Diarrhoeal Disease in Relation to Possible Household Risk Factors in South African Villages



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
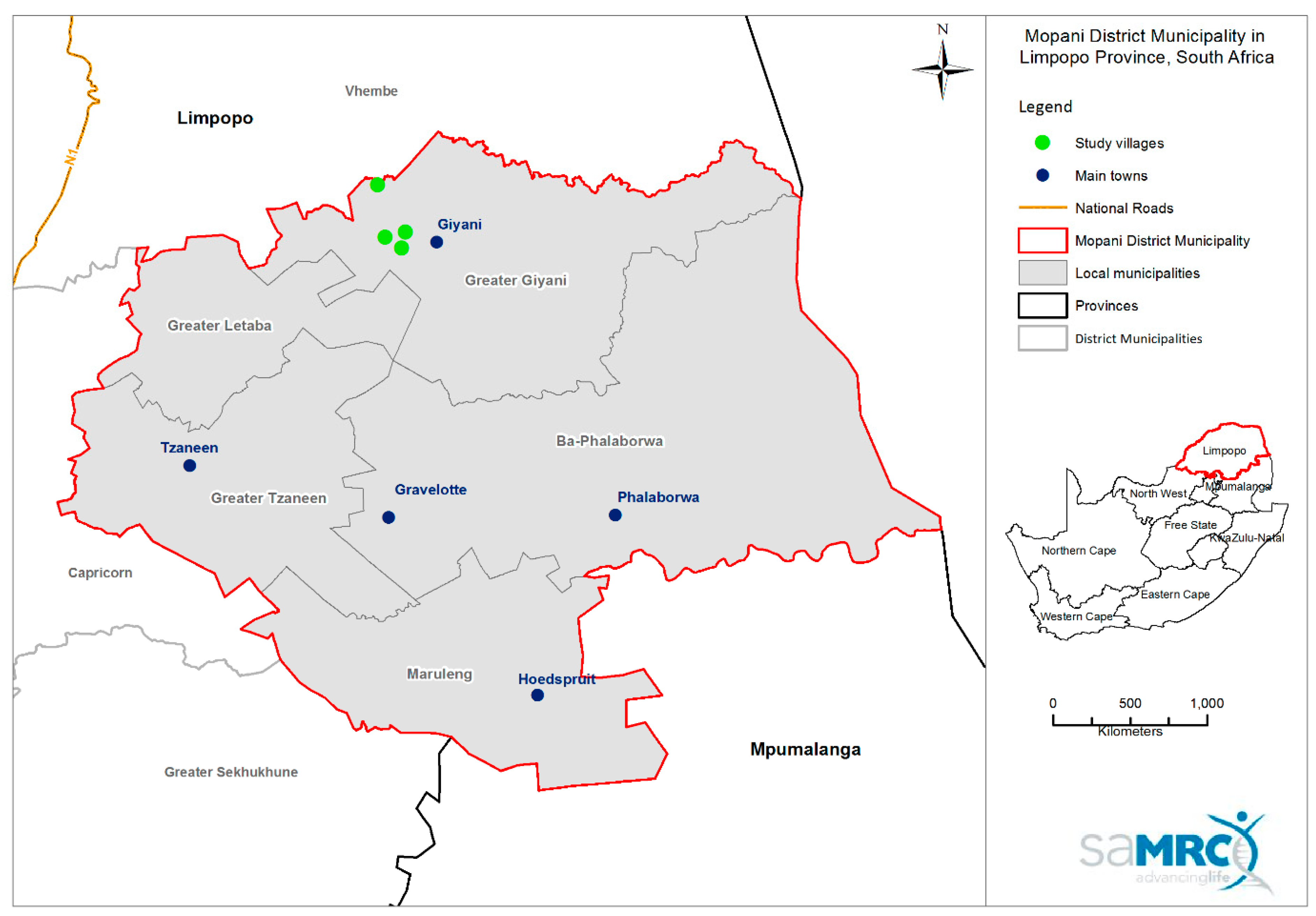
2.2. Study Area
2.3. Data Collection
2.4. Water Sample Collection
2.5. Microbiological Analysis of Water Samples
2.6. Data Management and Statistical Analyses
3. Results
3.1. Sample Description
3.2. Household Water Access and Storage
3.3. Assessment of Drinking Water Quality in A Sub-Sample of Households
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Diarrheal Disease—Key Facts. Available online: http://www.who.int/news-room/fact-sheets/detail/diarrhoeal-disease (accessed on 10 July 2018).
- World Health Organization. World Water Day Report. Available online: http://www.who.int/water_sanitation_health/takingcharge.html (accessed on 5 April 2017).
- Kosek, M.; Bern, C.; Guerrant, R.L. The global burden of diarrhoeal disease, as estimated from studies published between 1992 and 2000. Bull. World Health Organ. 2003, 81, 197–204. [Google Scholar] [PubMed]
- Checkley, W.; Gilman, R.H.; Black, R.E.; Epstein, L.D.; Cabrera, L.; Sterling, C.R.; Moutlon, L.H. Effect of water and sanitation on childhood health in a poor Peruvian peri-urban community. Lancet 2004, 363, 112–118. [Google Scholar] [CrossRef]
- Norman, G.; Pedley, S.; Takkouche, B. Effects of sewerage on diarrhoea and enteric infections: A systematic review and meta-analysis. Lancet Infect. Dis. 2010, 10, 536–544. [Google Scholar] [CrossRef]
- Global Burden of Disease. Data Resources 2015. Available online: http://ghdx.Healthdata.Org/gbd-2015 (accessed on 15 May 2018).
- Awotiwon, O.F.; Pillay-Van Wyk, V.; Dhansay, A.; Day, C.; Bradshaw, D. Diarrhoea in children under five years of age in South Africa (1997–2014). Trop. Med. Int. Health 2006, 21, 1060–1070. [Google Scholar] [CrossRef] [PubMed]
- Norman, R.; Bradshaw, D.; Schneider, M.; Pieterse, D.; Groenewald, P. Revised Burden of Disease Estimates for the Comparative Risk Factor Assessment, South Africa 2000. Available online: http://www.mrc.ac.za/sites/default/files/files/2017-07-03/RevisedBurdenofDiseaseEstimates1.pdf (accessed on 18 June 2018).
- Woldu, W.; Bitwe, B.D.; Gizaw, Z. Socioeconomic factors associated with diarrheal diseases among under-five children of the nomadic population in Northeast Ethiopia. Trop. Med. Health 2016, 44, 40. [Google Scholar] [CrossRef] [PubMed]
- Bitew, B.D.; Woldu, W.; Gizaw, Z. Childhood diarrheal morbidity and sanitation predictors in a nomadic community. Ital. J. Pediatr. 2003, 43, 91. [Google Scholar] [CrossRef] [PubMed]
- Lanata, C.F.; Fischer-Walker, C.L.; Olascoaga, A.C.; Torres, C.X.; Aryee, M.J.; Black, R.E. Global causes of diarrheal disease mortality in children <5 years of age: A systematic review. PLoS ONE 2013, 8, e72788. [Google Scholar] [CrossRef]
- Kotloff, K.L.; Nataro, J.P.; Blackwelder, W.C.; Nasrun, D.; Farag, T.H.; Panchalingam, S.; Wu, Y.; Sow, S.O.; Sur, D.; Breiman, R.F. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): A prospective, case-control study. Lancet 2013, 382, 209–222. [Google Scholar] [CrossRef]
- World Health Organization. Lack of Water and Inadequate Sanitation. 2017. Available online: http://www.who.int/ceh/risks/cehwater/en/ (accessed on 5 April 2017).
- George, C.M.; Perin, J.; Neiswender, D.E.; Calani, K.J.; Norman, W.R.; Perry, H.; Davis, T.P.; Lindquist, E.D. Risk factors for diarrhea in children under five years of age residing in peri-urban communities in Cochabamba, Bolivia. Am. J. Trop. Med. Hyg. 2014, 91, 1190–1196. [Google Scholar] [CrossRef] [PubMed]
- Naicker, N.; Teare, J.; Balakrishna, Y.; Wright, C.Y.; Mathee, A. Indoor temperatures in low cost housing in Johannesburg, South Africa. Int. J. Environ. Res. Pubulic Health 2017, 14, 1410. [Google Scholar] [CrossRef] [PubMed]
- John, J.; Wright, C.Y.; Oosthuizen, M.A.; Steyn, M.; Genthe, B.; le Roux, W.; Albers, P.N.; Oberholster, P.; Pauw, C. Environmental health outcomes and exposure risks among at-risk communities living in the Upper Olifants River Catchment, South Africa. Int. J. Environ. Health Res. 2014, 24, 195–214. [Google Scholar] [CrossRef] [PubMed]
- United States Environmental Protection Agency. Methodology for Deriving Ambient Water Quality Criteria for the Protection of Human Health (2000). Available online: https://www.nj.gov/drbc/library/documents/EPA_human-health-criteria2000.pdf (accessed on 17 July 2018).
- Stata Corp. Statistical Software, Release 14.0; Stata Corporation: College Station, TX, USA, 2001.
- Majuru, B.; Mokoena, M.M.; Jagals, P.; Hunter, P.R. Health impact of small-community water supply reliability. Int. J. Hyg. Environ. Health 2010, 214, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L. Challenges and recommendations for the study of socioeconomic factors and air pollution health effects. Environ. Sci. Policy 2005, 8, 525–533. [Google Scholar] [CrossRef]
- Centres For Disease Control and Prevention. Sample Design. Available online: https://www.cdc.gov/nchs/tutorials/Nhanes/SurveyDesign/SampleDesign/intro.htm (accessed on 10 November 2017).
- Augustina, R.; Sari, T.P.; Satroamidjojo, S.; Bovee-Oudenhoven, I.M.; Feskens, E.J.; Kok, F.J. Association of food-hygiene practices and diarrhea prevalence among Indonesian young children from low socioeconomic urban areas. BMC Public Health 2013, 13, 977. [Google Scholar] [CrossRef] [PubMed]
- Genser, B.; Strina, A.; Teles, C.A.; Prado, M.S.; Barreto, M.I. Risk factors for childhood diarrhea incidence: Dynamic analysis of a longitudinal study. Epidemiology 2006, 17, 658–667. [Google Scholar] [CrossRef] [PubMed]
- Dessalegn, M.; Kumie, A.; Tefera, W. Predictors of under-five childhood diarrhea: Mecha district, West Gojam, Ethiopia. Ethiop. J. Health Dev. 2011, 25, 192–200. [Google Scholar]
- South African Water Quality Guidelines. Available online: http://www.dwa.gov.za/iwqs/wq_guide/Pol_saWQguideFRESH_vol1_Domesticuse.PDF (accessed on 21 May 2018).
- Genthe, B.; Le Roux, W.J.; Schachtschneider, K.; Oberholster, P.J.; Aneck-Hahn, N.H.; Chamier, J. Health risk implications from simultaneous exposure to multiple environmental contaminants. Ecotoxicol. Environ. Saf. 2013, 93, 171–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abia, A.L.K.; Schaefer, L.; Umbombo-Jaswa, E.; Le Roux, W.J. Abundance of Pathogenic Escherichia coli Virulence-Associated Genes in Well and Borehole Water Used for Domestic Purposes in a Peri-Urban Community of South Africa. Int. J. Environ. Res. Public Health 2017, 14, 320. [Google Scholar] [CrossRef] [PubMed]
- Kaper, J.B.; Nataro, J.P.; Mobley, H.L. Pathogenic Escherichia coli. Nat. Rev. Microbiol. 2004, 2, 123–140. [Google Scholar] [CrossRef] [PubMed]
- Mothetha, M.; Nkuna, Z.; Mema, V. The challenges of Rural Water Supply: A Case Study of Rural Areas in Limpopo Province. Council for Scientific and Industrial Research. Available online: https://researchspace.csir.co.za/dspace/handle/10204/7593 (accessed on 18 June 2018).
- Kumpel, E.; Nelson, K.L. Comparing microbial water quality in an intermittent and continuous piped water supply. Water Res. 2013, 47, 5176–5188. [Google Scholar] [CrossRef] [PubMed]
- Machdar, E.; Van Der Steen, N.P.; Raschild-Sally, L.; Lens, P.N. Application of quantitative microbial risk assessment to analyze the public health risk from poor drinking water quality in a low income area in Accra, Ghana. Sci. Total Environ. 2013, 449, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Massey, R.S. Exploring counter-conduct in upgraded informal settlements: The case of women residents in Makhaza and New Rest (Cape Town), South Africa. Habitat Int. 2014, 44, 290–296. [Google Scholar] [CrossRef]
- Jagals, P.; Jagals, C.; Bokako, T. The effect of container-biofilm on the microbiological quality of water used from plastic household containers. J. Water Health 2003, 1, 101–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potgieter, N.; Becker, P.J.; Ehlers, M.M. Evaluation of the CDC safe water-storage intervention to improve the microbiological quality of point-of-use drinking water in rural communities in South Africa. Water S.A. 2009, 35, 505–516. [Google Scholar] [CrossRef]
- Shaheed, A.; Orgill, J.; Ratana, C.; Montgomery, M.A.; Jeuland, M.A.; Brown, J. Water quality risks of ‘improved’ water sources: Evidence from Cambodia. Trop. Med. Int. J. 2014, 19, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Thiam, S.; Diene, A.N.; Fuhrimann, S.; Winkler, M.S.; Sy, I.; Ndione, J.A.; Schindler, C.; Vounatsou, P.; Utzinger, J.; Faye, O. Prevalence of diarrhoea and risk factors among children under five years old in Mbour, Senegal: A cross-sectional study. Infect. Dis. Poverty 2017, 6, 109. [Google Scholar] [CrossRef] [PubMed]
- Levy, K.; Nelson, K.L.; Hubbard, A.; Eisenberg, J.N. Following the water: A controlled study of drinking water storage in northern coastal Ecuador. Environ. Health Perspect. 2008, 116, 1533. [Google Scholar] [CrossRef] [PubMed]
- Du Preez, M.; Mcguidan, K.G.; Conroy, R.M. Solar disinfection of drinking water in the prevention of dysentery in South African children aged under 5 years: The role of participant motivation. Environ. Sci. Technol. 2010, 44, 8744–8749. [Google Scholar] [CrossRef] [PubMed]
- John, V.; Jain, P.; Rahate, M.; Labhasetwar, P. Assessment of deterioration in water quality from source to household storage in semi-urban settings of developing countries. Environ. Monit. Assess. 2014, 186, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Jensen, P.K.; Ensink, J.H.; Jayasinghe, G.; Van Der Hoek, W.; Cairncross, S.; Dalsgaard, A. Domestic transmission routes of pathogens: The problem of in-house contamination of drinking water during storage in developing countries. Trop. Med. Int. Health 2002, 7, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Mellor, J.E.; Smith, J.A.; Samie, A.; Dillingham, R.A. Coliform sources and mechanisms for regrowth in household drinking water in Limpopo, South Africa. J. Environ. Eng. (New York) 2013, 139, 1152–1161. [Google Scholar] [CrossRef]
- Momba, M.N.; Kaleni, P. Regrowth and survival of indicator microorganisms on the surfaces of household containers used for the storage of drinking water in rural communities of South Africa. Water Res. 2002, 36, 3023–3028. [Google Scholar] [CrossRef]
- Taulo, S.; Wetlesen, A.; Abrahamse, R.; Kululanga, G.; Mkakosya, R.; Grimason, A. Microbiological hazard identification and exposure assessment of food prepared and served in rural households of Lungwena, Malawi. Int. J. Food Microbiol. 2008, 125, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Takanashi, J.; Chonan, Y.; Quyen, D.T.; Khan, N.C.; Poudel, K.C.; Jimba, M. Survey of food-hygiene practices at home and childhood diarrhoea in Hanoi, Vietnam. J. Health Popul. Nutr. 2009, 27, 602. [Google Scholar] [PubMed]
- Phaswana-Mafuya, N. Health aspects of sanitation among Eastern Cape (EC) rural communities, South Africa. Curationis 2006, 29, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Stocks, M.E.; Ogden, S.; Haddad, D.; Addiss, D.G.; McGuire, C.; Freeman, M.C. Effect of water, sanitation, and hygiene on the prevention of trachoma: A systematic review and meta-analysis. PLoS Med. 2014, 11, e1001605. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Number of Households | |
|---|---|---|
| n | % | |
| Prevalence of self-reported diarrhoea (for any individual in the household during the past summer) | 82 | 20 |
| Gender of respondent: | ||
| Male | 79 | 19 |
| Female | 329 | 81 |
| Age of respondent in years: | ||
| 18–24 years | 45 | 11 |
| 25–29 years | 46 | 11 |
| 30–39 years | 71 | 17 |
| 40–49 years | 49 | 12 |
| 50–59 years | 80 | 20 |
| ≥60 years | 117 | 29 |
| Number of people in household: | ||
| ≤5 people ! | 194 | 47 |
| 6–7 people | 167 | 41 |
| 8–10 people | 42 | 10 |
| >10 people | 5 | 1 |
| Number of children <5 years of age in household: | ||
| 0 children # | 239 | 58 |
| 2–3 children | 167 | 41 |
| >3 children | 2 | 0.4 |
| Number of years occupying dwelling: | ||
| ≤10 years | 69 | 17 |
| 11–20 years | 80 | 20 |
| >20 years | 259 | 63 |
| Level of education of respondent: | ||
| No schooling | 123 | 30 |
| Primary school | 53 | 13 |
| High school | 194 | 48 |
| Tertiary education | 29 | 7 |
| Average monthly income of household (excluding grants and pensions): | ||
| No income | 121 | 30 |
| ZAR1000 or less | 98 | 24 |
| ZAR1001–ZAR5000 | 100 | 25 |
| ≥ZAR5001 | 17 | 4 |
| Do not know | 72 | 18 |
| Proportion of households with a member receiving the following grants: | ||
| Old age pension | 179 | 44 |
| Disability | 17 | 3 |
| Child support | 284 | 70 |
| Other | 11 | 3 |
| Question and Responses | Prevalence | Univariate Results | ||
|---|---|---|---|---|
| n (%) | OR | 95% CI | p-Value | |
| Where do you mainly get your drinking water from: | ||||
| Stand-pipe (in yard) & | 184 (45) | 1 | - | - |
| Indoor tap | 122 (30) | 2.66 | 2.05–3.45 | <0.001 |
| Stand-pipe (communal) | 75 (19) | 1.57 | 0.90–2.72 | 0.080 |
| Private water seller | 12 (3) | 1.75 | 0.16–18.70 | 0.510 |
| Borehole | 11 (3) | 1.38 | 1.05–1.81 | 0.030 |
| Water tanker/truck * | 2 (0.5) | * | * | * |
| Do you store water for drinking or cooking in a container: | ||||
| Yes & | 394 (97) | 1 | - | - |
| No | 14 (3) | 1.20 | 0.03–43.22 | 0.880 |
| If you store water indoors, does the container have a lid: | ||||
| Yes | 369 (94) | 1 | - | - |
| No | 25 (6) | 1.07 | 0.61–1.87 | 0.740 |
| If you store water indoors, is the water container: | ||||
| Large hole-big enough to get hand in | 266 (68) | 1 | - | - |
| Small hole-too small to get hand in | 128 (33) | 1.91 | 1.00–3.63 | 0.050 |
| When do you add a fresh supply of water to the container: | ||||
| If totally empty | 339 (86) | 1 | - | - |
| If partially empty | 55 (14) | 1.39 | 0.22–0.28 | <0.001 |
| How often do you wash your drinking water storage container: | ||||
| Daily | 26 (7) | 0.72 | 0.38–1.35 | 0.200 |
| Once or twice a week | 237 (60) | - | - | - |
| Monthly | 91 (23) | 0.99 | 0.32–3.07 | 0.970 |
| Never | 39 (10) | 1.09 | 0.35–3.36 | 0.820 |
| Do you boil stored water before drinking it: | ||||
| No & | 373 (95) | 1 | - | - |
| Yes | 21 (5) | 0.69 | 0.27–1.72 | 0.280 |
| Do you add bleach to stored water before drinking it: | ||||
| No & | 341 (87) | 1 | - | - |
| Yes | 53 (13) | 1.83 | 0.86–3.90 | 0.080 |
| If you store food, do you store it in a sealed container: | ||||
| No | 20 (5) | 1.17 | 0.32–4.29 | 0.730 |
| Yes & | 388 (95) | - | - | - |
| When you need to store cooked/perishable food, do you store the food in a: | ||||
| Fridge | 353 (87) | 1 | - | - |
| Food cupboard | 42 (10) | 1.58 | 0.90–2.78 | 0.080 |
| Other (No further details provided) | 13 (3) | 1.8 | 0.63–5.17 | 0.170 |
| What type of toilet does the household mainly use: | ||||
| Flush (Not specified indoor or outdoor) | 12 (3) | 4.60 | 1.80–11.73 | 0.014 |
| Pit latrine | 391 (96) | - | - | - |
| Communal toilet * | 3 (0.7) | * | * | * |
| Open field * | 2 (0.4) | * | * | * |
| How often do you clean your toilet: | ||||
| Weekly | 274 (67) | 1 | - | - |
| Daily | 75 (18) | 1.02 | 0.72–1.44 | 0.890 |
| Seldom | 59 (15) | 0.67 | 0.56–0.81 | 0.010 |
| Variable | OR ^ | 95% CI @ | p-Value | AOR & | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| Do you mainly get your drinking water: | ||||||
| From an indoor tap | 2.51 | 1.51–4.15 | 0.010 | 2.75 | 1.13–6.73 | 0.040 |
| From a stand-pipe (communal) | 1.40 | 0.59–3.35 | 0.341 | 0.92 | 0.37–2.30 | 0.800 |
| From a borehole | 1.34 | 0.71–2.52 | 0.237 | 0.67 | 0.28–1.61 | 0.240 |
| Is the water container: | ||||||
| Small hole, too small to get hand through | 1.94 | 0.96–3.93 | 0.058 | 1.29 | 0.69–2.36 | 0.280 |
| When do you add a fresh supply of water to the container: | ||||||
| If partially empty | 1.75 | 0.85–3.61 | 0.090 | 1.61 | 0.46–5.62 | 0.309 |
| How often do you wash your drinking water storage container: | ||||||
| Once or twice a week | 1.01 | 0.49–2.06 | 0.981 | 0.71 | 0.35–1.45 | 0.220 |
| What do you do with water stored in a container before drinking it: | ||||||
| Add ‘Jik’ (bleach) | 2.13 | 0.67–6.82 | 0.130 | 2.41 | 0.53–11.00 | 0.160 |
| Do you store cooked/perishable food in a food cupboard (i.e., non-refrigerated conditions): | ||||||
| Yes | 2.04 | 1.02–4.06 | 0.046 | 2.14 | 1.44–3.19 | 0.009 |
| Do you store the cooked/perishable food in another way: | ||||||
| Yes | 1.91 | 0.40–9.08 | 0.275 | 1.99 | 0.34–11.43 | 0.30 |
| What type of toilet does the household mainly use: | ||||||
| Flush | 0.30 | 0.02–4.05 | 0.230 | 0.24 | 0.007–7.48 | 0.28 |
| How often do you clean your toilet: | ||||||
| Seldom | 0.83 | 0.63–1.11 | 0.136 | 0.78 | 0.18–3.36 | 0.63 |
| Point of Tested Water Sample | Number of Samples by Total Coliforms Range (Counts/100 mL) | Number of Samples by E. coli Range (Counts/100 mL) | |||||
|---|---|---|---|---|---|---|---|
| 0–5 | 5–100 | >100 | 0 | 1–10 | 11–20 | >20 | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Indoor tap (n = 3) ! | 2 (67) | 0 (0) | 1 (33) | 2 (67) | 0 (0) | 0 (0) | 1 (33) |
| Stand-pipe (inside yard) (n = 98) | 57 (58) | 13 (13) | 28 (28) | 70 (71) | 16 (16) | 1 (1) | 11 (11) |
| Stand-pipe (communal) (n = 8) | 2 (25) | 3 (38) | 3 (28) | 7 (88) | 0 (0) | 0 (0) | 1 (13) |
| Outdoor water tank (n = 2) | 1 (50) | 1 (50) | 0 (0) | 2 (100) | 0 (0) | 0 (0) | 0 (0) |
| Kitchen container (n = 57) | 7 (12) | 14 (25) | 36 (63) | 34 (60) | 10 (18) | 2 (4) | 11(19) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kapwata, T.; Mathee, A.; Le Roux, W.J.; Wright, C.Y. Diarrhoeal Disease in Relation to Possible Household Risk Factors in South African Villages. Int. J. Environ. Res. Public Health 2018, 15, 1665. https://doi.org/10.3390/ijerph15081665
Kapwata T, Mathee A, Le Roux WJ, Wright CY. Diarrhoeal Disease in Relation to Possible Household Risk Factors in South African Villages. International Journal of Environmental Research and Public Health. 2018; 15(8):1665. https://doi.org/10.3390/ijerph15081665
Chicago/Turabian StyleKapwata, Thandi, Angela Mathee, Wouter Jacobus Le Roux, and Caradee Yael Wright. 2018. "Diarrhoeal Disease in Relation to Possible Household Risk Factors in South African Villages" International Journal of Environmental Research and Public Health 15, no. 8: 1665. https://doi.org/10.3390/ijerph15081665
APA StyleKapwata, T., Mathee, A., Le Roux, W. J., & Wright, C. Y. (2018). Diarrhoeal Disease in Relation to Possible Household Risk Factors in South African Villages. International Journal of Environmental Research and Public Health, 15(8), 1665. https://doi.org/10.3390/ijerph15081665