Is Sunlight Exposure Enough to Avoid Wintertime Vitamin D Deficiency in United Kingdom Population Groups?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Studies and Population Groups
2.2. Personal Sun Exposure Assessments
2.3. Dietary Vitamin D and Vitamin D Status
2.4. Ambient UVR Monitoring
2.5. Data Analyses
3. Results
3.1. Volunteer Demographics
3.2. Daily Time Spent Outdoors
3.3. Skin Surface Area Exposed and Use of Sun Protection
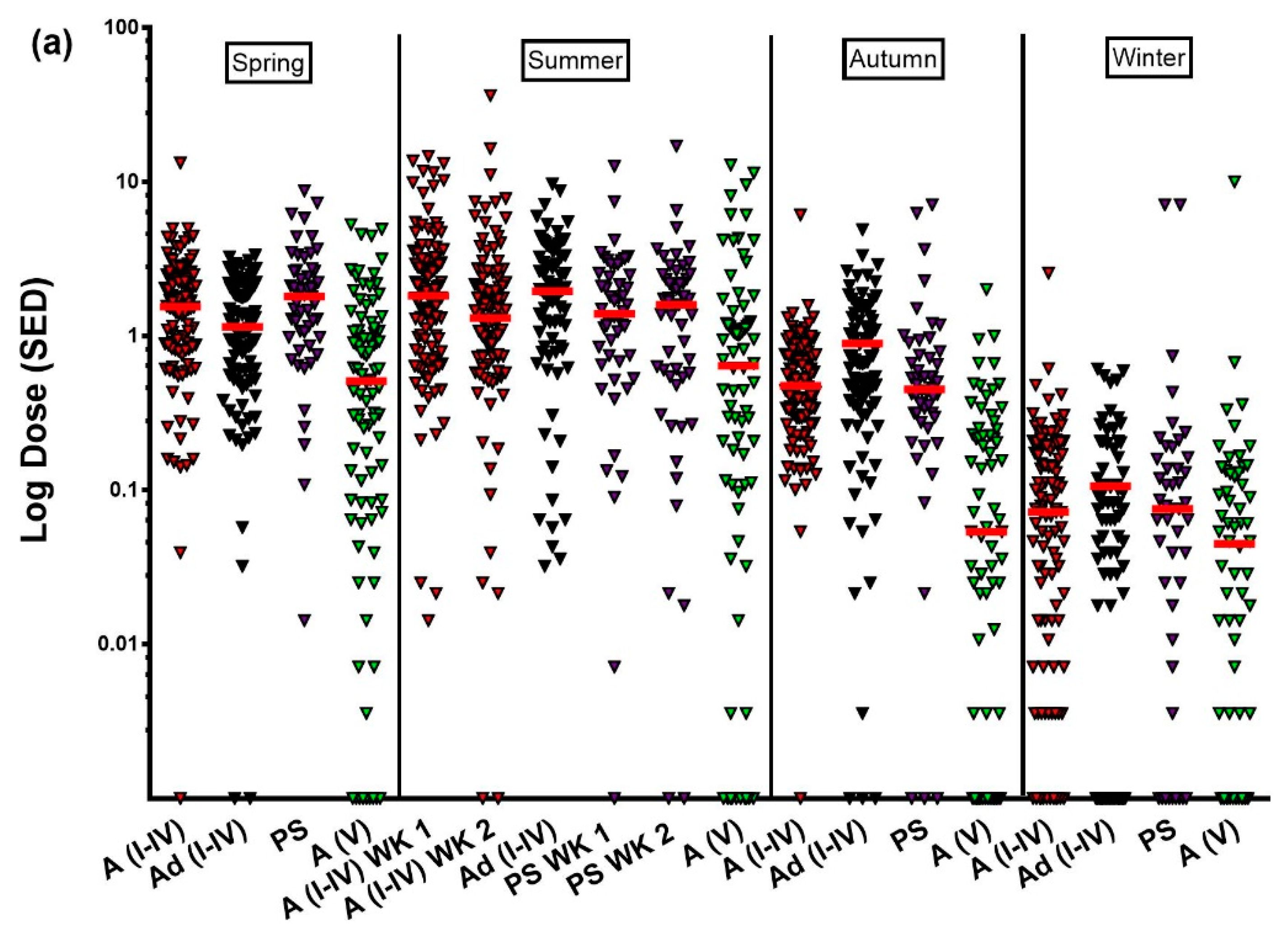
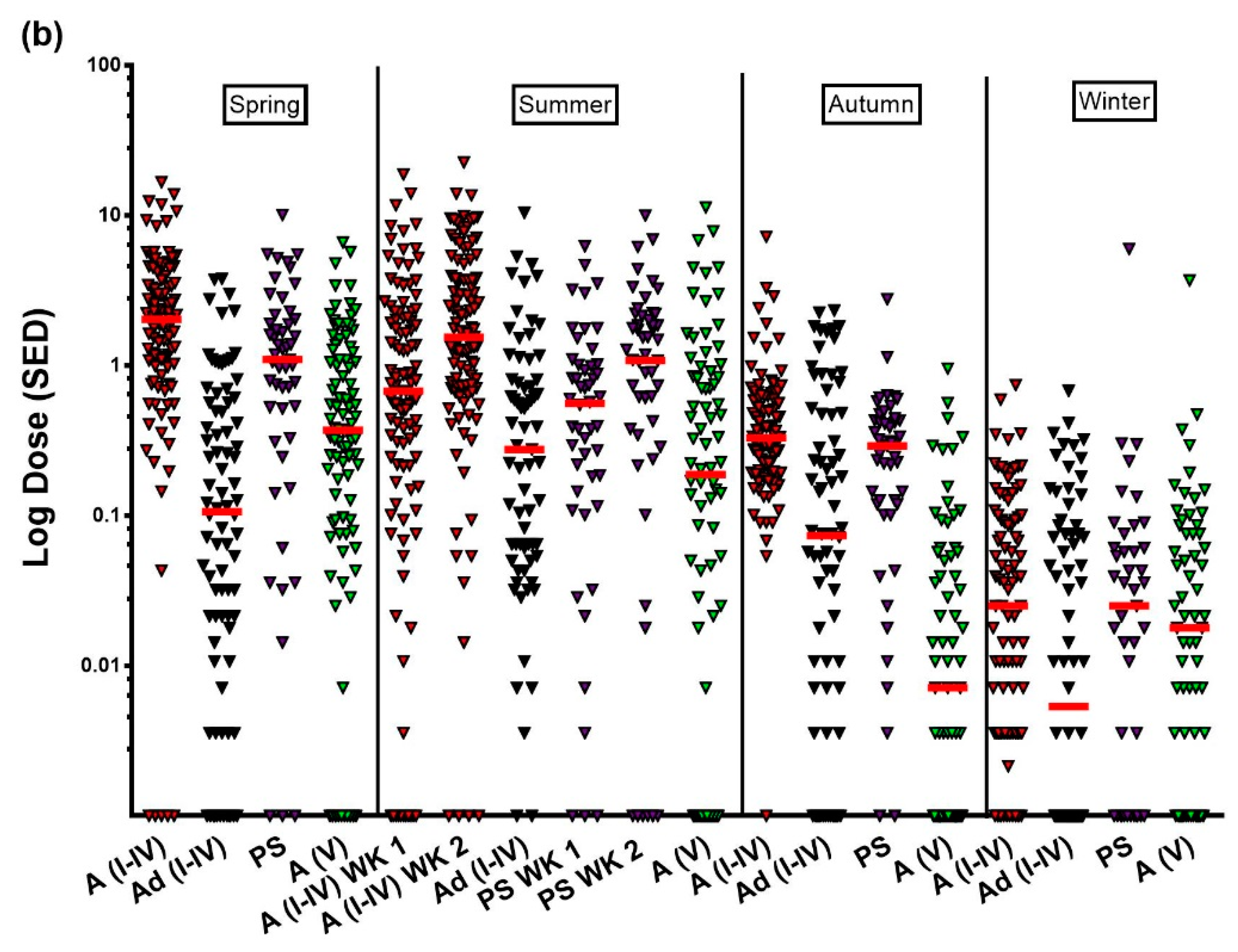
3.4. Personal Sun Exposure Measurements
3.5. Ambient UVR Monitoring
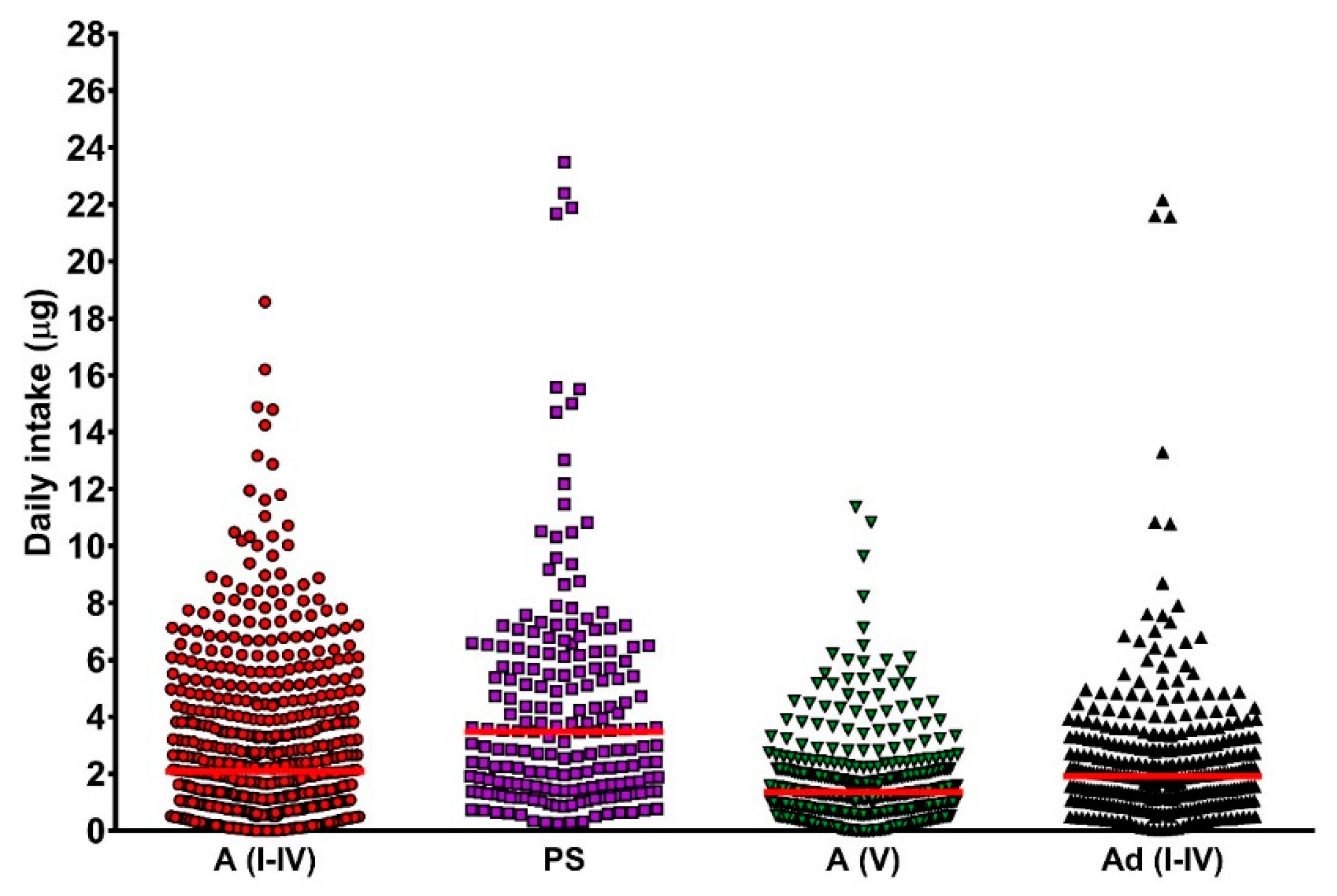
3.6. Dietary Vitamin D Intake
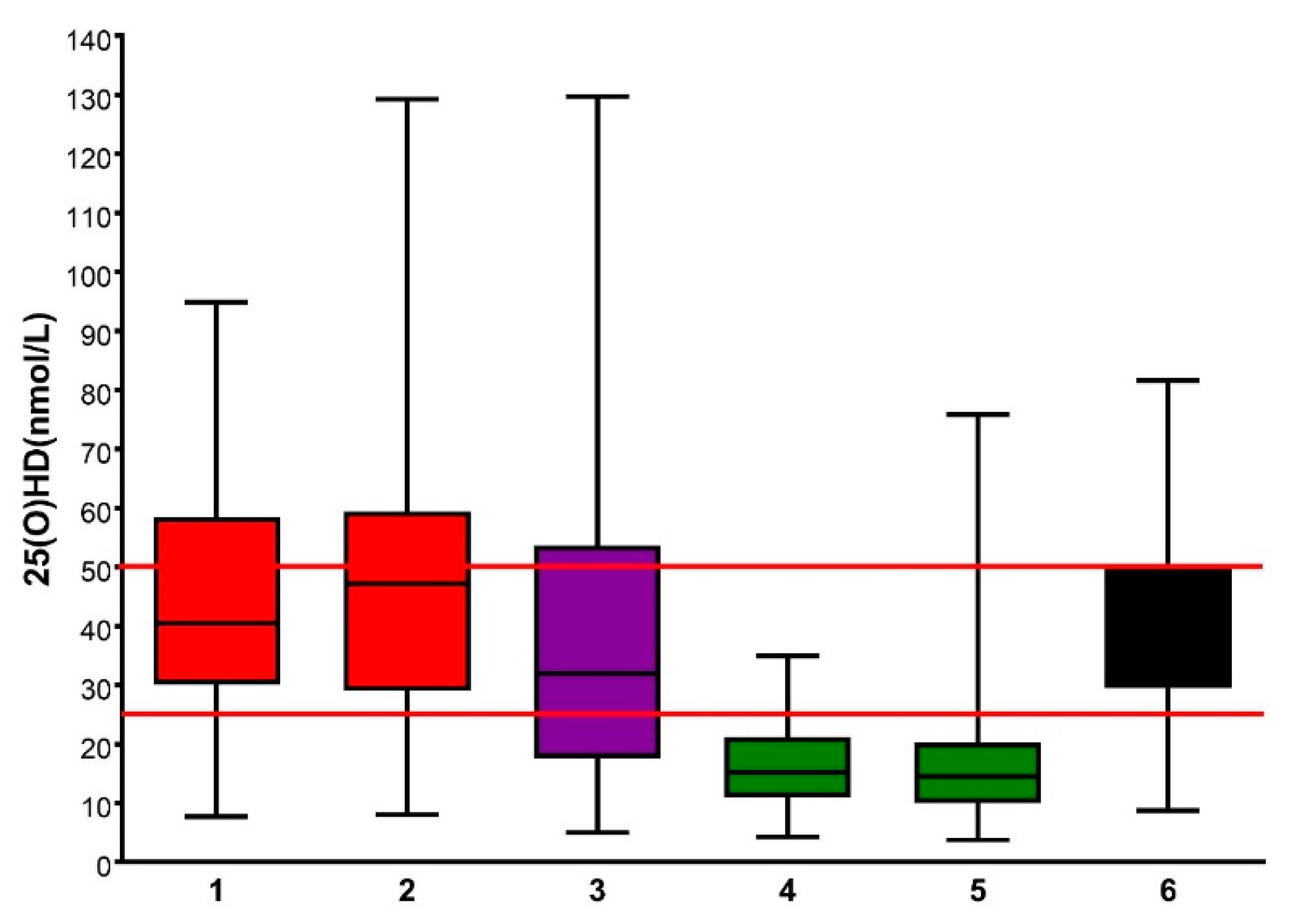
3.7. Assessment of Winter 25(OH)D Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- DeLuca, H.F. Overview of general physiologic features and functions of vitamin D. Am. J. Clin. Nutr. 2004, 80 (Suppl. 6), 1689S–1696S. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer. Vitamin D and Cancer; IARC Working Group Reports; World Health Organisation: Geneva, Switzerland, 2008; Volume 5. [Google Scholar]
- Grant, W.B. Epidemiology of disease risks in relation to vitamin D insufficiency. Prog. Biophys. Mol. Biol. 2006, 92, 65–79. [Google Scholar] [CrossRef] [PubMed]
- SACN Vitamin D and Health. 2016; Crown Copyright. Available online: https://www.gov.uk/government/publications/sacn-vitamin-d-and-health-report (accessed on 21 June 2018).
- Webb, A.R. Who, what, where and when—Influences on cutaneous vitamin D synthesis. Prog. Biophys. Mol. Biol. 2006, 92, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.R.; Holick, M.F. The role of sunlight in the cutaneous production of vitamin D3. In Annual Review of Nutrition; Olson, R.E., Ed.; Annual Reviews Inc.: Palo Alto, CA, USA, 1988; Volume 8, pp. 375–399. ISBN 0-8243-2808-6. [Google Scholar]
- Travel Trends: 2016. Office for National Statistics: London, UK, 2017. Available online: https://www.ons. gov.uk/releases/traveltrends2016 (accessed on 4 July 2018).
- Public Health England (PHE). Ultraviolet Radiation and Vitamin D: The Effects on Health. 2017. Available online: https://www.gov.uk/government/publications/ultraviolet-radiation-and-vitamin-d-the-effectson-health (accessed on 7 June 2018).
- Institute of Medicine. 2011 Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- European Food Safety Authority. Dietary Reference Values for Vitamin D. EFSA J. 2017, 14, e04547. [Google Scholar] [CrossRef]
- Kazantzidis, A.; Smedley, A.R.D.; Kift, R.; Rimmer, J.; Berry, J.L.; Rhodes, L.E.; Webb, A.R. A modeling approach to determine how much UV radiation is available across the UK and Ireland for health risk and benefit studies. Photochem. Photobiol. Sci. 2015, 14, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.R.; Kazantzidis, A.; Kift, R.C.; Farrar, M.D.; Wilkinson, J.; Rhodes, L.E. Meeting Vitamin D Requirements in White Caucasians at UK Latitudes: Providing a Choice. Nutrients 2018, 10, 497. [Google Scholar] [CrossRef] [PubMed]
- NICE Guideline [NG34] Sunlight Exposure: Risks and Benefits. Published Date: February 2016. Available online: https://www.nice.org.uk/guidance/ng34 (accessed on 20 February 2018).
- Rhodes, L.E.; Webb, A.R.; Fraser, H.I.; Kift, R.; Durkin, M.; Vail, A.; O’Brien, S.; Allan, D.; Berry, J.L. Recommended summer sunlight exposure levels can produce sufficient (≥20 ng mL−1) but not the proposed optimal (≥32 ng mL−1) 25(OH)D levels at UK latitudes. J. Investig. Dermatol. 2010, 130, 1411–1418. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.R.; Kift, R.; Durkin, M.T.; O’Brien, S.J.; Vail, A.; Berry, J.L.; Rhodes, L.E. The role of sunlight exposure in determining the vitamin D status of the UK white Caucasian adult population. Br. J. Dermatol. 2010, 163, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Kift, R.; Berry, J.L.; Vail, A.; Durkin, M.T.; Rhodes, L.E.; Webb, A.R. Lifestyle factors including less cutaneous sun exposure contribute to starkly lower vitamin D levels in U.K. South Asians compared with the white population. Br. J. Dermatol. 2013, 169, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, L.E.; Webb, A.R.; Berry, J.L.; Felton, S.J.; Marjanovi, E.J.; Wilkinson, J.D.; Vail, A.; Kift, R. Sunlight exposure behaviour and vitamin D status in photosensitive patients: Longitudinal comparative study with healthy individuals at UK latitude. Br. J. Dermatol. 2014, 171, 1478–1486. [Google Scholar] [CrossRef] [PubMed]
- Farrar, M.D.; Kift, R.; Cooper, S.J.; Berry, J.L.; Durkin, M.T.; Allan, D.; Vail, A.; Webb, A.R.; Rhodes, L.E. Recommended summer sunlight exposure levels fail to produce sufficient vitamin D status in UK adults of South Asian origin. Am. J. Clin. Nutr. 2011, 94, 1219–1224. [Google Scholar] [CrossRef] [PubMed]
- Farrar, M.D.; Mughal, M.Z.; Adams, J.E.; Wilkinson, J.; Berry, J.L.; Edwards, L.; Kift, R.; Marjanovic, E.; Vail, A.; Webb, A.R.; et al. Sun exposure behavior, seasonal vitamin D deficiency and relationship to bone health in adolescents. J. Clin. Endocrinol. Metab. 2016, 101, 3105–3113. [Google Scholar] [CrossRef] [PubMed]
- Schmalwieser, A.; Groebner, J.; Blumthaler, M. UV Index Monitoring in Europe. Photochem. Photobiol. Sci. 2017, 16, 1349–1370. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.; Deane, G.H.W.; Diffey, B.L. Possible dosimeter for ultraviolet radiation. Nature 1976, 261, 169–170. [Google Scholar] [CrossRef] [PubMed]
- Diffey, B.L.; Jansen, C.T.; Urbach, F.; Wulf, H.C. The standard erythema dose: A new photobiological concept. Photodermatol. Photoimmunol. Photomed. 1997, 13, 64–66. [Google Scholar] [CrossRef] [PubMed]
- Berry, J.L.; Selby, P.L.; Davies, M.; Martin, J. Observations from the UK Supra-Regional Assay Service laboratory for the measurement of vitamin D metabolites. J. Steroid. Biochem. Mol. Biol. 2007, 103, 477–479. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.R.; Kift, R.; Berry, J.L.; Rhodes, L.E. The Vitamin D Debate: Translating Controlled Experiments into Reality for Human Sun Exposure Times. Photochem. Photobiol. 2011, 87, 741–745. [Google Scholar] [CrossRef] [PubMed]
- Carrasco-Hernandez, R.; Smedley, A.R.D.; Webb, A.R. Fast calculations of the spectral diffuse-to-global ratios for approximating spectral irradiance at the street canyon level. Theor. Appl. Climatol. 2015. [Google Scholar] [CrossRef]
- Springbett, P.; Buglass, S.; Young, A. Photoprotection and vitamin D status. J. Photochem. Photobiol. B Biol. 2010, 101, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Young, A.R.; Boles, J.; Herzog, B.; Osterwalder, U.; Baschong, W. A sunscreen’s labelled sun protection factor (SPF) may overestimate protection at temperate latitudes: A human in vivo study. J. Investig. Dermatol. 2010, 130, 2457–2462. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.R.; Kazantzidis, A.; Kift, R.C.; Farrar, M.D.; Wilkinson, J.; Rhodes, L.E. Colour Counts: Sunlight and Skin Type as Drivers of Vitamin D Deficiency at UK Latitudes. Nutrients 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Farrar, M.D.; Webb, A.R.; Kift, R.; Durkin, M.T.; Allan, D.; Herbert, A.; Berry, J.L.; Rhodes, L.E. Efficacy of a dose-range of simulated sunlight exposures in raising vitamin D status in South Asian adults: Implications for targeted guidance on sun exposure. Am. J. Clin. Nutr. 2013, 97, 1210–1216. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.R.; Aseem, S.; Kift, R.; Rhodes, L.E.; Farrar, M.D. Target the message: A qualitative study exploring knowledge and cultural attitudes to sunlight and vitamin D in Greater Manchester, UK. Br. J. Dermatol. 2016, 175, 1401–1403. [Google Scholar] [CrossRef] [PubMed]
- Felton, S.J.; Kendall, A.C.; Almaedani, A.F.; Urquhart, P.; Webb, A.R.; Kift, R.; Vail, A.; Nicolaou, A.; Rhodes, L.E. Serum endocannabinoids and N-acyl ethanolamines and the influence of simulated solar UVR exposure in humans in vivo. Photochem. Photobiol. Sci. 2017, 16, 564–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, D.; Fernandez, B.O.; Hamilton, A.; Lang, N.N.; Gallagher, J.M.C.; Newby, D.E.; Feelisch, M.; Weller, R.B. UVA irradiation of human skin vasodilates arterial vasculature and lowers blood pressure independently of nitric oxide synthase. J. Investig. Dermatol. 2014, 134, 1839–1846. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population Group | Total n | Sex (n) | Skin Type (n) |
|---|---|---|---|
| White adults | 218 | 59 M; 159 F | I = 23, II = 116, III = 72, IV = 7 |
| White adolescents | 131 | 51 M; 80 F | I = 15, II = 38, III = 62, IV = 16 |
| Photosensitive adults | 53 | 9 M; 44 F | I = 11, II = 15, III = 13, IV = 7, V = 4, VI = 3 |
| S. Asian adults | 176 | 123 M; 53 F | V = 176 |
| Season | White Adults (Skin Type I–IV) | White Adolescents (Skin Type I–IV) | Photosensitive Adults | S. Asian Adults (Skin Type V) |
|---|---|---|---|---|
| Spring weekday | 52 (34–78) | 62 (40–105) | 70 (46–103) | 72 (46–104) |
| Summer weekday | 51 (34–82) | 76 (43–110) | 75 (45–112) | 63 (34–110) |
| Spring weekend | 95 (60–150) | 73 (36–122) | 80 (35–118) | 60 (30–90) |
| Summer weekend | 70 (30–100) | 80 (36–131) | 75 (40–125) | 80 (38–130) |
| Day | Population Group | Median (IQR) % Skin Surface Area Exposed | |||
|---|---|---|---|---|---|
| Spring | Summer | Autumn | Winter | ||
| Weekday | White adults (skin type I–IV) | 11 (8–13) | 14 (11–19) | 8 (8–16) | 7 (7–15) |
| White adolescents (skin type I–IV) | 11 (8–17) | 14 (8–17) | 8 (8–14) | 8 (8–14) | |
| Photosensitive adults | 11 (11–13) | 11 (11–17) | 11 (11–11) | 11 (11–11) | |
| S. Asian adults (skin type V) | 12 (9–17) | 14 (10–18) | 10 (8–15) | 8 (8–11) | |
| Weekend | White adults (skin type I–IV) | 14 (11–19) | 17 (14–26) | 8 (8–28) | 8 (8–14) |
| White adolescents (skin type I–IV) | 13 (8–19) | 14 (11–19) | 14 (8–17) | 8 (8–16) | |
| Photosensitive adults | 14 (11–17) | 11 (11–17) | 11 (11–11) | 11 (11–11) | |
| S. Asian adults (skin type V) | 10 (8–16) | 14 (8–18) | 8 (8–14) | 8 (8–10) | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kift, R.; Rhodes, L.E.; Farrar, M.D.; Webb, A.R. Is Sunlight Exposure Enough to Avoid Wintertime Vitamin D Deficiency in United Kingdom Population Groups? Int. J. Environ. Res. Public Health 2018, 15, 1624. https://doi.org/10.3390/ijerph15081624
Kift R, Rhodes LE, Farrar MD, Webb AR. Is Sunlight Exposure Enough to Avoid Wintertime Vitamin D Deficiency in United Kingdom Population Groups? International Journal of Environmental Research and Public Health. 2018; 15(8):1624. https://doi.org/10.3390/ijerph15081624
Chicago/Turabian StyleKift, Richard, Lesley E. Rhodes, Mark D. Farrar, and Ann R. Webb. 2018. "Is Sunlight Exposure Enough to Avoid Wintertime Vitamin D Deficiency in United Kingdom Population Groups?" International Journal of Environmental Research and Public Health 15, no. 8: 1624. https://doi.org/10.3390/ijerph15081624