.03–0.10) |
| 2012 | 77 | 0.21 (0.16–0.26) | 37 | 0.21 (0.14–0.29) | 40 | 0.20 (0.14–0.28) | 14 | 0.03 (0.02–0.05) | 6 | 0.03 (0.01–0.06) | 8 | 0.04 (0.01–0.08) |
| 2013 | 68 | 0.20 (0.15–0.25) | 33 | 0.18 (0.12–0.26) | 35 | 0.22 (0.15–0.31) | 14 | 0.04 (0.02–0.06) | 7 | 0.04 (0.01–0.08) | 7 | 0.04 (0.01–0.08) |
| APC | −4.49 (p < 0.001) | −5.19 (p < 0.001) | −3.87 (p < 0.001) | −6.60 (p < 0.001) | −2.40 (p = 0.30) | −8.24 (p < 0.001) | ||||||
| Year | Hydrocephalus | Rare CAs of the Circulatory System | ||||||||||
| Both Sexes | Men | Women | Both Sexes | Men | Women | |||||||
| n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | |
| 1999 | 20 | 0.08 (0.05–0.13) | 14 | 0.11 (0.06–0.19) | 6 | 0.05 (0.02–0.11) | 486 | 1.90 (1.73–2.09) | 274 | 2.11 (1.86–2.38) | 212 | 1.69 (1.46–1.95) |
| 2000 | 22 | 0.09 (0.05–0.14) | 13 | 0.10 (0.05–0.18) | 9 | 0.07 (0.03–0.14) | 480 | 1.85 (1.68–2.03) | 268 | 2.06 (1.82–2.34) | 212 | 1.63 (1.40–1.88) |
| 2001 | 12 | 0.05 (0.02–0.08) | 6 | 0.04 (0.02–0.10) | 6 | 0.05 (0.02–0.11) | 387 | 1.51 (1.36–1.67) | 224 | 1.69 (1.46–1.93) | 163 | 1.33 (1.12–1.56) |
| 2002 | 22 | 0.08 (0.05–0.12) | 10 | 0.07 (0.03–0.13) | 12 | 0.09 (0.05–0.17) | 421 | 1.60 (1.44–1.76) | 241 | 1.79 (1.57–2.04) | 180 | 1.39 (1.19–1.62) |
| 2003 | 15 | 0.05 (0.03–0.09) | 7 | 0.05 (0.02–0.10) | 8 | 0.06 (0.02–0.12) | 391 | 1.38 (1.24–1.53) | 211 | 1.48 (1.28–1.70) | 180 | 1.28 (1.09–1.49) |
| 2004 | 16 | 0.05 (0.03–0.09) | 12 | 0.08 (0.04–0.14) | 4 | 0.03 (0.01–0.07) | 404 | 1.39 (1.25–1.53) | 254 | 1.71 (1.50–1.94) | 150 | 1.05 (0.88–1.24) |
| 2005 | 12 | 0.04 (0.02–0.07) | 10 | 0.06 (0.03–0.11) | 2 | 0.02 (0.00–0.06) | 341 | 1.16 (1.03–1.29) | 205 | 1.37 (1.19–1.58) | 136 | 0.93 (0.78–1.11) |
| 2006 | 9 | 0.03 (0.01–0.06) | 7 | 0.05 (0.02–0.10) | 2 | 0.01 (0.00–0.05) | 380 | 1.21 (1.09–1.34) | 220 | 1.38 (1.20–1.58) | 160 | 1.04 (0.88–1.22) |
| 2007 | 11 | 0.03 (0.02–0.06) | 7 | 0.04 (0.02–0.09) | 4 | 0.03 (0.01–0.08) | 318 | 0.99 (0.88–1.11) | 170 | 1.09 (0.93–1.26) | 140 | 0.9 (0.75–1.07) |
| 2008 | 14 | 0.04 (0.02–0.07) | 7 | 0.04 (0.01–0.08) | 7 | 0.05 (0.02–0.10) | 350 | 1.05 (0.94–1.17) | 190 | 1.14 (0.98–1.32) | 160 | 0.95 (0.81–1.12) |
| 2009 | 9 | 0.02 (0.01–0.05) | 4 | 0.02 (0.01–0.06) | 5 | 0.03 (0.01–0.07) | 341 | 0.97 (0.86–1.08) | 190 | 1.06 (0.91–1.23) | 151 | 0.87 (0.73–1.02) |
| 2010 | 13 | 0.04 (0.02–0.06) | 8 | 0.05 (0.02–0.09) | 5 | 0.02 (0.01–0.06) | 349 | 0.97 (0.87–1.08) | 190 | 1.06 (0.91–1.23) | 159 | 0.88 (0.74–1.03) |
| 2011 | 10 | 0.03 (0.01–0.05) | 9 | 0.04 (0.02–0.09) | 1 | 0.01 (0.00–0.04) | 321 | 0.9 (0.80–1.01) | 184 | 1.01 (0.87–1.17) | 137 | 0.8 (0.66–0.95) |
| 2012 | 6 | 0.02 (0.01–0.03) | 1 | 0.01 (0.00–0.03) | 5 | 0.02 (0.01–0.06) | 295 | 0.81 (0.71–0.91) | 153 | 0.84 (0.71–0.99) | 142 | 0.77 (0.64–0.92) |
| 2013 | 8 | 0.02 (0.01–0.05) | 4 | 0.02 (0.01–0.06) | 4 | 0.02 (0.01–0.06) | 246 | 0.67 (0.59–0.77) | 134 | 0.71 (0.59–0.85) | 112 | 0.64 (0.52–0.78) |
| APC | −9.65 (p < 0.001) | −9.11 (p < 0.001) | −9.08 (p < 0.001) | −6.44 (p < 0.001) | −6.70 (p < 0.001) | −6.08 (p < 0.001) | ||||||
| Year | Severe CHD | Transposition of Great Vessels | ||||||||||
| Both Sexes | Men | Women | Both Sexes | Men | Women | |||||||
| n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | |
| 1999 | 145 | 0.59 (0.50–0.70) | 89 | 0.72 (0.57–0.89) | 56 | 0.47 (0.35–0.62) | 28 | 0.12 (0.08–0.18) | 18 | 0.16 (0.09–0.25) | 10 | 0.09 (0.04–0.16) |
| 2000 | 148 | 0.59 (0.49–0.69) | 75 | 0.59 (0.46–0.74) | 73 | 0.58 (0.45–0.74) | 30 | 0.13 (0.08–0.18) | 18 | 0.15 (0.09–0.24) | 12 | 0.10 (0.05–0.18) |
| 2001 | 100 | 0.39 (0.32–0.48) | 56 | 0.42 (0.31–0.55) | 44 | 0.36 (0.26–0.49) | 15 | 0.06 (0.03–0.10) | 9 | 0.07 (0.03–0.14) | 6 | 0.05 (0.02–0.11) |
| 2002 | 119 | 0.46 (0.38–0.56) | 66 | 0.49 (0.38–0.63) | 53 | 0.43 (0.32–0.57) | 22 | 0.09 (0.06–0.14) | 15 | 0.11 (0.06–0.19) | 7 | 0.06 (0.03–0.13) |
| 2003 | 102 | 0.38 (0.31–0.47) | 52 | 0.39 (0.29–0.51) | 50 | 0.38 (0.28–0.50) | 13 | 0.05 (0.03–0.09) | 7 | 0.06 (0.02–0.12) | 6 | 0.05 (0.02–0.11) |
| 2004 | 117 | 0.40 (0.33–0.49) | 79 | 0.53 (0.42–0.67) | 38 | 0.27 (0.19–0.37) | 22 | 0.08 (0.05–0.12) | 13 | 0.09 (0.05–0.16) | 9 | 0.07 (0.03–0.13) |
| 2005 | 101 | 0.33 (0.27–0.41) | 58 | 0.37 (0.28–0.49) | 43 | 0.29 (0.21–0.39) | 17 | 0.06 (0.03–0.09) | 13 | 0.08 (0.04–0.15) | 4 | 0.03 (0.01–0.07) |
| 2006 | 109 | 0.35 (0.29–0.43) | 60 | 0.38 (0.29–0.49) | 49 | 0.33 (0.24–0.44) | 15 | 0.05 (0.03–0.08) | 9 | 0.06 (0.02–0.11) | 6 | 0.04 (0.01–0.09) |
| 2007 | 101 | 0.31 (0.25–0.38) | 63 | 0.39 (0.29–0.50) | 38 | 0.23 (0.16–0.32) | 12 | 0.04 (0.02–0.07) | 9 | 0.06 (0.03–0.11) | 3 | 0.02 (0.00–0.06) |
| 2008 | 83 | 0.26 (0.20–0.32) | 48 | 0.29 (0.21–0.38) | 35 | 0.22 (0.15–0.31) | 14 | 0.05 (0.02–0.08) | 7 | 0.05 (0.02–0.09) | 7 | 0.05 (0.02–0.10) |
| 2009 | 80 | 0.23 (0.18–0.29) | 51 | 0.29 (0.21–0.38) | 29 | 0.17 (0.11–0.25) | 12 | 0.04 (0.02–0.07) | 9 | 0.06 (0.03–0.11) | 3 | 0.02 (0.00–0.06) |
| 2010 | 71 | 0.19 (0.15–0.25) | 38 | 0.21 (0.14–0.28) | 33 | 0.18 (0.13–0.26) | 9 | 0.03 (0.01–0.05) | 6 | 0.03 (0.01–0.07) | 3 | 0.02 (0.00–0.06) |
| 2011 | 65 | 0.18 (0.14–0.23) | 35 | 0.19 (0.13–0.26) | 30 | 0.17 (0.12–0.25) | 11 | 0.03 (0.01–0.05) | 9 | 0.05 (0.02–0.09) | 2 | 0.01 (0.00–0.04) |
| 2012 | 68 | 0.19 (0.14–0.24) | 36 | 0.20 (0.14–0.27) | 32 | 0.18 (0.12–0.25) | 9 | 0.03 (0.01–0.05) | 6 | 0.03 (0.01–0.08) | 3 | 0.02 (0.00–0.05) |
| 2013 | 66 | 0.18 (0.14–0.24) | 35 | 0.19 (0.13–0.26) | 31 | 0.18 (0.12–0.26) | 6 | 0.02 (0.01–0.04) | 3 | 0.02 (0.00–0.05) | 3 | 0.02 (0.00–0.05) |
| APC | −8.55 (p < 0.001) | −8.59 (p < 0.001) | −8.53 (p < 0.001) | −11.80 (p < 0.001) | −11.03 (p < 0.001) | −12.43 (p < 0.001) | ||||||
| Year | Hypoplastic Left Heart | Rare CAs of the Respiratory System | ||||||||||
| Both Sexes | Men | Women | Both Sexes | Men | Women | |||||||
| n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | |
| 1999 | 23 | 0.11 (0.07–0.16) | 13 | 0.12 (0.06–0.21) | 10 | 0.10 (0.05–0.18) | 25 | 0.11 (0.07–0.17) | 11 | 0.10 (0.05–0.18) | 14 | 0.13 (0.07–0.21) |
| 2000 | 19 | 0.09 (0.05–0.14) | 9 | 0.08 (0.04–0.16) | 10 | 0.10 (0.05–0.18) | 23 | 0.10 (0.06–0.15) | 14 | 0.12 (0.07–0.21) | 9 | 0.07 (0.03–0.14) |
| 2001 | 22 | 0.10 (0.06–0.15) | 11 | 0.10 (0.05–0.18) | 11 | 0.11 (0.05–0.19) | 24 | 0.11 (0.07–0.16) | 16 | 0.14 (0.08–0.22) | 8 | 0.08 (0.03–0.15) |
| 2002 | 25 | 0.11 (0.07–0.16) | 14 | 0.12 (0.07–0.20) | 11 | 0.10 (0.05–0.18) | 22 | 0.09 (0.05–0.14) | 14 | 0.11 (0.06–0.19) | 8 | 0.07 (0.03–0.14) |
| 2003 | 21 | 0.09 (0.05–0.14) | 13 | 0.11 (0.06–0.18) | 8 | 0.07 (0.03–0.14) | 35 | 0.14 (0.10–0.19) | 24 | 0.18 (0.12–0.28) | 11 | 0.09 (0.04–0.16) |
| 2004 | 21 | 0.08 (0.05–0.13) | 15 | 0.12 (0.07–0.19) | 6 | 0.05 (0.02–0.11) | 31 | 0.12 (0.08–0.17) | 17 | 0.12 (0.07–0.20) | 14 | 0.12 (0.06–0.19) |
| 2005 | 17 | 0.06 (0.04–0.10) | 9 | 0.07 (0.03–0.13) | 8 | 0.06 (0.03–0.12) | 25 | 0.09 (0.06–0.14) | 15 | 0.11 (0.06–0.18) | 10 | 0.08 (0.04–0.14) |
| 2006 | 21 | 0.08 (0.05–0.12) | 15 | 0.10 (0.06–0.17) | 6 | 0.05 (0.02–0.10) | 20 | 0.07 (0.04–0.11) | 12 | 0.08 (0.04–0.14) | 8 | 0.06 (0.02–0.11) |
| 2007 | 17 | 0.06 (0.04–0.10) | 13 | 0.09 (0.05–0.15) | 4 | 0.03 (0.01–0.08) | 28 | 0.10 (0.06–0.14) | 17 | 0.11 (0.06–0.18) | 11 | 0.08 (0.04–0.15) |
| 2008 | 16 | 0.05 (0.03–0.09) | 11 | 0.07 (0.04–0.13) | 5 | 0.04 (0.01–0.08) | 20 | 0.06 (0.04–0.10) | 10 | 0.07 (0.03–0.12) | 10 | 0.06 (0.03–0.11) |
| 2009 | 11 | 0.04 (0.02–0.06) | 7 | 0.04 (0.02–0.09) | 4 | 0.03 (0.01–0.07) | 22 | 0.06 (0.04–0.10) | 14 | 0.08 (0.04–0.14) | 8 | 0.04 (0.02–0.09) |
| 2010 | 12 | 0.04 (0.02–0.07) | 8 | 0.05 (0.02–0.10) | 4 | 0.03 (0.01–0.07) | 22 | 0.07 (0.04–0.10) | 15 | 0.09 (0.05–0.14) | 7 | 0.04 (0.02–0.09) |
| 2011 | 12 | 0.04 (0.02–0.07) | 6 | 0.04 (0.01–0.08) | 6 | 0.04 (0.01–0.09) | 32 | 0.10 (0.07–0.14) | 16 | 0.10 (0.05–0.16) | 16 | 0.1 (0.06–0.17) |
| 2012 | 10 | 0.03 (0.02–0.06) | 4 | 0.02 (0.01–0.06) | 6 | 0.04 (0.01–0.09) | 23 | 0.07 (0.05–0.11) | 14 | 0.08 (0.05–0.14) | 9 | 0.06 (0.03–0.11) |
| 2013 | 9 | 0.03 (0.01–0.06) | 7 | 0.04 (0.02–0.09) | 2 | 0.01 (0.00–0.05) | 16 | 0.05 (0.03–0.08) | 9 | 0.06 (0.03–0.11) | 7 | 0.05 (0.02–0.09) |
| APC | −9.00 (p < 0.001) | −7.47 (p < 0.001) | −10.53 (p < 0.001) | −4.07 (p < 0.001) | −4.46 (p < 0.001) | −3.72 (p = 0.87) | ||||||
| Year | Rare CAs of the Digestive System | Rare CAs of the Urinary System | ||||||||||
| Both Sexes | Men | Women | Both Sexes | Men | Women | |||||||
| n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | |
| 1999 | 42 | 0.15 (0.10–0.21) | 28 | 0.2 (0.13–0.29) | 14 | 0.11 (0.06–0.19) | 60 | 0.16 (0.12–0.22) | 39 | 0.24 (0.16–0.34) | 21 | 0.10 (0.05–0.17) |
| 2000 | 37 | 0.14 (0.09–0.19) | 21 | 0.15 (0.09–0.24) | 16 | 0.12 (0.07–0.21) | 70 | 0.17 (0.13–0.22) | 37 | 0.20 (0.13–0.29) | 33 | 0.14 (0.09–0.21) |
| 2001 | 37 | 0.12 (0.08–0.17) | 22 | 0.16 (0.10–0.25) | 15 | 0.08 (0.04–0.15) | 52 | 0.13 (0.09–0.18) | 24 | 0.14 (0.09–0.22) | 28 | 0.11 (0.07–0.18) |
| 2002 | 42 | 0.15 (0.11–0.21) | 18 | 0.15 (0.09–0.23) | 24 | 0.15 (0.09–0.24) | 50 | 0.12 (0.09–0.17) | 27 | 0.16 (0.10–0.24) | 23 | 0.09 (0.05–0.15) |
| 2003 | 48 | 0.16 (0.11–0.21) | 34 | 0.22 (0.15–0.31) | 14 | 0.1 (0.05–0.18) | 46 | 0.11 (0.08–0.16) | 27 | 0.15 (0.10–0.23) | 19 | 0.07 (0.04–0.13) |
| 2004 | 56 | 0.18 (0.13–0.23) | 29 | 0.17 (0.11–0.26) | 27 | 0.18 (0.12–0.27) | 35 | 0.08 (0.05–0.11) | 19 | 0.09 (0.05–0.15) | 16 | 0.07 (0.03–0.12) |
| 2005 | 64 | 0.19 (0.15–0.25) | 32 | 0.19 (0.13–0.28) | 32 | 0.19 (0.13–0.28) | 49 | 0.11 (0.08–0.15) | 23 | 0.11 (0.07–0.17) | 26 | 0.11 (0.07–0.17) |
| 2006 | 39 | 0.13 (0.09–0.18) | 17 | 0.12 (0.07–0.19) | 22 | 0.14 (0.08–0.22) | 51 | 0.12 (0.08–0.16) | 32 | 0.17 (0.11–0.24) | 19 | 0.07 (0.04–0.13) |
| 2007 | 61 | 0.16 (0.12–0.21) | 35 | 0.19 (0.13–0.27) | 26 | 0.13 (0.08–0.20) | 39 | 0.09 (0.06–0.13) | 22 | 0.12 (0.07–0.18) | 17 | 0.06 (0.03–0.11) |
| 2008 | 58 | 0.15 (0.11–0.20) | 33 | 0.17 (0.11–0.24) | 25 | 0.13 (0.08–0.20) | 44 | 0.11 (0.08–0.15) | 16 | 0.08 (0.05–0.14) | 28 | 0.13 (0.08–0.20) |
| 2009 | 46 | 0.12 (0.09–0.16) | 19 | 0.11 (0.06–0.17) | 27 | 0.13 (0.08–0.20) | 39 | 0.07 (0.05–0.10) | 16 | 0.06 (0.03–0.11) | 23 | 0.08 (0.05–0.13) |
| 2010 | 53 | 0.13 (0.10–0.18) | 24 | 0.12 (0.07–0.18) | 29 | 0.15 (0.10–0.23) | 61 | 0.13 (0.09–0.17) | 31 | 0.15 (0.10–0.22) | 30 | 0.10 (0.06–0.16) |
| 2011 | 68 | 0.15 (0.12–0.20) | 36 | 0.18 (0.12–0.25) | 32 | 0.12 (0.08–0.19) | 44 | 0.08 (0.06–0.12) | 22 | 0.09 (0.05–0.14) | 22 | 0.08 (0.04–0.13) |
| 2012 | 56 | 0.12 (0.09–0.16) | 29 | 0.13 (0.08–0.19) | 27 | 0.12 (0.07–0.18) | 50 | 0.07 (0.05–0.10) | 25 | 0.09 (0.05–0.14) | 25 | 0.06 (0.04–0.10) |
| 2013 | 46 | 0.09 (0.06–0.13) | 25 | 0.1 (0.06–0.15) | 21 | 0.09 (0.05–0.15) | 63 | 0.11 (0.08–0.14) | 31 | 0.13 (0.08–0.19) | 32 | 0.09 (0.05–0.14) |
| APC | −1.49 (p = 0.20) | −2.61 (p = 0.10) | −0.16 (p = 0.90) | −3.96 (p < 0.001) | −5.10 (p < 0.001) | −2.08 (p = 0.20) | ||||||
| Year | Rare CAs of the Musculoskeletal System | Diaphragmatic Hernia | ||||||||||
| Both Sexes | Men | Women | Both Sexes | Men | Women | |||||||
| n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | |
| 1999 | 61 | 0.26 (0.20–0.34) | 34 | 0.29 (0.20–0.41) | 27 | 0.23 (0.15–0.34) | 32 | 0.15 (0.10–0.21) | 19 | 0.18 (0.11–0.27) | 13 | 0.13 (0.07–0.22) |
| 2000 | 59 | 0.25 (0.19–0.32) | 27 | 0.23 (0.15–0.34) | 32 | 0.26 (0.18–0.38) | 26 | 0.12 (0.08–0.18) | 16 | 0.15 (0.08–0.24) | 10 | 0.10 (0.05–0.18) |
| 2001 | 49 | 0.21 (0.15–0.28) | 31 | 0.26 (0.17–0.37) | 18 | 0.15 (0.09–0.25) | 29 | 0.13 (0.09–0.19) | 19 | 0.17 (0.10–0.27) | 10 | 0.10 (0.05–0.18) |
| 2002 | 51 | 0.21 (0.15–0.27) | 25 | 0.20 (0.13–0.30) | 26 | 0.21 (0.14–0.32) | 22 | 0.10 (0.06–0.15) | 14 | 0.12 (0.07–0.20) | 8 | 0.07 (0.03–0.14) |
| 2003 | 67 | 0.23 (0.18–0.30) | 35 | 0.24 (0.17–0.34) | 32 | 0.22 (0.15–0.32) | 30 | 0.13 (0.09–0.18) | 17 | 0.14 (0.08–0.22) | 13 | 0.11 (0.06–0.19) |
| 2004 | 40 | 0.13 (0.09–0.19) | 22 | 0.16 (0.10–0.25) | 18 | 0.11 (0.06–0.18) | 13 | 0.05 (0.03–0.09) | 9 | 0.07 (0.03–0.13) | 4 | 0.03 (0.01–0.09) |
| 2005 | 46 | 0.15 (0.11–0.21) | 19 | 0.12 (0.07–0.19) | 27 | 0.19 (0.12–0.28) | 23 | 0.09 (0.05–0.13) | 12 | 0.08 (0.04–0.15) | 11 | 0.09 (0.04–0.16) |
| 2006 | 50 | 0.17 (0.12–0.22) | 35 | 0.23 (0.16–0.33) | 15 | 0.10 (0.06–0.17) | 25 | 0.09 (0.06–0.14) | 17 | 0.12 (0.07–0.19) | 8 | 0.06 (0.03–0.12) |
| 2007 | 43 | 0.14 (0.10–0.19) | 25 | 0.16 (0.10–0.24) | 18 | 0.12 (0.07–0.20) | 18 | 0.06 (0.04–0.10) | 9 | 0.06 (0.03–0.12) | 9 | 0.07 (0.03–0.13) |
| 2008 | 56 | 0.18 (0.13–0.23) | 28 | 0.17 (0.11–0.25) | 28 | 0.18 (0.12–0.27) | 25 | 0.09 (0.06–0.13) | 11 | 0.07 (0.04–0.13) | 14 | 0.10 (0.05–0.17) |
| 2009 | 40 | 0.12 (0.08–0.16) | 21 | 0.12 (0.07–0.19) | 19 | 0.11 (0.06–0.17) | 16 | 0.05 (0.03–0.08) | 8 | 0.05 (0.02–0.10) | 8 | 0.05 (0.02–0.10) |
| 2010 | 47 | 0.14 (0.10–0.18) | 28 | 0.17 (0.11–0.24) | 19 | 0.10 (0.06–0.17) | 26 | 0.08 (0.06–0.12) | 17 | 0.11 (0.06–0.17) | 9 | 0.06 (0.03–0.11) |
| 2011 | 62 | 0.18 (0.14–0.23) | 28 | 0.16 (0.11–0.23) | 34 | 0.20 (0.14–0.28) | 25 | 0.08 (0.05–0.12) | 12 | 0.07 (0.04–0.13) | 13 | 0.09 (0.05–0.15) |
| 2012 | 28 | 0.08 (0.06–0.12) | 10 | 0.06 (0.03–0.11) | 18 | 0.11 (0.06–0.18) | 11 | 0.04 (0.02–0.06) | 3 | 0.02 (0.00–0.05) | 8 | 0.05 (0.02–0.11) |
| 2013 | 29 | 0.08 (0.06–0.12) | 11 | 0.07 (0.03–0.12) | 18 | 0.10 (0.06–0.17) | 18 | 0.06 (0.04–0.09) | 8 | 0.05 (0.02–0.10) | 10 | 0.07 (0.03–0.13) |
| APC | −5.75 (p < 0.001) | −6.48 (p < 0.001) | −4.76 (p < 0.001) | −6.45 (p < 0.001) | −8.09 (p < 0.001) | −3.85 (p < 0.001) | ||||||
| Year | Other Rare Congenital Malformations | Rare Chromosomal Abnormalities, Not Elsewhere Classified | ||||||||||
| Both Sexes | Men | Women | Both Sexes | Men | Women | |||||||
| n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | n | AR (CI) | |
| 1999 | 158 | 0.63 (0.53–0.74) | 87 | 0.68 (0.54–0.85) | 71 | 0.58 (0.45–0.74) | 157 | 0.55 (0.46–0.55) | 64 | 0.55 (0.46–0.65) | 93 | 0.67 (0.53–0.83) |
| 2000 | 168 | 0.64 (0.55–0.75) | 87 | 0.67 (0.53–0.83) | 81 | 0.62 (0.48–0.78) | 119 | 0.42 (0.35–0.51) | 55 | 0.42 (0.35–0.51) | 64 | 0.47 (0.36–0.61) |
| 2001 | 154 | 0.61 (0.51–0.71) | 89 | 0.68 (0.54–0.85) | 65 | 0.53 (0.40–0.68) | 116 | 0.38 (0.31–0.46) | 47 | 0.38 (0.31–0.46) | 69 | 0.47 (0.36–0.61) |
| 2002 | 158 | 0.57 (0.48–0.68) | 84 | 0.62 (0.49–0.78) | 74 | 0.52 (0.40–0.66) | 123 | 0.4 (0.33–0.49) | 51 | 0.4 (0.33–0.49) | 72 | 0.48 (0.37–0.62) |
| 2003 | 136 | 0.47 (0.39–0.56) | 84 | 0.57 (0.45–0.71) | 52 | 0.36 (0.26–0.48) | 163 | 0.51 (0.43–0.60) | 63 | 0.51 (0.43–0.60) | 100 | 0.67 (0.54–0.82) |
| 2004 | 123 | 0.41 (0.34–0.50) | 67 | 0.44 (0.34–0.57) | 56 | 0.38 (0.28–0.50) | 171 | 0.5 (0.43–0.59) | 80 | 0.5 (0.43–0.59) | 91 | 0.55 (0.44–0.68) |
| 2005 | 143 | 0.44 (0.37–0.53) | 77 | 0.46 (0.36–0.58) | 66 | 0.43 (0.33–0.55) | 176 | 0.5 (0.43–0.59) | 78 | 0.5 (0.43–0.59) | 98 | 0.57 (0.54–0.70) |
| 2006 | 130 | 0.42 (0.34–0.50) | 73 | 0.46 (0.36–0.58) | 57 | 0.37 (0.28–0.49) | 148 | 0.39 (0.33–0.46) | 68 | 0.39 (0.33–0.46) | 80 | 0.45 (0.35–0.56) |
| 2007 | 122 | 0.36 (0.30–0.43) | 70 | 0.41 (0.32–0.53) | 52 | 0.3 (0.22–0.40) | 161 | 0.41 (0.35–0.48) | 85 | 0.41 (0.35–0.48) | 76 | 0.41 (0.32–0.52) |
| 2008 | 136 | 0.38 (0.32–0.46) | 70 | 0.39 (0.31–0.50) | 66 | 0.37 (0.28–0.48) | 146 | 0.36 (0.30–0.43) | 69 | 0.33 (0.26–0.42) | 77 | 0.39 (0.31–0.50) |
| 2009 | 126 | 0.35 (0.29–0.42) | 65 | 0.34 (0.26–0.44) | 61 | 0.35 (0.27–0.46) | 175 | 0.42 (0.36–0.50) | 93 | 0.44 (0.36–0.55) | 82 | 0.41 (0.32–0.51) |
| 2010 | 121 | 0.31 (0.26–0.38) | 70 | 0.35 (0.27–0.45) | 51 | 0.28 (0.21–0.37) | 172 | 0.42 (0.36–0.49) | 79 | 0.37 (0.29–0.47) | 93 | 0.46 (0.37–0.57) |
| 2011 | 117 | 0.32 (0.26–0.38) | 59 | 0.32 (0.24–0.41) | 58 | 0.32 (0.24–0.42) | 164 | 0.39 (0.34–0.46) | 78 | 0.36 (0.29–0.46) | 86 | 0.43 (0.34–0.54) |
| 2012 | 99 | 0.25 (0.21–0.31) | 51 | 0.26 (0.19–0.35) | 48 | 0.25 (0.18–0.34) | 159 | 0.38 (0.32–0.44) | 77 | 0.36 (0.28–0.45) | 82 | 0.4 (0.32–0.51) |
| 2013 | 87 | 0.23 (0.18–0.29) | 42 | 0.22 (0.16–0.30) | 45 | 0.24 (0.18–0.29) | 163 | 0.37 (0.31–0.43) | 81 | 0.36 (0.28–0.45) | 82 | 0.38 (0.30–0.47) |
| APC | −6.66 (p < 0.001) | −7.19 (p < 0.001) | −6.00 (p < 0.001) | −1.77 (p < 0.001) | −0.16 (p = 0.90) | −3.05 (p < 0.001) | ||||||
| Year | Edwards Syndrome/Trisomy 18 | |||||||||||
| Both Sexes | Men | Women | ||||||||||
| n | AR (CI) | n | AR (CI) | n | AR (CI) | |||||||
| 1999 | 26 | 0.12 (0.08–0.18) | 4 | 0.04 (0.01–0.09) | 22 | 0.21 (0.13–0.32) | ||||||
| 2000 | 20 | 0.09 (0.06–0.14) | 7 | 0.06 (0.03–0.13) | 13 | 0.12 (0.07–0.21) | ||||||
| 2001 | 21 | 0.10 (0.06–0.15) | 4 | 0.04 (0.01–0.09) | 17 | 0.16 (0.09–0.26) | ||||||
| 2002 | 14 | 0.06 (0.03–0.10) | 5 | 0.04 (0.01–0.10) | 9 | 0.08 (0.04–0.15) | ||||||
| 2003 | 26 | 0.11 (0.07–0.16) | 3 | 0.02 (0.01–0.07) | 23 | 0.20 (0.13–0.30) | ||||||
| 2004 | 24 | 0.10 (0.06–0.14) | 7 | 0.05 (0.02–0.11) | 17 | 0.14 (0.08–0.23) | ||||||
| 2005 | 26 | 0.10 (0.06–0.15) | 9 | 0.07 (0.03–0.13) | 17 | 0.13 (0.08–0.21) | ||||||
| 2006 | 17 | 0.06 (0.04–0.10) | 3 | 0.02 (0.00–0.06) | 14 | 0.11 (0.06–0.18) | ||||||
| 2007 | 19 | 0.07 (0.04–0.10) | 4 | 0.03 (0.01–0.07) | 15 | 0.11 (0.06–0.18) | ||||||
| 2008 | 21 | 0.07 (0.04–0.11) | 9 | 0.06 (0.03–0.11) | 12 | 0.08 (0.04–0.15) | ||||||
| 2009 | 17 | 0.05 (0.03–0.09) | 6 | 0.04 (0.01–0.08) | 11 | 0.07 (0.04–0.13) | ||||||
| 2010 | 17 | 0.05 (0.03–0.09) | 3 | 0.02 (0.00–0.06) | 14 | 0.09 (0.05–0.16) | ||||||
| 2011 | 20 | 0.06 (0.04–0.10) | 8 | 0.05 (0.02–0.10) | 12 | 0.08 (0.04–0.14) | ||||||
| 2012 | 9 | 0.03 (0.01–0.06) | 4 | 0.03 (0.01–0.06) | 5 | 0.03 (0.01–0.08) | ||||||
| 2013 | 11 | 0.04 (0.02–0.06) | 5 | 0.03 (0.01–0.07) | 6 | 0.04 (0.01–0.09) | ||||||
| APC | −6.60 (p < 0.001) | −2.44 (p = 0.30) | −8.24 (p < 0.001) | |||||||||
| Standardised Mortality Ratio for Rare Congenital Anomalies, 1999–2013 (95% CI) | |||||
|---|---|---|---|---|---|
| District | Province | Location | Both Sexes | Men | Women |
| Significantly Lower than the Expected for the Country as Reference | |||||
| Marquesado | Alicante | E | 0.69 (0.48–0.97) | – | – |
| Central | Alicante | E | 0.76 (0.64–0.90) | 0.78 (0.62–0.98) | 0.74 (0.57–0.94) |
| Meridional | Alicante | E | 0.84 (0.71–0.98) | 0.80 (0.63–0.99) | – |
| Badajoz | Badajoz | W | 0.68 (0.47–0.94) | 0.58 (0.33–0.95) | – |
| Ibiza | Baleares | E * | – | – | 0.42 (0.17–0.86) |
| Mallorca | Baleares | E * | 0.71 (0.61–0.83) | 0.66 (0.53–0.82) | 0.77 (0.62–0.95) |
| Osona | Barcelona | NE | – | 0.57 (0.32–0.94) | – |
| Penedès | Barcelona | NE | 0.76 (0.58–0.98) | – | 0.62 (0.39–0.94) |
| Vallès Oriental | Barcelona | NE | 0.76 (0.61–0.94) | – | 0.69 (0.48–0.95) |
| Vallès Occidental | Barcelona | NE | 0.71 (0.62–0.82) | 0.68 (0.56–0.83) | 0.75 (0.61–0.92) |
| Litoral del Norte | Castellón | E | – | 0.42 (0.13–0.97) | – |
| Cerdanya | Girona | NE | 0.00 (0.00–0.87) | – | – |
| La Selva | Girona | NE | 0.63 (0.43–0.90) | 0.58 (0.32–0.96) | – |
| Bajo Cinca | Huesca | N | – | 0.00 (0.00–0.96) | – |
| Costa | Lugo | NW | – | – | 0.22 (0.02–0.79) |
| Sur Occidental | Madrid | C | 0.61 (0.52–0.72) | 0.62 (0.49–0.77) | 0.61 (0.47–0.78) |
| Litoral | Pontevedra | NW | 0.76 (0.65–0.89) | 0.76 (0.60–0.94) | 0.78 (0.61–0.97) |
| Costera | Cantabria | N | 0.62 (0.50–0.76) | 0.61 (0.45–0.81) | 0.63 (0.46–0.85) |
| Sagra–Toledo | Toledo | C | 0.71 (0.53–0.92) | 0.60 (0.39–0.88) | – |
| Riberas del Júcar | Valencia | E | – | – | 0.67 (0.44–0.99) |
| Significantly Higher than the Expected for the Country as Reference | |||||
| Campo de Níjar y Bajo Andarax | Almería | SE | 1.25 (1.02–1.52) | – | 1.40 (1.04–1.83) |
| Ávila | Avila | C | – | 1.85 (1.05–3.00) | – |
| Don Benito | Badajoz | W | 1.43 (1.02–1.94) | – | – |
| Osona | Barcelona | NE | – | – | 1.48 (1.02–2.07) |
| Arlanzón | Burgos | N | – | 1.40 (1.01–1.88) | – |
| Caceres | Caceres | W | 1.42 (1.02–1.86) | 1.82 (1.28–2.52) | 1.44 (1.14–1.80) |
| Campiña de Cádiz | Cadiz | SW | 1.20 (1.01–1.42) | – | – |
| Los Pedroches | Cordoba | S | 1.47 (1.01–2.07) | – | – |
| Campiña Baja | Cordoba | S | 1.29 (1.11–1.50) | – | 1.35 (1.07–1.67) |
| Las Colonias | Cordoba | S | 1.95 (1.05–3.00) | 2.13 (1.02–3.92) | – |
| Campiña Alta | Cordoba | S | 1.33 (1.04–1.67) | – | 1.73 (1.26–2.31) |
| Serranía Baja | Cuenca | C | – | 3.63 (1.17–8.47) | – |
| La Vega | Granada | S | 1.32 (1.15–1.51) | 1.29 (1.06–1.56) | 1.36 (1.11–1.65) |
| Guadix | Granada | S | 1.77 (1.11–2.67) | – | – |
| Montefrío | Granada | S | – | – | 3.56 (1.77–6.36) |
| Sierra | Huelva | SW | – | – | 2.16 (1.08–3.87) |
| La Loma | Jaén | S | 1.44 (1.03–1.96) | – | 1.85 (1.19–2.16) |
| Campiña del Sur | Jaén | S | 1.66 (1.36–2.02) | 1.88 (1.44–2.42) | 1.41 (1.00–1.92) |
| Mágina | Jaén | S | – | – | 2.21 (1.06–4.06) |
| Montaña de Riaño | León | N | 2.37 (1.08–4.49) | – | – |
| Guadalhorce | Malaga | S | 1.31 (1.19–1.43) | 1.34 (1.18–1.52) | 1.27 (1.11–1.45) |
| Vélez–Málaga | Malaga | S | 1.40 (1.10–1.75) | 1.51 (1.10–2.02) | – |
| Río Segura | Murcia | SE | 1.22 (1.07–1.37) | 1.31 (1.11–1.53) | – |
| Suroeste y Valle del Guadalentín | Murcia | SE | 1.31 (1.05–1.60) | 1.41 (1.06–1.84) | – |
| Campo de Cartagena | Murcia | SE | 1.59 (1.36–1.84) | 1.68 (1.37–2.04) | 1.48 (1.16–1.85) |
| Grado | Asturias | N | – | – | 2.33 (1.16–4.17) |
| Oviedo | Asturias | N | 1.40 (1.17–1.66) | 1.55 (1.22–1.94) | – |
| Gran Canaria | Las Palmas | SW * | 1.34 (1.20–1.49) | 1.33 (1.14–1.54) | 1.36 (1.15–1.59) |
| Sur de Tenerife | Tenerife | SW * | 1.30 (1.11–1.51) | 1.32 (1.06–1.62) | 1.28 (1.01–1.60) |
| Sierra Norte | Seville | SW | 1.77 (1.22–2.49) | 2.40 (1.54–3.57) | – |
| La Vega | Seville | SW | 1.27 (1.15–1.39) | 1.29 (1.14–1.47) | 1.24 (1.07–1.42) |
| Ceuta | Ceuta | S | 1.61 (1.18–2.14) | 1.97 (1.34–2.80) | – |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alonso-Ferreira, V.; Sánchez-Díaz, G.; Villaverde-Hueso, A.; Posada de la Paz, M.; Bermejo-Sánchez, E. A Nationwide Registry-Based Study on Mortality Due to Rare Congenital Anomalies. Int. J. Environ. Res. Public Health 2018, 15, 1715. https://doi.org/10.3390/ijerph15081715
Alonso-Ferreira V, Sánchez-Díaz G, Villaverde-Hueso A, Posada de la Paz M, Bermejo-Sánchez E. A Nationwide Registry-Based Study on Mortality Due to Rare Congenital Anomalies. International Journal of Environmental Research and Public Health. 2018; 15(8):1715. https://doi.org/10.3390/ijerph15081715
Chicago/Turabian StyleAlonso-Ferreira, Verónica, Germán Sánchez-Díaz, Ana Villaverde-Hueso, Manuel Posada de la Paz, and Eva Bermejo-Sánchez. 2018. "A Nationwide Registry-Based Study on Mortality Due to Rare Congenital Anomalies" International Journal of Environmental Research and Public Health 15, no. 8: 1715. https://doi.org/10.3390/ijerph15081715