Weather and Health Symptoms


Abstract
1. Introduction
2. Materials and Methods
2.1. Data
2.1.1. Japanese Health Diary Study
2.1.2. Weather Data
2.2. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A


References
- Timmermans, E.J.; van der Pas, S.; Schaap, L.A.; Sánchez-Martínez, M.; Zambon, S.; Peter, R.; Pedersen, N.L.; Dennison, E.M.; Denkinger, M.; Castell, M.V.; et al. Self-perceived weather sensitivity and joint pain in older people with osteoarthritis in six European countries: Results from the European Project on OSteoArthritis (EPOSA). BMC Musculoskelet. Disord. 2014, 15, 66. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.; Scott, D.; Taneja, A.; Gow, P.; Gosai, A. Weather changes and pain in rheumatology patients. Int. J. Rheum. Dis. 2004, 7, 204–206. [Google Scholar] [CrossRef]
- Ferreira, M.L.; Zhang, Y.; Metcalf, B.; Makovey, J.; Bennell, K.L.; March, L.; Hunter, D.J. The influence of weather on the risk of pain exacerbation in patients with knee osteoarthritis—A case-crossover study. Osteoarthr. Cartil. 2016, 24, 2042–2047. [Google Scholar] [CrossRef] [PubMed]
- Dorleijn, D.M.J.; Luijsterburg, P.A.J.; Burdorf, A.; Rozendaal, R.M.; Verhaar, J.A.N.; Bos, P.K.; Bierma-Zeinstra, S.M. Associations between weather conditions and clinical symptoms in patients with hip osteoarthritis: A 2-year cohort study. Pain 2014, 155, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.C.; Fuh, J.-L.; Huang, N.E.; Shia, B.-C.; Wang, S.-J. Patients with migraine are right about their perception of temperature as a trigger: time series analysis of headache diary data. J. Headache Pain 2015, 16, 49. [Google Scholar] [CrossRef] [PubMed]
- Smedslund, G.; Hagen, K.B. Does rain really cause pain? A systematic review of the associations between weather factors and severity of pain in people with rheumatoid arthritis. Eur. J. Pain Lond. Engl. 2011, 15, 5–10. [Google Scholar] [CrossRef] [PubMed]
- de Figueiredo, E.C.Q.; Figueiredo, G.C.; Dantas, R.T. Influence of meteorological elements on osteoarthritis pain: a review of the literature. Rev. Bras. Reumatol. 2011, 51, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, N.; Clore, G.L. Mood, misattribution, and judgments of well-being: informative and directive functions of affective states. J. Pers. Soc. Psychol. 1983, 45, 513. [Google Scholar] [CrossRef]
- Klimstra, T.A.; Frijns, T.; Keijsers, L.; Denissen, J.J.A.; Raaijmakers, Q.A.W.; van Aken, M.A.G.; Koot, H.M.; van Lier, P.A.; Meeus, W.H. Come rain or come shine: individual differences in how weather affects mood. Emotion 2011, 11, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Kööts, L.; Realo, A.; Allik, J. The Influence of the Weather on Affective Experience. J. Individ. Differ. 2011, 32, 74–84. [Google Scholar] [CrossRef]
- Keller, M.C.; Fredrickson, B.L.; Ybarra, O.; Côté, S.; Johnson, K.; Mikels, J.; Conway, A.; Wager, T. A warm heart and a clear head. The contingent effects of weather on mood and cognition. Psychol. Sci. 2005, 16, 724–731. [Google Scholar] [CrossRef] [PubMed]
- McAlindon, T.; Formica, M.; Schmid, C.H.; Fletcher, J. Changes in barometric pressure and ambient temperature influence osteoarthritis pain. Am. J. Med. 2007, 120, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Fukui, T.; Rahman, M.; Ohde, S.; Hoshino, E.; Kimura, T.; Urayama, K.Y.; Omata, F.; Deshpande, G.A.; Takahashi, O. Reassessing the Ecology of Medical Care in Japan. J. Community Health 2017, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wonca. ICPC-2. International Classification of Primary Care. [Internet]. 2nd ed. Oxford: Oxford University Press. 1998. Available online: http://www.who.int/classifications/icd/adaptations/icpc2/en/ (accessed on 12 January 2018).
- Wallace, J.M.; Hobbs, P.V. Atmospheric Science: An Introductory Survey [Internet]. Elsevier Science. 2006. 83 p. (International Geophysics). Available online: https://books.google.co.jp/books?id=HZ2wNtDOU0oC (accessed on 16 January 2018).
- Wanielista, M.; Kersten, R.; Eaglin, R. Hydrology: Water Quantity and Quality Control, 2nd ed.; John Wiley Sons: Hoboken, NJ, USA, 1997; p. 592. [Google Scholar]
- Fitzmaurice, G.M.; Laird, N.M.; Ware, J.H. Applied Longitudinal Analysis; John Wiley Sons: Hoboken, NJ, USA, 2004; p. 506. [Google Scholar]
- Timmermans, E.J.; Schaap, L.A.; Herbolsheimer, F.; Dennison, E.M.; Maggi, S.; Pedersen, N.L.; Castell, M.V.; Denkinger, M.D.; Edwards, M.H.; Limongi, F.; et al. The Influence of Weather Conditions on Joint Pain in Older People with Osteoarthritis: Results from the European Project on OSteoArthritis. J. Rheumatol. 2015, 42, 1885. [Google Scholar] [CrossRef] [PubMed]
- Werner, J. System properties, feedback control and effector coordination of human temperature regulation. Eur. J. Appl. Physiol. 2010, 109, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Seltenrich, N. Between Extremes: Health Effects of Heat and Cold. Environ. Health. Perspect. 2015, 123, A275–A279. [Google Scholar] [CrossRef] [PubMed]
- Gabler, R.E.; Petersen, J.F.; Trapasso, L.M.; Sack, D. Physical Geography, 9th ed.; Cengage Learning: Belmont, NC, USA, 2008; p. 679. [Google Scholar]
- Hosono, T.; Takashima, Y.; Morita, Y.; Nishimura, Y.; Sugita, Y.; Isami, C.; Sakamoto, I.; Tagami, K.; Hidaka, Y.; Suzuki, A. Effects of a heat- and steam-generating sheet on relieving symptoms of primary dysmenorrhea in young women. J. Obstet. Gynaecol. Res. 2010, 36, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Igwea, S.E.; Tabansi-Ochuogu, C.S.; Abaraogu, U.O. TENS and heat therapy for pain relief and quality of life improvement in individuals with primary dysmenorrhea: A systematic review. Complement. Ther. Clin. Pract. 2016, 24, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Navvabi Rigi, S.; kermansaravi, F.; Navidian, A.; Safabakhsh, L.; Safarzadeh, A.; Khazaian, S.; Shafie, S.; Salehian, T. Comparing the analgesic effect of heat patch containing iron chip and ibuprofen for primary dysmenorrhea: a randomized controlled trial. BMC Womens Health 2012, 12, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Huibers, M.J.H.; de Graaf, L.E.; Peeters, F.P.M.L.; Arntz, A. Does the weather make us sad? Meteorological determinants of mood and depression in the general population. Psychiatry Res. 2010, 180, 143–146. [Google Scholar] [CrossRef] [PubMed]
- Mukamal, K.J.; Wellenius, G.A.; Suh, H.H.; Mittleman, M.A. Weather and air pollution as triggers of severe headaches. Neurology 2009, 72, 922–927. [Google Scholar] [CrossRef] [PubMed]
- Strusberg, I.; Mendelberg, R.C.; Serra, H.A.; Strusberg, A.M. Influence of weather conditions on rheumatic pain. J. Rheumatol. 2002, 29, 335–358. [Google Scholar] [PubMed]
- Ozeki, K.; Noda, T.; Nakamura, M.; Ojima, T. Weather and headache onset: A large-scale study of headache medicine purchases. Int. J. Biometeorol. 2015, 59, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Messlinger, K.; Funakubo, M.; Sato, J.; Mizumura, K. Increases in Neuronal Activity in Rat Spinal Trigeminal Nucleus Following Changes in Barometric Pressure—Relevance for Weather-Associated Headaches? Headache J. Head Face Pain 2010, 50, 1449–1463. [Google Scholar] [CrossRef] [PubMed]
- Steffens, D.; Maher, C.G.; Li, Q.; Ferreira, M.L.; Pereira, L.S.M.; Koes, B.W.; Latimer, J. Effect of Weather on Back Pain: Results From a Case-Crossover Study. Arthritis Care Res. 2014, 66, 1867–1872. [Google Scholar] [CrossRef] [PubMed]
- Wilder, F.V.; Hall, B.J.; Barrett, J.P. Osteoarthritis pain and weather. Rheumatology 2003, 42, 955–958. [Google Scholar] [CrossRef] [PubMed]
- Fillingim, R.B.; King, C.D.; Ribeiro-Dasilva, M.C.; Rahim-Williams, B.; Riley, J.L. Sex, Gender, and Pain: A Review of Recent Clinical and Experimental Findings. J. Pain Off. J. Am. Pain Soc. 2009, 10, 447–485. [Google Scholar] [CrossRef] [PubMed]
- Bartley, E.J.; Fillingim, R.B. Sex differences in pain: A brief review of clinical and experimental findings. Br. J. Anaesth. 2013, 111, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Pieretti, S.; Di Giannuario, A.; Di Giovannandrea, R.; Marzoli, F.; Piccaro, G.; Minosi, P.; Aloisi, A.M. Gender differences in pain and its relief. Ann. Ist. Super. Sanita. 2016, 52, 184–189. [Google Scholar] [PubMed]
- Sheppard, L.; Burnett, R.T.; Szpiro, A.A.; Kim, S.-Y.; Jerrett, M.; Pope, C.A.; Brunekreef, B. Confounding and exposure measurement error in air pollution epidemiology. Air Qual. Atmosphere Health 2012, 5, 203–216. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | Statistic |
|---|---|
| Age, Mean (S.D.) | 44.7 (23.3) |
| Age Group, no. (%) | |
| ≤18 yr | 801 (17.6) |
| >18 and <65 | 2680 (58.9) |
| ≥65 | 1067 (23.5) |
| Female, no. (%) | 2365 (52.0) |
| BMI > 25, no. (%) | 722 (15.9) |
| Current Smoker (%) | 499 (11.0) |
| Heavy Drinker † (%) | 1055 (23.3) |
| Family Income, no. (%) | |
| ≥¥10 million | 475 (10.5) |
| ≥¥4 million and <¥10 million | 2836 (62.5) |
| <¥4 million | 1225 (27.0) |
| Education, no. (%) | |
| ≤Junior High | 966 (21.4) |
| ~ Associate | 2305 (51.1) |
| ≥Bachelor | 1236 (27.4) |
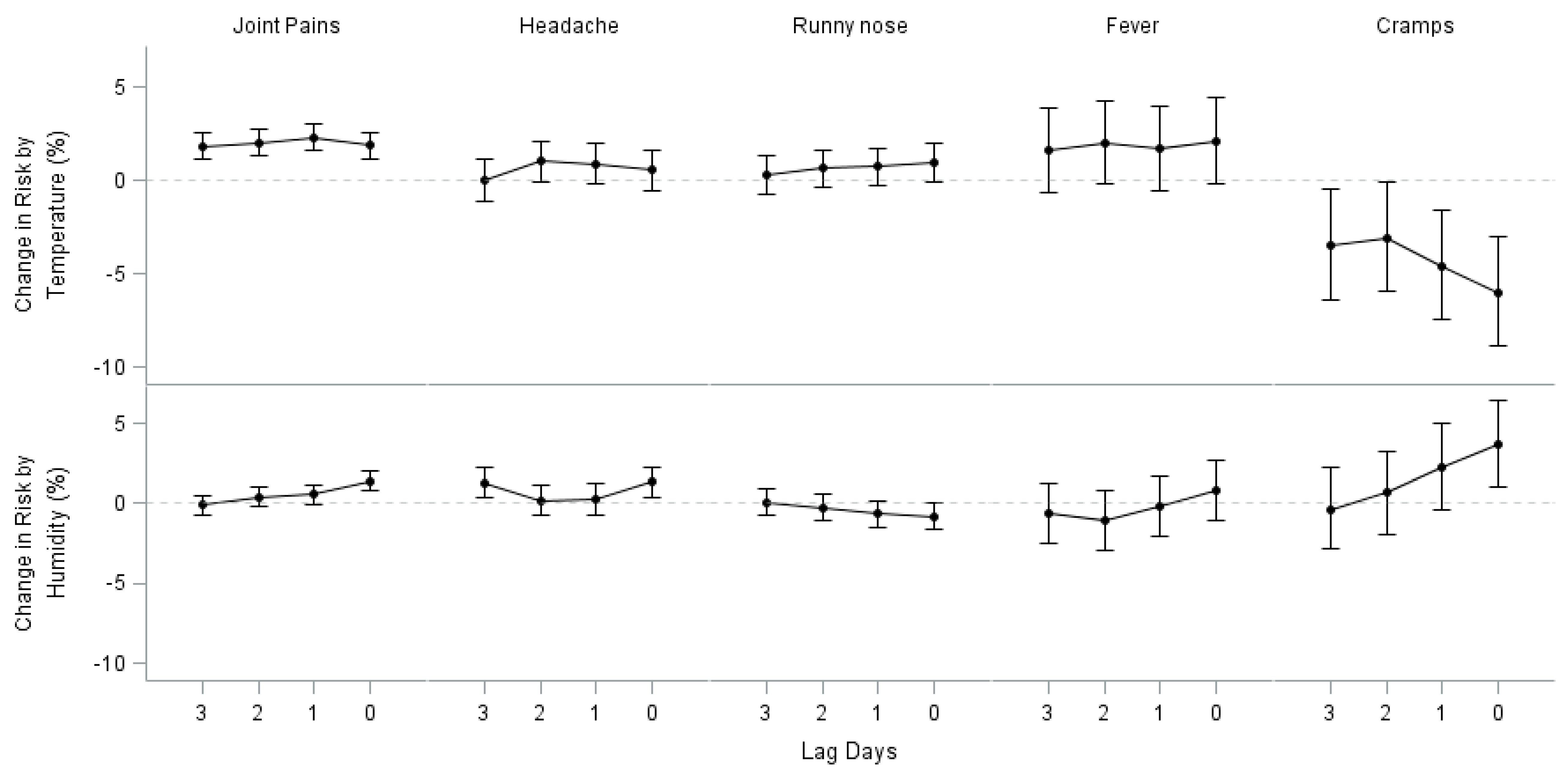
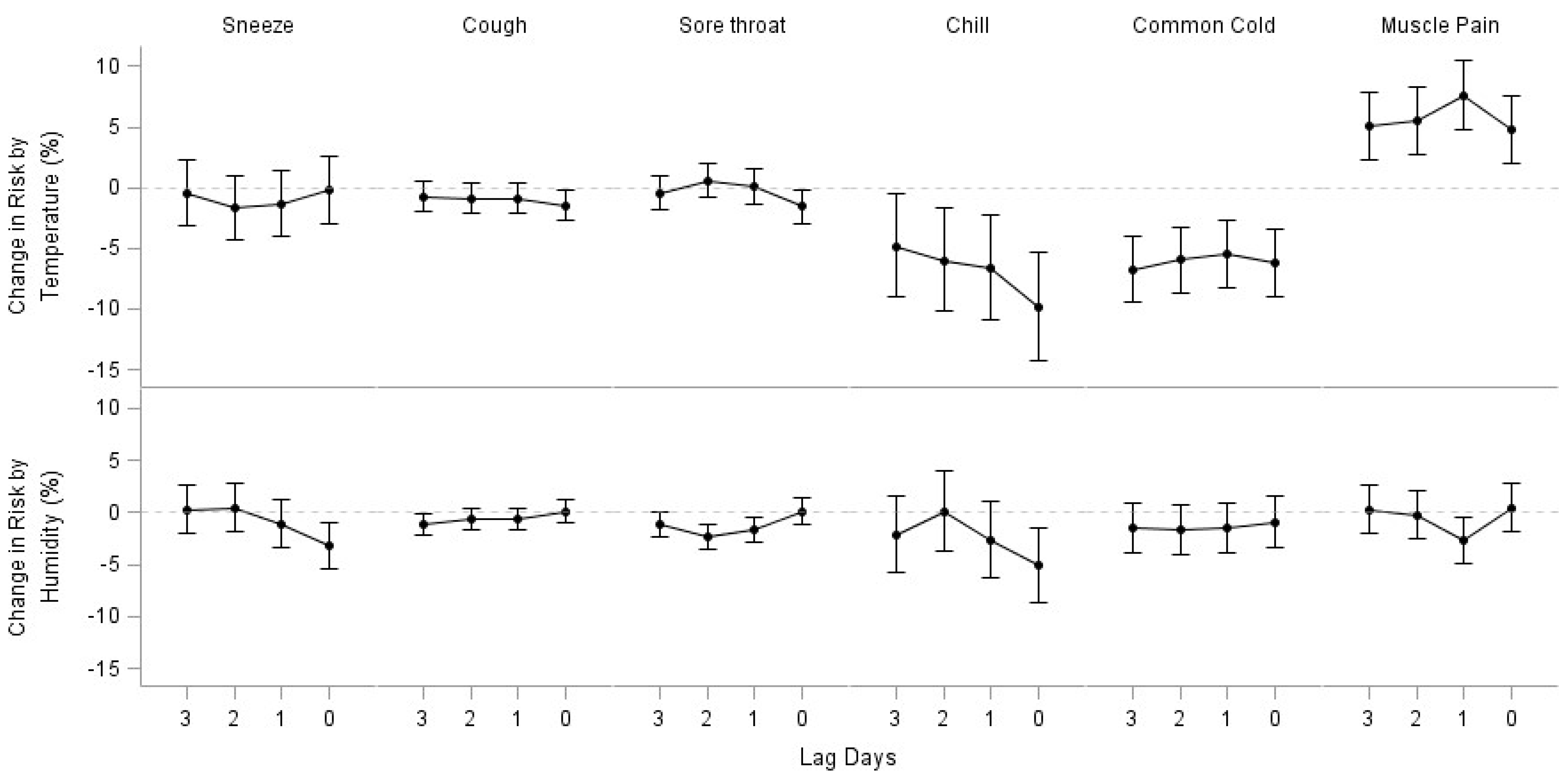
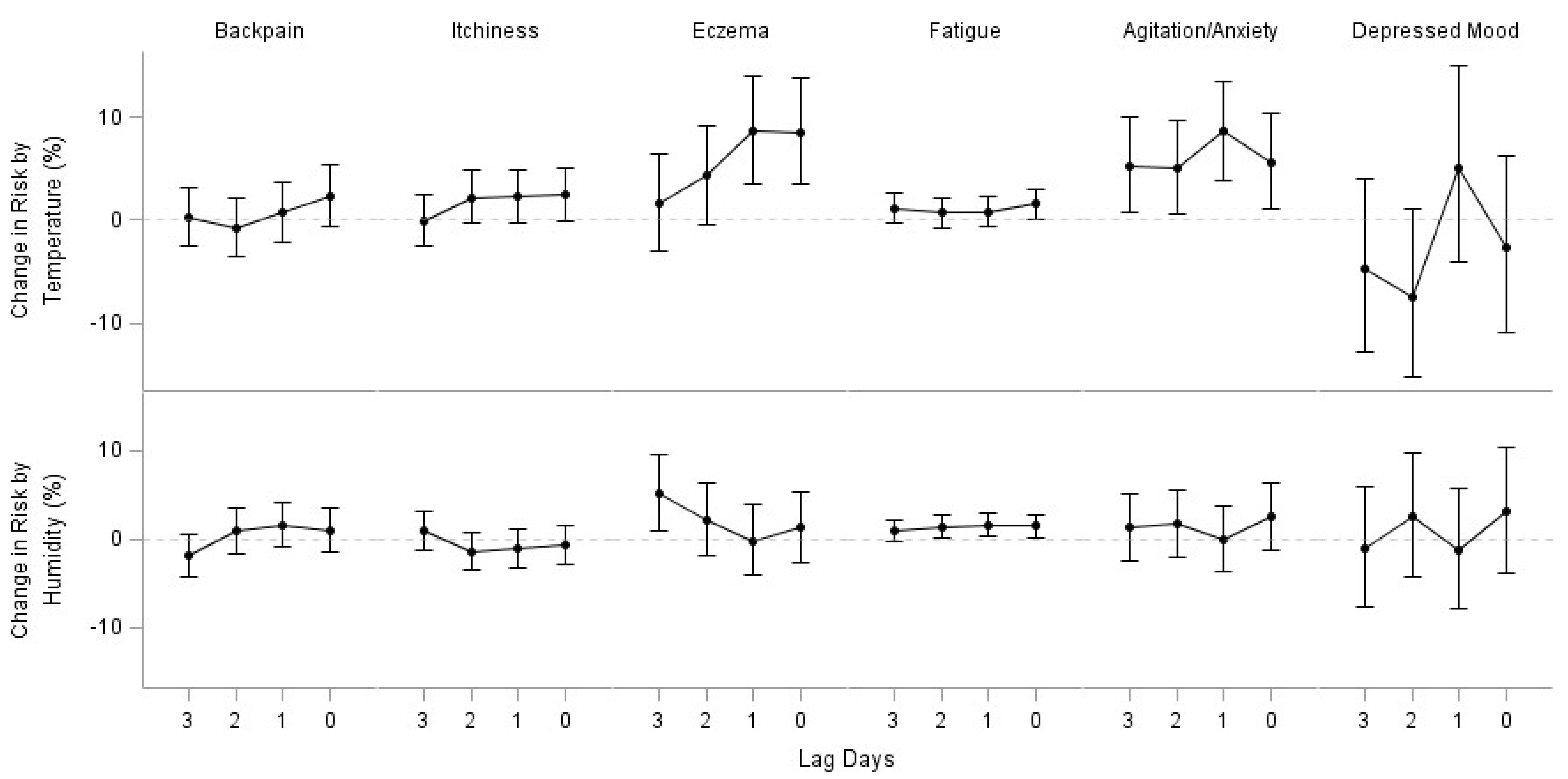
| N | Temperature (95% CI) | Humidity (95% CI) | |
|---|---|---|---|
| Joint Pains | 14,099 | 1.87 (1.15, 2.59) * | 1.38 (0.78, 2.00) * |
| Headache | 2,899 | 0.56 (−0.55, 1.77) | 1.35 (0.40, 2.30) * |
| Runny nose | 4,266 | 0.98 (−0.03, 2.01) | −0.81 (−1.65, 0.03) |
| Sneeze | 502 | −0.21 (−2.95, 2.62) | −3.15 (−5.35, −0.91) * |
| Cough | 3,031 | −1.45 (−2.67, −0.22) * | 0.14 (−0.89, 1.18) |
| Sore throat | 1,634 | −1.57 (−2.99, −0.14) * | 0.12 (−1.10, 1.35) |
| Fever | 696 | 2.13 (−0.13, 4.43) | 0.79 (−1.11, 2.173) |
| Chill | 154 | −9.89 (−14.24, −5.33) * | −5.12 −8.59, −1.52) * |
| Common cold | 424 | −6.21 (−8.96, −3.38) * | −0.91 (−3.31, 1.54) |
| Muscle pain | 483 | 4.77 (2.02, 7.59) * | 0.45 −1.78, 2.73) |
| Backpain | 527 | 2.35 (−0.58, 5.37) | 1.02 (−1.48, 3.59) |
| Itchiness | 995 | 2.48 (−0.10, 5.13) | −0.66 (−2.79, 1.51) |
| Eczema | 358 | 8.54 (3.47, 13.87) * | 1.33 (−2.65, 5.47) |
| Cramps | 319 | −6.00 (−8.88, −3.04) * | 3.70 (1.03, 6.54) * |
| Fatigue | 1,903 | 1.55 (0.09, 3.03) * | 1.52 (0.28, 2.77) * |
| Agitation/anxiety | 256 | 5.57 (1.05, 10.30) * | 2.50 (−1.23, 6.38) |
| Depressed mood | 175 | −2.71 (−10.98, 6.33) | 3.12 (−3.73, 10.45) |
| Symptom | Men | Women | ||
|---|---|---|---|---|
| Temperature (CI) | Humidity (CI) | Temperature (CI) | Humidity (CI) | |
| Joint pains | 1.19 (0.06, 2.34) * | 1.89 (0.92, 2.87) * | 2.34 (1.41, 3.28) * | 1.05 (0.26, 1.83) * |
| Headache | 1.26 (−0.73, 3.28) | −0.16 (−1.82, 1.52) | 0.28 (−1.04, 1.62) | 2.04 (0.9, 3.2) * |
| Runny nose | 0.76 (−0.69, 2.24) | −1.68 (−2.86, −0.5) * | 1.18 (−0.23, 2.62) | 0.04 (−1.14, 1.24) |
| Sneeze | 0.65 (−3.68, 5.18) | −2.81 (−6.21, 0.7) | −0.75 (−4.29, 2.92) | −3.48 (−6.35, −0.52) * |
| Cough | −2.12 (−3.9, −0.3) * | −0.54 (−2.03, 0.98) | −0.9 (−2.55, 0.78) | 0.72 (−0.69, 2.15) |
| Sore throat | −0.5 (−2.7, 1.74) | −1.54 (−3.37, 0.32) | −2.17 (−4, −0.3) * | 1.27 (−0.34, 2.91) |
| Fever | 3.8 (0.3, 7.43) * | −1.94 (−4.66, 0.87) | 0.83 (−2.1, 3.85) | 3.09 (0.44, 5.81) * |
| Chill | −10 (−17.18, −2.19) * | −3.66 (−9.36, 2.39) | −9.9 (−15.26, −4.2) * | −5.97 (−10.28, −1.45) * |
| Common cold | −4.26 (−7.93, −0.44) * | −0.62 (−3.85, 2.71) | −9.14 (−13.28, −4.81) * | −1.37 (−4.95, 2.34) |
| Muscle pain | 5.02 (0.95, 9.26) * | −1.24 (−4.38, 2.01) | 4.45 (0.76, 8.29) * | 2.08 (−1.09, 5.35) |
| Backpain | 5.49 (0.11, 11.16) * | −1.23 (−5.57, 3.31) | 0.92 (−2.55, 4.51) | 2.08 (−0.97, 5.21) |
| Itchiness | 8.8 (4.67, 13.08) * | −1.18 (−4.44, 2.19) | −2.55 (−5.87, 0.89) | −0.22 (−3.01, 2.65) |
| Eczema | 10.39 (2.38, 19.04) * | 0.27 (−6.14, 7.13) | 7.31 (0.87, 14.15) * | 1.92 (−3.05, 7.16) |
| Cramps | N/A | N/A | −5.76 (−8.64, −2.79) * | 3.7 (1.02, 6.45) * |
| Fatigue | 2.91 (0.59, 5.29) * | 0.49 (−1.41, 2.43) | 0.52 (−1.36, 2.44) | 2.29 (0.66, 3.95) * |
| Agitation/anxiety | −1.81 (−9.01, 5.96) | 6.94 (0.18, 14.14) * | 9.46 (3.67, 15.58) * | 0.29 (−4.17, 4.96) |
| Depressed mood | 10.37 (−4.97, 28.17) | 4.9 (−6.9, 18.21) | −10.81 (−20.83, 0.47) | 2.13 (−6.22, 11.23) |
| Symptom | Age ≤ 18 | 18 < Age < 65 | Age ≥ 65 | |||
|---|---|---|---|---|---|---|
| Temperature (CI) | Humidity (CI) | Temperature (CI) | Humidity (CI) | Temperature (CI) | Humidity (CI) | |
| Joint pains | 6.87 (3.68, 10.15) * | 1.52 (−1.04, 4.14) | 1.36 (0.45, 2.27) * | 1.56 (0.79, 2.33) * | 2.56 (1.28, 3.85) * | 0.96 (−0.11, 2.04) |
| Headache | 0.11 (3.49, 3.85) | 1.75 (−1.43, 5.03) | 1.06 (−0.21, 2.35) | 1.12 (0.05, 2.21) * | −2.81 (−5.49, −0.05) * | 2.26 (−0.15, 4.73) |
| Runny nose | −0.19 (−1.8, 1.44) | −0.57 (−1.91, 0.79) | 2.43 (0.97, 3.9) * | −1.59 (−2.76, −0.42) * | −3.56 (−6.38, −0.64) * | 2.38 (−0.2, 5.02) |
| Sneeze | −10.83 (−16.34, −4.95) * | 0.43 (−4.52, 5.62) | 3.13 (−0.39, 6.77) | −5.05 (−7.71, −2.32) * | 0.84 (−6.43, 8.67) | 0.05 (−6.13, 6.64) |
| Cough | −0.84 (−2.8, 1.16) | −2.1 (−3.66, −0.51) * | −0.32 (−2.16, 1.56) | 1.47 (−0.11, 3.07) | −5.91 (−8.72, −3.01) * | 2.05 (−0.55, 4.72) |
| Sore throat | −3.31 (−6.4, −0.12) * | 1.45 (−1.37, 4.35) | −0.42 (−2.16, 1.34) | −0.89 (−2.33, 0.57) | −4.17 (−7.84, −0.35) * | 3.32 (−0.19, 6.94) |
| Fever | 3.91 (−0.12, 8.1) | 0.82 (−2.57, 4.32) | 1.11 (−2.03, 4.36) | 1.08 (−1.61, 3.85) | 1.76 (−3.42, 7.21) | 0.16 (−4.09, 4.61) |
| Chill | N/A | N/A | −8.67 (−13.83, −3.2) * | −5.9 (−10.07, −1.53) * | −15.96 (−24.14, −6.9) * | −1.99 (−8.54, 5.04) |
| Common cold | −10.29 (−20.45, 1.18) | −8.4 (−15.58, −0.61) * | −5.11 (−8.61, −1.47) * | −0.44 (−3.52, 2.74) | −7.96 (−12.85, −2.8) * | 0.42 (−4.04, 5.09) |
| Muscle pain | 9.03 (1.86, 16.7) * | −2.67 (−7.8, 2.74) | 3.55 (0.31, 6.9) * | 1.99 (−0.78, 4.84) | 5.42 (−1.72, 13.08) | −2.51 (−7.86, 3.15) |
| Backpain | N/A | N/A | 1.03 (−2.4, 4.58) | −0.32 (−3.27, 2.73) | 5.44 (−0.22, 11.41) | 4.26 (−0.55, 9.3) |
| Itchiness | 8.99 (3.74, 14.51) * | −1.7 (−5.79, 2.56) | 3.31 (−0.45, 7.23) | −0.4 (−3.43, 2.72) | −6.23 (−10.98, −1.23) * | −0.83 (−5.06, 3.58) |
| Eczema | 6.73 (−0.84, 14.88) | −1.33 (−7.63, 5.4) | 1.61 (−5.97, 9.79) | 8.9 (1.41, 16.94) * | 28.01 (13.57, 44.28) * | −5.16 (−12.27, 2.52) |
| Cramps | −0.79 (−10.63, 10.13) | 8.17 (−2.19, 19.64) | −6.48 (−9.46, −3.39) * | 3.28 (0.53, 6.1) * | N/A | N/A |
| Fatigue | 7.95 (0.49, 15.97) * | 0.41 (−5.27, 6.44) | 0.83 (−0.96, 2.66) | 1.8 (0.26, 3.37) * | 2.31 (−0.35, 5.04) | 0.99 (−1.21, 3.24) |
| Agitation/anxiety | N/A | N/A | 5.71 (−0.1, 11.85) | 0.76 (−3.74, 5.46) | 5.37 (−1.94, 13.22) | 5.43 (−1.31, 12.64) |
| Depressed mood | N/A | N/A | −0.39 (−9.63, 9.79) | 2.36 (−4.89, 10.17) | −15.87 (−34.43, 7.93) | 8.46 (−12.12, 33.85) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, M.; Ohde, S.; Urayama, K.Y.; Takahashi, O.; Fukui, T. Weather and Health Symptoms. Int. J. Environ. Res. Public Health 2018, 15, 1670. https://doi.org/10.3390/ijerph15081670
Lee M, Ohde S, Urayama KY, Takahashi O, Fukui T. Weather and Health Symptoms. International Journal of Environmental Research and Public Health. 2018; 15(8):1670. https://doi.org/10.3390/ijerph15081670
Chicago/Turabian StyleLee, Mihye, Sachiko Ohde, Kevin Y. Urayama, Osamu Takahashi, and Tsuguya Fukui. 2018. "Weather and Health Symptoms" International Journal of Environmental Research and Public Health 15, no. 8: 1670. https://doi.org/10.3390/ijerph15081670
APA StyleLee, M., Ohde, S., Urayama, K. Y., Takahashi, O., & Fukui, T. (2018). Weather and Health Symptoms. International Journal of Environmental Research and Public Health, 15(8), 1670. https://doi.org/10.3390/ijerph15081670