Do Challenge Stress and Hindrance Stress Affect Quality of Health Care? Empirical Evidence from China


Abstract
:1. Introduction
2. Methods
2.1. Sample
2.2. Variables and Instruments
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics of Respondents
3.2. Correlations between Job Stress, Health, and the Quality of Health Care
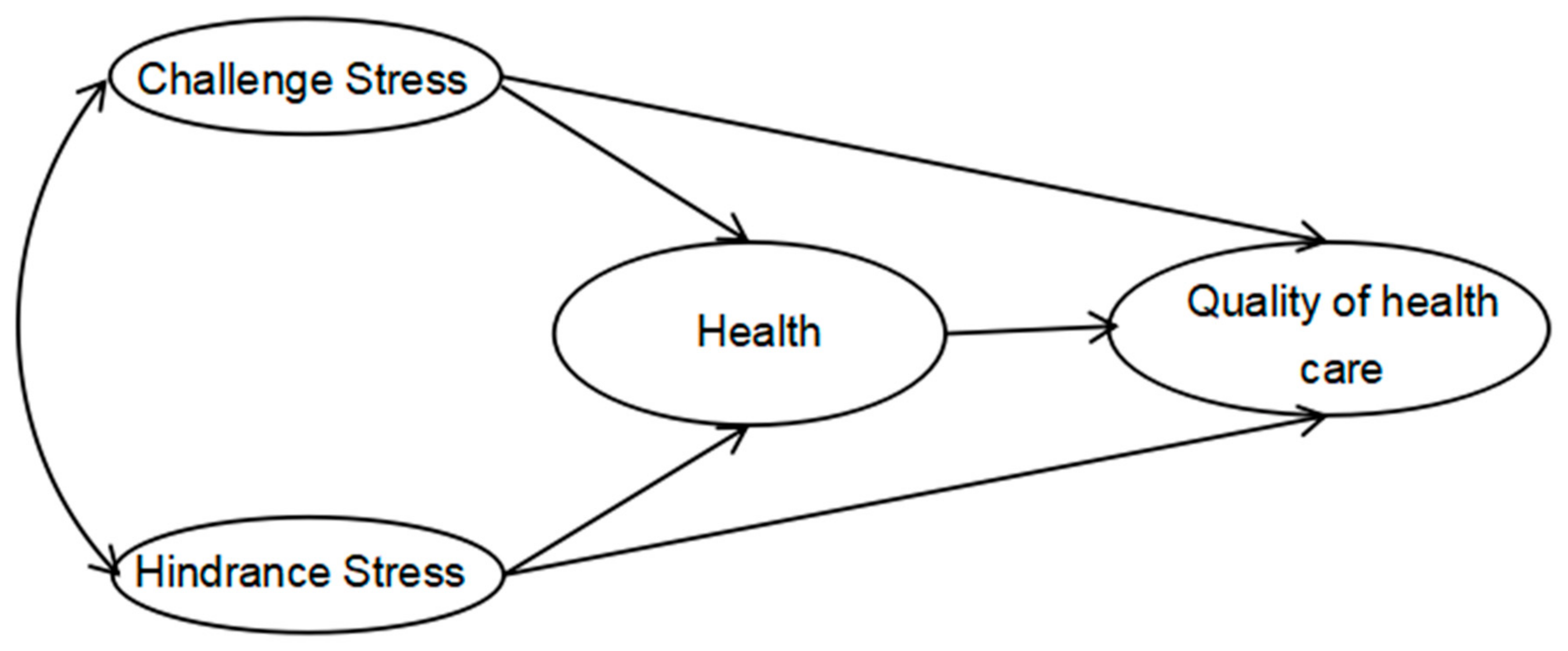
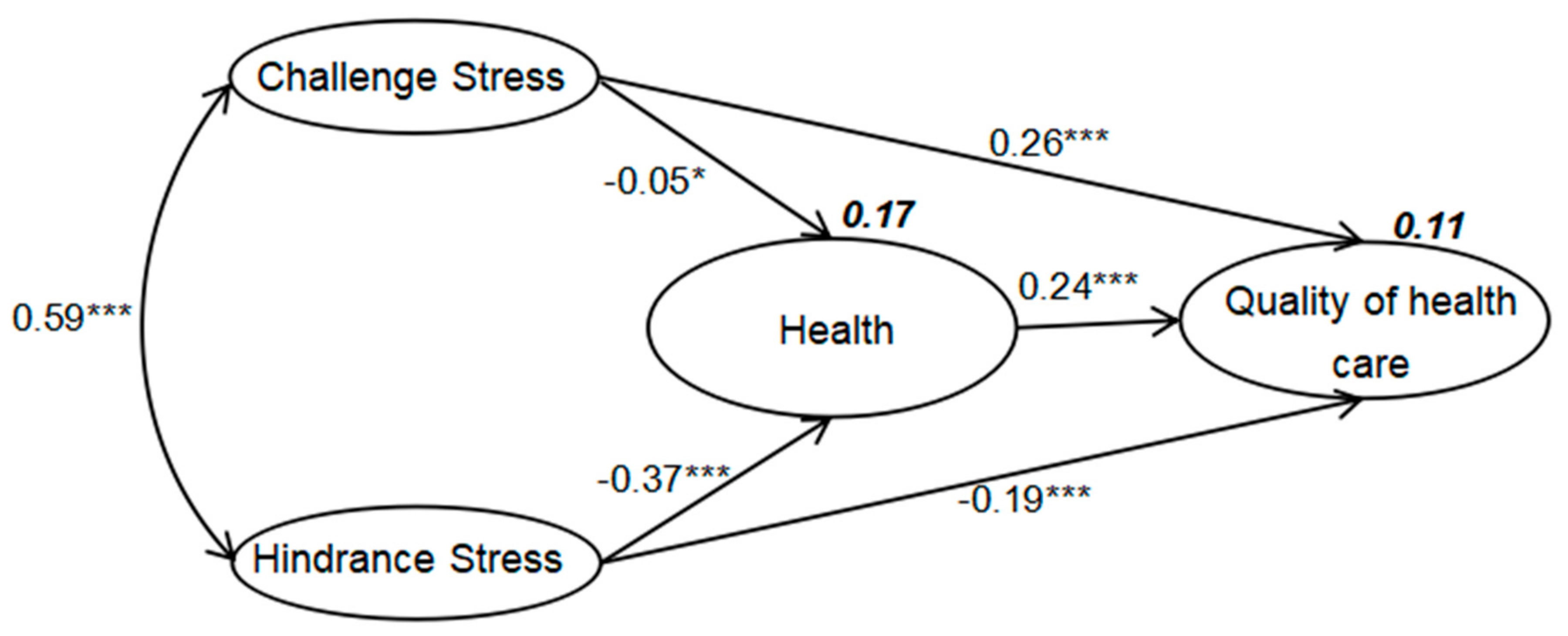
3.3. SEM
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Donabedian, A. The quality of care—How can it be assessed? (reprinted from JAMA, vol. 260, pp. 1743–1748, 1988). Arch. Pathol. Lab. Med. 1997, 121, 1145–1150. [Google Scholar] [PubMed]
- Mant, J. Process versus outcome indicators in the assessment of quality of health care. Int. J. Qual. Health Care 2001, 13, 475–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butt, M.M.; de Run, E.C. Private healthcare quality: Applying a servqual model. Int. J. Health Care Qual. Assur. 2010, 23, 658–673. [Google Scholar] [CrossRef] [PubMed]
- Hayward, R.A.; Hofer, T.P. Estimating hospital deaths due to medical errors—Preventability is in the eye of the reviewer. JAMA 2001, 286, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.W. Medical error: The second victim—The doctor who makes the mistake needs help too. Br. Med. J. 2000, 320, 726–727. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; West, C.; Zhao, X.H.; Novotny, P.; Kolars, J.; Habermann, T.; Sloan, J. Relationship between increased personal well-being and enhanced empathy among internal medicine residents. J. Gen. Intern. Med. 2005, 20, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.S.; Skinner, A.C. Outcomes of physician job satisfaction: A narrative review, implications, and directions for future research. Health Care Manag. Rev. 2003, 28, 119–139. [Google Scholar] [CrossRef]
- Klein, J.; Frie, K.G.; Blum, K.; von dem Knesebeck, O. Psychosocial stress at work and perceived quality of care among clinicians in surgery. BMC Health Serv. Res. 2011, 11, 109. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Ma, M.; Zhu, M.; Liu, Y.; Chen, Q.; Zhang, S.; Deng, J. Challenge or hindrance: Does job stress affect presenteeism among Chinese healthcare workers? J. Occup. Health 2018, 60, 163–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, J.E.; Lemaire, J.B.; Ghali, W.A. Physician wellness: A missing quality indicator. Lancet 2009, 374, 1714–1721. [Google Scholar] [CrossRef]
- Cavanaugh, M.A.; Boswell, W.R.; Roehling, M.V.; Boudreau, J.W. An empirical examination of self-reported work stress among U.S. Managers. J. Appl. Psychol. 2000, 85, 65. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Dong, M.; Wang, S.B.; Zhang, L.; Ng, C.H.; Ungvari, G.S.; Li, J.; Xiang, Y.T. Prevalence of workplace violence against health-care professionals in China: A comprehensive meta-analysis of observational surveys. Trauma Violence Abuse 2018. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.Q.; Wu, J.; Yuan, L.X.; Zhang, S.C.; Jing, M.J.; Zhang, H.S.; Luo, J.L.; Lei, Y.X.; Wang, P.X. Workplace violence and job performance among community healthcare workers in China: The mediator role of quality of life. Int. J. Environ. Res. Public Health 2015, 12, 14872–14886. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Lin, S.; Li, H.; Chai, W.; Zhang, Q.; Wu, Y.; Zhu, W. A study on workplace violence and its effect on quality of life among medical professionals in China. Arch. Environ. Occup. Health 2014, 69, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Qiao, Z.X.; Chen, L.; Chen, M.Q.; Guan, X.; Wang, L.; Jiao, Y.; Yang, J.R.; Tang, Q.H.; Yang, X.X.; Qiu, X.H.; et al. Prevalence and factors associated with occupational burnout among HIV/aids healthcare workers in China: A cross-sectional study. BMC Public Health 2016, 16, 335. [Google Scholar] [CrossRef] [PubMed]
- Wenzhi, C.; Ling, D.; Meng, L.; Min, Y. Antecedents of medical workplace violence in South China. J. Interpers Violence 2011, 26, 312–327. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Fu, H.Q. China’s health care system reform: Progress and prospects. Int. J. Health Plan. Manag. 2017, 32, 240–253. [Google Scholar] [CrossRef] [PubMed]
- Health, M.O. A Hierarchical Approach to Hospital Management; Ministry of Health: Beijing, China, 1989.
- Yang, T.; Ma, T.; Guo, Y.; Chen, Q.; Liu, J.; Deng, J. Reliability and Validity of Chinese Version of Chirurgisches Qualitätssiegel (CQS). Available online: http://kns.cnki.net/KCMS/detail/21.1234.R.20180611.1124.010.html (accessed on 11 June 2018).
- Ansorg, J.; Betzler, M. Das chirurgische qualitätssiegel (CQS). Allgemein Viszeralchirurgie Up2date 2010, 4, 179–190. [Google Scholar] [CrossRef]
- Klingenberg, A. Evaluating the “surgery quality seal” (CQS), a new method of continuous professional development of surgeons, by participants. Results of a pilot study. Der Chirurg Suppl. 2006, 6, 181–186. [Google Scholar]
- Turner-Bowker, D.M.; Bayliss, M.S.; Ware, J.E.; Kosinski, M. Usefulness of the SF-8TM health survey for comparing the impact of migraine and other conditions. Qual. Life Res. 2003, 12, 1003–1012. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E. Improvements in short-form measures of health status: Introduction to a series. J. Clin. Epidemiol. 2008, 61, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Monheit, A.C. Encyclopedia of health services research. Inq. J. Health Care 2010, 47, 262–264. [Google Scholar]
- Ware, J.E.; Snow, K.; Kosinski, M.; Gandek, B. New England Medical Center Hospital. Health Institute. SF-36 Health Survey: Manual and Interpretation Guide; The Health Institute: Boston, MA, USA, 1993. [Google Scholar]
- Mueller, R.O. Basic Principles of Structural Equation Modeling; Springer: New York, NY, USA, 1996. [Google Scholar]
- Gagne, M.; Deci, E.L. Self-determination theory and work motivation. J. Organ Behav. 2005, 26, 331–362. [Google Scholar] [CrossRef] [Green Version]
- Deci, E.L.; Ryan, R.M. Intrinsic Motivation and Self-Determination in Human Behavior; Springer: New York, NY, USA, 1985. [Google Scholar]
- Rasskazova, E.; Ivanova, T.; Sheldon, K. Comparing the effects of low-level and high-level worker need-satisfaction: A synthesis of the self-determination and maslow need theories. Motiv. Emot. 2016, 40, 541–555. [Google Scholar] [CrossRef]
- Hakanen, J.J.; Schaufeli, W.B.; Ahola, K. The job demands-resources model: A three-year cross-lagged study of burnout, depression, commitment, and work engagement. Work Stress 2008, 22, 224–241. [Google Scholar] [CrossRef]
- Bandura, A. Social cognitive theory: An agentic perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Prentice-dunn, S.; Rogers, R.W. Protection motivation theory and preventive health: Beyond the health belief model. Health Educ. Res. 1986, 1, 153–161. [Google Scholar] [CrossRef]
- Milne, S.; Sheeran, P.; Orbell, S. Prediction and intervention in health-related behavior: A meta-analytic review of protection motivation theory. J. Appl. Soc. Psychol. 2000, 30, 106–143. [Google Scholar] [CrossRef]
- Kendler, K.S.; Myers, J.; Prescott, C.A. Sex differences in the relationship between social support and risk for major depression: A longitudinal study of opposite-sex twin pairs. Am. J. Psychiatry 2005, 162, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Lai, C. Exploration of arousing young medical workers’ working enthusiasm. Mod. Hosp. 2008, 11, 113–114. [Google Scholar]
- Loughlin, C.; Barling, J. Young workers’ work values, attitudes, and behaviours. J. Occup. Organ. Psychol. 2001, 74, 543–558. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Sloan, J.A.; Habermann, T.M. The well-being of physicians. Am. J. Med. 2003, 114, 513–519. [Google Scholar] [CrossRef]
- Glasberg, A.L.; Eriksson, S.; Norberg, A. Burnout and ‘stress of conscience’ among healthcare personnel. J. Adv. Nurs. 2007, 57, 392–403. [Google Scholar] [CrossRef] [PubMed]
- Penney, L.M.; Spector, P.E. Job stress, incivility, and counterproductive work behavior (CWB). J. Organ. Behav. 2005, 26, 777–796. [Google Scholar] [CrossRef]
- Weinberg, A.; Creed, F. Stress and psychiatric disorder in healthcare professionals and hospital staff. Lancet 2000, 355, 533–537. [Google Scholar] [CrossRef]
- Babakus, E.; Mangold, W.G. Adapting the servqual scale to hospital services: An empirical investigation. Health Serv. Res. 1992, 26, 767. [Google Scholar] [PubMed]
- Parasuraman, A.; Zeithaml, V.A.; Berry, L.L. Servqual—A multiple-item scale for measuring consumer perceptions of service quality. J. Retail. 1988, 64, 12–40. [Google Scholar]
- Harvey, J.H.; Weary, G. Current issues in attribution theory and research. Annu. Rev. Psychol. 1984, 35, 427–459. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Item | Mean | SD | |
|---|---|---|---|
| Challenge Stress (CS) (1–6) | CS 1. The number of projects and/or assignments I have. | 3.47 | 0.85 |
| CS 2. The amount of time I spend at work. | 3.51 | 0.84 | |
| CS 3. The volume of work that must be accomplished in the allotted time. | 3.40 | 0.91 | |
| CS 4. Time pressures I experience. | 3.45 | 0.90 | |
| CS 5. The amount of responsibility I have. | 3.58 | 0.90 | |
| CS 6. The scope of responsibility my position entails. | 3.47 | 0.88 | |
| Hindrance Stress (HS) (1–5) | HS 1. The degree to which politics rather than performance affects organizational decisions. | 2.82 | 1.12 |
| HS 2. The inability to clearly understand what is expected of me on the job. | 2.33 | 1.06 | |
| HS 3. The amount of red tape I need to go through to get my job done. | 3.07 | 1.05 | |
| HS 4. The lack of job security I have. | 3.05 | 1.15 | |
| HS 5. The degree to which my career seems stalled. | 2.99 | 1.06 | |
| Health (H) (1–8) | H 1. Overall, how would you rate your health during the past 4 weeks? | 3.39 | 0.92 |
| H 2. During the past 4 weeks, how much did physical health problems limit your physical activities (such as walking or climbing stairs)? | 3.79 | 0.95 | |
| H 3. During the past 4 weeks, how much difficulty did you have doing your daily work, both at home and away from home, because of your physical health? | 3.81 | 0.94 | |
| H 4. How much bodily pain have you had during the past 4 weeks? | 4.16 | 1.20 | |
| H 5. During the past 4 weeks, how much energy did you have? | 3.38 | 0.91 | |
| H 6. During the past 4 weeks, how much did your physical health or emotional problems limit your usual social activities with family or friends? | 3.61 | 0.94 | |
| H 7. During the past 4 weeks, how much have you been bothered by emotional problems (such as feeling anxious, depressed, or irritable)? | 3.56 | 0.93 | |
| H 8. During the past 4 weeks, how much did personal or emotional problems keep you from doing your usual work, school or other daily activities? | 3.70 | 0.92 | |
| Quality of health care (QHC) (1–13) | QHC 1. Perform surgeries. | 3.44 | 1.00 |
| QHC 2. Assess diagnostic information. | 3.77 | 0.78 | |
| QHC 3. Make correct diagnoses. | 3.82 | 0.76 | |
| QHC 4. Select appropriate treatments. | 3.82 | 0.79 | |
| QHC 5. Maintain medical records. | 3.85 | 0.76 | |
| QHC 6. Inform patients about rationale for treatment. | 3.90 | 0.78 | |
| QHC 7. Consider psychosocial aspects of illness. | 3.77 | 0.79 | |
| QHC 8. Manage health care resources efficiently. | 3.82 | 0.78 | |
| QHC 9. Evaluate medical literature to optimize clinical decision making. | 3.73 | 0.83 | |
| QHC 10. Participate in implementation of quality improvement programs. | 3.73 | 0.82 | |
| QHC 11. Show empathy for patients and their relatives. | 3.93 | 0.78 | |
| QHC 12. Involve patients in decision-making. | 3.74 | 0.83 | |
| QHC 13. Consider advance health care directives. | 3.89 | 0.79 |
| Final Sample (n = 2426) | Percentage (%) | |
|---|---|---|
| Sex | ||
| Male | 849 | 36.0 |
| Female | 1508 | 64.0 |
| Age | ||
| <25 | 225 | 9.4 |
| 25~30 | 679 | 28.4 |
| 31~35 | 568 | 23.8 |
| 36~40 | 344 | 14.4 |
| 41~45 | 219 | 9.2 |
| 46~50 | 196 | 8.2 |
| >50 | 158 | 5.6 |
| Education | ||
| Below Junior College | 121 | 5.1 |
| Junior College | 514 | 21.6 |
| Bachelor Degree | 1099 | 46.1 |
| Master Degree | 430 | 18.0 |
| Doctor Degree | 221 | 9.3 |
| Title | ||
| Primary | 1058 | 45.6 |
| Middle | 844 | 36.4 |
| Deputy Senior | 297 | 12.8 |
| Senior | 119 | 5.1 |
| Working Age (Year) | ||
| <3 | 436 | 18.3 |
| 3~5 | 486 | 20.4 |
| 6~10 | 616 | 25.9 |
| 11~20 | 470 | 19.8 |
| >20 | 369 | 15.5 |
| Department | ||
| Internal Medicine | 582 | 24.7 |
| Surgical | 411 | 17.4 |
| Maternity | 248 | 10.5 |
| Pediatric | 207 | 8.8 |
| Chinese Medicine/Rehabilitation | 130 | 5.5 |
| Emergency/ICU | 128 | 5.4 |
| Infection/Oncology | 42 | 1.8 |
| Other Clinical Department | 142 | 6.0 |
| Medical Technician | 213 | 9.0 |
| Administration and Logistics | 108 | 4.6 |
| Other | 150 | 6.4 |
| Variables (Mean (M), SD) | Items | |||
|---|---|---|---|---|
| CS | HS | QHC | H | |
| CS (2.41, 1.39) | 1 | |||
| HS (3.89, 0.66) | 0.49 ** | 1 | ||
| QHC (3.66, 0.78) | 0.08 ** | −0.14 ** | 1 | |
| H (3.66, 0.81) | −0.25 ** | −0.36 ** | 0.25 ** | 1 |
| Female | Male | Young | Old | Primary | Secondary | Tertiary | Total | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | |
| Path | ||||||||||||||||
| CS to H | −0.09 | ** | 0.00 | - | 0.02 | - | −0.11 | ** | −0.18 | * | −0.03 | - | −0.40 | - | −0.06 | ** |
| CS to QHC | 0.26 | *** | 0.28 | *** | 0.18 | *** | 0.28 | *** | 0.18 | * | 0.20 | *** | 0.29 | *** | 0.26 | *** |
| HS to H | −0.38 | *** | −0.41 | *** | −0.51 | *** | −0.31 | *** | −0.30 | *** | −0.34 | *** | −0.39 | *** | −0.37 | *** |
| HS to QHC | −0.24 | *** | −0.14 | ** | −0.31 | *** | −0.16 | *** | −0.20 | * | −0.22 | *** | −0.17 | *** | −0.20 | *** |
| H to QHC | 0.22 | *** | 0.29 | *** | 0.16 | *** | 0.29 | *** | 0.32 | *** | 0.18 | *** | 0.25 | *** | 0.24 | *** |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, T.; Yang, T.; Guo, Y.; Wang, Y.; Deng, J. Do Challenge Stress and Hindrance Stress Affect Quality of Health Care? Empirical Evidence from China. Int. J. Environ. Res. Public Health 2018, 15, 1628. https://doi.org/10.3390/ijerph15081628
Ma T, Yang T, Guo Y, Wang Y, Deng J. Do Challenge Stress and Hindrance Stress Affect Quality of Health Care? Empirical Evidence from China. International Journal of Environmental Research and Public Health. 2018; 15(8):1628. https://doi.org/10.3390/ijerph15081628
Chicago/Turabian StyleMa, Tengyang, Tianan Yang, Yilun Guo, Yifei Wang, and Jianwei Deng. 2018. "Do Challenge Stress and Hindrance Stress Affect Quality of Health Care? Empirical Evidence from China" International Journal of Environmental Research and Public Health 15, no. 8: 1628. https://doi.org/10.3390/ijerph15081628